
Impact of Cognitive Reserve and Premorbid IQ on Cognitive and Functional Status in Older Outpatients

 ,
,  , ,
, , 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject and Study Design
2.2. Outcome Measures
2.2.1. Cognitive Functioning
2.2.2. Functional Status
2.2.3. Cognitive Reserve
2.2.4. Premorbid IQ
2.3. Data Analysis
3. Results
3.1. Demographic and Clinical Features of the Study Sample
3.2. Associations of CR and Premorbid IQ with Functional Status
3.3. Association of CR and Premorbid IQ with Cognitive Status
4. Discussion
4.1. Cognitive Reserve, Premorbid IQ, Functional Variables and Cognitive Performance: Need for Multidimensional Assessment
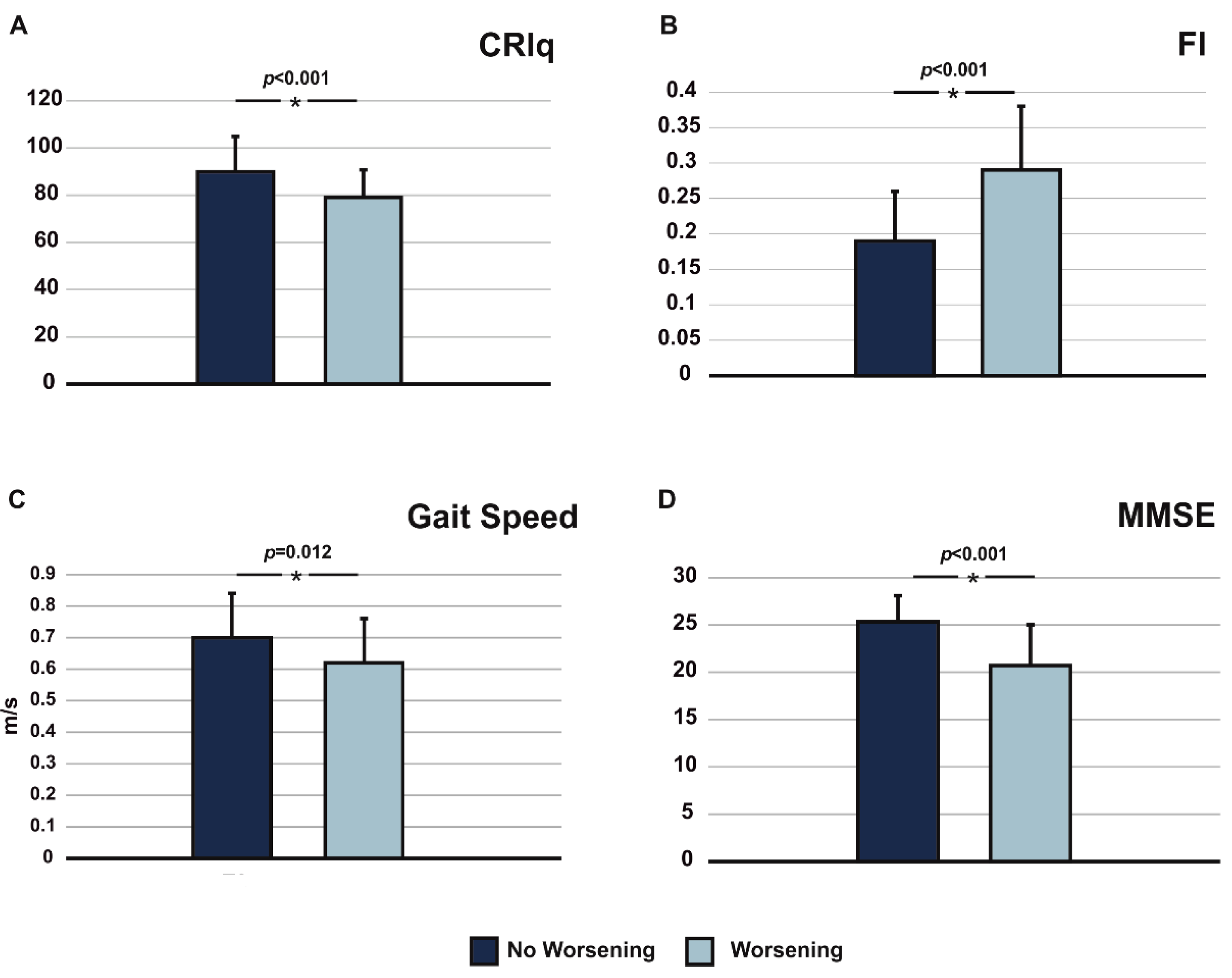
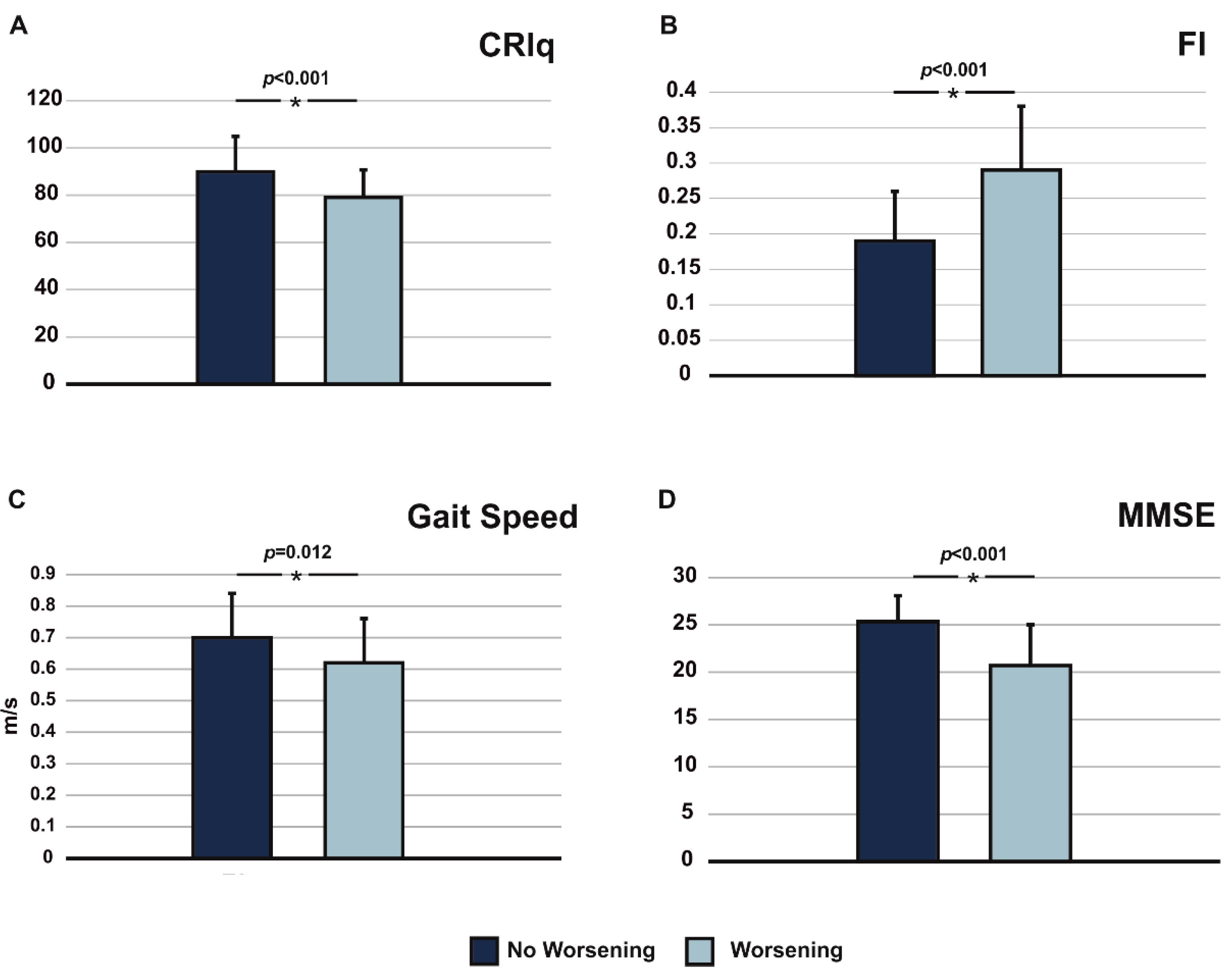
4.2. Impact of Functional Variables and CR on Worsening of Cognitive Functions
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mulasso, A.; Roppolo, M.; Giannotta, F.; Rabaglietti, E. Associations of Frailty and Psychosocial Factors with Autonomy in Daily Activities: A Cross-Sectional Study in Italian Community-Dwelling Older Adults. Clin. Interv. Aging 2016, 11, 37–45. [Google Scholar] [PubMed] [Green Version]
- Friedman, E.M.; Ryff, C.D. Living Well with Medical Comorbidities: A Biopsychosocial Perspective. J. Gerontol. B Psychol. Sci. Soc. Sci. 2012, 67, 535–544. [Google Scholar] [CrossRef] [Green Version]
- Quattropani, M.C.; Lenzo, V.; Mucciardi, M.; Toffle, M.E. Psychometric properties of the Italian version of the short form of the metacognitions questionnaire (MCQ−30). BPA Appl. Psychol. Bull. 2015, 269, 30–42. [Google Scholar]
- Paszkiel, S.; Dobrakowski, P.; Łysiak, A. The Impact of Different Sounds on Stress Level in the Context of EEG, Cardiac Measures and Subjective Stress Level: A Pilot Study. Brain Sci. 2020, 10, 728. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive Reserve in Ageing and Alzheimer’s Disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [Green Version]
- Pettigrew, C.; Soldan, A. Defining Cognitive Reserve and Implications for Cognitive Aging. Curr. Neurol. Neurosci. Rep. 2019, 19, 1. [Google Scholar] [CrossRef]
- Stern, Y. What Is Cognitive Reserve? Theory and Research Application of the Reserve Concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y. Cognitive Reserve and Lifestyle. J. Clin. Exp. Neuropsychol. 2003, 25, 625–633. [Google Scholar] [CrossRef]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. The Reserve, Resilience and Protective Factors PIA Empirical Definitions and Conceptual Frameworks Workgroup. Whitepaper: Defining and Investigating Cognitive Reserve, Brain Reserve, and Brain Maintenance. Alzheimers. Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef]
