
Clinical Spectrum and Neuroimagistic Features in Hospitalized Patients with Neurological Disorders and Concomitant Coronavirus-19 Infection


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Clinical and Biochemical Evaluation
2.3. Radiologic Findings and Electrophysiological Studies of Nerve Conduction
2.4. Statistical Analyses
3. Results
3.1. Demographic Characteristics
3.2. Clinical Features
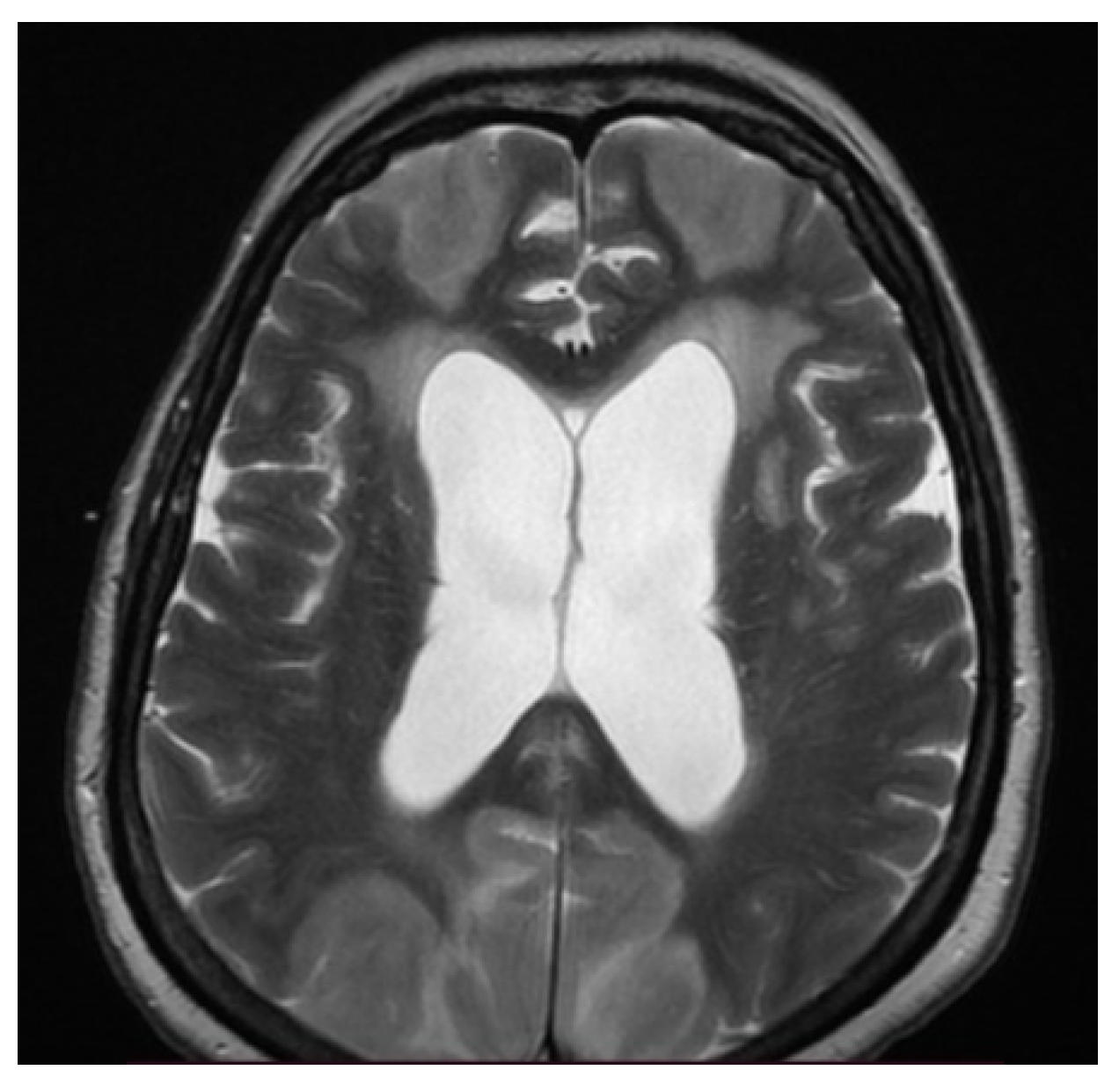
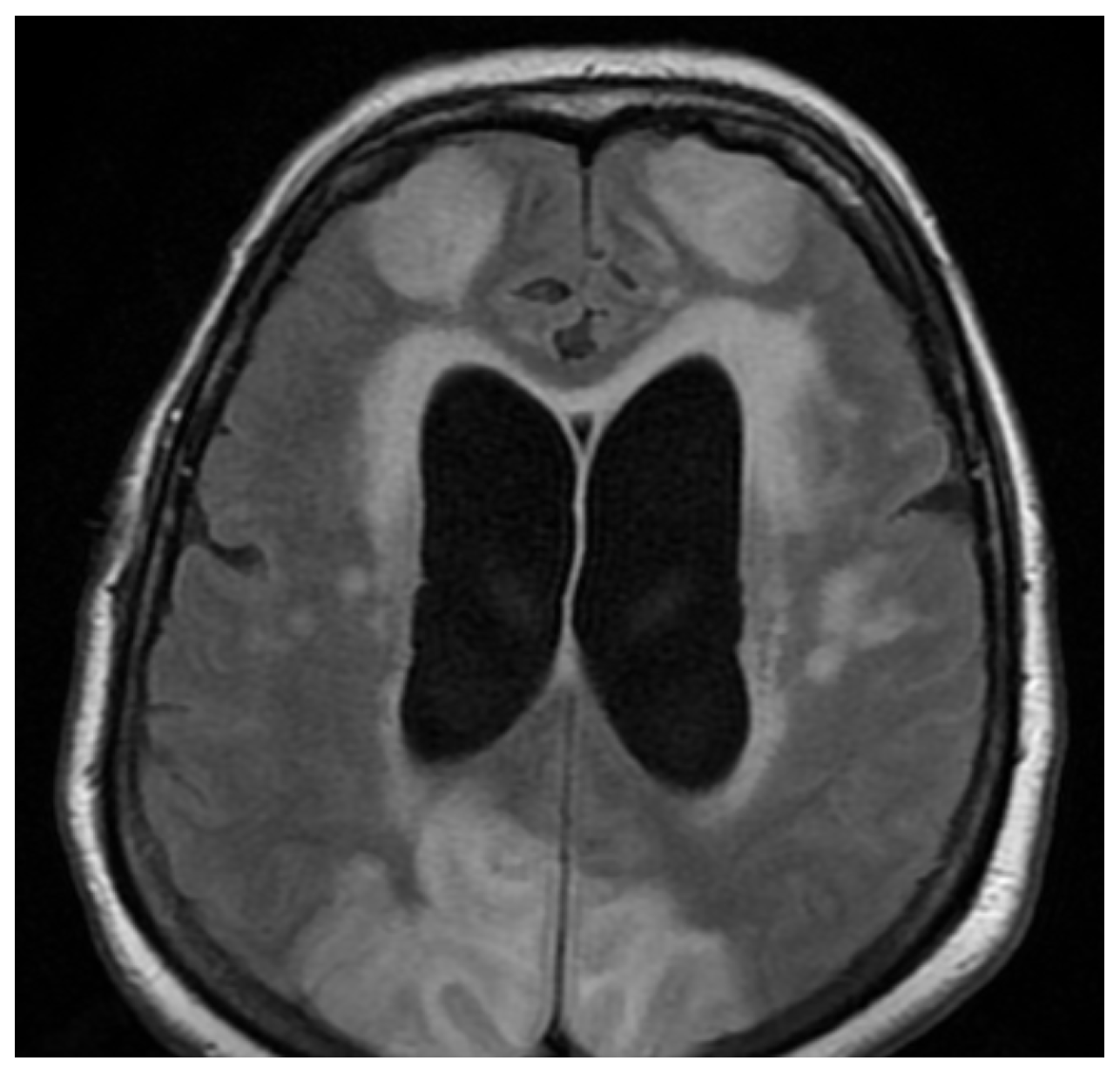
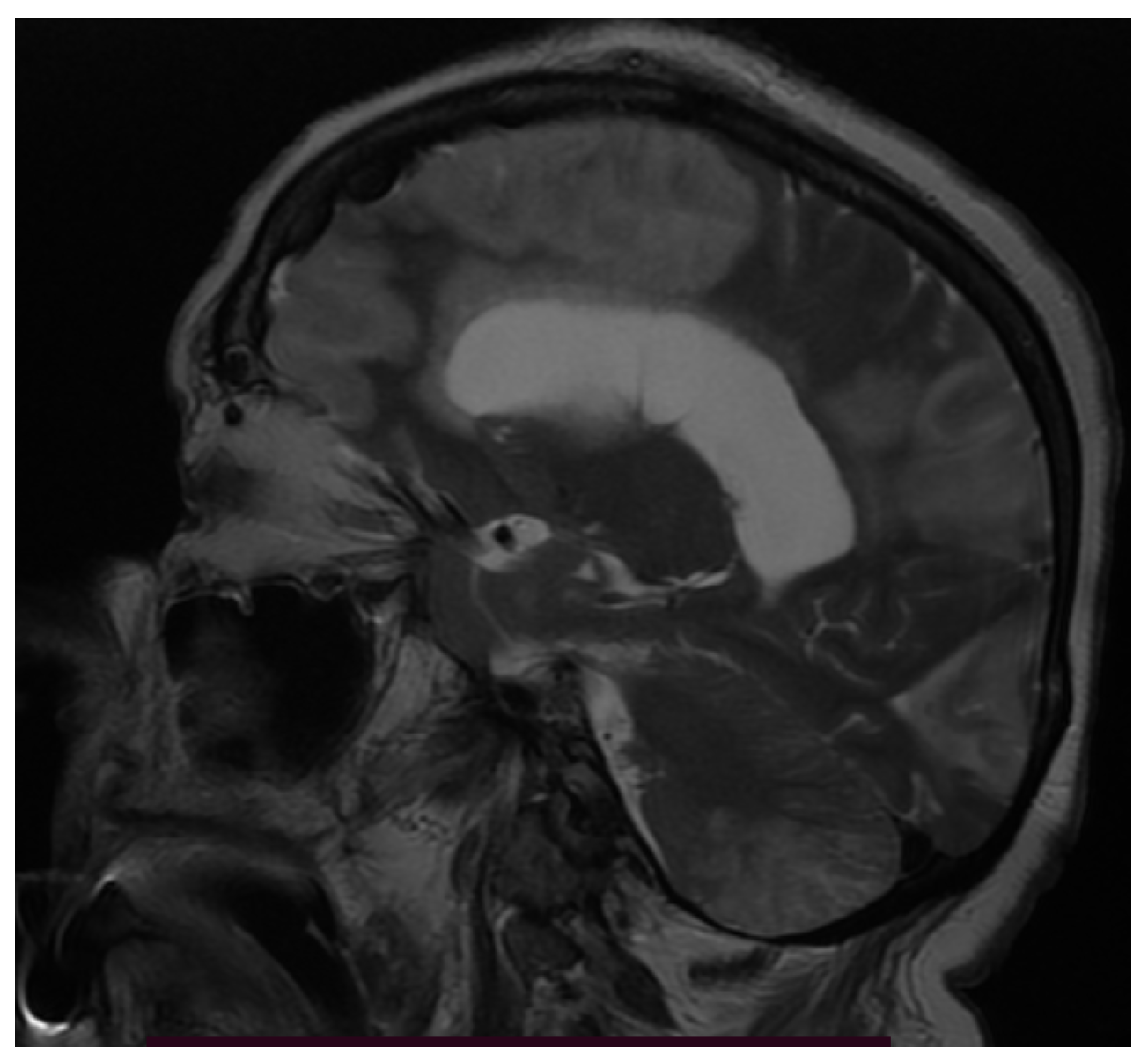
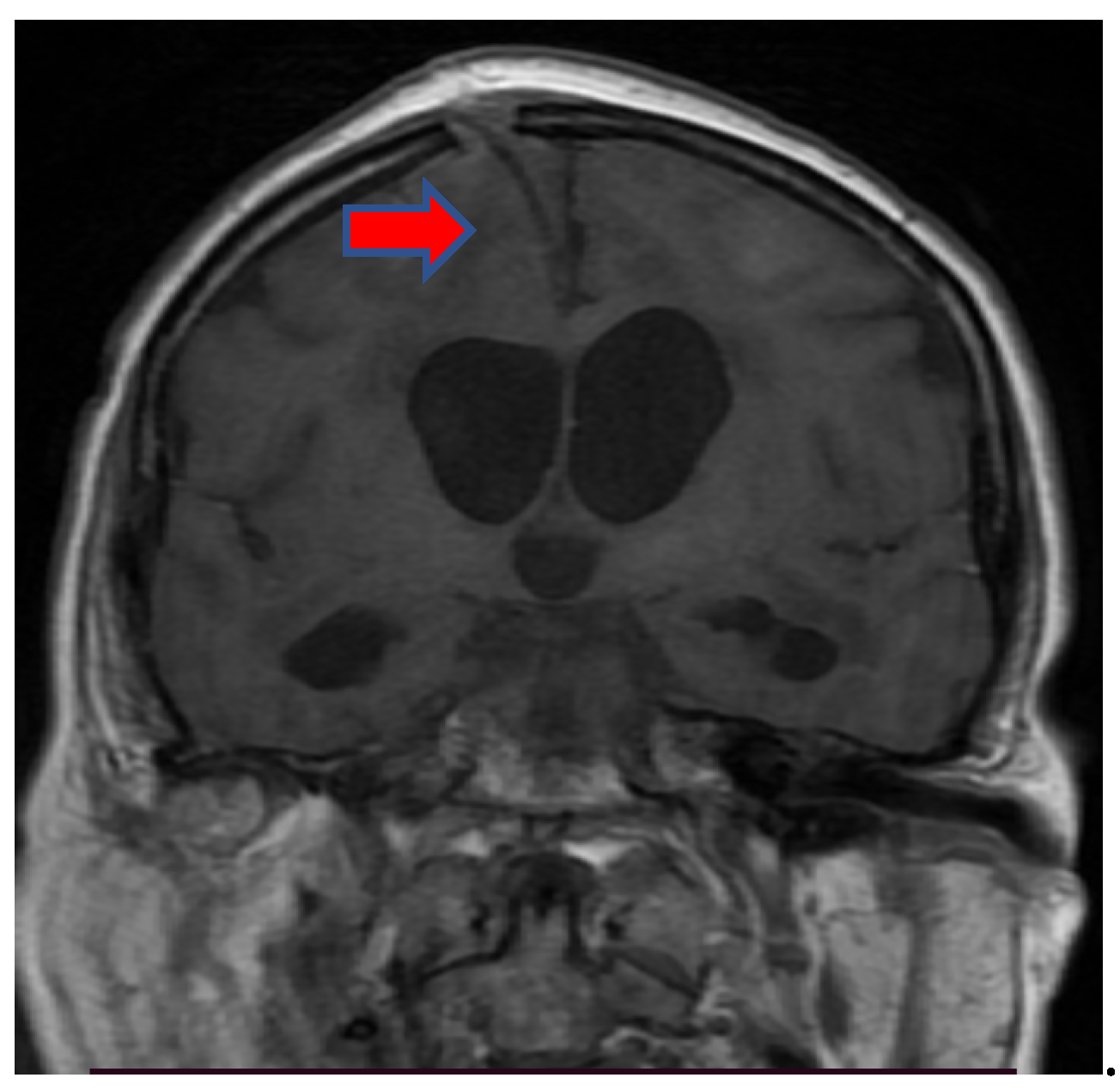
3.3. Neuroimaging
3.4. Biochemical Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharifian-Dorche, M.; Huot, P.; Osherov, M.; Wen, D.; Saveriano, A.; Giacomini, P.; Antel, J.P.; Mowla, A. Neurological complications of coronavirus infection; a comparative review and lessons learned during the COVID-19 pandemic. J. Sci. 2020, 417, 117085. [Google Scholar] [CrossRef]
- Troyer, E.A.; Kohn, J.N.; Hong, S. Are we facing a crashing wave of neuropsychiatric sequalae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav. Immun. 2020, 87, 34–39. [Google Scholar] [CrossRef]
- Martin, P.; Martin-Granel, E. 2500-year evolution of the term epidemic. Emerg. Infect. Dis. 2006, 12, 976–980. [Google Scholar] [CrossRef]
- Carlos, C.R.; Gerardo, M.M.; Jaime, O.G.; Isauro, G.H.L.; Dios, A.P.J.; Neurosurgical Group. Prevalence of neurological manifestations in COVID-19 and their association with mortality. Neurol. Perspect. 2021, 1, 11–16. [Google Scholar] [CrossRef]
