
Patterns of Restricted and Repetitive Behaviors in Autism Spectrum Disorders: A Cross-Sectional Video Recording Study. Preliminary Report



 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
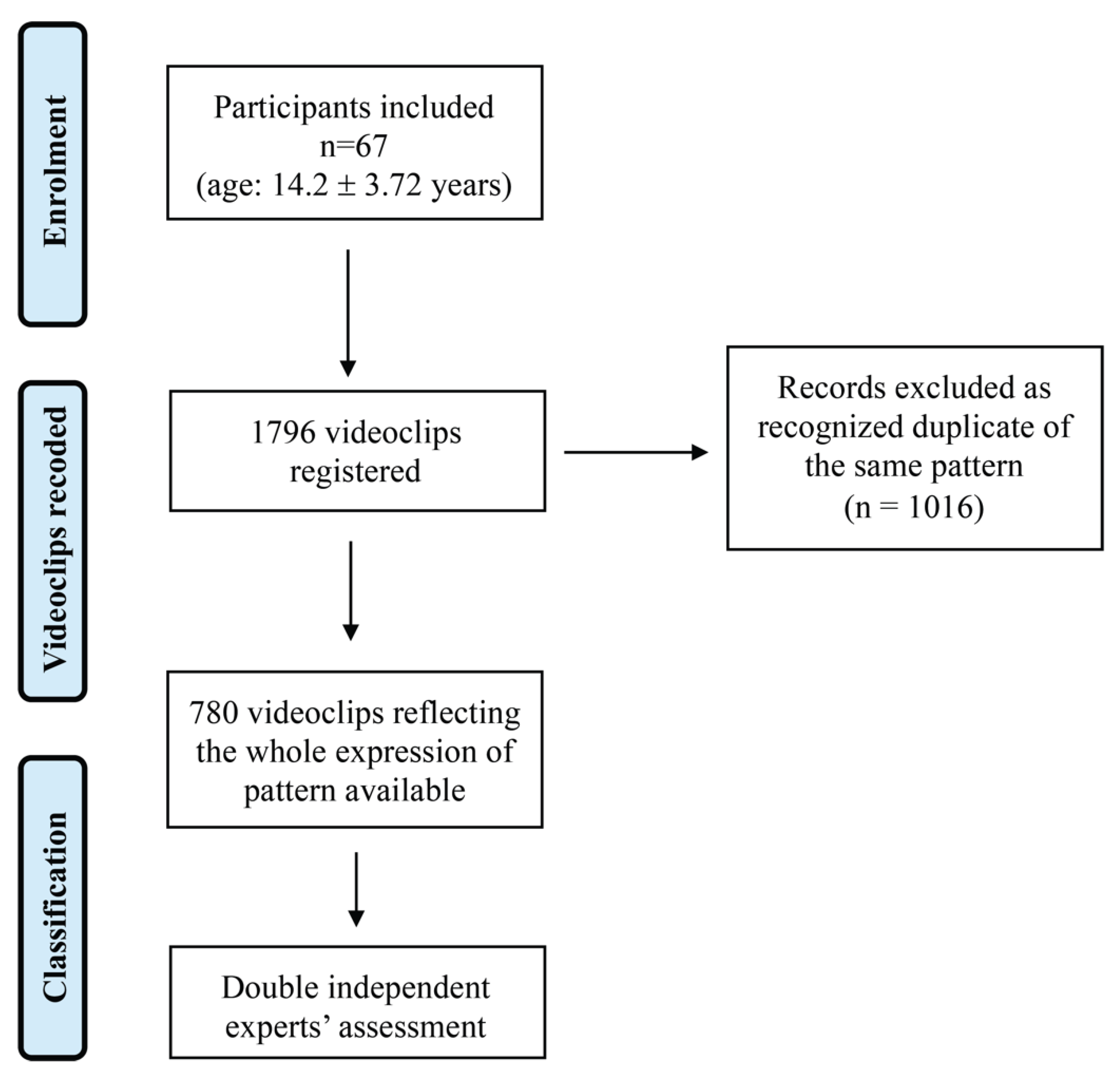
2.1. Participants
2.2. Procedures
- Simple Motor (M1): behavior consisting of one movement (e.g., finger tapping or hand waving, repetitive limb movements, body rocking, etc.);
- Complex Motor (M2): behavior consisting of repeated sequences of movements in several body districts (e.g., toe walking, jumping while walking or running, etc.);
- Simple Sensory (S1): involves a single sensorial aspect (e.g., touching an object or a surface, licking body parts or objects, etc.);
- Complex Sensory (S2): involves different sensory channels (e.g., grasping small items from the floor and put them in the mouth);
- Simple Vocal (V1): repeated simple vocalizations or “noises” (e.g., emitting grunt, raspberries, clearing throat, blowing, etc.);
- Complex Vocal (V2): repeating words phonemes, echolalia, coprolalia;
- Intellective: rigid, repetitive, stereotyped behaviors that express a need for routine, resistance to change, and a tendency to maintain environmental immutability. The Intellective domain was further divided between simple and complex behaviors as follows:
- Simple Intellective (I1): simple rituals of rigid and repetitive behaviors that express a need for routine, resistance to change, e.g., crumble the food before eating it; always put the glass in the same place, keep the door of the cupboard open in the same way.
- Complex Intellective (I2): complex ritual from the point of view of the reiterated behavioral sequence, e.g., trashing items while following the same path, line up different objects in the same order, etc.
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Number of RRBs and Autism Severity
4.2. Pattern of RRB and Autism Severity
4.3. Measuring RRBs in Individuals with ASD
4.4. Study Limitations and Strengths
4.5. Directions for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turner, M. Annotation: Repetitive Behaviour in Autism: A Review of Psychological Research. J. Child. Psychol. Psychiatry 1999, 40, 839–849. [Google Scholar] [CrossRef]
- Cunningham, A.B.; Schreibman, L. Stereotypy in autism: The importance of function. Res. Autism Spectr. Disord. 2008, 2, 469–479. [Google Scholar] [CrossRef]
- Melo, C.; Ruano, L.; Jorge, J.; Ribeiro, T.P.; Oliveira, G.; Azevedo, L.; Temudo, T. Prevalence and determinants of motor stereotypies in autism spectrum disorder: A systematic review and meta-analysis. Autism 2020, 24, 569–590. [Google Scholar] [CrossRef]