- Vallet, F.; Mella, N.; Ihle, A.; Beaudoin, M.; Fagot, D.; Ballhausen, N.; Baeriswyl, M.; Schlemmer, M.; Oris, M.; Kliegel, M.; et al. Motivation as a Mediator of the Relation between Cognitive Reserve and Cognitive Performance. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 1199–1205. [Google Scholar] [CrossRef]
- Perneczky, R.; Kempermann, G.; Korczyn, A.D.; Matthews, F.E.; Ikram, M.A.; Scarmeas, N.; Chetelat, G.; Stern, Y.; Ewers, M. Translational Research on Reserve against Neurodegenerative Disease: Consensus Report of the International Conference on Cognitive Reserve in the Dementias and the Alzheimer’s Association Reserve, Resilience and Protective Factors Professional Interest Area Working Groups. BMC Med. 2019, 17, 47. [Google Scholar]
- Gale, C.R.; Booth, T.; Starr, J.M.; Deary, I.J. Intelligence and Socioeconomic Position in Childhood in Relation to Frailty and Cumulative Allostatic Load in Later Life: The Lothian Birth Cohort 1936. J. Epidemiol. Community Health 2016, 70, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Russ, T.C.; Hannah, J.; Batty, G.D.; Booth, C.C.; Deary, I.J.; Starr, J.M. Childhood Cognitive Ability and Incident Dementia: The 1932 Scottish Mental Survey Cohort into Their 10th Decade. Epidemiology 2017, 28, 361–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzeo, S.; Padiglioni, S.; Bagnoli, S.; Bracco, L.; Nacmias, B.; Sorbi, S.; Bessi, V. The Dual Role of Cognitive Reserve in Subjective Cognitive Decline and Mild Cognitive Impairment: A 7-Year Follow-up Study. J. Neurol. 2019, 266, 487–497. [Google Scholar] [CrossRef]
- Künzi, M.; Joly-Burra, E.; Zuber, S.; Haas, M.; Tinello, D.; Da Silva Coelho, C.; Hering, A.; Ihle, A.; Laera, G.; Mikneviciute, G.; et al. The Relationship between Life Course Socioeconomic Conditions and Objective and Subjective Memory in Older Age. Brain Sci. 2021, 11, 61. [Google Scholar] [CrossRef]
- Sardella, A.; Catalano, A.; Lenzo, V.; Bellone, F.; Corica, F.; Quattropani, M.C.; Basile, G. Association between Cognitive Reserve Dimensions and Frailty among Older Adults: A Structured Narrative Review. Geriatr. Gerontol. Int. 2020, 20, 1005–1023. [Google Scholar] [CrossRef] [PubMed]
- Devita, M.; Bordignon, A.; Trevisan, C.; Sergi, G.; Girardi, A.; Mapelli, D.; Manzato, E.; Coin, A. Longitudinal Investigation of the Role of Cognitive Reserve in the Evolution of Dementia in Outpatients Prescribed AChEI. J. Clin. Exp. Neuropsychol. 2020, 42, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Castelli, L.; De Giglio, L.; Haggiag, S.; Traini, A.; De Luca, F.; Ruggieri, S.; Prosperini, L. Premorbid Functional Reserve Modulates the Effect of Rehabilitation in Multiple Sclerosis. Neurol. Sci. 2020, 41, 1251–1257. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kang, J.M.; Kim, D.J.; Woo, S.K.; Lee, J.-Y.; Cho, S.-J. Cognitive Reserve, Leisure Activity, and Neuropsychological Profile in the Early Stage of Cognitive Decline. Front. Aging Neurosci. 2020, 12, 590607. [Google Scholar] [CrossRef]
