
Physiological Reactions in the Therapist and Turn-Taking during Online Psychotherapy with Children and Adolescents with Autism Spectrum Disorder


 , ,
, , 
Abstract
1. Introduction
2. Method
2.1. Design
2.2. Participants
2.3. Instruments
2.4. Procedure
2.5. Data Analysis
3. Results
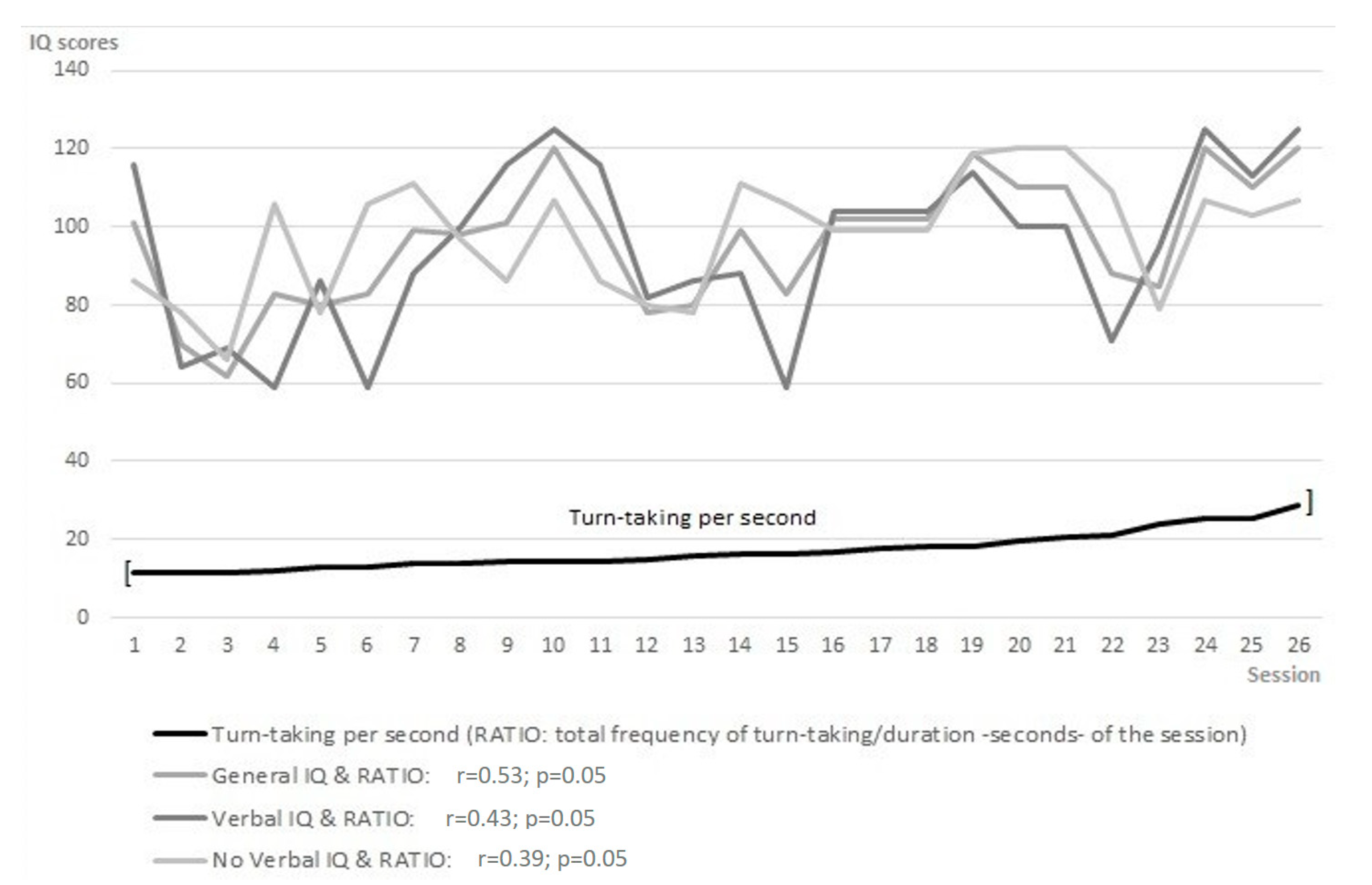
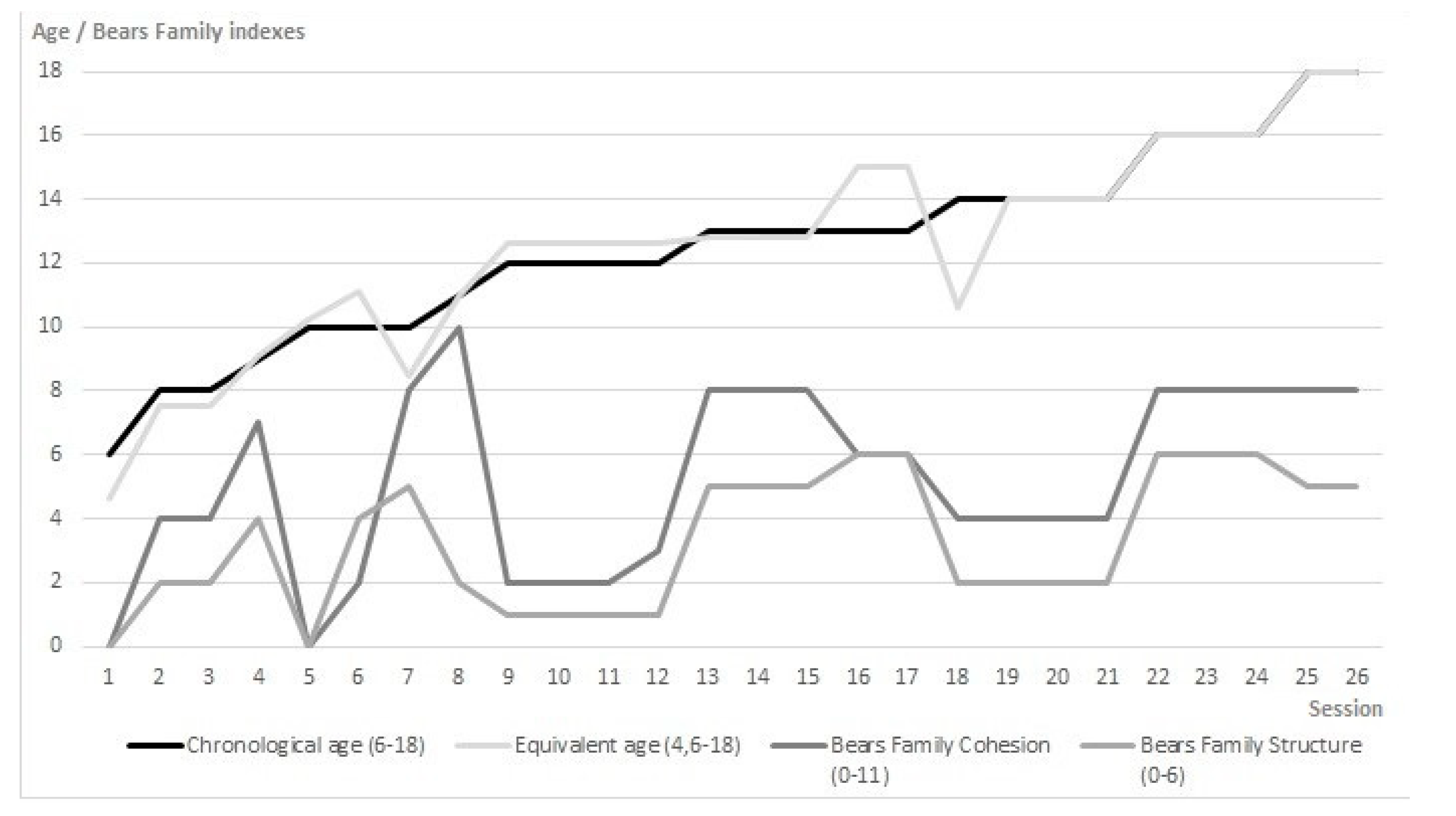
3.1. Changes in Turn-Taking per Second, Participants’ Intelligence, Age, Narrative, and Social Skills
3.2. Participants’ Difficulties and Turn-Taking with the Therapist
3.3. Therapist’s Heart Rate Variability (HRV) and Patient’s Turn-Taking Synchrony
4. Discussion
4.1. Changes in Turn-Taking per Second, Participants’ Intelligence, Age, Narrative, and Social Skills
4.2. Participants’ Difficulties and Turn-Taking with the Therapist
4.3. Therapist’s Heart Rate Variability (HRV) and Patient’s Turn-Taking Synchrony
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reda, M. Sistemi Cognitivi Complessi e Psicoterapia; La Nuova Italia Scientifica: Roma, Italy, 2001. [Google Scholar]
- Canestri, L.; della Lunga, S.D.; Reda, M.A. Correlaciones psicofisiológicas durante una sesión standard de psicoterapia entre paciente y terapeuta: Observaciones preliminares. Rev. Argent. Clin. Psicol. 2010, 19, 183–187. [Google Scholar]
- Ainsworth, M.D.S.; Bell, S.M.; Stayton, D.F. Infant-mother attachment and social development: Socialization as a product of reciprocal responsiveness to signals. In The Integration of a Child into a Social World; Cambridge University Press: Cambridge, UK, 1974; pp. 99–135. ISBN 0521203066. [Google Scholar]
- Belsky, J.; Rovine, M.; Taylor, D.G. The Pennsylvania Infant and Family Development Project, III: The origins of individual differences in infant-mother attachment: Maternal and infant contributions. Child Dev. 1984, 55, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Tronick, E.D.; Als, H.; Brazelton, T.B. Mutuality in Mother-Infant Interaction. J. Commun. 1977, 27, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Maccoby, E.E.; Martin, J. Socialization in the Context of the Family: Parent-Child Interaction. In Handbook of Child Psychology: {Vol}.~4. {Socialization}, Personality, and Social Development; Wiley: Hoboken, NJ, USA, 1983; pp. 1–101. [Google Scholar]