- Carod-Artal, F.J. Complicaciones neurologicas por coronavirus y COVID-19. Rev. Neurol. 2020, 70, 311–322. [Google Scholar] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- To, K.F.; Lo, A.W. Exploring the pathogenesis of severe acute respiratory syndrome (SARS): The tissue distribution of the coronavirus (SARS-CoV) and putative receptor, angiotensin-converting enzyme 2 (ACE2). J. Pathol. 2004, 203, 740–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Wohlford- Lenane, C.; Perlman, S.; Zhao, J.; Jewell, A.K.; Reznicow, L.R.; Gibson-Corley, K.N.; Meyerholz, D.K.; McCray, P.B., Jr. Middle east respiratory syndrome coronaviruses causes multiple organ damage and lethal disease in mice transgenic for human dipeptidyl peptidase. J. Infect. Dis. 2016, 213, 712–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netland, J.; Meyerholz, D.K.; Moore, S.; Cassell, M.; Perlman, S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J. Virol. 2008, 82, 7264–7275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gogu, A.E.; Jianu, D.C.; Dumitrascu, V.; Ples, H.; Stroe, A.Z.; Axelerad, D.D.; Axelerad, A.D. MTHFR Gene Polymorphisms and Cardiovascular Risk Factors, Clinical-Imagistic Features and Outcome in Cerebral Venous Sinus Thrombosis. Brain Sci. 2020, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44, 27–72. [Google Scholar] [CrossRef]
- Gogu, A.E.; Motoc, A.G.; Stroe, Z.A.; Axelerad Docu, A.; Axelerad Docu, D.; Petrica, L.; Jianu, D.C. Plasminogen Activator Inhibitor-1 (PAI-1) gene polymorphisms associated with cardiovascular risk factors involved in cerebral venous sinus thrombosis. Metab. J. 2021, 22, 266. [Google Scholar]