- Lutz, C.K. Stereotypic Behavior in Nonhuman Primates as a Model for the Human Condition. ILAR J. 2014, 55, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.; Tordjman, S.; Baumann, C.; Burglen, L.; Excoffier, E.; Lazar, G.; Mazet, P.; Verloes, A. Specific Genetic Disorders and Autism: Clinical Contribution Towards their Identification. J. Autism Dev. Disord. 2005, 35, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Langen, M.; Durston, S.; Kas, M.J.; van Engeland, H.; Staal, W.G. The neurobiology of repetitive behavior: …and men. Neurosci. Biobehav. Rev. 2011, 35, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Leekam, S.R.; Prior, M.R.; Uljarevic, M. Restricted and repetitive behaviors in autism spectrum disorders: A review of research in the last decade. Psychol. Bull. 2011, 137, 562–593. [Google Scholar] [CrossRef]
- Singer, H.S. Motor Stereotypies. Semin. Pediatr. Neurol. 2009, 16, 77–81. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Howell, C.T.; Mcconaughy, S.H.; Stanger, C. Six-Year Predictors of Problems in a National Sample: IV. Young Adult Signs of Disturbance. J. Am. Acad. Child. Adolesc. Psychiatry 1998, 37, 718–727. [Google Scholar] [CrossRef]
- MacDonald, R.; Green, G.; Mansfield, R.; Geckeler, A.; Gardenier, N.; Anderson, J.; Holcomb, W.; Sanchez, J. Stereotypy in young children with autism and typically developing children. Res. Dev. Disabil. 2007, 28, 266–277. [Google Scholar] [CrossRef]
- Robinson, S.; Woods, M.; Cardona, F.; Hedderly, T. Intense Imagery Movements (IIM): More to motor stereotypies than meets the eye. Eur. J. Paediatr. Neurol. 2016, 20, 61–68. [Google Scholar] [CrossRef]
- Sallustro, F.; Atwell, C.W. Body rocking, head banging, and head rolling in normal children. J. Pediatr. 1978, 93, 704–708. [Google Scholar] [CrossRef]
- De Lissovoy, V. Head banging in early childhood: A study of incidence. J. Pediatr. 1961, 58, 803–805. [Google Scholar] [CrossRef]
- Berkson, G.; Tupa, M. Early Development of Stereotyped and Self-Injurious Behaviors. J. Early Interv. 2016, 23, 1–19. [Google Scholar] [CrossRef]
- Harris, K.; Mahone, E.M.; Singer, H.S. Nonautistic Motor Stereotypies: Clinical Features and Longitudinal Follow-Up. Pediatr. Neurol. 2008, 38, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Oakley, C.; Mahone, E.M.; Morris-Berry, C.; Kline, T.; Singer, H.S. Primary Complex Motor Stereotypies in Older Children and Adolescents: Clinical Features and Longitudinal Follow-Up. Pediatr. Neurol. 2015, 52, 398–403.e39. [Google Scholar] [CrossRef] [PubMed]
- Chebli, S.S.; Martin, V.; Lanovaz, M.J. Prevalence of Stereotypy in Individuals with Developmental Disabilities: A Systematic Review. Rev. J. Autism Dev. Disord. 2016, 3, 107–118. [Google Scholar] [CrossRef]
