
A Comparison of IgG Index and Oligoclonal Band in the Cerebrospinal Fluid for Differentiating between RRMS and NMOSD


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. IgG Index and CSF-OCB
2.3. Statistical Analyses
3. Results
3.1. Identification of the Optimal Cutoff Values between Groups by ROC Curve Analysis
3.2. Comparison of the IgG Index and CSF-OCB for Differentiating between RRMS and AQP4-Ab NMOSD Based on the Stratification of the Onset Age
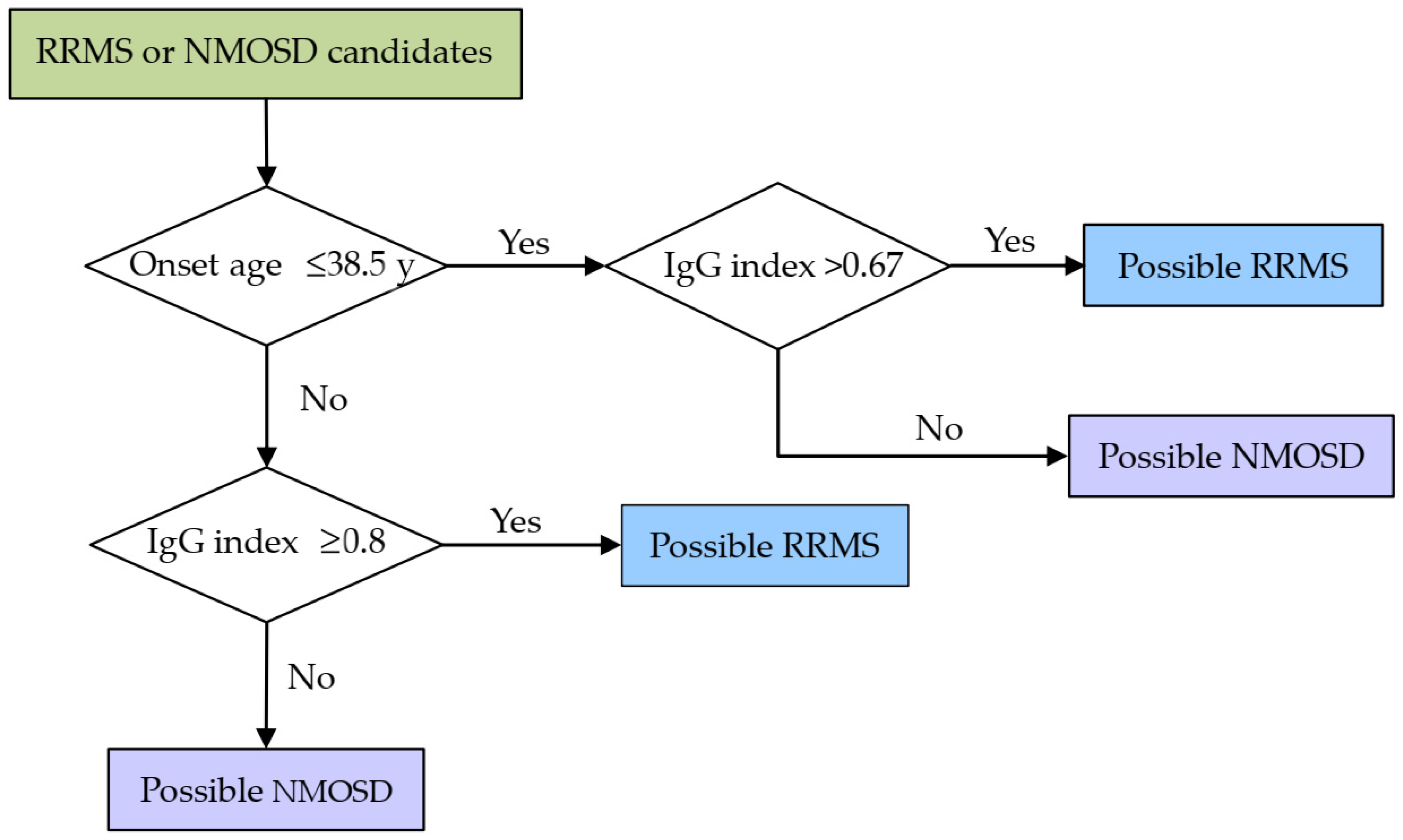
3.3. Establishment of a Discriminative Model
3.4. Sex-Related Differences in CSF Analysis between RRMS and NMOSD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McLean, B.N.; Luxton, R.W.; Thompson, E.J. A study of immunoglobulin G in the cerebrospinal fluid of 1007 patients with suspected neurological disease using isoelectric focusing and the Log IgG-Index. A comparison and diagnostic applications. Brain 1990, 113 Pt 5, 1269–1289. [Google Scholar] [CrossRef]
- Simonsen, C.S.; Flemmen, H.; Lauritzen, T.; Berg-Hansen, P.; Moen, S.M.; Celius, E.G. The diagnostic value of IgG index versus oligoclonal bands in cerebrospinal fluid of patients with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2020, 6, 2055217319901291. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Andersson, M.; Alvarez-Cermeño, J.; Bernardi, G.; Cogato, I.; Fredman, P.; Frederiksen, J.; Fredrikson, S.; Gallo, P.; Grimaldi, L.M.; Grønning, M.; et al. Cerebrospinal fluid in the diagnosis of multiple sclerosis: A consensus report. J. Neurol. Neurosurg. Psychiatry 1994, 57, 897–902. [Google Scholar] [CrossRef] [Green Version]
- Lu, T.; Zhao, L.; Sun, X.; Au, C.; Huang, Y.; Yang, Y.; Bao, J.; Wu, A.; Kermode, A.G.; Qiu, W.; et al. Comparison of multiple sclerosis patients with and without oligoclonal IgG bands in South China. J. Clin. Neurosci. 2019, 66, 51–55. [Google Scholar] [CrossRef]
- Nakashima, I.; Fujihara, K.; Sato, S.; Itoyama, Y. Oligoclonal IgG bands in Japanese patients with multiple sclerosis. A comparative study between isoelectric focusing with IgG immunofixation and high-resolution agarose gel electrophoresis. J. Neuroimmunol. 2005, 159, 133–136. [Google Scholar] [CrossRef]
- Lee, S.S.; Sohn, E.H.; Nam, S.W. Preliminary studies on the clinical features of multiple sclerosis in Korea. J. Clin. Neurol. 2006, 2, 231–237. [Google Scholar] [CrossRef]
- Lunding, J.; Midgard, R.; Vedeler, C.A. Oligoclonal bands in cerebrospinal fluid: A comparative study of isoelectric focusing, agarose gel electrophoresis and IgG index. Acta Neurol. Scand. 2000, 102, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Link, H.; Huang, Y.M. Oligoclonal bands in multiple sclerosis cerebrospinal fluid: An update on methodology and clinical usefulness. J. Neuroimmunol. 2006, 180, 17–28. [Google Scholar] [CrossRef]