- Jianu, D.C.; Jianu, S.N.; Motoc, A.G.; Poenaru, M.; Petrica, L.; Vlad, A.; Ursoniu, S.; Gogu, A.E.; Dan, F.T. Diagnosis and management of a young women with acute isolated sinus thrombosis. Rom. J. Morphol. Embryol. 2017, 58, 1515–1518. [Google Scholar] [PubMed]
- Gogu, A.E. New clinical-imagistic features in cerebral venous and sinus thrombosis. Elsevier Procedia Soc. Behav. Sci. 2015, 191, 1650–1659. [Google Scholar] [CrossRef] [Green Version]
- Vacchiano, V.; Riguzzi, P.; Volpi, L.; Tappata, M.; Avoni, P.; Rizzo, G.; Guerra, L.; Zaccaroni, S.; Cortelli, P.; Michelucci, R.; et al. Early neurological manifestations of hospitalized COVID-19 patients. Neurol. Sci. 2020, 41, 2029–2031. [Google Scholar] [CrossRef] [PubMed]
- Degeneffe, A.; Bruneau, M.; Spitaels, J.; Gilis, N.; De Witte, O.; Lubansu, A. Acute hemorrhage after intracerebral biopsy in COVID-19 patients: A report of 3 cases. World Neurosurg. 2020, 141, 157–161. [Google Scholar] [CrossRef]
- Gogu, A.E.; Scutelnicu, D.; Ignea, A. Relationships between low total serum cholesterol levels and intracerebral hemorrhage. J. Neurol. 2013, 260, 80. [Google Scholar]
- Gogu, A.E.; Scutelnicu, D. Cerebral venous and sinus thrombosis at young patients. Eur. J. Neurol. 2012, 19, 519. [Google Scholar]
- Speeckaert, M.M.; Speeckaert, R.; Delanghe, J.R. Potential underlying mechanisms of cerebral venous thrombosis associated with COVID-19. J. Neuroradiol. 2020, 47, 473–474. [Google Scholar] [CrossRef]
- Lantos, J.E.; Strauss, S.B.; Lin, E. COVID-19—Associated Miller Fisher Syndrome: MRI Findings. AJNR Am. J. Neuroradiol. 2020, 41, 1184–1186. [Google Scholar] [CrossRef]
