
Primitive Reflex Activity in Relation to Motor Skills in Healthy Preschool Children

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
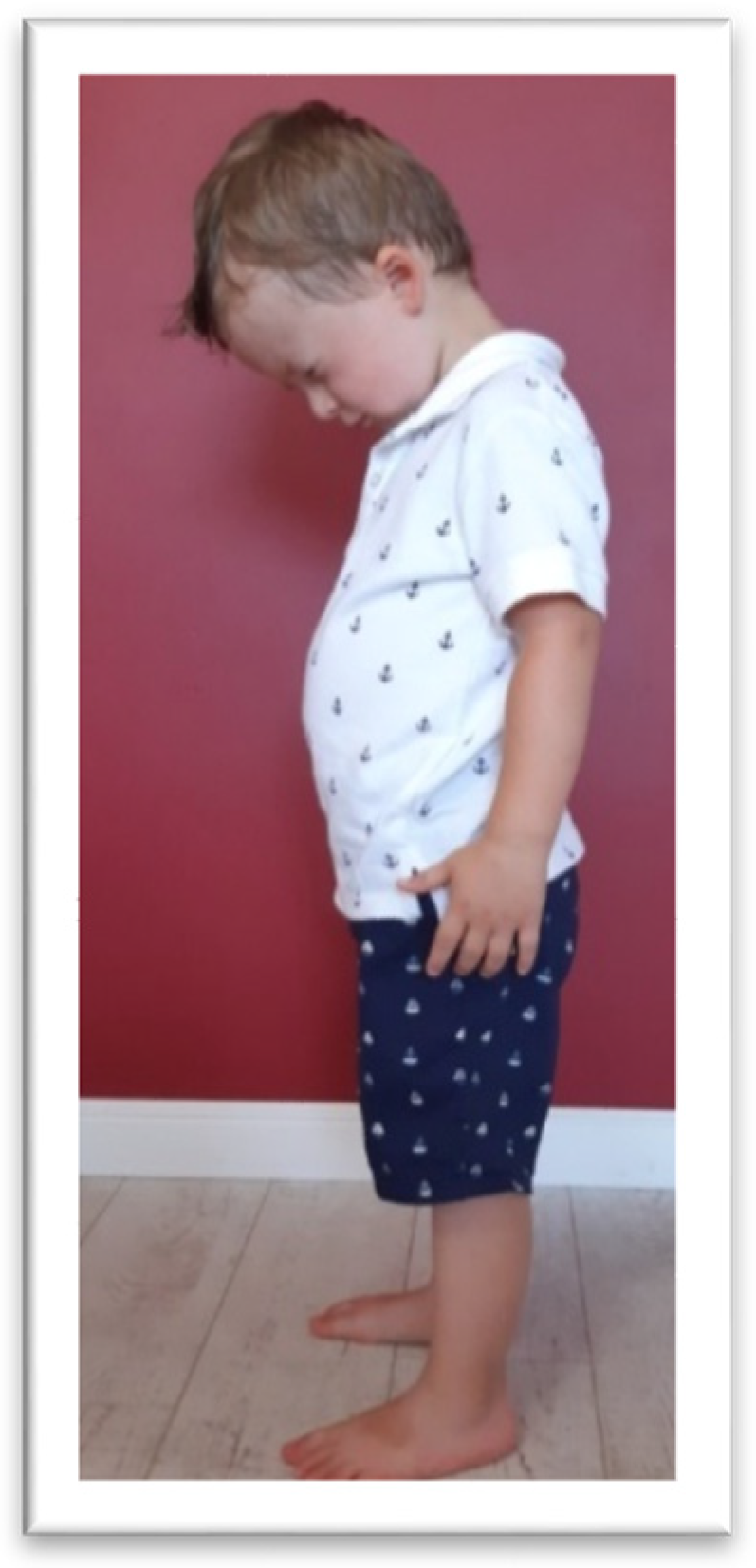
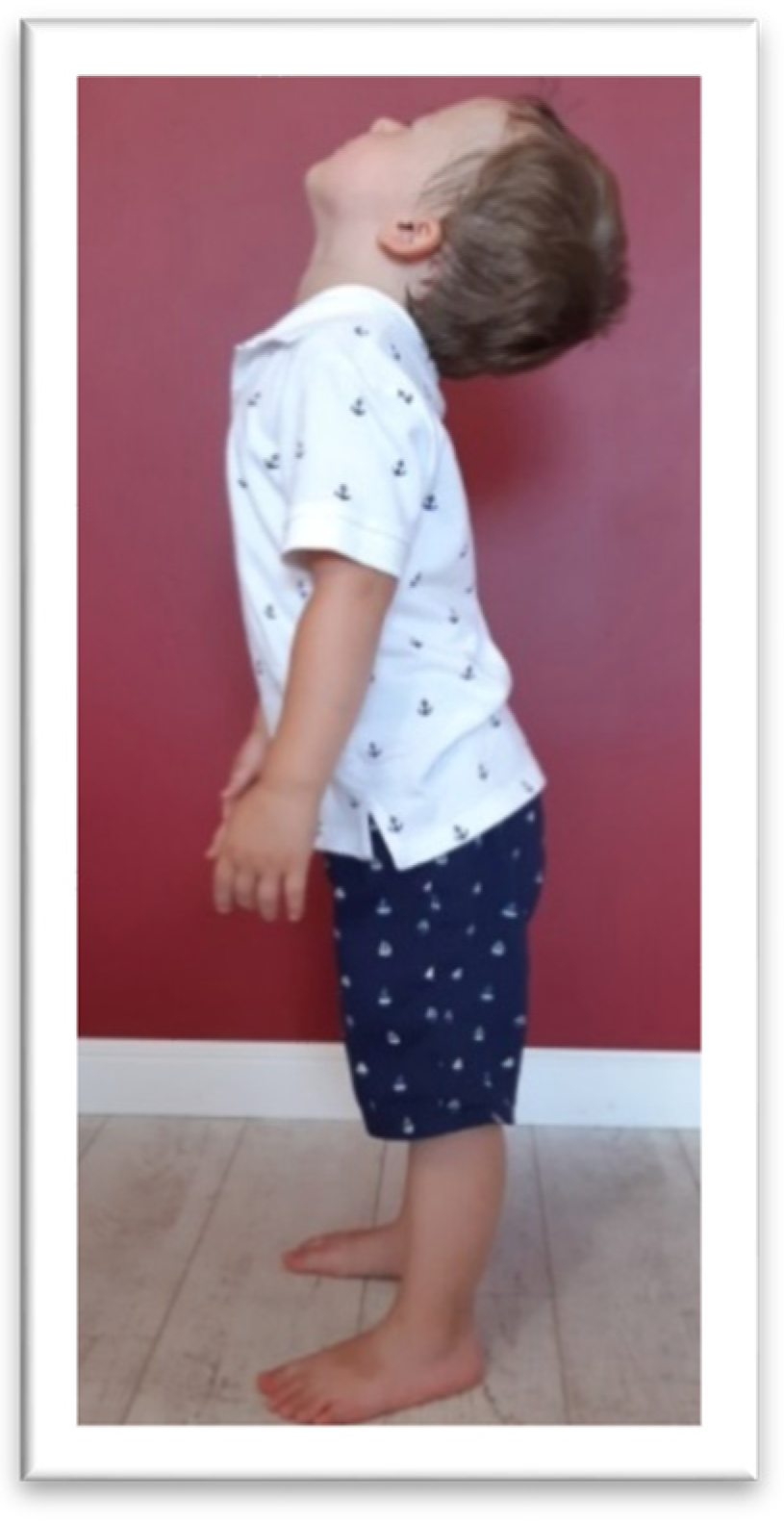
2.2. Assessment of Reflex Activity
2.3. Motor Proficiency Test (MOT) Assessment
2.4. Statistics
3. Results
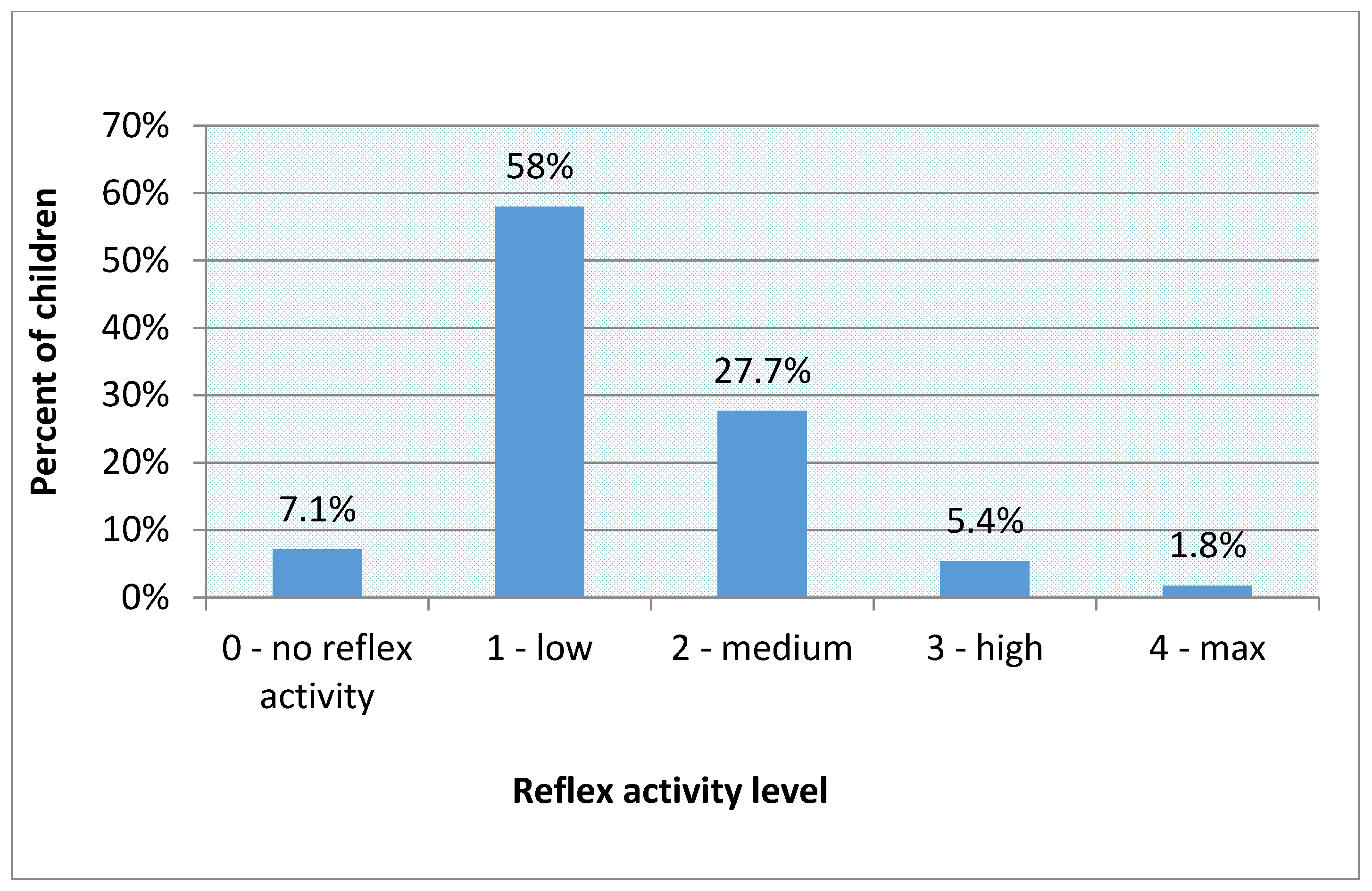
3.1. Reflex Activity Level in the Examined Group
3.2. Results of APR Examination
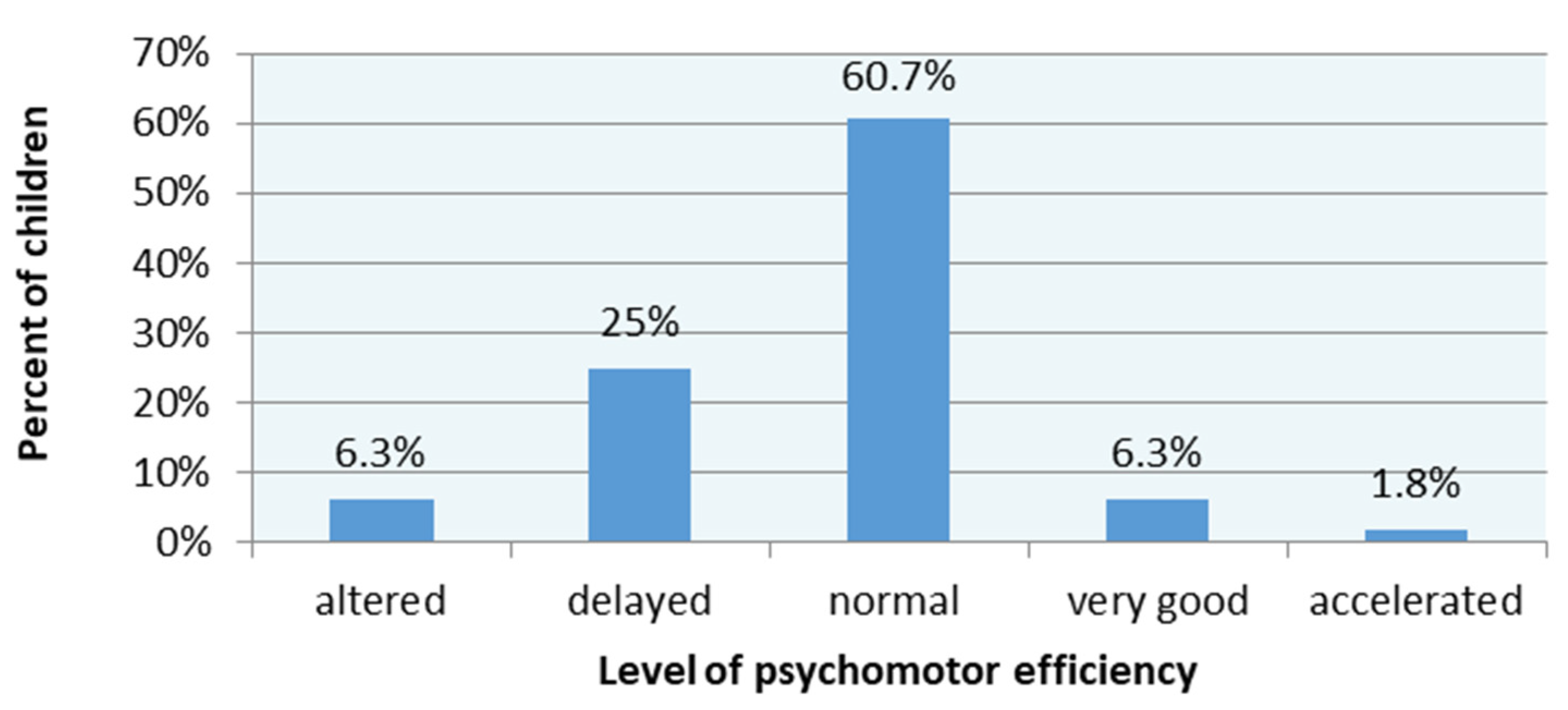
3.3. MOT 4–6 Results
3.4. The Results of the Motor Proficiency Test and Reflex Activity
3.5. Relationship between Age, Reflex Activity and Motor Perfomance
3.6. Relationship between Age, Gender, and Motor Performance
3.7. Differences between Girls and Boys in the Reflex Activity and MOT 4–6
3.8. The Relation of Results of the Reflex Level and MOT Test to BMI
4. Discussion
4.1. The APRs Releted to Motor Skills
4.2. APRs in Preschool Children in Relation to Age
4.3. APRs Integrating Therapies
4.4. Motor Skills of Preschool Children
4.5. APRs and Motor Skills Releted to Gender and BMI
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hickey, J.; Feldhacker, D.R. Primitive reflex retention and attention among preschool children. J. Occup. Ther. Sch. Early Interv. 2021. [Google Scholar] [CrossRef]
- Zafeiriou, D.I. Primitive reflexes and postural reactions in the neurodevelopmental examination. Pediatr. Neurol. 2004, 31, 1–8. [Google Scholar] [CrossRef]
- De Jager, M. Sequence of Primitive Reflexes in Development; Mind Moves Institute: Johannesburg, South Africa, 2009. [Google Scholar]
- Sigafoos, J.; Roche, L.; O’Reilly, M.F.; Lancioni, G.E. Persistence of Primitive Reflexes in Developmental Disorders. Curr. Dev. Disord. Rep. 2021. [Google Scholar] [CrossRef]