- Perin, C.; Valagussa, G.; Mazzucchelli, M.; Gariboldi, V.; Cerri, C.G.; Meroni, R.; Grossi, E.; Cornaggia, C.M.; Menant, J.; Piscitelli, D. Physiological Profile Assessment of Posture in Children and Adolescents with Autism Spectrum Disorder and Typically Developing Peers. Brain Sci. 2020, 10, 681. [Google Scholar] [CrossRef]
- American Psychiatric Association. DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; p. 947. [Google Scholar]
- Burns, C.O.; Matson, J.L. An evaluation of the clinical application of the DSM-5 for the diagnosis of autism spectrum disorder. Expert Rev. Neurother. 2017, 17, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Dempsey, T.; Fodstad, J.C. Stereotypies and repetitive/restrictive behaviours in infants with autism and pervasive developmental disorder. Dev. Neurorehabilit. 2009, 12, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Péter, Z.; Oliphant, M.E.; Fernandez, T.V. Motor Stereotypies: A Pathophysiological Review. Front. Neurosci. 2017, 11, 171. [Google Scholar] [CrossRef] [PubMed]
- Unal, C.T.; Beverley, J.A.; Willuhn, I.; Steiner, H. Long-lasting dysregulation of gene expression in corticostriatal circuits after repeated cocaine treatment in adult rats: Effects onzif 268andhomer 1a. Eur. J. Neurosci. 2009, 29, 1615–1626. [Google Scholar] [CrossRef] [PubMed]
- Canales, J.J.; Graybiel, A.M. A measure of striatal function predicts motor stereotypy. Nat. Neurosci. 2000, 3, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Imeh-Nathaniel, A.; Rincon, N.; Orfanakos, V.B.; Brechtel, L.; Wormack, L.; Richardson, E.; Huber, R.; Nathaniel, T.I. Effects of chronic cocaine, morphine and methamphetamine on the mobility, immobility and stereotyped behaviors in crayfish. Behav. Brain Res. 2017, 332, 120–125. [Google Scholar] [CrossRef]
- Cinque, S.; Zoratto, F.; Poleggi, A.; Leo, D.; Cerniglia, L.; Cimino, S.; Tambelli, R.R.; Alleva, E.; Gainetdinov, R.; Laviola, G.; et al. Behavioral Phenotyping of Dopamine Transporter Knockout Rats: Compulsive Traits, Motor Stereotypies, and Anhedonia. Front. Psychiatry 2018, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Bouchekioua, Y.; Tsutsui-Kimura, I.; Sano, H.; Koizumi, M.; Tanaka, K.; Yoshida, K.; Kosaki, Y.; Watanabe, S.; Mimura, M. Striatonigral direct pathway activation is sufficient to induce repetitive behaviors. Neurosci. Res. 2018, 132, 53–57. [Google Scholar] [CrossRef]
- Harris, A.D.; Singer, H.S.; Horska, A.; Kline, T.; Ryan, M.; Edden, R.A.E.; Mahone, E.M. GABA and Glutamate in Children with Primary Complex Motor Stereotypies: An1H-MRS Study at 7T. AJNR Am. J. Neuroradiol. 2015, 37, 552–557. [Google Scholar] [CrossRef]
