
Mindful Coping Power: Comparative Effects on Children’s Reactive Aggression and Self-Regulation

Abstract
1. Introduction
1.1. Reactive Aggression
1.2. Active Mechanisms of Reactive Aggression
1.3. Rationale for Mindful Coping Power
1.4. Current Study
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analyses
3. Results
3.1. Child Self-Report Outcomes
3.2. Parent-Report Outcomes
3.3. Teacher-Report Outcomes
3.4. Implementation Fidelity and Quality
3.5. School and Leader Effects
3.6. Feasibility and Participant Satisfaction
4. Discussion
4.1. Child Self-Report Findings
4.2. Parent-Report Findings
4.3. Teacher-Report Findings
4.4. Implementation Findings
4.5. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powell, N.P.; Lochman, J.E.; Boxmeyer, C.L.; Barry, T.D.; Pardini, D.A. The Coping Power Program for aggressive behavior in children. In Evidence-Based Psychotherapies for Children and Adolescents, 3rd ed.; Weisz, J.R., Kazdin, A.E., Eds.; Guilford Press: New York, NY, USA, 2017; pp. 159–176. Available online: https://psycnet.apa.org/record/2017-25888-010 (accessed on 1 June 2021).
- Lochman, J.E.; Wells, K.C. Contextual social-cognitive mediators and child outcome: A test of the theoretical model in the Coping Power Program. Dev. Psychopathol. 2002, 14, 971–993. [Google Scholar] [CrossRef]
- Zonnevylle-Bender, M.J.; Matthys, W.; van de Wiel, N.M.; Lochman, J.E. Preventive effects of treatment of disruptive behavior disorder in middle childhood on substance use and delinquent behavior. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Lochman, J.E.; Baden, R.E.; Boxmeyer, C.L.; Powell, N.P.; Qu, L.; Salekin, K.L.; Windle, M. Does a booster intervention augment the preventive effects of an abbreviated version of the Coping Power Program for aggressive children? J. Abnorm. Child Psychol. 2014, 42, 367–381. [Google Scholar] [CrossRef][Green Version]
- Lochman, J.E.; Wells, K.C. The Coping Power Program at the middle school transition: Universal and indicated prevention effects. Psychol. Addict. Behav. 2002, 16, S40–S54. [Google Scholar] [CrossRef]
- Mushtaq, A.; Lochman, J.E.; Tariq, P.N.; Sabih, F. Preliminary effectiveness study of Coping Power program for aggressive children in Pakistan. Prev. Sci. 2017, 18, 762–771. [Google Scholar] [CrossRef]
- Fite, P.J.; Colder, C.R.; Lochman, J.E.; Wells, K.C. Pathways from proactive and reactive aggression to substance use. Psychol. Addict. Behav. 2007, 21, 355–364. [Google Scholar] [CrossRef]
- Dodge, K.A.; Coie, J.D. Social-information-processing factors in reactive and proactive aggression in children’s peer groups. J. Personal. Soc. Psychol. 1987, 53, 1146–1158. [Google Scholar] [CrossRef]
- Fite, P.J.; Colder, C.; Pelham, W. A factor analytic approach to distinguish pure and co-occurring dimensions of proactive and reactive aggression. J. Clin. Child Adolesc. Psychol. 2006, 35, 578–582. [Google Scholar] [CrossRef]
- Bezdjian, S.; Raine, A.; Baker, L.A.; Lyman, D.R. Psychopathic personality in children: Genetic and environmental contributions. Psychol. Med. 2011, 41, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, J.A.; Smithmyer, C.M.; Ramsden, S.R.; Parker, E.H.; Flanagan, K.D.; Dearing, K.F.; Simons, R.F. Observational, physiological, and self–report measures of children’s anger: Relations to reactive versus proactive aggression. Child Dev. 2002, 73, 1101–1118. [Google Scholar] [PubMed]
- Bierman, K.L.; Coie, J.; Dodge, K.; Greenberg, M.; Lochman, J.; McMahon, R.; Pinderhughes, E.; CPPRG. School outcomes of aggressive-disruptive children: Prediction from kindergarten risk factors and impact of the fast track prevention program. Aggress. Behav. 2013, 39, 114–130. [Google Scholar] [CrossRef]
- Ellis, M.L.; Weiss, B.; Lochman, J.E. Executive functions in children: Associations with aggressive behavior and appraisal processing. J. Abnorm. Child Psychol. 2009, 37, 945–956. [Google Scholar] [CrossRef]
