
Chimeric Anterolateral Thigh Flap in Skull Base Reconstruction: A Case-Based Update and Literature Review

 ,
, 
Abstract
1. Introduction
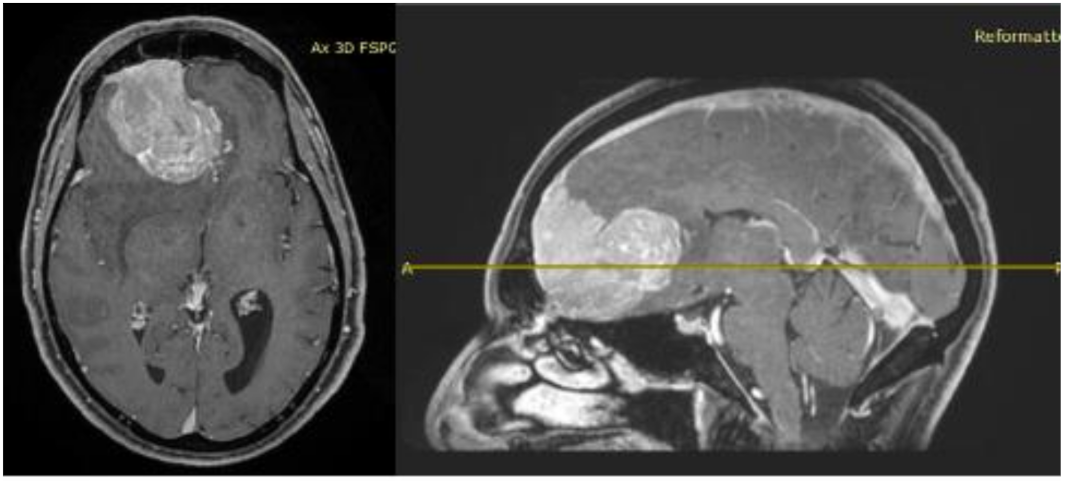
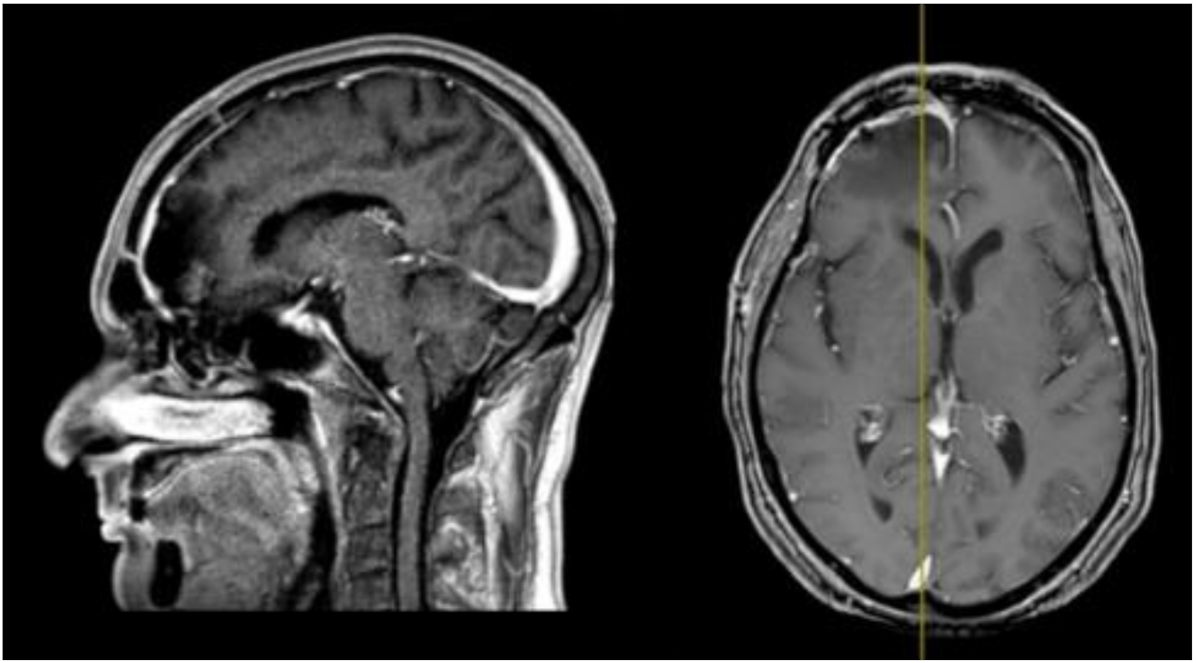
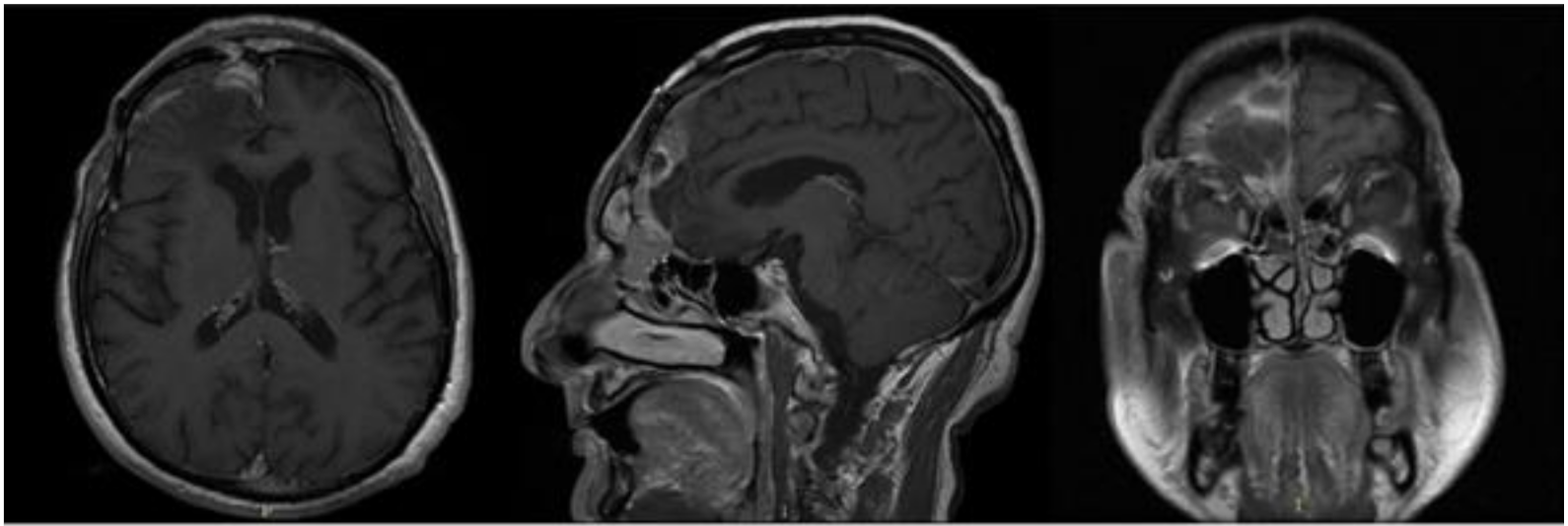
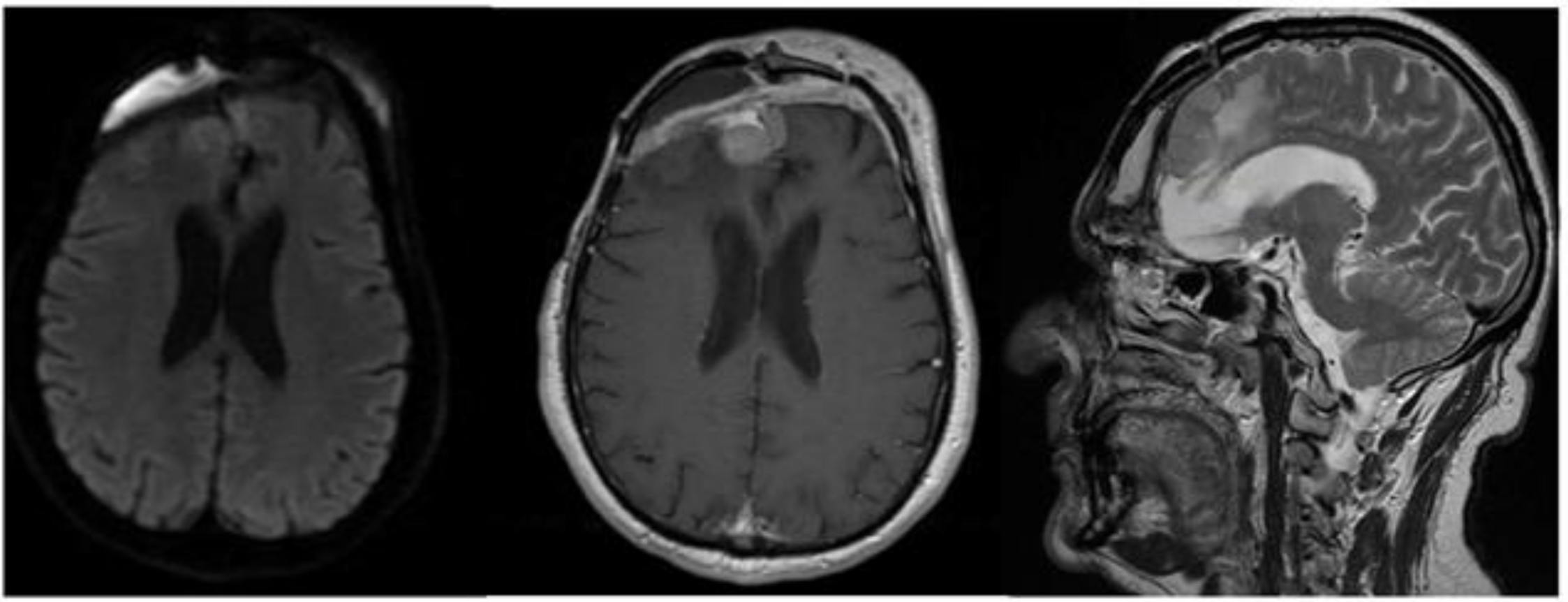
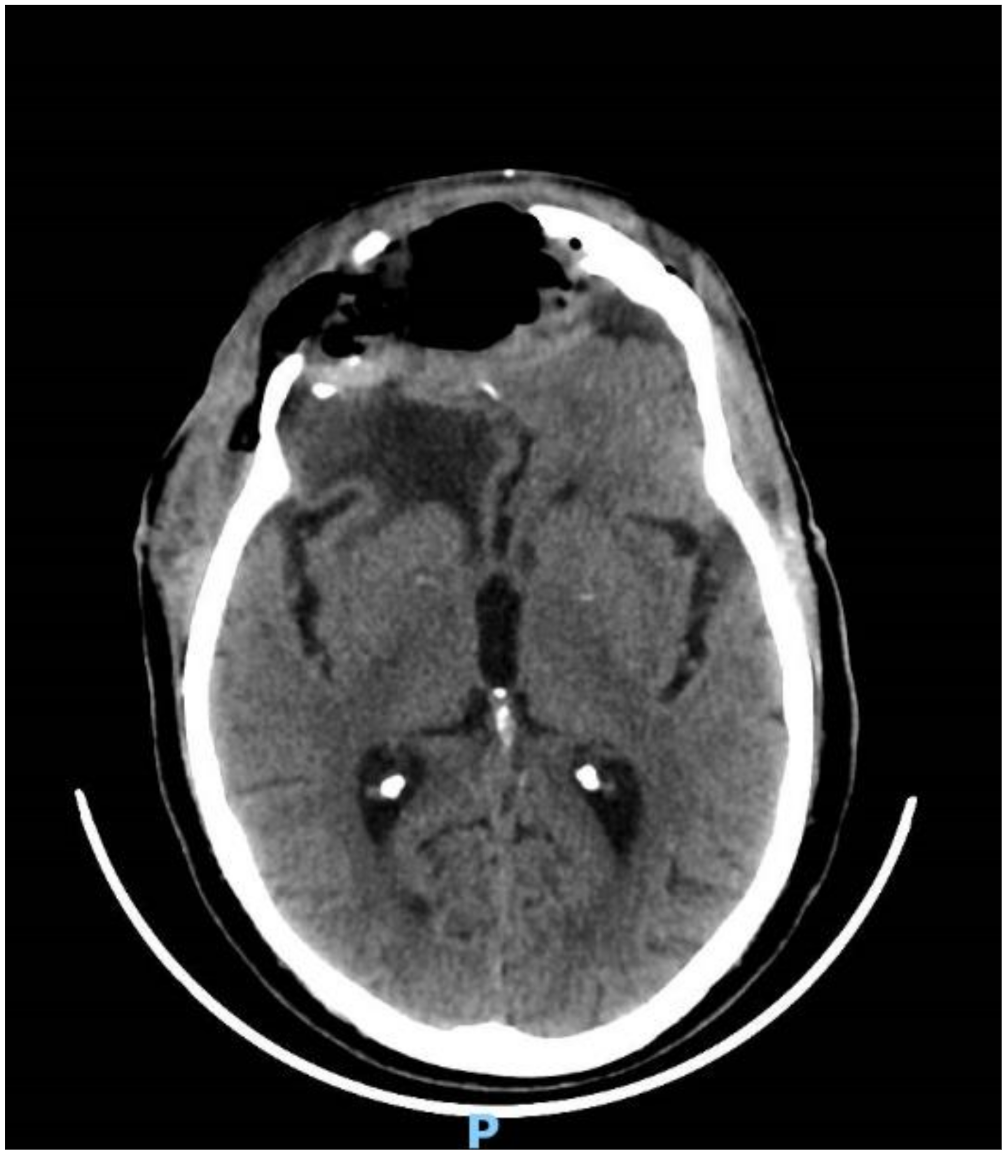
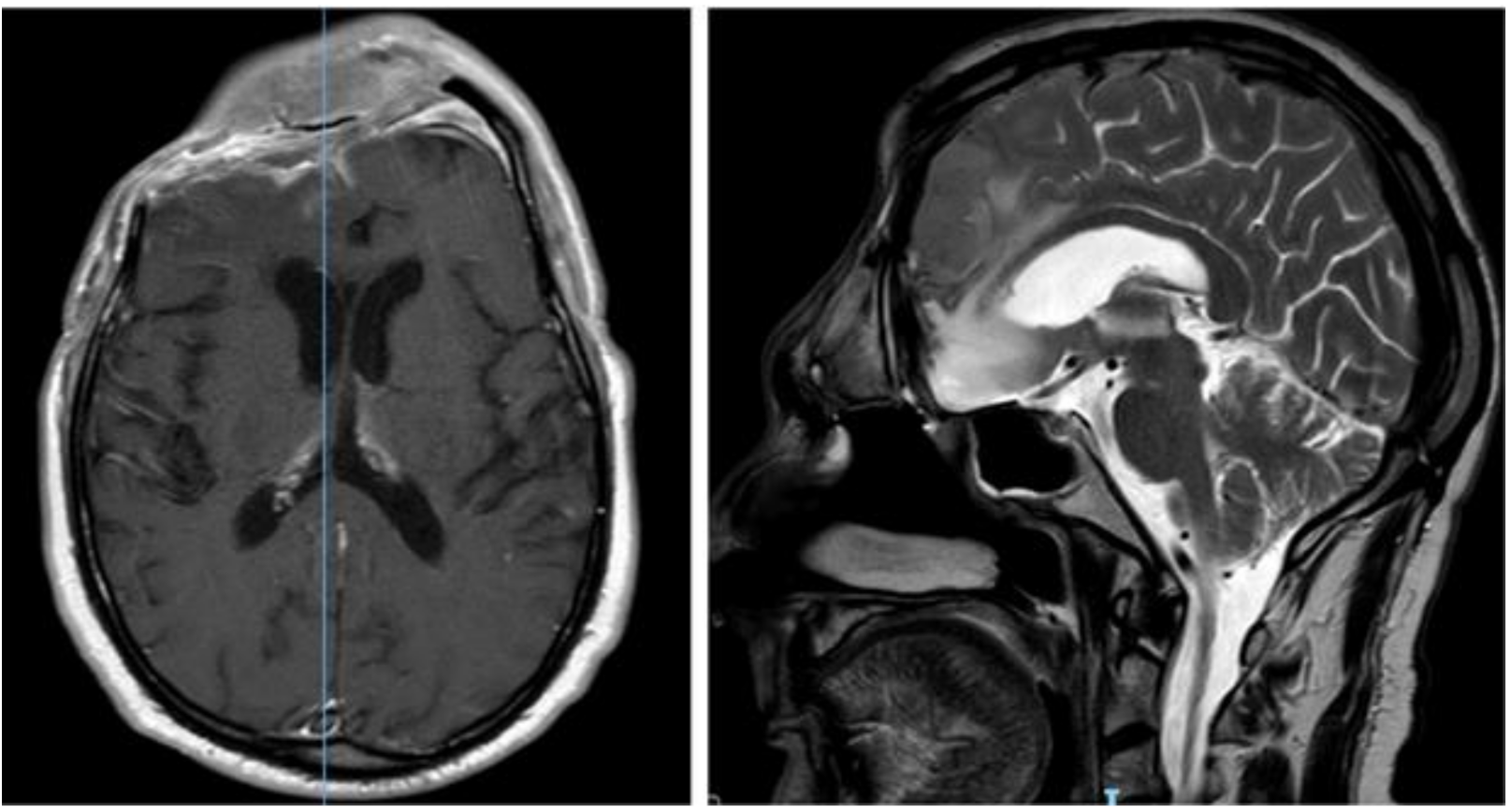
2. Case Report
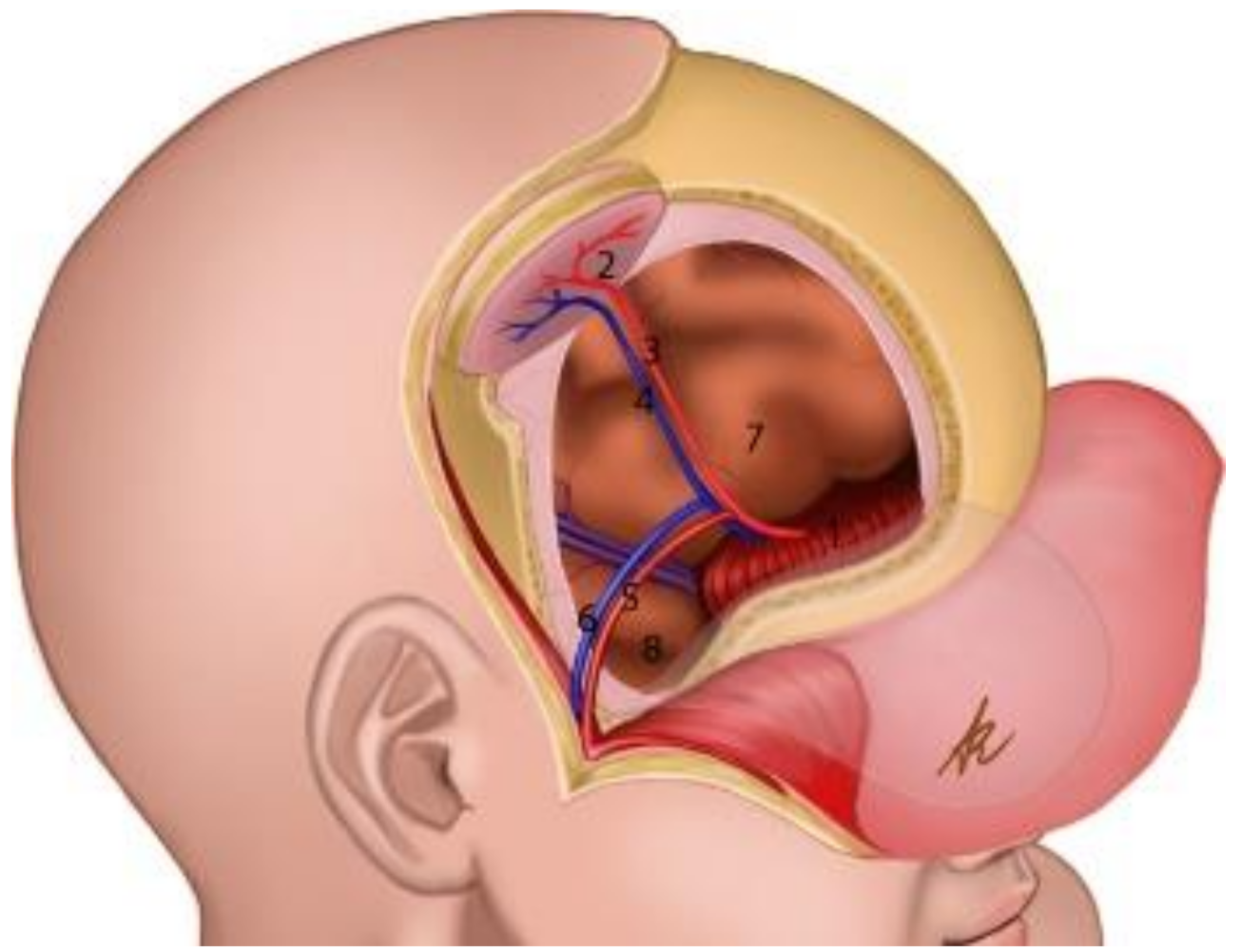
3. Surgical Technique
4. Discussion and Literature Review
- -
- High rate of good results, with relatively low risk of complications as necrosis and infection;
- -
- Adaptable to large cranial defects;
- -
- Additional skin is not necessary;
- -
- Adequate thickness;
- -
- Good microvascular anastomosis;
- -
- -
- The well-vascularized fascia components of ALT flaps can be used to seal dural defects and avoid refractory infections in the donor site;
- -
- The plasticity of the flap: it can be harvested as thinned skin and as a fasciocutaneous, myocutaneous or chimeric flap in order to provide the necessary volume in restoring the natural scalp edge [24].
- -
- The difficulty in harvesting represents the most important limitation in its choice [4].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Adler, N.; Dorafshar, A.; Agarwal, J.P.; Gottlieb, L.J. Harvesting the lateral femoral circumflex chimera free flap: Guidelines for elevation. Plast. Reconstr. Surg. 2009, 123, 918–925. [Google Scholar] [CrossRef]
- Hanasono, M.M. Reconstruction after open surgery for skull-base malignancies. J. Neuro-Oncol. 2020, 150, 469–475. [Google Scholar] [CrossRef]
- Koshima, I.; Yamamoto, H.; Hosoda, M.; Moriguchi, T.; Orita, Y.; Nagayama, H. Free combined composite flaps using the lateral circumflex femoral system for repair of massive defects of the head and neck regions. Plast. Reconstr. Surg. 1993, 92, 411–420. [Google Scholar] [CrossRef]