- Goldman, S.; O’Brien, L.M.; Filipek, P.A.; Rapin, I.; Herbert, M.R. Motor stereotypies and volumetric brain alterations in children with Autistic Disorder. Res. Autism Spectr. Disord. 2013, 7, 82–92. [Google Scholar] [CrossRef]
- Scahill, L.; Aman, M.G.; Lecavalier, L.; Halladay, A.K.; Bishop, S.L.; Bodfish, J.W.; Grondhuis, S.; Jones, N.; Horrigan, J.P.; Cook, E.H.; et al. Measuring repetitive behaviors as a treatment endpoint in youth with autism spectrum disorder. Autism 2015, 19, 38–52. [Google Scholar] [CrossRef]
- Goldman, S.; Wang, C.; Salgado, M.W.; E Greene, P.; Kim, M.; Rapin, I. Motor stereotypies in children with autism and other developmental disorders. Dev. Med. Child. Neurol. 2009, 51, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Militerni, R.; Bravaccio, C.; Falco, C.; Fico, C.; Palermo, M.T. Repetitive behaviors in autistic disorder. Eur. Child. Adolesc. Psychiatry 2002, 11, 210–218. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. (ADOS-2) Manual (Part I): Modules 1–4. In Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Services: Torrance, ON, Canada, 2012. [Google Scholar]
- Randall, M.; Egberts, K.J.; Samtani, A.; Scholten, R.J.; Hooft, L.; Livingstone, N.; Sterling-Levis, K.; Woolfenden, S.; Williams, K. Diagnostic tests for autism spectrum disorder (ASD) in preschool children. Cochrane Database Syst. Rev. 2018, 7, CD009044. [Google Scholar] [CrossRef]
- Boyd, B.A.; McDonough, S.G.; Bodfish, J.W. Evidence-Based Behavioral Interventions for Repetitive Behaviors in Autism. J. Autism Dev. Disord. 2012, 42, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Lanzarini, E.; Pruccoli, J.; Grimandi, I.; Spadoni, C.; Angotti, M.; Pignataro, V.; Sacrato, L.; Franzoni, E.; Parmeggiani, A. Phonic and Motor Stereotypies in Autism Spectrum Disorder: Video Analysis and Neurological Characterization. Brain Sci. 2021, 11, 431. [Google Scholar] [CrossRef] [PubMed]
- Willemsen-Swinkels, S.H.N.; Buitelaar, J.K.; Dekker, M.; van Engeland, H. Subtyping stereotypic behavior in children: The association between stereotypic behavior, mood, and heart rate. J. Autism Dev. Disord. 1998, 28, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Akshoomoff, N.; Farid, N.; Courchesne, E.; Haas, R. Abnormalities on the Neurological Examination and EEG in Young Children with Pervasive Developmental Disorders. J. Autism Dev. Disord. 2007, 37, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.S.L.; Aman, M.G. The Repetitive Behavior Scale-Revised: Independent Validation in Individuals with Autism Spectrum Disorders. J. Autism Dev. Disord. 2007, 37, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Rivet, T.T. Characteristics of challenging behaviours in adults with autistic disorder, PDD-NOS, and intellectual disability. J. Intellect. Dev. Disabil. 2008, 33, 323–329. [Google Scholar] [CrossRef]