- Wöbbeking-Sánchez, M.; Bonete-López, B.; Cabaco, A.S.; Urchaga-Litago, J.D.; Afonso, R.M. Relationship between Cognitive Reserve and Cognitive Impairment in Autonomous and Institutionalized Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 5777. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Segawa, E.; Buchman, A.S.; Boyle, P.A.; Hizel, L.P.; Bennett, D.A. Terminal decline in motor function. Psychol. Aging 2012, 27, 998–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frederiksen, H.; Hjelmborg, J.; Mortensen, J.; McGue, M.; Vaupel, J.W.; Christensen, K. Age trajectories of grip strength: Cross-sectional and longitudinal data among 8,342 Danes aged 46 to 102. Ann. Epidemiol. 2006, 16, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhetri, J.K.; Chan, P.; Vellas, B.; Cesari, M. Motoric Cognitive Risk Syndrome: Predictor of Dementia and Age-Related Negative Outcomes. Front. Med. 2017, 4, 166. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.V.; Hsu, T.H.; Wu, W.T.; Huang, K.C.; Han, D.S. Association Between Sarcopenia and Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1164.e7–1164.e15. [Google Scholar] [CrossRef]
- Ward, D.D.; Wallace, L.M.K.; Rockwood, K. Cumulative health deficits, APOE genotype, and risk for later-life mild cognitive impairment and dementia. J. Neurol. Neurosurg. Psychiatry 2021, 92, 136–142. [Google Scholar] [CrossRef]
- Canevelli, M.; Arisi, I.; Bacigalupo, I.; Arighi, A.; Galimberti, D.; Vanacore, N.; D’Onofrio, M.; Cesari, M.; Bruno, G. Alzheimer’s Disease Neuroimaging Initiative. Biomarkers and phenotypic expression in Alzheimer’s disease: Exploring the contribution of frailty in the Alzheimer’s Disease Neuroimaging Initiative. Geroscience 2021, 43, 1039–1051. [Google Scholar] [CrossRef]
- Duda, B.; Puente, A.N.; Miller, L.S. Cognitive Reserve Moderates Relation between Global Cognition and Functional Status in Older Adults. J. Clin. Exp. Neuropsychol. 2014, 36, 368–378. [Google Scholar] [CrossRef]
- Piccinini, G.; Imbimbo, I.; Ricciardi, D.; Coraci, D.; Santilli, C.; Lo Monaco, M.R.; Loreti, C.; Vulpiani, M.C.; Silveri, M.C.; Padua, L. The Impact of Cognitive Reserve on the Effectiveness of Balance Rehabilitation in Parkinson’s Disease. Eur. J. Phys. Rehabil. Med. 2018, 54, 554–559. [Google Scholar] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Metitieri, T.; Geroldi, C.; Pezzini, A.; Frisoni, G.B.; Bianchetti, A.; Trabucchi, M. The Itel-MMSE: An Italian Telephone Version of the Mini-Mental State Examination. Int. J. Geriatr. Psychiatry 2001, 16, 166–167. [Google Scholar] [CrossRef]