- Lin, P.-Y.; Miguel, R.; Chew, K.-Y.; Kuo, Y.-R.; Yang, J.C.-S. The role of the anterolateral thigh flap in complex defects of the scalp and cranium. Microsurgery 2013, 34, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Patel, U.A.; Hernandez, D.; Shnayder, Y.; Wax, M.K.; Hanasono, M.M.; Hornig, J.; Ghanem, T.A.; Old, M.; Jackson, R.; Ledgerwood, L.G.; et al. Free flap reconstruction monitoring techniques and frequency in the era of restricted resident work hours. JAMA Otolaryngol. Neck Surg. 2017, 143, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Batstone, M.D.; Blackburn, T.K.; Brown, J.S. The anterolateral thigh flap in head and neck reconstruction: “Pearls and pitfalls”. Br. J. Oral Maxillofac. Surg. 2010, 48, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Sokoya, M.; Misch, E.; Vincent, A.; Wang, W.; Kadakia, S.; Ducic, Y.; Smith, J. Free tissue reconstruction of the scalp. Semin. Plast. Surg. 2019, 33, 067–071. [Google Scholar] [CrossRef] [PubMed]
- Trignano, E.; Fallico, N.; Nitto, A.; Chen, H.-C. The treatment of composite defect of bone and soft tissues with a combined latissimus dorsi and serratus anterior and RIB free flap. Microsurgery 2012, 33, 173–183. [Google Scholar] [CrossRef]
- Visconti, G.; Pagliara, D.; Bianchi, A.; La Rocca, G.; Olivi, A.; Salgarello, M. Successful treatment of pneumocephalus using a free-style chimeric free flap from a scarred thigh. J. Craniofacial Surg. 2018, 29, e658–e660. [Google Scholar] [CrossRef]
- Yoshioka, N. Versatility of the latissimus dorsi free flap during the treatment of complex postcraniotomy surgical site infections. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1355. [Google Scholar] [CrossRef]