- Bodfish, J.W.; Symons, F.J.; Parker, D.E.; Lewis, M.H. Varieties of Repetitive Behavior in Autism: Comparisons to Mental Retardation. J. Autism Dev. Disord. 2000, 30, 237–243. [Google Scholar] [CrossRef]
- Bishop, S.L.; Richler, J.; Lord, C. Association Between Restricted and Repetitive Behaviors and Nonverbal IQ in Children with Autism Spectrum Disorders. Child. Neuropsychol. 2006, 12, 247–267. [Google Scholar] [CrossRef]
- Mirenda, P.; Smith, I.M.; Vaillancourt, T.; Georgiades, S.; Duku, E.; Szatmari, P.; Bryson, S.E.; Fombonne, E.; Roberts, W.L.; Volden, J.; et al. Validating the Repetitive Behavior Scale-Revised in Young Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2010, 40, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Joseph, L.; Thurm, A.; Farmer, C.; Shumway, S. Repetitive behavior and restricted interests in young children with autism: Comparisons with controls and stability over 2 years. Autism Res. 2013, 6, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.J.; Botteron, K.N.; Dager, S.R.; Elison, J.T.; Estes, A.M.; Gu, H.; Hazlett, H.C.; Pandey, J.; Paterson, S.J.; Schultz, R.T.; et al. Longitudinal patterns of repetitive behavior in toddlers with autism. J. Child. Psychol. Psychiatry 2014, 55, 945–953. [Google Scholar] [CrossRef]
- Goldman, S.; Greene, P.E. Stereotypies in autism: A video demonstration of their clinical variability. Front. Integr. Neurosci. 2013, 6, 121. [Google Scholar] [CrossRef] [PubMed]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Fleischmann, R.L.; Hill, C.L.; Heninger, G.R.; Charney, D.S. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch. Gen. Psychiatry 1989, 46, 1006–1011. [Google Scholar] [CrossRef]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Delgado, P.; Heninger, G.R.; Charney, D.S. The Yale-Brown Obsessive Compulsive Scale. II. Validity. Arch. Gen. Psychiatry 1989, 46, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Scahill, L.; Riddle, M.A.; McSwiggin-Hardin, M.; Ort, S.I.; King, R.A.; Goodman, W.K.; Cicchetti, D.; Leckman, J.F. Children’s Yale-Brown Obsessive Compulsive Scale: Reliability and Validity. J. Am. Acad. Child. Adolesc. Psychiatry 1997, 36, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.W.; Leckman, J.F.; Carter, A.; Reznick, J.S.; Henshaw, D.; King, R.A.; Pauls, D. Ritual, habit, and perfectionism: The prevalence and development of compulsive-like behavior in normal young children. Child Dev. 1997, 68, 58–68. [Google Scholar] [CrossRef]
- Turner, M. Towards an executive dysfunction account of repetitive behaviour in autism. In Autism as an Executive Disorder; Oxford University Press: Oxford, UK, 2015; pp. 57–100. [Google Scholar]