- Fite, P.J.; Raine, A.; Stouthamer-Loeber, M.; Loeber, R.; Pardini, D.A. Reactive and proactive aggression in adolescent males: Examining differential outcomes 10 years later in early adulthood. Crim. Justice Behav. 2009, 37, 141–157. [Google Scholar] [CrossRef]
- Acton, G.S. Measurement of impulsivity in a hierarchical model of personality traits: Implications for substance use. Subst. Use Misuse 2003, 38, 67–83. [Google Scholar] [CrossRef]
- Moeller, F.G.; Dougherty, D.M. Impulsivity and substance abuse: What is the connection? Addict. Disord. Treat. 2002, 1, 3–10. [Google Scholar] [CrossRef]
- Pardini, D.; Lochman, J.; Wells, K. Negative emotions and alcohol use initiation in high-risk boys: The moderating effect of good inhibitory control. J. Abnorm. Child Psychol. 2004, 32, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Marsee, M.A.; Frick, P.J. Exploring the cognitive and emotional correlates to proactive and reactive aggression in a sample of detained girls. J. Abnorm. Child Psychol. 2007, 35, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Barry, T.D.; Thompson, A.; Barry, C.T.; Lochman, J.E.; Adler, K.; Hill, K. The importance of narcissism is predicting proactive and reactive aggression in moderately to highly aggressive children. Aggress. Behav. 2007, 33, 185–197. [Google Scholar] [CrossRef]
- Eisenberg, N.; Fabes, R.A.; Nyman, M.; Bernzweig, J.; Pinuelas, A. The relations of emotionality and regulation to children’s anger-related reactions. Child Dev. 1994, 65, 109–128. [Google Scholar] [CrossRef] [PubMed]
- Cummings, E.M.; Iannotti, R.J.; Zahn-Waxler, C. Influence of conflict between adults on the emotions and aggression of young children. Dev. Psychol. 1985, 21, 495–507. [Google Scholar] [CrossRef]
- Vitaro, F.; Brendgen, M.; Tremblay, R.E. Reactively and proactively aggressive children: Antecedent and subsequent characteristics. J. Child Psychol. Psychiatry 2002, 43, 495–506. [Google Scholar] [CrossRef]
- Dodge, K.A. The structure and function of reactive and proactive aggression. In The Development and Treatment of Childhood Aggression; Pepler, D.J., Rubin, K.H., Eds.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1991; pp. 201–218. [Google Scholar]
- Murray, A.L.; Obsuth, I.; Zirk-Sadowsklli, J.; Ribeaud, D.; Eisner, M. Developmental relations between ADHD symptoms and reactive versus proactive aggression across childhood and adolescence. J. Atten. Disord. 2016, 10, 1701–1710. [Google Scholar] [CrossRef] [PubMed]
- De Castro, B.O.; Merk, W.; Koops, W.; Veerman, J.W.; Bosch, J.D. Emotions in social information processing and their relations with reactive and proactive aggression in referred aggressive boys. J. Clin. Child Adolesc. Psychol. 2005, 34, 105–116. [Google Scholar] [CrossRef]
- White, B.A.; Turner, K.A. Anger rumination and effortful control: Mediation effects on reactive but not proactive aggression. Personal. Individ. Differ. 2014, 56, 186–189. [Google Scholar] [CrossRef]
- Denson, T.F.; De Wall, C.N.; Finkel, E.J. Self-control and aggression. Curr. Dir. Psychol. Sci. 2012, 21, 20–25. [Google Scholar] [CrossRef]
- Rohlf, H.L.; Holl, A.K.; Kirsch, F.; Krahé, B.; Elsner, B. Longitudinal links between executive function, anger, and aggression in middle childhood. Front. Behav. Neurosci. 2018, 12, 27. [Google Scholar] [CrossRef] [PubMed]
- Dodge, K.A.; Lochman, J.E.; Harnish, J.D.; Bates, J.E.; Pettit, G.S. Reactive and proactive aggression in school children and psychiatrically impaired chronically assaultive youth. J. Abnorm. Psychol. 1997, 106, 37–51. [Google Scholar] [CrossRef]
- Schippel, P.L.; Vasey, M.W.; Cravens-Brown, L.M.; Bretveld, R.A. Suppressed attention to rejecction, ridicule, and failure cues: A unique correlate of reactive but not proactive aggression in youth. J. Clin. Child Adolesc. Psychol. 2003, 32, 40–55. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Jha, A.P.; Stanley, E.A.; Kiyonaga, A.; Wong, L.; Gelfand, L. Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion 2010, 10, 54–64. [Google Scholar] [CrossRef]