- Goddard Blythe, S.; Duncombe, R.; Preedy, P.; Gorely, T. Neuromotor readiness for school: The primitive reflex status of young children at the start and end of their first year at school in the United Kingdom. In Education 3-13: International Journal of Primary, Elementary and Early Years Education; Taylor&Francis Online: London, UK, 2021. [Google Scholar] [CrossRef]
- Gieysztor, E.Z.; Choińska, A.M.; Paprocka-Borowicz, M. Persistence of primitive reflexes and associated motor problems in health preschool children. Arch. Med. Sci AMS 2018, 14, 167. [Google Scholar] [CrossRef]
- Gieysztor, E.Z.; Pecuch, A.; Kowal, M.; Borowicz, W.; Paprocka-Borowicz, M. Pelvic Symmetry Is Influenced by Asymmetrical Tonic Neck Reflex during Young Children’s Gait. Int. J. Environ. Res. Public Health 2020, 17, 4759. [Google Scholar] [CrossRef]
- Kawakami, M.; Liu, M.; Otsuka, T.; Wada, A.; Uchikawa, K.; Aoki, A.; Otaka, Y. Asymmetrical skull deformity in children with Cerebral Palsy: Frequencyand correlation with postural abnormalities and deformties. J. Rehabil. Med. 2013, 45, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Chandradasa, M.; Rathnayake, L. Retained primitive reflexes in children, clinical implications and targeted home-based interventions. Nurs. Child. Young People 2021, 33. [Google Scholar] [CrossRef]
- Bilbilaj, S.; Gjipali, A.; Shkurti, F. Measuring Primitive Reflexes in Children with Learning Disorders. Eur. J. Multidiscip. Stud. 2017, 2, 285–298. [Google Scholar] [CrossRef]
- McPhilips, M.; Sheehy, N. Prevalence of persistent primary reflexes and motor problems in children with reading difficulties. Dyslexia 2004, 10, 316–338. [Google Scholar] [CrossRef]
- Pecuch, A.; Gieysztor, E.Z.; Telenga, M.; Wolańska, E.; Kowal, M.; Paprocka-Borowicz, M. Primitive reflex activity in relation to the sensory profile in healthy preschool children. Int. Environ. Res. Public Health 2020, 17, 8210. [Google Scholar] [CrossRef]