- Rutter, M.; le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised Manual; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Piscitelli, D.; Pellicciari, L. Responsiveness: Is it time to move beyond ordinal scores and approach interval measurements? Clin. Rehabil. 2018, 32, 1426–1427. [Google Scholar] [CrossRef]


{kind=link}
| Age Range—Years | 7.1—24.8 |
|---|---|
| Mean Age—years (SD) | 14.2 (3.72) |
| Male n. (%) | 58 (82%) |
| Female n. (%) | 9 (18%) |
| Mean ADOS Total score (SA + RRB) (SD) | 21.14 (5.34) |
| Mean ADOS CSS (SD) | 7.93 (1.72) |
| ADOS CSS Range [Min, Max] | 6 [4,10] |
| ADOS CSS—high severity n. subjects (%) | 39 (58%) |
| ADOS CSS—moderate severity n. subjects (%) | 26 (39%) |
| ADOS CSS—low severity n. subjects (%) | 2 (3%) |
| Epilepsy co-occurrence | 10 (15%) |
| Intellectual disability—mild n. subjects (%) | 3 (4.48%) |
| Intellectual disability—moderate n. subjects (%) | 19 (28.36%) |
| Intellectual disability—severe n. subjects (%) | 44 (65.67%) |
| Intellectual disability—profound n. subjects (%) | 1 (1.49%) |
| RRBs Pattern | Frequency | RRBs Pattern | Frequency |
|---|---|---|---|
| M1 S1 | 23.08% | V2 | 0.51% |
| M1 | 8.97% | M2 S1 I1 | 0.51% |
| S1 | 7.95% | S2 I1 | 0.38% |
| M2 S1 | 7.95% | M2 S2 I1 | 0.38% |
| I2 | 4.62% | I2 V1 | 0.38% |
| M2 | 4.36% | I1 V2 | 0.26% |
| M2 S2 | 3.97% | M2 S2 V2 | 0.26% |
| S2 M1 | 3.97% | V2 S1 I1 | 0.26% |
| I1 | 3.59% | I2 S1 M2 | 0.26% |
| M1 S1 V1 | 3.08% | M2 V1 I1 | 0.26% |
| S2 | 2.44% | S1 V2 | 0.13% |
| S2 M2 V1 | 2.31% | M1 V2 | 0.13% |
| I1 M1 | 2.18% | S2 M1 I1 | 0.13% |
| S1 V1 | 2.18% | M2 I1 V2 | 0.13% |
| M1 V1 | 1.67% | M2 V2 | 0.13% |
| M2 V1 | 1.67% | M1 S2 V2 | 0.13% |
| M2 S1 V1 | 1.54% | I2 S2 V2 | 0.13% |
| S1 I1 | 1.41% | I2 M2 S1 V1 | 0.13% |
| S2 M1 V1 | 1.41% | M2 S1 V2 | 0.13% |
| I1 M2 | 1.41% | M2 S2 V2 I1 | 0.13% |
| S2 V1 | 1.28% | I2 S2 M2 | 0.13% |
| M1 S1 I1 | 1.15% | I1 M1 V1 | 0.13% |
| I2 M2 | 0.90% | M1 V1 S1 I1 | 0.13% |
| I2 S1 | 0.90% | M2 S1 V1 I1 | 0.13% |
| V1 | 0.64% | M1 V1 I1 S2 | 0.13% |
| N | Percentage | |
|---|---|---|
| Body as a whole | 222 | 39.0% |
| Upper limb | 209 | 36.7% |
| Mouth | 58 | 10.2% |
| Hands | 57 | 10.0% |
| Head | 37 | 6.5% |
| Eyes | 22 | 3.9% |
| Face | 17 | 3.0% |
| Ears | 15 | 2.6% |
| Tongue | 7 | 1.2% |
| Trunk | 7 | 1.2% |
| Nose | 6 | 1.1% |
| Feet | 5 | 0.9% |
| Fingers | 5 | 0.9% |
| Lower arms | 3 | 0.5% |
| Teeth | 2 | 0.4% |
| Variable | RRBs Low Number (n = 10) | RRBs High Number (n = 11) | Test | p-Value |
|---|---|---|---|---|
| Mean Age (SD) | 14.5 (4.57) | 13.8 (3.48) | T = −0.38 | 0.70 |
| Male | 8 (80%) | 9 (82%) | χ2 = 0.0112 | 0.91 |
| Female | 2 (20%) | 2 (18%) | ||
| Mean ADOS CSS (SD) | 7.2 (1.68) | 8.7 (1.55) | t = −2.16 | 0.044 * |