- Katz, S. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A Standard Procedure for Creating a Frailty Index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Nucci, M.; Mapelli, D.; Mondini, S. Cognitive Reserve Index Questionnaire (CRIq): A New Instrument for Measuring Cognitive Reserve. Aging Clin. Exp. Res. 2012, 24, 218–226. [Google Scholar]
- Colombo, L.; Sartori, G.; Brivio, C. Stima del quoziente intellettivo tramite l’applicazione del TIB (Test di Intelligenza Breve). G. Ital. Psicol. 2000, 3, 613–637. [Google Scholar]
- Nelson, H.E.; O’Connell, A. Dementia: The Estimation of Premorbid Intelligence Levels Using the New Adult Reading Test. Cortex 1978, 14, 234–244. [Google Scholar] [CrossRef]
- Colombo, L.; Brivio, C.; Benaglio, I.; Siri, S.; Cappa, S.F. Alzheimer patients’ ability to read words with irregular stress. Cortex 2000, 36, 703–714. [Google Scholar] [CrossRef]
- McGurn, B.; Deary, I.J.; Starr, J.M. Childhood Cognitive Ability and Risk of Late-Onset Alzheimer and Vascular Dementia. Neurology 2008, 71, 1051–1056. [Google Scholar] [CrossRef] [Green Version]
- Basile, G.; Sardella, A. From Cognitive to Motor Impairment and from Sarcopenia to Cognitive Impairment: A Bidirectional Pathway towards Frailty and Disability. Aging Clin. Exp. Res. 2021, 33, 469–478. [Google Scholar] [CrossRef]
- Guzzetti, S.; Mancini, F.; Caporali, A.; Manfredi, L.; Daini, R. The Association of Cognitive Reserve with Motor and Cognitive Functions for Different Stages of Parkinson’s Disease. Exp. Gerontol. 2019, 115, 79–87. [Google Scholar] [CrossRef]
- Meiner, Z.; Ayers, E.; Verghese, J. Motoric Cognitive Risk Syndrome: A Risk Factor for Cognitive Impairment and Dementia in Different Populations. Ann. Geriatr. Med. Res. 2020, 24, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Wang, C.; Lipton, R.; Verghese, J. The Protective Effects of Executive Functions and Episodic Memory on Gait Speed Decline in Aging Defined in the Context of Cognitive Reserve. J. Am. Geriatr. Soc. 2012, 60, 2093–2098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, T.L.; Gogniat, M.A.; Jean, K.R.; Miller, L.S. Pre-Morbid IQ Moderates the Relationship between Cognitive Performance and Performance-Based Functional Status in Older Adults. Clin. Gerontol. 2020, 1–11. [Google Scholar] [CrossRef]