- Tang, Y.; Ma, Y.; Wang, J.; Fan, Y.; Feng, S.; Lu, Q.; Posner, M.I. Short-term meditation training improves attention and self-regulation. Proc. Natl. Acad. Sci. USA 2007, 104, 17152–17156. [Google Scholar] [CrossRef]
- Metz, S.M.; Frank, J.L.; Reibel, D.; Cantrell, T.; Sanders, R.; Broderick, P.C. The effectiveness of the Learning to BREATHE Program on adolescent emotion regulation. Res. Hum. Dev. 2013, 10, 252–272. [Google Scholar] [CrossRef]
- Holzel, B.K.; Carmody, J.; Vangel, M.; Congleton, C.; Yerramsetti, S.M.; Lazar, S.W. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. 2011, 191, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.Y.; Tang, R.; Posner, M. Mindfulness meditation improves emotion regulation and reduces drug abuse. Drug Alcohol Depend. 2016, 163, 13–18. [Google Scholar] [CrossRef]
- Mendelson, T.; Greenberg, M.T.; Dariotis, J.K.; Gould, L.F.; Rhoades, B.L.; Leaf, P.J. Feasibility and preliminary outcomes of a school-based mindfulness intervention for urban youth. J. Abnorm. Child Psychol. 2010, 38, 985–994. [Google Scholar] [CrossRef]
- Franco, C.; Amutio, A.; López-González, L.; Oriol, X.; Martínez-Taboada, C. Effect of a mindfulness training program on the impulsivity and aggression levels of adolescents with behavioral problems in the classroom. Front. Psychol. 2016, 7, 1385. [Google Scholar] [CrossRef] [PubMed]
- Schonert-Reichl, K.A.; Oberle, E.; Lawlor, M.S.; Abbott, D.; Thomson, K.; Oberlander, T.F.; Diamond, A. Enhancing cognitive and social-emotional development through simple-to-administer mindfulness-based school program for elementary school children: A randomized controlled trial. Dev. Psychol. 2015, 51, 52–66. [Google Scholar] [CrossRef]
- Singh, N.N.; Singh, A.N.; Lancioni, G.E.; Singh, J.; Winton, A.S.W.; Adkins, A.D. Mindfulness training for parents and their children with ADHD increases the children’s compliance. J. Child Fam. Stud. 2010, 19, 157–166. [Google Scholar] [CrossRef]
- van der Oord, S.; Bögels, S.M.; Peijnenburg, D. The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. J. Child Fam. Stud. 2012, 21, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Muratori, P.; Conversano, C.; Levantini, V.; Masi, G.; Milone, A.; Villani, S.; Bögels, S.; Gemignani, A. Exploring the Efficacy of a Mindfulness Program for Boys with Attention-Deficit Hyperactivity Disorder and Oppositional Defiant Disorder. J. Atten. Disord. 2020, 25, 1544–1553. [Google Scholar] [CrossRef]
- Bögels, S.; Hoogstad, B.; van Dun, L.; de Schutter, S.; Restifo, K. Mindfulness training for adolescents with externalizing disorders and their parents. Behav. Cogn. Psychother. 2008, 36, 193–209. [Google Scholar] [CrossRef]
- Sibinga, E.; Perry-Parrish, C.; Chung, S.E.; Johnson, S.B.; Smith, M.; Ellen, J.M. School-based mindfulness instruction for urban male youth: A small randomized controlled trial. Prev. Med. 2013, 57, 799–801. [Google Scholar] [CrossRef]
- Keune, P.M.; Bostanov, V.; Kotchoubey, B.; Hautzinger, M. Mindfulness versus rumination and behavioral inhibition: A perspective from research on frontal brain asymmetry. Personal. Individ. Differ. 2012, 53, 323–328. [Google Scholar] [CrossRef]
- Evans, D.R.; Segerstrom, S.C. Why do mindful people worry less? Cogn. Ther. Res. 2010, 35, 505–510. [Google Scholar] [CrossRef]
- Moore, A.; Malinowski, P. Meditation, mindfulness and cognitive flexibility. Conscious. Cogn. 2009, 18, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.; Krompinger, J.; Baine, M.J. Mindfulness training modifies subsystems of attention. Cogn. Affect. Behav. Neurosci. 2007, 7, 109–119. [Google Scholar] [CrossRef] [PubMed]