- Pinna, P.; Grewal, P.; Hall, J.P.; Tavarez, T.; Dafer, R.M.; Garg, R.; Osteraas, N.D.; Pellack, D.R.; Asthana, A.; Fegan, K.; et al. Neurological manifestations and COVID-19. Experiences from a tertiary case center at the Frontline. J. Neurol. Sci. 2020, 415, 116969. [Google Scholar] [CrossRef] [PubMed]
- Gaddam, S. Implications of COVID-19 in Neurological Disorders. J. Neurol. Res. 2020, 10, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Romero-Sanchez, C.M.; Diaz-Maroto, I.; Fernandez-Diaz, E.; Sánchez-Larsen, Á.; Layos-Romero, A.; García-García, J.; González, E.; Redondo-Peñas, I.; Perona-Moratalla, A.B.; Valle-Pérez, J.A.D.; et al. Neurologic manifestations in hospitalized patients with COVID-19. Neurology 2020, 95, 1060–1070. [Google Scholar] [CrossRef]
- Virhammar, J.; Kumlien, E.; Falmar, D.; Frithiof, R.; Jackmann, S.; Sköld, M.K.; Kadir, M.; Frick, J.; Lindeberg, J.; Olivero-Reinius, H.; et al. Acute necrotizing encephalopathy with SARS-CoV-2 RNA confirmed in cerebrospinal fluid. Neurology 2020, 95, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Radmanesh, A.; Derman, A.; Ishida, K. COVID-19 associated delayed posthypoxic necrotizing leukoencephalopathy. J. Neurol. Sci. 2020, 415, 116945. [Google Scholar] [CrossRef] [PubMed]
- Bolay, H.; Gull, A.; Baykan, B. COVID-19 is a real headache! Headache 2020, 60, 1415–1421. [Google Scholar] [CrossRef]
- Mao, L.; Jin, M.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of coronavirus disease (COVID-19): A multicentric European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Jose, J.R.; Manuel, A. COVID-19 cytokine storm: The interplay between inflammation and coagulation. Lancet Respir. Med. 2020, 8, 46–47. [Google Scholar] [CrossRef]