- Yam, A.; Marsiske, M. Cognitive Longitudinal Predictors of Older Adults’ Self-Reported IADL Function. J. Aging Health 2013, 25 (Suppl. 8), 163S–185S. [Google Scholar] [CrossRef] [Green Version]
- Gross, A.L.; Rebok, G.W.; Unverzagt, F.W.; Willis, S.L.; Brandt, J. Cognitive Predictors of Everyday Functioning in Older Adults: Results from the ACTIVE Cognitive Intervention Trial. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Malmstrom, T.K.; Miller, D.K. A Simple Frailty Questionnaire (FRAIL) Predicts Outcomes in Middle Aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Basile, G.; Catalano, A.; Mandraffino, G.; Maltese, G.; Alibrandi, A.; Ciancio, G.; Brischetto, D.; Morabito, N.; Lasco, A.; Cesari, M. Frailty Modifications and Prognostic Impact in Older Patients Admitted in Acute Care. Aging Clin. Exp. Res. 2018, 31, 151–155. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Lyall, D.M.; Gray, S.R.; Esteban-Cornejo, I.; Quinn, T.J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Associations between physical frailty and dementia incidence: A prospective study from UK Biobank. Lancet Healthy Longev. 2020, 1, e58–e68. [Google Scholar] [CrossRef]
- Canevelli, M.; Cesari, M. Cognitive Frailty: Far from Clinical and Research Adoption. J. Am. Med. Dir. Assoc. 2017, 18, 816–818. [Google Scholar] [CrossRef] [PubMed]
- Devita, M.; Mondini, S.; Bordignon, A.; Sergi, G.; Girardi, A.; Manzato, E.; Mapelli, D.; Coin, A. The Importance of Cognitive Reserve in Comprehensive Geriatric Assessment for Dementia. Aging Clin. Exp. Res. 2020, 32, 1179–1181. [Google Scholar] [CrossRef]
- Sardella, A.; Quattropani, M.C.; Basile, G. Can Cognitive Reserve Protect Frail Individuals from Dementia? Lancet Healthy Longev. 2021, 2, e67. [Google Scholar] [CrossRef]
- Grande, G.; Triolo, F.; Nuara, A.; Welmer, A.-K.; Fratiglioni, L.; Vetrano, D.L. Measuring Gait Speed to Better Identify Prodromal Dementia. Exp. Gerontol. 2019, 124, 110625. [Google Scholar] [CrossRef]
- Zammit, A.R.; Piccinin, A.M.; Duggan, E.C.; Koval, A.; Clouston, S.; Robitaille, A.; Brown, C.L.; Handschuh, P.; Wu, C.; Jarry, V.; et al. A Coordinated Multi-Study Analysis of the Longitudinal Association between Handgrip Strength and Cognitive Function in Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapko, D.; McCormack, R.; Black, C.; Staff, R.; Murray, A. Life-Course Determinants of Cognitive Reserve (CR) in Cognitive Aging and Dementia—A Systematic Literature Review. Aging Ment. Health 2018, 22, 915–926. [Google Scholar] [CrossRef]
- Giogkaraki, E.; Michaelides, M.P.; Constantinidou, F. The Role of Cognitive Reserve in Cognitive Aging: Results from the Neurocognitive Study on Aging. J. Clin. Exp. Neuropsychol. 2013, 35, 1024–1035. [Google Scholar] [CrossRef]