- Neligan, P.C.; Mulholland, S.; Irish, J.; Gullane, P.J.; Boyd, J.B.; Gentili, F.; Brown, D.; Freeman, J. Flap selection in cranial base reconstruction. Plast. Reconstr. Surg. 1996, 98, 1159–1166. [Google Scholar] [CrossRef]
- Chiu, W.-K.; Lin, W.-C.; Chen, S.-Y.; Tzeng, W.-D.; Liu, S.-C.; Lee, T.-P.; Chen, S.-G. Computed tomography angiography imaging for the chimeric anterolateral thigh flap in reconstruction of full thickness buccal defect. ANZ J. Surg. 2010, 81, 142–147. [Google Scholar] [CrossRef]
- Gong, Z.-J.; Zhang, S.; Ren, Z.-H.; Zhu, Z.-F.; Liu, J.-B.; Wu, H.-J. Application of anteromedial thigh flap for the reconstruction of oral and maxillofacial defects. J. Oral Maxillofac. Surg. 2014, 72, 1212–1225. [Google Scholar] [CrossRef]
- Hallock, G.G. Further clarification of the nomenclature for compound flaps. Plast. Reconstr. Surg. 2006, 117, 151e–160e. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.L.; Zenga, J.; Roland, L.T.; Pipkorn, P. Complications of double free flap and free flap combined with locoregional flap in head and neck reconstruction: A systematic review. Head Neck 2017, 40, 632–646. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.-G.; Chen, G.-Z. The free thigh flap: A new free flap concept based on the septocutaneous artery. Br. J. Plast. Surg. 1984, 37, 149–159. [Google Scholar] [CrossRef]
- Wu, K.; Ji, T.; Cao, W.; Wu, H.-J.; Ren, Z.-H. Application of a new classification of chimeric anterolateral thigh free flaps. J. Cranio-Maxillofac. Surg. 2019, 47, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Costantino, P.D.; Shamouelian, D.; Tham, T.; Andrews, R.; Dec, W. The laparoscopically harvested omental free flap: A compelling option for craniofacial and cranial base reconstruction. J. Neurol. Surg. B Skull Base 2016, 78, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Kleiber, G.M.; Pelletier, A.T.; Reid, R.R.; Gottlieb, L.J. Autologous immediate cranioplasty with vascularized bone in high-risk composite cranial defects. Plast. Reconstr. Surg. 2013, 132, 967–975. [Google Scholar] [CrossRef]