- MacLean, K.A.; Ferrer, E.; Aichele, S.R.; Bridwell, D.A.; Zanesco, A.P.; Jacobs, T.L.; Saron, C.D. Intensive meditation training improves perceptual discrimination and sustained attention. Psychol. Sci. 2010, 21, 829–839. [Google Scholar] [CrossRef]
- Moore, A.; Gruber, T.; Derose, J.; Malinowski, P. Regular, brief mindfulness meditation practice improves electrophysiological markers of attentional control. Front. Hum. Neurosci. 2012, 6, 18. [Google Scholar] [CrossRef]
- Creswell, J.D.; Taren, A.A.; Lindsay, E.K.; Greco, C.M.; Gianaros, P.J.; Fairgrieve, A.; Marsland, A.L.; Brown, K.W.; Way, B.M.; Rosen, R.K.; et al. Alterations in resting-state functional connectivity link mindfulness meditation with reduced Interleukin-6: A randomized controlled trial. Biol. Psychiatry 2016, 80, 53–61. [Google Scholar] [CrossRef]
- Crane, R.S.; Kuyken, W.; Williams, J.M.G.; Hastings, R.P.; Cooper, L.; Fennell, M.J. Competence in teaching mindfulness-based courses: Concepts, development and assessment. Mindfulness 2012, 3, 76–84. [Google Scholar] [CrossRef]
- Emerson, L.; de Diaz, N.N.; Sherwood, A.; Waters, A.; Farrell, L. Mindfulness interventions in schools: Integrity and feasibility of implementation. Int. J. Behav. Dev. 2020, 44, 62–75. [Google Scholar] [CrossRef]
- Greenberg, M.T.; Harris, A.R. Nurturing mindfulness in children and youth: Current state of research. Child Dev. Perspect. 2012, 6, 161–166. [Google Scholar] [CrossRef]
- McKeering, P.; Hwang, Y.S. A systematic review of mindfulness-based school interventions with early adolescents. Mindfulness 2019, 10, 593–610. [Google Scholar] [CrossRef]
- Zenner, C.; Herrnleben-Kurz, S.; Walach, H. Mindfulness-based interventions in schools—A systematic review and meta-analysis. Front. Psychol. 2014, 5, 603–623. [Google Scholar] [CrossRef] [PubMed]
- Shegog, R.; Markham, C.M.; Peskin, M.F.; Johnson, K.; Cuccaro, P.; Tortolero, S.R. It’s Your Game. Keep It Real: Can innovative public health prevention research thrive within a comparative effectiveness research framework? J. Prim. Prev. 2013, 34, 89–108. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Johnston, L.D.; O’Malley, P.M.; Bachman, J.G.; Schulenberg, J.E. Monitoring the Future: National Survey Results on Drug Use; Institute for Social Research: Ann Arbor, MI, USA, 2011; pp. 1975–2010. [Google Scholar]
- Reynolds, C.R.; Kamphaus, R.W. Behavior Assessment System for Children; American Guidance Service: Circle Pines, MN, USA, 1992. [Google Scholar]
- Lochman, J.E.; Wells, K.C. Effectiveness study of Coping Power and classroom intervention with aggressive children: Outcomes at a one-year follow-up. Behav. Ther. 2003, 34, 493–515. [Google Scholar] [CrossRef]
- Lochman, J.E.; Wells, K.C. The coping power program for preadolescent aggressive boys and their parents: Outcome effects at the 1-year follow-up. J. Consult. Clin. Psychol. 2004, 72, 571–578. [Google Scholar] [CrossRef]
- Miller, S.; Boxmeyer, C.; Romero, D.E.; Powell, N.; Jones, S.; Lochman, J.E. Theoretical model of Mindful Coping Power: Optimizing a cognitive behavioral program for high risk children and their parents by integrating mindfulness. Clin. Child Fam. Psychol. Rev. 2020, 23, 393–406. [Google Scholar] [CrossRef]
- Mezzich, A.C.; Tarter, R.E.; Giancola, P.R.; Lu, S.; Kirisci, L.; Parks, S. Substance use and risky sexual behavior in female adolescents. Drug Alcohol Depend. 1997, 44, 157–166. [Google Scholar] [CrossRef]
- Capaldi, D.M.; Rothbart, M.K. Development and validation of an early adolescent temperament measure. J. Early Adolesc. 1992, 12, 153–173. [Google Scholar] [CrossRef]
- Ellis, L.K.; Rothbart, M.K. Revision of the Early Adolescent Temperament Questionnaire. In Proceedings of the 2001 Biennial Meeting of the Society for Research in Child Development, Minneapolis, MI, USA, 2001; Available online: https://research.bowdoin.edu/rothbart-temperament-questionnaires/files/2016/09/lesa-ellis-srcd-poster-reprint.pdf (accessed on 1 June 2018).