- Goddard-Blythe, S. Attention, Balance and Coordination: The, A.B.C of Learning Succes; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Konicarova, J.; Bob, P.; Raboch, J. Persisting Primitive Reflexes in Medication-Naïve Girls with Attention-Deficit and Hyperactivity Disorder. Neuropsychiatr. Dis. Treat. 2013, 9, 1457. [Google Scholar] [CrossRef]
- McPhilips, M.; Jordan-Black, J.N. Primary reflex persistence in children with reading difficulties (dyslexia): A cross-sectional study. Neuropsychologia 2007, 45, 748–754. [Google Scholar] [CrossRef]
- Taylor, M.; Houghton, S.; Chapman, E. Primitive reflexes and attention-deficit/hyperactivity disorder: Developmental origins of classroom dysfunction. Int. J. Spec. Educ. 2004, 19, 23–37. [Google Scholar]
- Gieysztor, E.Z.; Sadowska, L.; Choińska, A.M. The degree of primitive reflexes integration as a diagnostic tool to assess the neurological maturity of healthy preschool and early school age children. Pielęgniarstwo Zdr. Publiczne Nurs. Public Health 2017, 7, 5–11. [Google Scholar] [CrossRef]
- Grzywniak, C. The effect of the form of persistent trace reflexes to rise the difficulties of school. Szk. Spec. 2010, 2, 98–112. [Google Scholar]
- Goddard-Blythe, G. Releasing Educational Potential through Movement: A Summary of Individual Studies Carried out Using the INPP Test Battery and Developmental Exercise Programme for use in Schools with Children with Special Needs. Child Care Pract. 2005, 11, 415–432. [Google Scholar] [CrossRef]
- Demyi, A.; Kalemba, A.; Lorent, M.; Pecuch, A.; Wolańska, E.; Telenga, M.; Gieysztor, E.Z. A Child’s Perception of Their Developmental Difficulties in Relation to Their Adult Assessment. Analysis of the INPP Questionnaire. J. Pers. Med. 2020, 10, 156. [Google Scholar] [CrossRef]