- Sun, B.; Ramberger, M.; O’Connor, K.C.; Bashford-Rogers, R.J.M.; Irani, S.R. The B cell immunobiology that underlies CNS autoantibody-mediated diseases. Nat. Rev. Neurol. 2020, 16, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Jurynczyk, M.; Geraldes, R.; Probert, F.; Woodhall, M.R.; Waters, P.; Tackley, G.; DeLuca, G.; Chandratre, S.; Leite, M.I.; Vincent, A.; et al. Distinct brain imaging characteristics of autoantibody-mediated CNS conditions and multiple sclerosis. Brain 2017, 140, 617–627. [Google Scholar] [CrossRef]
- Manouchehrinia, A.; Beiki, O.; Hillert, J. Clinical course of multiple sclerosis: A nationwide cohort study. Mult. Scler. 2017, 23, 1488–1495. [Google Scholar] [CrossRef]
- Scalfari, A.; Neuhaus, A.; Degenhardt, A.; Rice, G.P.; Muraro, P.A.; Daumer, M.; Ebers, G.C. The natural history of multiple sclerosis: A geographically based study 10: Relapses and long-term disability. Brain 2010, 133, 1914–1929. [Google Scholar] [CrossRef]
- Mao-Draayer, Y.; Thiel, S.; Mills, E.A.; Chitnis, T.; Fabian, M.; Katz Sand, I.; Leite, M.I.; Jarius, S.; Hellwig, K. Neuromyelitis optica spectrum disorders and pregnancy: Therapeutic considerations. Nat. Rev. Neurol. 2020, 16, 154–170. [Google Scholar] [CrossRef]
- Wingerchuk, D.M.; Banwell, B.; Bennett, J.L.; Cabre, P.; Carroll, W.; Chitnis, T.; de Seze, J.; Fujihara, K.; Greenberg, B.; Jacob, A.; et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015, 85, 177–189. [Google Scholar] [CrossRef]
- Freedman, M.S.; Thompson, E.J.; Eisenhammer, F.D.; Giovannoni, G.; Grimsley, G.; Keir, G.; Ohman, S.; Racke, M.K.; Sharief, M.; Sindic, C.J. Recommended standard of cerebrospinal fluid analysis in the diagnosis of multiple sclerosis—A consensus statement. Arch. Neurol. 2005, 62, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Reiber, H. Cerebrospinal fluid—Physiology, analysis and interpretation of protein patterns for diagnosis of neurological diseases. Mult. Scler. 1998, 4, 99–107. [Google Scholar] [CrossRef]
- Gasperi, C.; Salmen, A.; Antony, G.; Bayas, A.; Heesen, C.; Kümpfel, T.; Linker, R.A.; Paul, F.; Stangel, M.; Tackenberg, B.; et al. Association of Intrathecal Immunoglobulin G Synthesis With Disability Worsening in Multiple Sclerosis. JAMA Neurol. 2019, 76, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Lucchinetti, C.; Brück, W.; Parisi, J.; Scheithauer, B.; Rodriguez, M.; Lassmann, H. Heterogeneity of multiple sclerosis lesions: Implications for the pathogenesis of demyelination. Ann. Neurol. 2000, 47, 707–717. [Google Scholar] [CrossRef]
- Hauser, S.L.; Waubant, E.; Arnold, D.L.; Vollmer, T.; Antel, J.; Fox, R.J.; Bar-Or, A.; Panzara, M.; Sarkar, N.; Agarwal, S.; et al. B-cell depletion with rituximab in relapsing-remitting multiple sclerosis. N. Engl. J. Med. 2008, 358, 676–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granqvist, M.; Boremalm, M.; Poorghobad, A.; Svenningsson, A.; Salzer, J.; Frisell, T.; Piehl, F. Comparative Effectiveness of Rituximab and Other Initial Treatment Choices for Multiple Sclerosis. JAMA Neurol. 2018, 75, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ineichen, B.V.; Moridi, T.; Granberg, T.; Piehl, F. Rituximab treatment for multiple sclerosis. Mult. Scler. 2020, 26, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Salzer, J.; Svenningsson, R.; Alping, P.; Novakova, L.; Björck, A.; Fink, K.; Islam-Jakobsson, P.; Malmeström, C.; Axelsson, M.; Vågberg, M.; et al. Rituximab in multiple sclerosis: A retrospective observational study on safety and efficacy. Neurology 2016, 87, 2074–2081. [Google Scholar] [CrossRef] [Green Version]