- Price, C.J.; Thompson, E.A.; Cheng, S.C. Scale of Body Connection: A multi-sample construct validation study. PLoS ONE 2017, 12, e0184757. [Google Scholar] [CrossRef]
- Coman, E.N.; Picho, K.; McArdle, J.J.; Villagra, V.; Dierker, L.; Iordache, E. The paired t-test as a simple latent change score model. Front. Psychol. 2013, 4, 738. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/ (accessed on 15 June 2018).
- Enders, C.K. Applied Missing Data Analysis; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Mezzich, A.C.; Tarter, R.E.; Giancola, P.R.; Kirisci, L. The Dysregulation Inventory: A new scale to assess the risk for substance use disorder. J. Child Adolesc. Subst. Abus. 2001, 10, 35–43. [Google Scholar] [CrossRef]
- Melnychuk, M.C.; Dockree, P.M.; O’Connell, R.G.; Murphy, P.R.; Balsters, J.H.; Robertson, I.H. Coupling of respiration and attention via the locus coeruleus: Effects of meditation and pranayama. Psychophysiology 2018, 55, e13091. [Google Scholar] [CrossRef] [PubMed]
- Lochman, J.E.; Boxmeyer, C.L.; Jones, S.; Qu, L.; Ewoldsen, D.; Nelson, W.M., III. Testing the feasibility of a briefer school-based preventive intervention with aggressive children: A hybrid intervention with face-to-face and internet components. J. Sch. Psychol. 2017, 62, 33–50. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic variable | Overall Sample (n = 102) | MCP Condition (n = 52) | CP Condition (n = 50) |
|---|---|---|---|
| M (SD) | M (SD) | M (SD) | |
| Child age | 9.97 (0.48) | 10 (0.49) | 9.94 (0.47) |
| Child 4th grade reactive aggression | 11.18 (2.37) | 11.17 (2.39) | 11.18 (2.37) |
| n (%) | n (%) | n (%) | |
| Child gender | |||
| Male | 62 (60.8%) | 33 (63.5%) | 29 (58.0%) |
| Female | 40 (39.2%) | 19 (36.5%) | 21 (42.0%) |
| Child ethnicity | |||
| Hispanic or Latino | 3 (2.9%) | 1 (1.9%) | 2 (4.0%) |
| Not Hispanic or Latino | 92 (90.2%) | 47 (90.4%) | 45 (90.0%) |