- Blythe, S.G. Neuromotor Immaturity in Children and Adults: The INPP Screening Test for Clinicans and Health Practitioners; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Zimmer, R.; Volkamer, M. Motor Skills Test for 4–6 Yearsold Children; Beltz: Weinheim, Germany, 1987. [Google Scholar]
- Hazzaa, N.; Shalaby, A.; Hassanein, S.; Naeem, F.; Khattab, A.; Metwally, N. Assessment of balance functions and primitive reflexes in children with learning disability. Ain Shams Med. J. 2021, 72, 97–103. [Google Scholar] [CrossRef]
- Cools, W.; De Martelaer, K.; Vandaele, B. Assessment of movement skill performance in preschool children: Convergent validity between MOT 4–6 and M-ABC. J. Sports Sci. Med. 2010, 9, 597. [Google Scholar] [PubMed]
- Gieysztor, E.; Sadowska, L.; Choińska, A.; Paprocka-Borowicz, M. Trunk rotation due to persistence of primitive reflexes in early school age children. Adv. Clin. Exp. Med. 2018, 27, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Alibakhshi, H.; Salmani, M.; Ahmadizadeh, Z.; Siminghalam, M. Relationship between primitive reflexes and fine motor skills in children with specific learning disorders. Koomesh 2018, 20, 478–483. [Google Scholar]
- Matuszkiewicz, M.; Gałkowski, T. Developmental Language Disorder and Uninhibited Primitive Reflexes in Young Children. J. Speech Lang. Hear. Res. 2021, 64, 935–948. [Google Scholar] [CrossRef]
- Accardo, P.J.; Barrow, W. Toe walking in autism: Further observations. J. Child. Neurol. 2015, 30, 606–609. [Google Scholar] [CrossRef]
- Sohn, M.; Ahn, Y.; Lee, S. Assessment of primitive reflexes in high-risk newborns. J. Clin. Med. Res. 2011, 3, 285. [Google Scholar] [CrossRef][Green Version]
- Bruijn, S.M.; Massaad, F.; Maclellan, M.J.; Van Gestel, L.; Ivanenko, Y.P.; Duysens, J. Are effects of the symmetric and asymmetric tonic reflexes still visible in healthy adults? Neurosci. Lett. 2013, 556, 89–92. [Google Scholar] [CrossRef]