- Chana, J.S.; Odili, J. Perforator flaps in head and neck reconstruction. Semin. Plast. Surg. 2010, 24, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Khadakban, D.; Kudpaje, A.; Thankappan, K.; Jayaprasad, K.; Gorasia, T.; Vidhyadharan, S.; Mathew, J.; Sharma, M.; Iyer, S. Reconstructive indications of anterolateral thigh free flaps in head and neck reconstruction. Cranio-Maxillofac. Trauma Reconstr. 2016, 9, 040–045. [Google Scholar] [CrossRef] [PubMed]
- Numajiri, T.; Sowa, Y.; Nishino, K.; Sugimoto, K.; Iwashina, Y.; Ikebuchi, K.; Nakano, H.; Shimada, T.; Hisa, Y. Successful retrograde arterial inflow through a muscular branch in a free anterolateral thigh chimeric flap transfer. Microsurgery 2012, 32, 318–321. [Google Scholar] [CrossRef]
- Xu, Z.-F.; Duan, W.-Y.; Tan, X.-X.; Sun, C.-F. Reconstruction of complex total parotidectomy defect with a chimeric anterolateral thigh perforator flap and vascularized motor branch of femoral nerve grafting. J. Oral Maxillofac. Surg. 2015, 73, 2448.e1–2448.e7. [Google Scholar] [CrossRef]
- Zaretski, A.; Wei, F.-C.; Lin, C.-H.; Cheng, M.-H.; Tsao, C.-K.; Wallace, C.G. Anterolateral thigh perforator flaps in head and neck reconstruction. Semin. Plast. Surg. 2006, 20, 064–072. [Google Scholar] [CrossRef]
- Irish, J.C.; Gullane, P.J.; Gentili, F.; Freeman, J.; Boyd, J.B.; Brown, D.; Rutka, J. Tumors of the skull base: Outcome and survival analysis of 77 cases. Head Neck 1994, 16, 3–10. [Google Scholar] [CrossRef]
- Jones, N.F.; Schramm, V.L.; Sekhar, L.N. Reconstruction of the cranial base following tumour resection. Br. J. Plast. Surg. 1987, 40, 155–162. [Google Scholar] [CrossRef]