| Intellectual Disability | χ2 = 6.20454 | 0.045 * | ||
| Moderate | 5 | 1 | ||
| Severe | 4 | 10 | ||
| Profound | 1 | - |
| Variable | Simple Pattern Group (n = 40) | Complex Pattern Group (n = 27) | Test | p-Value |
|---|---|---|---|---|
| Mean Age (SD) | 13.87 (3.88) | 13.66 (3.47) | t = −0.22 | 0.81 |
| Male | 36 (90%) | 22 (81%) | χ2 = 1.0059 | 0.32 |
| Female | 4 (10%) | 5 (19%) | ||
| Mean number of RRB (SD) | 12.21 (7.82) | 10.85 (5.43) | t = −0.79 | 0.43 |
| Mean ADOS CSS (SD) | 7.63 (1.88) | 8.07 (1.26) | t = 1.06 | 0.29 |
| Intellectual Disability | χ2 = 2.8778 | 0.044 * | ||
| Mild | 3 (7.5%) | - | ||
| Moderate | 11 (27.5%) | 8 (29.6%) | ||
| Severe | 25 (62.5%) | 19 (70.4%) | ||
| Profound | 1 (2.5%) | - |
| Variables | N Stereotypies Per Subject | N Simple RRBs | N Complex RRBs | Age | ADOS SA | ADOS RRBs | ADOS CSS |
|---|---|---|---|---|---|---|---|
| N RRBs per subject | - | ||||||
| N Simple RRBs | 0.809 * | - | |||||
| N Complex RRBs | 0.684 * | 0.126 | - | ||||
| Age | 0.102 | 0.093 | 0.057 | - | |||
| ADOS SA | 0.245 | 0.141 | 0.239 | −0.025 | - | ||
| ADOS RRBs | 0.425 * | 0.210 | 0.458 * | 0.148 | 0.500 * | - | |
| ADOS CSS | 0.376 * | 0.232 | 0.347 * | 0.094 | 0.817 * | 0.757 * | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grossi, E.; Caminada, E.; Goffredo, M.; Vescovo, B.; Castrignano, T.; Piscitelli, D.; Valagussa, G.; Franceschini, M.; Vanzulli, F. Patterns of Restricted and Repetitive Behaviors in Autism Spectrum Disorders: A Cross-Sectional Video Recording Study. Preliminary Report. Brain Sci. 2021, 11, 678. https://doi.org/10.3390/brainsci11060678
Grossi E, Caminada E, Goffredo M, Vescovo B, Castrignano T, Piscitelli D, Valagussa G, Franceschini M, Vanzulli F. Patterns of Restricted and Repetitive Behaviors in Autism Spectrum Disorders: A Cross-Sectional Video Recording Study. Preliminary Report. Brain Sciences. 2021; 11(6):678. https://doi.org/10.3390/brainsci11060678
Chicago/Turabian StyleGrossi, Enzo, Elisa Caminada, Michela Goffredo, Beatrice Vescovo, Tristana Castrignano, Daniele Piscitelli, Giulio Valagussa, Marco Franceschini, and Franco Vanzulli. 2021. "Patterns of Restricted and Repetitive Behaviors in Autism Spectrum Disorders: A Cross-Sectional Video Recording Study. Preliminary Report" Brain Sciences 11, no. 6: 678. https://doi.org/10.3390/brainsci11060678
APA StyleGrossi, E., Caminada, E., Goffredo, M., Vescovo, B., Castrignano, T., Piscitelli, D., Valagussa, G., Franceschini, M., & Vanzulli, F. (2021). Patterns of Restricted and Repetitive Behaviors in Autism Spectrum Disorders: A Cross-Sectional Video Recording Study. Preliminary Report. Brain Sciences, 11(6), 678. https://doi.org/10.3390/brainsci11060678