- Grzywniak, C. Role of early-childhood reflexes in psychomotor development of a child, and in learning. Acta Neuropsychol. 2016, 14, 113–129. [Google Scholar] [CrossRef]
- Pilecki, W.; Masgutova, S.; Kowalewska, J.; Masgutov, D.; Akhmatova, N.; Poręba, M.; Sobieszczańska, M.; Koleda, P.; Pilecka, A.; Kałka, D. The Impact of Rehabilitation Carried out Using the Masgutova Neurosensorimotor Reflex Integration Method in Children with Cerebral Palsy on the Results of Brain Stem Auditory Potential Examinations. Adv. Clin. Exp. Med. 2012, 21, 363–371. [Google Scholar]
- Goddard Blythe, S. The Well Balanced Child: Movement and Early Learning, 2nd ed.; Hawthorn Press: Stroud, UK, 2005. [Google Scholar]
- Grzywniak, C. Integration exercise programme for children with learning difficulties who have preserved vestigial primitive reflexes. Acta Neuropsychol. 2017, 15, 241–256. [Google Scholar] [CrossRef]
- Grigg, T.M.; Fox-Turnbull, W.; Culpan, I. Retained primitive reflexes: Perceptions of parents who have used Rhythmic Movement Training with thei children. J.Child Health Care 2018, 22, 406–418. [Google Scholar] [CrossRef] [PubMed]
- Melillo, R.; Leisman, G.; Mualem, R.; Ornai, A.; Carmeli, E. Persistent Childhood Primitive Reflex Reduction Effects on Cognitive, Sensorimotor, and Academic Performance in ADHD. Front. Public Health 2020, 8, 684. [Google Scholar] [CrossRef]
- Wagh, S.C.; Malawade, M.R.; Vardharajulu, G. Effect of Specific Reflex Integration Approach on Primitive Reflexes in Spastic Cerebral Palsy Children. Int. J. Health Sci. Res. 2019, 9, 87–93. [Google Scholar]
- Preedy, P.; Duncombe, R.; Gorely, T. Physical development in the early years: The impact of a daily movement programme on young children’s physical development. Education 2020. [Google Scholar] [CrossRef]