- Sturiale, C.L.; La Rocca, G.; Puca, A.; Fernandez, E.; Visocchi, M.; Marchese, E.; Sabatino, G.; Albanese, A. Minipterional craniotomy for treatment of unruptured middle cerebral artery aneurysms. A single-center comparative analysis with standard pterional approach as regard to safety and efficacy of aneurysm clipping and the advantages of reconstruction. Acta Neurochir. Suppl. 2017, 124, 93–100. [Google Scholar] [CrossRef]
- Giovanni, S.; Della Pepa, G.M.; La Rocca, G.; Lofrese, G.; Albanese, A.; Maria, G.; Marchese, E. Galea-pericranium dural closure: Can we safely avoid sealants? Clin. Neurol. Neurosurg. 2014, 123, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Acartürk, T.O. Femur-vastus intermedius-anterolateral thigh osteomyocutaneous composite chimeric free flap: A new free flap for the reconstruction of complex wounds. J. Reconstr. Microsurg. 2010, 27, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Hanasono, M.M.; Sacks, J.M.; Goel, N.; Ayad, M.; Skoracki, R.J. The anterolateral thigh free flap for skull base reconstruction. Otolaryngol. Neck Surg. 2009, 140, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Heller, F.; Hsu, C.-M.; Chuang, C.-C.; Wei, K.-C.; Wei, F.-C. Anterolateral thigh fasciocutaneous flap for simultaneous reconstruction of refractory scalp and dural defects. J. Neurosurg. 2004, 100, 1094–1097. [Google Scholar] [CrossRef]
- Cherubino, M.; Turri-Zanoni, M.; Battaglia, P.; Giudice, M.; Pellegatta, I.; Tamborini, F.; Maggiulli, F.; Guzzetti, L.; Di Giovanna, D.; Bignami, M.; et al. Chimeric anterolateral thigh free flap for reconstruction of complex cranio-orbito-facial defects after skull base cancers resection. J. Cranio-Maxillofac. Surg. 2016, 45, 87–92. [Google Scholar] [CrossRef]