- Kartschmit, N.; Mikolajczyk, R.; Schubert, T.; Lacruz, M.E. Measuring Cognitive Reserve (CR)—A Systematic Review of Measurement Properties of CR Questionnaires for the Adult Population. PLoS ONE 2019, 14, e0219851. [Google Scholar] [CrossRef]
- Arcara, G.; Mondini, S.; Bisso, A.; Palmer, K.; Meneghello, F.; Semenza, C. The Relationship between Cognitive Reserve and Math Abilities. Front. Aging Neurosci. 2017, 9, 429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puccioni, O.; Vallesi, A. High Cognitive Reserve Is Associated with a Reduced Age-Related Deficit in Spatial Conflict Resolution. Front. Hum. Neurosci. 2012, 6, 327. [Google Scholar] [CrossRef] [Green Version]
- Ciccarelli, N.; Monaco, M.R.L.; Fusco, D.; Vetrano, D.L.; Zuccalà, G.; Bernabei, R.; Brandi, V.; Pisciotta, M.S.; Silveri, M.C. The Role of Cognitive Reserve in Cognitive Aging: What We Can Learn from Parkinson’s Disease. Aging Clin. Exp. Res. 2018, 30, 877–880. [Google Scholar] [CrossRef] [PubMed]
- Volpi, L.; Pagni, C.; Radicchi, C.; Cintoli, S.; Miccoli, M.; Bonuccelli, U.; Tognoni, G. Detecting Cognitive Impairment at the Early Stages: The Challenge of First Line Assessment. J. Neurol. Sci. 2017, 377, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P.; Montagnese, S.; Spinelli, G.; Schiff, S.; Mapelli, D. Cognitive Reserve Is a Resilience Factor for Cognitive Dysfunction in Hepatic Encephalopathy. Metab. Brain Dis. 2017, 32, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Mondini, S.; Madella, I.; Zangrossi, A.; Bigolin, A.; Tomasi, C.; Michieletto, M.; Villani, D.; Di Giovanni, G.; Mapelli, D. Cognitive Reserve in Dementia: Implications for Cognitive Training. Front. Aging Neurosci. 2016, 8, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caffò, A.O.; Lopez, A.; Spano, G.; Saracino, G.; Stasolla, F.; Ciriello, G.; Grattagliano, I.; Lancioni, G.E.; Bosco, A. The Role of Pre-Morbid Intelligence and Cognitive Reserve in Predicting Cognitive Efficiency in a Sample of Italian Elderly. Aging Clin. Exp. Res. 2016, 28, 1203–1210. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sociodemographic characteristics 1 | |
| Age (years) | 80.31 ± 6.84 |
| Gender 2 Male (n, %) Female (n, %) | 42 (29.8) |
| 99 (70.2) | |
| Education (years) | 7.09 (± 3.83) |
| Marital status Married (n, %) Widow/er (n, %) Other (n, %) | 71 (50.4) |
| 56 (39.7) | |
| 14 (9.9) | |
| Clinical features 1 | |
| MMSE | 22.61 (± 4.52) |
| Handgrip (kg) | 17.25 (± 7.14) |
| Gait speed (m/s) | 0.64 (± 0.19) |
| BADL 3 | 4.23 (± 1.59) |
| IADL 3 | 3.67 (± 2.41) |
| FI | 0.25 (± 0.11) |
| Frailty status 4 Frail (n, %) Not frail (n, %) | 71 (50.4) |
| 70 (49.6) | |