- Kubota, T.; Kuroda, N. Exacerbation of neurological symptoms and COVID-19 severity in patients with preexisting neuro-logical disorders and COVID-19: A systematic review. Clin. Neurol. Neurosurg. 2021, 200, 106349. [Google Scholar] [CrossRef] [PubMed]
- Kochi, A.N.; Tagliari, A.P.; Forleo, G.B.; Fassini, G.M.; Tondo, C. Cardiac and arrhythmic complications in patients with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 1003–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, D.C.; Eldahshan, W.; Rutkowski, E. COVID-19 related stroke. Transl. Stroke Res. J. 2020, 11, 322–325. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 101) | Non-Severe Group (n = 75) | Severe Group (n = 26) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| No | Variable | Mean ± Std = Deviation | Mean ± Std = Deviation | Mean Rank | Mean ± Std = Deviation | Mean Rank | |
| (Median) | (Median) | (Median) | |||||
| 1 | Age, years | 70.05 ± 11.21 | 69.13 ± 11.64 | 67.76 | 72.69 ± 9.55 | 74.04 | p < 0.05 * |
| 2 | Male, n (%) | 63 (62.37%) | 49 (65.33%) | 39.24 | 14 (53.84%) | 23.74 | p < 0.05 * |
| 3 | Female, n (%) | 38 (37.63%) | 26 (34.67%) | 21.89 | 12 (46.15%) | 16.1 | p < 0.05 * |
| Symptoms | |||||||
| 4 | Fever, n (%) | 70 (69.30%) | 46 (61.33%) | 39.38 | 24 (92.30%) | 30.6 | p < 0.05 * |
| 5 | Dyspnea, n (%) | 75 (74.25) | 51 (68%) | 43.05 | 24 (92.30%) | 31.93 | p < 0.05 * |
| 6 | Fatigue, n (%) | 62 (61.38%) | 40 (53.33%) | 34.51 | 22 (84.61%) | 27.47 | p < 0.05 * |