| Unknown or not reported | 7 (6.9%) | 4 (7.7%) | 3 (6.0%) |
| Child race | |||
| Black or African American | 89 (87.3%) | 47 (90.4%) | 42 (84.0%) |
| White or Caucasian | 6 (5.9%) | 2 (3.8%) | 4 (8.0%) |
| More than one race | 4 (3.9%) | 1 (1.9%) | 3 (6.0%) |
| Unknown or not reported | 3 (2.9%) | 2 (3.8%) | 1 (2.0%) |
| Child repeated grade | 18 (17.5%) | 9 (17.3%) | 9 (18.0%) |
| Caregiver relation to child | |||
| Biological parent | 85 (82.5%) | 44 (84.6%) | 41 (82%) |
| Adoptive parent | 5 (4.9%) | 3 (5.8%) | 2 (3.8%) |
| Grandparent | 7 (6.8%) | 2 (3.8%) | 5 (10%) |
| Other | 5 (4.9%) | 3 (5.8%) | 2 (3.8%) |
| Annual family income | |||
| Less than USD 15,000 | 34 (33.4%) | 17 (32.7%) | 17 (34.0%) |
| USD 15,000 to <29,999 | 30 (29.4%) | 13 (25.0%) | 17 (34.0%) |
| USD 30,000 to <49,999 | 22 (21.5%) | 14 (26.9%) | 8 (16.0%) |
| More than USD 50,000 | 14 (13.8%) | 7 (13.5%) | 7 (14.0%) |
| Unknown or not reported | 2 (1.9%) | 1 (1.9%) | 1 (2.0%) |
| Means | Latent Change Score (LCS) | Group Differences in LCS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Standard Coping Power | Mindful Coping Power | Standard Coping Power | Mindful Coping Power | |||||||
| Pre | Post | Pre | Post | Estimate | p | Estimate | p | Cohen’s d (95% CI) | p | |
| Child-reported outcomes | ||||||||||
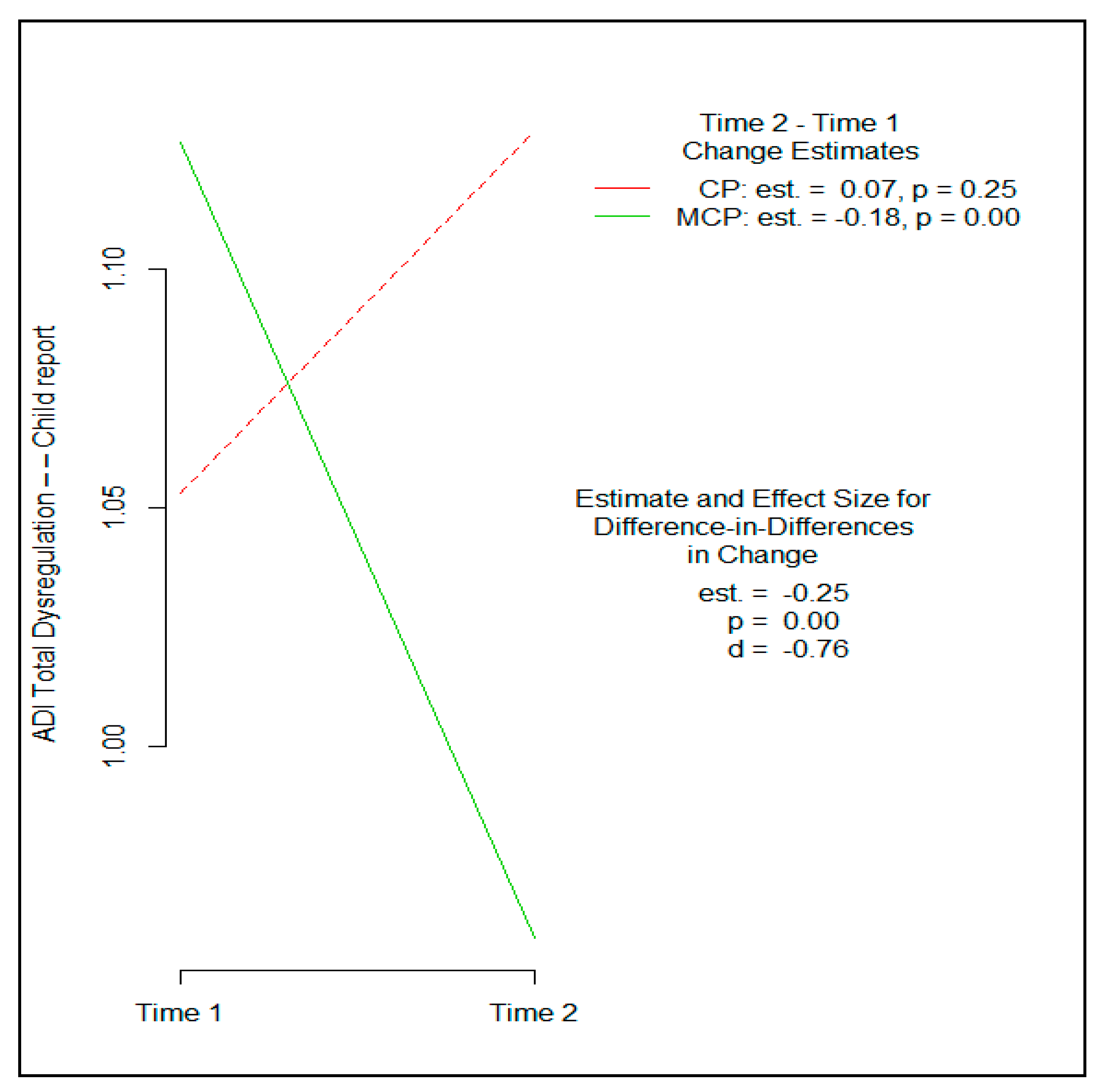
| Total Dysregulation (ADI) a | 1.05 | 1.13 | 1.13 | 0.96 | 0.07 | 0.248 | −0.18 | 0.000 | −0.76 (−1.40, −0.10) | 0.001 |
| Anger Scale (ADI) a | 1.02 | 1.09 | 1.07 | 0.80 | 0.08 | 0.540 | −0.28 | 0.010 | −0.45 (−0.70, −0.03) | 0.033 |
| Inhibitory Control (EATQ) b | 3.64 | 3.56 | 3.57 | 3.77 | −0.07 | 0.558 | 0.20 | 0.043 | 0.37 (−0.03, 0.58) | 0.081 |
| Breath Awareness (SBC) b | 3.33 | 3.37 | 3.11 | 3.64 | 0.07 | 0.702 | 0.53 | 0.008 | 0.31 (−0.07, 0.99) | 0.090 |
| Parent-reported outcomes | ||||||||||
| Attention (EATQ) b | 3.28 | 3.16 | 3.08 | 3.23 | −0.09 | 0.326 | 0.16 | 0.228 | 0.32 (−0.07, 0.58) | 0.121 |