- Parkes, W.J.; Krein, H.; Heffelfinger, R.; Curry, J. Use of the anterolateral thigh in cranio-orbitofacial reconstruction. Plast. Surg. Int. 2011, 2011, 1–6. [Google Scholar] [CrossRef]
- Lo, K.-C.; Jeng, C.-H.; Lin, H.-C.; Hsieh, C.-H.; Chen, C.-L. A free composite de-epithelialized anterolateral thigh and the vastus lateralis muscle flap for the reconstruction of a large defect of the anterior skull base: A case report. Microsurgery 2011, 31, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Posch, N.; Mureau, M.; Flood, S.; Hofer, S. The combined free partial vastus lateralis with anterolateral thigh perforator flap reconstruction of extensive composite defects. Br. J. Plast. Surg. 2005, 58, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Yano, T.; Okazaki, M.; Tanaka, K.; Iida, H. The flap sandwich technique for a safe and aesthetic skull base reconstruction. Ann. Plast. Surg. 2016, 76, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Chan, F.C.; Yang, X.; Zong, X.; Sun, H.; Qi, Z.; Jin, X. Salvage free anterolateral thigh composite flap transfer based on the musculocutaneous perforator retrograde blood flow principle. J. Craniofacial Surg. 2016, 27, e178–e181. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Min, K.H.; Eun, S.C.; Lee, J.H.; Hong, S.H.; Kim, C.W. Scalp free flap reconstruction using anterolateral thigh flap pedicle for interposition artery and vein grafts. Arch. Plast. Surg. 2012, 39, 55–58. [Google Scholar] [CrossRef]
- Llorente, J.L.; Camporro, D.; Fueyo, A.; Rial, J.C.; de Leon, R.F.; Suarez, C.; Lopez, F. Outcomes following microvascular free tissue transfer in reconstructing skull base defects. J. Neurol. Surg. B Skull Base 2013, 74, 324–330. [Google Scholar] [CrossRef]
- Wong, C.-H.; Wei, F.-C.; Fu, B.; Chen, Y.-A.; Lin, J.-Y. Alternative vascular pedicle of the anterolateral thigh flap: The oblique branch of the lateral circumflex femoral artery. Plast. Reconstr. Surg. 2009, 123, 571–577. [Google Scholar] [CrossRef]