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple Sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef]
- Parrado-Fernández, C.; Blennow, K.; Hansson, M.; Leoni, V.; Cedazo-Minguez, A.; Björkhem, I. Evidence for sex difference in the CSF/plasma albumin ratio in ~20 000 patients and 335 healthy volunteers. J. Cell. Mol. Med. 2018, 22, 5151–5154. [Google Scholar] [CrossRef] [Green Version]
- Castellazzi, M.; Morotti, A.; Tamborino, C.; Alessi, F.; Pilotto, S.; Baldi, E.; Caniatti, L.M.; Trentini, A.; Casetta, I.; Granieri, E.; et al. Increased age and male sex are independently associated with higher frequency of blood-cerebrospinal fluid barrier dysfunction using the albumin quotient. Fluids Barriers CNS 2020, 17, 14. [Google Scholar] [CrossRef]
- Meixensberger, S.; Bechter, K.; Dersch, R.; Feige, B.; Maier, S.; Schiele, M.A.; Runge, K.; Denzel, D.; Nickel, K.; Spieler, D.; et al. Sex difference in cerebrospinal fluid/blood albumin quotients in patients with schizophreniform and affective psychosis. Fluids Barriers CNS 2020, 17, 67. [Google Scholar] [CrossRef]
- McCudden, C.R.; Brooks, J.; Figurado, P.; Bourque, P.R. Cerebrospinal Fluid Total Protein Reference Intervals Derived from 20 Years of Patient Data. Clin. Chem. 2017, 63, 1856–1865. [Google Scholar] [CrossRef]
- Misu, T.; Fujihara, K.; Kakita, A.; Konno, H.; Nakamura, M.; Watanabe, S.; Takahashi, T.; Nakashima, I.; Takahashi, H.; Itoyama, Y. Loss of aquaporin 4 in lesions of neuromyelitis optica: Distinction from multiple sclerosis. Brain 2007, 130, 1224–1234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roemer, S.F.; Parisi, J.E.; Lennon, V.A.; Benarroch, E.E.; Lassmann, H.; Bruck, W.; Mandler, R.N.; Weinshenker, B.G.; Pittock, S.J.; Wingerchuk, D.M.; et al. Pattern-specific loss of aquaporin-4 immunoreactivity distinguishes neuromyelitis optica from multiple sclerosis. Brain 2007, 130, 1194–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadopoulos, M.C.; Verkman, A.S. Aquaporin 4 and neuromyelitis optica. Lancet Neurol. 2012, 11, 535–544. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; Royston, P. The cost of dichotomising continuous variables. BMJ 2006, 332, 1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | RRMS | AQP4-Ab NMOSD | p | Correlation Coefficient ▲ |
|---|---|---|---|---|
| No. of participants | 81 | 90 | ||
| No. of females (%) | 57 (70.3) | 71 (78.9) | 0.22 | −0.098 |
| Age at onset, median (range), year | 30 (14–68) | 48.5 (18–72) | <0.001 | 0.540 |
| Age at LP, median (range), year | 33 (14–68) | 52 (18–72) | <0.001 | 0.516 |
| CSF | ||||