| Social Skills T-score (BASC) b | 53.78 | 52.05 | 51.06 | 51.63 | −1.77 | 0.149 | 0.65 | 0.593 | 0.30 (−0.96, 5.79) | 0.161 |
| Externalizing Problems T-score (BASC) a | 52.57 | 49.80 | 51.98 | 53.18 | −2.81 | 0.104 | 1.11 | 0.422 | 0.36 (−0.42, 8.25) | 0.077 |
| Teacher-reported outcomes | ||||||||||
| Reactive Aggression (TRRPA) a | 9.40 | 10.08 | 9.80 | 10.56 | 0.69 | 0.215 | 0.87 | 0.029 | 0.13 (−1.17, 1.51) | 0.802 |
| Social Skills T-score (BASC) b | 41.16 | 44.14 | 39.87 | 42.00 | 2.81 | 0.013 | 2.06 | 0.019 | −0.02 (−3.55, 2.04) | 0.598 |
| Externalizing Problems T-score (BASC) a | 57.78 | 61.59 | 58.58 | 60.74 | 4.12 | 0.001 | 2.13 | 0.021 | −0.04 (−5.61, 1.62) | 0.279 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boxmeyer, C.L.; Miller, S.; Romero, D.E.; Powell, N.P.; Jones, S.; Qu, L.; Tueller, S.; Lochman, J.E. Mindful Coping Power: Comparative Effects on Children’s Reactive Aggression and Self-Regulation. Brain Sci. 2021, 11, 1119. https://doi.org/10.3390/brainsci11091119
Boxmeyer CL, Miller S, Romero DE, Powell NP, Jones S, Qu L, Tueller S, Lochman JE. Mindful Coping Power: Comparative Effects on Children’s Reactive Aggression and Self-Regulation. Brain Sciences. 2021; 11(9):1119. https://doi.org/10.3390/brainsci11091119
Chicago/Turabian StyleBoxmeyer, Caroline L., Shari Miller, Devon E. Romero, Nicole P. Powell, Shannon Jones, Lixin Qu, Stephen Tueller, and John E. Lochman. 2021. "Mindful Coping Power: Comparative Effects on Children’s Reactive Aggression and Self-Regulation" Brain Sciences 11, no. 9: 1119. https://doi.org/10.3390/brainsci11091119
APA StyleBoxmeyer, C. L., Miller, S., Romero, D. E., Powell, N. P., Jones, S., Qu, L., Tueller, S., & Lochman, J. E. (2021). Mindful Coping Power: Comparative Effects on Children’s Reactive Aggression and Self-Regulation. Brain Sciences, 11(9), 1119. https://doi.org/10.3390/brainsci11091119