- Yu, P. Characteristics of the anterolateral thigh flap in a Western population and its application in head and neck reconstruction. Head Neck 2004, 26, 759–769. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Type of Chimeric ALT Flap (Number of Cases) | Cause of Cranial Defect (Number of Cases) | Neurocranial Defect (Number of Cases) | Complication (Number of Cases) |
|---|---|---|---|---|
| Present case | Rectus femoris and fascia lata (1) | Atypical meningioma (1) | Sphenoidal planum (1) | - |
| Cherubino et al. (2017) [32] | Vastus lateralis and rectus femoris (7), with septocutaneous vessels (2) and muscolocutaneous vessels (5) | Squamocellar Carcinoma (2) Adenocarcinoma (1) Melanoma (3) Neuroblastoma (1) | Ethmoid (3) sphenoid (1) frontal sinus (1) orbit (2) | Venous congestion and failure (1) |
| Parkes et al. (2011) [33] | Vastus lateralis and rectus femoris (1) | Meningioma (4) Squamocellar carcinoma (12) Basal Cell carcinoma (6) Esthesioneuroblastoma (1) Frontal bone osteomyelitis (1) Hemangiopericytoma (1) Basosquamous carcinoma (1) Melanoma (3) | Orbital (29) | Wound infection (2) Hematoma (1) CSF leak (3) Failure (3) |
| Lo et al. (2011) [34] | Vastus lateralis and de-epithelialized skin paddle (1) | Meningioma (1) | Anterior skull base (1) | - |
| Posch et al. (2005) [35] | Partial Vastus lateralis (4) | Squamous cell carcinoma (2) Basal cell carcinoma (2) | Parietal frontal orbital (4) | Hematoma (1) Arterial occlusion (1) |
| Vastus lateralis (31) | Squamous cell carcinoma (19) Sarcoma (5) Basal cell carcinoma (5) Sebaceous cell carcinoma (1) Acinic cell carcinoma (1) | Anterior fossa (2) Middle fossa (5) Posterior fossa (17) Middle posterior fossa (4) Anterior middle fossa (6) | CSF leakage (3) Infection (3) Wound dehiscence (2) Sieroma (2) | |