| CRIq | 83.33 (± 14.53) |
| TIB | 96.34 (± 13.63) |
| CRIq | TIB | |||||||
|---|---|---|---|---|---|---|---|---|
| B | β | t | p | B | β | t | p | |
| Handgrip | 0.170 | 0.346 | 4.35 | <0.001 | 0.042 | 0.081 | 0.95 | 0.34 |
| Gait speed | 0.002 | 0.185 | 2.20 | 0.029 | 0.002 | 0.117 | 1.37 | 0.17 |
| BADL | 0.024 | 0.221 | 2.66 | 0.009 | 0.008 | 0.072 | 0.85 | 0.39 |
| IADL | 0.045 | 0.272 | 3.32 | 0.001 | 0.037 | 0.211 | 2.54 | 0.012 |
| FI | −0.002 | −0.290 | −3.56 | <0.001 | −0.001 | −0.161 | −1.91 | 0.0571 |
| Model Summary | Coefficients | ||||||
|---|---|---|---|---|---|---|---|
| Step | R2 | F | p | β | t | p | |
| Step 1 | 0.084 | 4.12 | 0.008 | ||||
| Age | −0.118 | −1.43 | 0.15 | ||||
| Gender 1 | −0.180 | −2.11 | 0.036 | ||||
| Education | 0.157 | 1.84 | 0.067 | ||||
| Step 2 | 0.173 | 5.58 | <0.001 | ||||
| Age | −0.19 | −0.22 | 0.82 | ||||
| Gender 1 | 0.066 | 0.058 | 0.95 | ||||
| Education | 0.128 | 1.56 | 0.12 | ||||
| Handgrip | 0.244 | 2.29 | 0.023 | ||||
| Gait speed | 0.197 | 2.29 | 0.023 | ||||
| Step 3 | 0.307 | 8.28 | <0.001 | ||||
| Age | −0.029 | −0.37 | 0.70 | ||||
| Gender 1 | 0.164 | 1.61 | 0.10 | ||||
| Education | 0.283 | 2.46 | 0.015 | ||||
| Handgrip | 0.287 | 2.90 | 0.004 | ||||
| Gait speed | 0.145 | 1.80 | 0.073 | ||||
| CRIq | 0.418 | 3.36 | 0.001 | ||||
| TIB | 0.271 | 3.14 | 0.002 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quattropani, M.C.; Sardella, A.; Morgante, F.; Ricciardi, L.; Alibrandi, A.; Lenzo, V.; Catalano, A.; Squadrito, G.; Basile, G. Impact of Cognitive Reserve and Premorbid IQ on Cognitive and Functional Status in Older Outpatients. Brain Sci. 2021, 11, 824. https://doi.org/10.3390/brainsci11070824
Quattropani MC, Sardella A, Morgante F, Ricciardi L, Alibrandi A, Lenzo V, Catalano A, Squadrito G, Basile G. Impact of Cognitive Reserve and Premorbid IQ on Cognitive and Functional Status in Older Outpatients. Brain Sciences. 2021; 11(7):824. https://doi.org/10.3390/brainsci11070824
Chicago/Turabian StyleQuattropani, Maria C., Alberto Sardella, Francesca Morgante, Lucia Ricciardi, Angela Alibrandi, Vittorio Lenzo, Antonino Catalano, Giovanni Squadrito, and Giorgio Basile. 2021. "Impact of Cognitive Reserve and Premorbid IQ on Cognitive and Functional Status in Older Outpatients" Brain Sciences 11, no. 7: 824. https://doi.org/10.3390/brainsci11070824
APA StyleQuattropani, M. C., Sardella, A., Morgante, F., Ricciardi, L., Alibrandi, A., Lenzo, V., Catalano, A., Squadrito, G., & Basile, G. (2021). Impact of Cognitive Reserve and Premorbid IQ on Cognitive and Functional Status in Older Outpatients. Brain Sciences, 11(7), 824. https://doi.org/10.3390/brainsci11070824