| Blood test parameters | |||||||
| 7 | Leucocyte count (×1000/L) | 12.85 ± 7.7 | 13 ± 8.27 | 12.45 | 12.42 ± 5.88 | 12.96 | 0.639 |
| 8 | Lymphocyte count (×1000/L) | 2.45 ± 5.41 | 2.78 ± 6.21 | 2.39 | 1.5 ± 1.23 | 1.88 | 0.288 |
| 9 | Thrombocyte count (×1000/L) | 233.53 ± 114.33 | 235.35 ± 118.54 | 226.21 | 228.26 ± 103.25 | 237.35 | 0.053 |
| 10 | Blood glucose, mg/dL | 148.05 ± 88.01 | 136.67 ± 61.66 | 142.67 | 180.88 ± 134.99 | 174.84 | p < 0.05 * |
| 11 | LDH (U/L) | 438.95 ± 482.33 | 356.11 ± 290.39 | 420.13 | 677.92 ± 775.23 | 613.8 | p < 0.05 * |
| 12 | hsCRP, mg/L | 87.88 ± 93.21 | 77.98 ± 95.4 | 84.61 | 116.42 ± 81.69 | 110.26 | p < 0.05 * |
| 13 | VSH, mm/1 h | 39.81 ± 19.8 | 35.76 ± 16.67 | 38.3 | 51.5 ± 23.55 | 48.94 | p < 0.05 * |
| 14 | D-dimer, ng/mL | 1252.09 ± 2115.51 | 1206.4 ± 2250.4 | 1185.98 | 1383.88 ± 1699.08 | 1303.1 | p < 0.05 * |
| 15 | Fibrinogen, mg/dL | 535.02 ± 189.41 | 521.4 ± 178.94 | 517.22 | 574.31 ± 215.78 | 578.39 | p < 0.05 * |
| 16 | APTT (s) | 28.04 ± 7.09 | 27.62 ± 5.25 | 27.12 | 29.24 ± 10.83 | 29.73 | 0.471 |
| 17 | PT (s) | 15.13 ± 17.79 | 13.17 ± 2.84 | 14.53 | 20.8 ± 34.59 | 19.42 | 0.08 |
| 18 | INR | 1.49 ± 1.62 | 1.28 ± 0.28 | 1.53 | 2.53 ± 3.69 | 2.27 | 0.421 |
| Chest CT findings (pneumonia) | |||||||
| 19 | Unilateral, n (%) | 33 (32.67%) | 27 (36%) | 21.22 | 6 (23.07%) | 11.77 | p < 0.05 * |
| 20 | Bilateral, n (%) | 52 (51.48%) | 32 (42.66%) | 28.17 | 20 (76.92%) | 23.82 | p < 0.05 * |
| 21 | OTI at admission, n (%) | 6 (5.94%) | 2 (2.66%) | 2.4 | 4 (15.38%) | 3.59 | 0.34 |