- Cools, W.; De Martelaer, K.; Samaey, C.; Andries, C. Movement skill assessment of typically developing preschool children: A review of seven movement skill assessment to tools. J. Sports Sci. Med. 2009, 8, 154. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | 4 Years | 5 Years | 6 Years |
|---|---|---|---|
| Age, mean ± SD Girls | 4.1 ± 0.2 38 | 5.1 ± 0.2 15 | 6.24 ± 0.4 10 |
| Boys | 23 | 19 | 7 |
| Height, mean ± SD [m] | 103.7 ± 6.1 | 111.1 ± 5.5 | 118.69 ± 5.9 |
| Weight, mean ± SD [kg] | 17.6 ± 3.8 | 19.4 ± 3.1 | 22.92 ± 4.7 |
| BMI, mean ± SD [kg/m²] | 18.3 ± 13.6 | 15.8 ± 2.2 | 16.19 ± 3.1 |
| Final Score in APR Examination | Reflex Activity Level |
|---|---|
| 0–1 | 0—no activity |
| 2–8 | 1—low activity |
| 9–14 | 2—medium activity |
| 15–21 | 3—high activity |
| 21–24 | 4—maximum activity |
| Description of Items | |
|---|---|
| 0. Forward jump in a hoop * 1. Forward balance (b) 2. Placing dots on a sheet (d) 3. Grasping a tissue with toes (d) 4. Sideward jump (b) 5. Catching a stick (c) 6. Carrying balls from one box to another (b,c) 7. Reverse balance (b) 8. Throwing at a target disk (c) 9. Collecting matches (d) | 10. Passing through a hoop (a,b) 11. Jumping in a hoop on 1 foot, standing on 1 leg (a,b) 12. Catching a tennis ring (c) 13. Jumping jacks (b) 14. Jumping over the cord (b) 15. Rolling around the long axis of the body(a,b) 16. Standing up while holding a ball on the head (b,c) 17. Jumping and turning in a hoop (a,b) |
| Final Score in MOT Test | Level of Psychomotor Efficiency |
|---|---|
| 0–8 | 0—altered |
| 9–15 | 1—delated |
| 16–25 | 2—normal |
| 26–29 | 3—very good |
| 30–34 | 4—accelerated |
| SCALE | ATNR R | ATNR L | STNR FLX | STNR EXT | TLR FLX | TLR EXT |
|---|---|---|---|---|---|---|
| 0 | 26.8% | 19.6% | 55.4% | 32.1% | 44.6% | 25.9% |
| 1 | 28.6% | 41.1% | 28.6% | 32.1% | 33.0% | 28.5% |
| 2 | 23.2% | 19.7% | 6.2% | 19.6% | 12.5% | 18.8% |
| 3 | 13.4% | 8.9% | 7.1% | 12.5% | 4.5% | 9.8% |
| 4 | 8.0% | 10.7% | 2.7% | 2.7% | 5.4% | 17.0% |