| Yano et al. (2016) [36] | Vastus lateralis (3) | Olfactory neuroblastoma (1) Hemangiopericytoma (1) Meningioma (1) | Anterior skull base (2) Middle skull base (1) | - |
| Zhao et al. (2016) [37] | Vastus lateralis (1) | Trauma (1) | Frontal (1) | Atrophy and failure (1) |
| Park et al. (2012) [38] | Vastus lateralis and latissimus dorsi (1) | Trauma (1) | Fronto-parietal (1) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auricchio, A.M.; Mazzucchi, E.; Rapisarda, A.; Sabatino, G.; Della Pepa, G.M.; Visconti, G.; Salgarello, M.; Olivi, A.; La Rocca, G. Chimeric Anterolateral Thigh Flap in Skull Base Reconstruction: A Case-Based Update and Literature Review. Brain Sci. 2021, 11, 1076. https://doi.org/10.3390/brainsci11081076
Auricchio AM, Mazzucchi E, Rapisarda A, Sabatino G, Della Pepa GM, Visconti G, Salgarello M, Olivi A, La Rocca G. Chimeric Anterolateral Thigh Flap in Skull Base Reconstruction: A Case-Based Update and Literature Review. Brain Sciences. 2021; 11(8):1076. https://doi.org/10.3390/brainsci11081076
Chicago/Turabian StyleAuricchio, Anna Maria, Edoardo Mazzucchi, Alessandro Rapisarda, Giovanni Sabatino, Giuseppe Maria Della Pepa, Giuseppe Visconti, Marzia Salgarello, Alessandro Olivi, and Giuseppe La Rocca. 2021. "Chimeric Anterolateral Thigh Flap in Skull Base Reconstruction: A Case-Based Update and Literature Review" Brain Sciences 11, no. 8: 1076. https://doi.org/10.3390/brainsci11081076
APA StyleAuricchio, A. M., Mazzucchi, E., Rapisarda, A., Sabatino, G., Della Pepa, G. M., Visconti, G., Salgarello, M., Olivi, A., & La Rocca, G. (2021). Chimeric Anterolateral Thigh Flap in Skull Base Reconstruction: A Case-Based Update and Literature Review. Brain Sciences, 11(8), 1076. https://doi.org/10.3390/brainsci11081076