| 22 | Mortality, n (%) | 28 (27.72%) | 16 (21.33%) | 14.55 | 12 (46.15%) | 13.44 | 0.213 |
| No | Variable | Total, n = 101 | Non-Severe, n = 75 (74.25%) | Severe, n = 26 (25.75%) | p-Value |
|---|---|---|---|---|---|
| Nonspecific symptoms | |||||
| 1 | Headaches | 73 (72.27%) | 55 (73.33%) | 18 (69.23%) | 0.24 |
| 2 | Dizziness | 15 (14.85%) | 9 (12%) | 6 (23.07%) | 0.35 |
| Cerebrovascular events | |||||
| 3 | Ischemic stroke | 51 (50.49%) | 36 (48%) | 15 (57.69%) | p < 0.05 * |
| 4 | Cerebral hemorrhage | 5 (4.95%) | 2 (2.66%) | 3 (11.53%) | 0.08 |
| 5 | Cerebral venous sinus thrombosis | 2 (1.98%) | 1 (1.33%) | 1 (3.84%) | 0.29 |
| Inflammatory manifestations | |||||
| 6 | Encephalitis | 2 (1.98%) | 0 | 2 (7.69%) | 0.46 |
| 7 | Guillain–Barré Syndrome | 2 (1.98%) | 0 | 2 (7.69%) | 0.46 |
| 8 | Seizures | 13 (12.87%) | 10 (13.33%) | 3 (11.53%) | p < 0.05 * |
| Cranial nerve abnormalities | |||||
| 9 | Anosmia | 31 (30.69%) | 24 (32%) | 7 (26.92%) | p < 0.05 * |
| 10 | Dysgeusia/ageusia | 47 (46.53%) | 36 (48%) | 11 (42.30%) | p < 0.05 * |
| 11 | Impaired eye movement | 1 (0.99%) | 1 (1.33%) | 0 | NA |
| 12 | Facial nerve palsy | 2 (1.98%) | 2 (2.66%) | 0 | 0.38 |
| Depressed level of consciousness | |||||
| 13 | Acute confusional syndrome | 25 (24.75%) | 20 (26.66%) | 5 (19.23%) | 0.57 |
| 14 | Coma | 7 (6.93%) | 0 | 7 (26.92%) | p < 0.05 * |
| Neuropsychiatric symptoms | |||||
| 15 | Anxiety | 24 (23.76%) | 18 (24%) | 6 (23.07%) | 0.22 |
| 16 | Depression | 15 (14.85%) | 11 (14.66%) | 4 (15.38%) | 0.33 |
| Neurological comorbidities | |||||
| 17 | Prior stroke | 8 (7.92%) | 5 (6.66%) | 3 (11.53%) | 0.06 |