| MEAN | 1.5 | 1.5 | 0.7 | 1.2 | 0.9 | 1.6 |
| SD | 1.2 | 1.2 | 1.0 | 1.1 | 1.1 | 1.4 |
| TASK | ||||||||
|---|---|---|---|---|---|---|---|---|
| SCALE | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| 0 | 33.0% | 18.2% | 31.5% | 49.1% | 28.6% | 87.5% | 85.7% | 74.1% |
| 1 | 35.7% | 23.5% | 18.2% | 34.8% | 58.9% | 10.7% | 10.7% | 23.2% |
| 2 | 31.3% | 58.3% | 50.3% | 16.1% | 12.5% | 1.8% | 3.6% | 2.7% |
| MEAN | 1.0 | 1.4 | 1.2 | 0.7 | 0.8 | 0.2 | 0.2 | 0.3 |
| SD | 0.8 | 0.8 | 0.9 | 0.7 | 0.6 | 0.4 | 0.5 | 0.5 |
| TASK | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| SCALE | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 |
| 0 | 57.1% | 7.1% | 42.0% | 45.2% | 26.8% | 23.2% | 11.6% | 0.9% | 23.5% |
| 1 | 28.6% | 17.0% | 26.8% | 27.4% | 33.9% | 33.0% | 38.4% | 8.0% | 29.8% |
| 2 | 14.3% | 75.9% | 31.2% | 27.4% | 39.3% | 43.8% | 50.0% | 91.1% | 46.7% |
| MEAN | 0.6 | 1.7 | 0.9 | 0.8 | 1.2 | 1.2 | 1.4 | 1.9 | 1.3 |
| SD | 0.7 | 0.6 | 0.9 | 0.8 | 0.8 | 0.8 | 0.7 | 0.3 | 0.9 |
| Reflex | Correlation Coefficient |
|---|---|
| ATNR R | −0.204 * |
| ATNR L | −0.161 |
| STNR FLX | −0.201 * |
| STNR EXT | −0.317 * |
| TLR FLX | −0.294 * |
| TLR EXT | −0.157 |
| TOTAL SCORE | −0.327 * |
| REFLEX ACTIVITY LEVEL | −0.306 * |
| MOT 4–6 Task | Correlation Coefficient |
|---|---|
| 1. Forward balance | −0.215 * |
| 2. Placing dots on a sheet | −0.125 |
| 3. Grasping a tissue with toes | −0.190 |
| 4. Sideward jump | −0.010 |
| 5. Catching a stick | −0.072 |
| 6. Carrying balls from one box to another | −0.100 |
| 7. Reverse balance | −0.256 * |
| 8. Throwing at a target disk | −0.092 |
| 9. Collecting matches | −0.055 |
| 10. Passing through a hoop | −0.028 |
| 11. Jumping in a hoop on 1 foot, standing on 1 leg | −0.030 |
| 12. Catching a tennis ring | −0.072 |
| 13. Jumping jacks | −0.262 * |
| 14. Jumping over a cord | −0.288 * |