- Leclère, C.; Viaux, S.; Avril, M.; Achard, C.; Chetouani, M.; Missonnier, S.; Cohen, D. Why synchrony matters during mother-child interactions: A systematic review. PLoS ONE 2014, 9, e113571. [Google Scholar] [CrossRef] [PubMed]
- Venuti, P.; Bentenuto, A.; Cainelli, S.; Landi, I.; Suvini, F.; Tancredi, R.; Igliozzi, R.; Muratori, F. A joint behavioral and emotive analysis of synchrony in music therapy of children with autism spectrum disorders. Health Psychol. Rep. 2017, 2, 162–172. [Google Scholar] [CrossRef]
- Reda, M.; Mahoney, M. Cognitive Psychotherapies; Ballinger: Cambridge, MA, USA, 1984. [Google Scholar]
- Black, B.; Logan, A. Links between Communication Patterns in Mother-Child, Father-Child, and Child-Peer Interactions and Children’s Social Status. Child Dev. 1995, 66, 255–271. [Google Scholar] [CrossRef]
- Cole, P.M.; Hall, S.E.; Radzioch, A.M. Emotional dysregulation and the development of serious misconduct. In Biopsychosocial Regulatory Processes in the Development of Childhood Behavioral Problems; Cambridge University Press: Cambridge, UK, 2009; pp. 186–211. ISBN 9780511575877. [Google Scholar]
- Harrist, A.W.; Waugh, R.M. Dyadic synchrony: Its structure and function in children’s development. Dev. Rev. 2002, 22, 555–592. [Google Scholar] [CrossRef]
- Adolph, K.E.; Berger, S.E.; Borstein, M.H.; Lamb, M.E. Developmental Science: An Advanced Textbook; Psychology Press: London, UK, 2015. [Google Scholar]
- Feldman, R. Parent-infant synchrony: Biological foundations and developmental outcomes. Curr. Dir. Psychol. Sci. 2007, 16, 340–345. [Google Scholar] [CrossRef]
- Cohen, D. The developmental being. Modeling a probabilistic approach to child development and psychopathology. Neuropsychiatr. Enfance Adolesc. 2012, 60, S25–S26. [Google Scholar] [CrossRef]
- Calabrò, G.; Bizzego, A.; Cainelli, S.; Furlanello, C.; Venuti, P. M-MS: A Multi-Modal Synchrony Dataset to Explore Dyadic Interaction in ASD. In Smart Innovation, Systems and Technologies; Springer: Berlin/Heidelberg, Germany, 2021; Volume 184, pp. 543–553. [Google Scholar]