| Total protein, median, mg/L (range) | 326 (160–1167) | 381.5 (185–2883) | 0.029 | 0.168 |
| Albumin, median, mg/L (range) | 182 (95–711) | 219 (87–1790) | 0.023 | 0.175 |
| IgG, median, mg/L (range) | 43.4 (12.2–155) | 38.05 (9.3–448) | 0.319 | −0.076 |
| Serum | ||||
| Albumin, median, g/L (range) | 42.1 (28.8–49.1) | 39.75 (33.1–51.5) | <0.001 | −0.279 |
| IgG, median, g/L (range) | 10.3 (4.7–21.1) | 10.7 (4.1–35.7) | 0.746 | 0.025 |
| C3, g/L (range) # | 0.75 (0.56–1.21) | 0.76 (0.55–1.22) | 0.484 | −0.068 |
| C4, g/L (range) # | 0.18 (0.07–0.4) | 0.17 (0.08–0.49) | 0.797 | −0.025 |
| Qalb, median (range) | 4.22 (2.05–18.37) | 5.47 (2.28–49.31) | 0.005 | 0.215 |
| QIgG, median (range) | 4.24 (1.04–14.83) | 3.67 (1.12–24.62) | 0.477 | −0.055 |
| IgG index, median (range) | 0.87 (0.4–2.09) | 0.66 (0.37–1.46) | <0.001 | −0.411 |
| No. of positive CSF-OCB (%) * | 38 (67.9) | 6 (23.1) | <0.001 | −0.418 |
| Onset Age | Methods | Results | Diagnosis | k | p | Sen | Spe | PPV | NPV | PA | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| RRMS | NMOSD | ||||||||||
| ≤38.5 y | CSF-OCB | − | 12 | 2 | 0.10 | 0.578 | 0.707 | 0.5 | 0.935 | 0.143 | 0.689 |
| + | 29 | 2 | |||||||||
| >38.5 y | − | 6 | 18 | 0.43 | 0.015 | 0.6 | 0.818 | 0.692 | 0.75 | 0.73 | |
| + | 9 | 4 | |||||||||
| Total | − | 18 | 20 | 0.40 | <0.001 | 0.679 | 0.769 | 0.864 | 0.526 | 0.707 | |
| + | 38 | 6 | |||||||||
| ≤38.5 y | IgG index | − * | 13 | 12 | 0.40 | <0.001 | 0.783 | 0.667 | 0.887 | 0.48 | 0.756 |
| + | 47 | 6 | |||||||||
| >38.5 y | − | 5 | 58 | 0.49 | <0.001 | 0.762 | 0.806 | 0.533 | 0.921 | 0.796 | |
| + | 16 | 14 | |||||||||
| Total | − | 18 | 70 | 0.56 | <0.001 | 0.778 | 0.778 | 0.759 | 0.795 | 0.778 | |
| + | 63 | 20 | |||||||||
| Diagnosis | Female | CSF-Tpro | CSF-Alb | CSF-IgG | Qalb | IgG Index |
|---|---|---|---|---|---|---|
| RRMS | Correlation coefficient | −0.218 | −0.248 | −0.115 | −0.201 | −0.16 |
| p | 0.051 | 0.026 | 0.306 | 0.072 | 0.155 | |
| NMOSD | Correlation coefficient | −0.27 | −0.275 | −0.132 | −0.253 | 0.057 |
| p | 0.01 | 0.009 | 0.217 | 0.016 | 0.593 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, B.; Tian, D.-S.; Bu, B.-T. A Comparison of IgG Index and Oligoclonal Band in the Cerebrospinal Fluid for Differentiating between RRMS and NMOSD. Brain Sci. 2022, 12, 69. https://doi.org/10.3390/brainsci12010069
Chen B, Tian D-S, Bu B-T. A Comparison of IgG Index and Oligoclonal Band in the Cerebrospinal Fluid for Differentiating between RRMS and NMOSD. Brain Sciences. 2022; 12(1):69. https://doi.org/10.3390/brainsci12010069
Chicago/Turabian StyleChen, Bo, Dai-Shi Tian, and Bi-Tao Bu. 2022. "A Comparison of IgG Index and Oligoclonal Band in the Cerebrospinal Fluid for Differentiating between RRMS and NMOSD" Brain Sciences 12, no. 1: 69. https://doi.org/10.3390/brainsci12010069
APA StyleChen, B., Tian, D.-S., & Bu, B.-T. (2022). A Comparison of IgG Index and Oligoclonal Band in the Cerebrospinal Fluid for Differentiating between RRMS and NMOSD. Brain Sciences, 12(1), 69. https://doi.org/10.3390/brainsci12010069