| 15. Rolling around the long axis of the body | −0.251 * |
| 16. Standing up while holding a ball on the head | −0.158 |
| 17. Jumping and turning in a hoop | −0.090 |
| Coefficient | 95% CI | Beta (ß) | 95% CI | t | p | |
|---|---|---|---|---|---|---|
| Intercept | −50.67 | (−69.15; −32.19) | −5.43 | 0.000 | ||
| Age | 91.86 | (67.81; 115.91) | 0.57 | (0.42; 0.73) | 7.57 | 0.000 |
| APR | −0.66 | (−1.23; −0.09) | −0.17 | (−0.33; −0.02) | −2.30 | 0.023 |
| Coefficient | 95% CI | Beta (ß) | 95% CI | t | p | |
|---|---|---|---|---|---|---|
| Intercept | −58.69 | (−77.70;−39.69) | −6.12 | 0.000 | ||
| Gender (=1) | −15.02 | (−34.02; 3.98) | −2.55 | (−5.78; 0.68) | −1.57 | 0.120 |
| Age | 99.28 | (74.28; 124.28) | 0.62 | (0.46; 0.78) | 7.87 | 0.000 |
| Gender (=1) × Age | 19.13 | (−5.87; 44.13) | 2.47 | (−0.76; 5.69) | 1.52 | 0.132 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pecuch, A.; Gieysztor, E.; Wolańska, E.; Telenga, M.; Paprocka-Borowicz, M. Primitive Reflex Activity in Relation to Motor Skills in Healthy Preschool Children. Brain Sci. 2021, 11, 967. https://doi.org/10.3390/brainsci11080967
Pecuch A, Gieysztor E, Wolańska E, Telenga M, Paprocka-Borowicz M. Primitive Reflex Activity in Relation to Motor Skills in Healthy Preschool Children. Brain Sciences. 2021; 11(8):967. https://doi.org/10.3390/brainsci11080967
Chicago/Turabian StylePecuch, Anna, Ewa Gieysztor, Ewelina Wolańska, Marlena Telenga, and Małgorzata Paprocka-Borowicz. 2021. "Primitive Reflex Activity in Relation to Motor Skills in Healthy Preschool Children" Brain Sciences 11, no. 8: 967. https://doi.org/10.3390/brainsci11080967
APA StylePecuch, A., Gieysztor, E., Wolańska, E., Telenga, M., & Paprocka-Borowicz, M. (2021). Primitive Reflex Activity in Relation to Motor Skills in Healthy Preschool Children. Brain Sciences, 11(8), 967. https://doi.org/10.3390/brainsci11080967