| 18 | Myasthenia Gravis | 3 (2.97%) | 0 | 3 (11.53%) | p < 0.05 * |
| 19 | Parkinson’s Disease | 2 (1.98%) | 0 | 2 (7.69%) | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gogu, A.E.; Motoc, A.G.; Stroe, A.Z.; Docu Axelerad, A.; Docu Axelerad, D.; Pârv, F.; Munteanu, G.; Dan, F.; Jianu, D.C. Clinical Spectrum and Neuroimagistic Features in Hospitalized Patients with Neurological Disorders and Concomitant Coronavirus-19 Infection. Brain Sci. 2021, 11, 1138. https://doi.org/10.3390/brainsci11091138
Gogu AE, Motoc AG, Stroe AZ, Docu Axelerad A, Docu Axelerad D, Pârv F, Munteanu G, Dan F, Jianu DC. Clinical Spectrum and Neuroimagistic Features in Hospitalized Patients with Neurological Disorders and Concomitant Coronavirus-19 Infection. Brain Sciences. 2021; 11(9):1138. https://doi.org/10.3390/brainsci11091138
Chicago/Turabian StyleGogu, Anca Elena, Andrei Gheorghe Motoc, Alina Zorina Stroe, Any Docu Axelerad, Daniel Docu Axelerad, Florina Pârv, Georgiana Munteanu, Flavius Dan, and Dragos Catalin Jianu. 2021. "Clinical Spectrum and Neuroimagistic Features in Hospitalized Patients with Neurological Disorders and Concomitant Coronavirus-19 Infection" Brain Sciences 11, no. 9: 1138. https://doi.org/10.3390/brainsci11091138
APA StyleGogu, A. E., Motoc, A. G., Stroe, A. Z., Docu Axelerad, A., Docu Axelerad, D., Pârv, F., Munteanu, G., Dan, F., & Jianu, D. C. (2021). Clinical Spectrum and Neuroimagistic Features in Hospitalized Patients with Neurological Disorders and Concomitant Coronavirus-19 Infection. Brain Sciences, 11(9), 1138. https://doi.org/10.3390/brainsci11091138