- Reda, M. Un approccio post-razionalista alla relazione in psicoterapia [A post-rationalist approach to the relationship in psychotherapy]. Quad. Psicoter. Cogn. 2006, 19, 36–40. [Google Scholar]
- Trevarthen, C. Conversations with a two-month-old. In Parent-Infant Psychodynamics: Wild Things, Mirrors and Ghosts; Taylor and Francis: Boca Raton, FL, USA, 2018; pp. 25–34. ISBN 9780429902925. [Google Scholar]
- Trevarthen, C.; Aitken, K.J. Infant Intersubjectivity: Research, Theory, and Clinical Applications. J. Child Psychol. Psychiatry 2001, 42, 3–48. [Google Scholar] [CrossRef] [PubMed]
- Hougaard, E. The therapeutic alliance–A conceptual analysis. Scand. J. Psychol. 1994, 35, 67–85. [Google Scholar] [CrossRef] [PubMed]
- Mundy, P.; Sigman, M. Specifying the nature of the social impairment in autism. In Autism: New Perspectives on Diagnosis, Nature, and Treatment; Guilford: New York, NY, USA, 1989; pp. 3–21. [Google Scholar]
- Hobson, R.P. What is autism? Psychiatr. Clin. 1991, 14, 1–17. [Google Scholar] [CrossRef]
- BOSA, C.A. As relações entre autismo, comportamento social e função executiva [The relationships between autism, social behavior and executive function]. Psicol. Reflexão Crítica 2001, 14, 281–287. [Google Scholar] [CrossRef]
- Bosa, C. Atenção compartilhada e identificação precoce do autismo [Shared attention and early identification of autism]. Psicol. Reflexão Crítica 2002, 15, 77–88. [Google Scholar] [CrossRef]
- Lyra, M.C. Desenvolvimento de um sistema de relações historicamente construído: Contribuições da comunicação no início da vida [Development of a historically constructed system of relationships: Contributions of communication in early life]. Psicol. Reflexão Crítica 2000, 13, 257–268. [Google Scholar] [CrossRef]
- Pantoja, A.P.F.; Nelson-Goens, G.C. Desenvolvimento da vida emocional durante o segundo ano de vida: Narrativas e sistemas dinâmicos [Development of emotional life during the second year of life: Narratives and dynamic systems]. Psicol. Reflexão Crítica 2000, 13, 269–280. [Google Scholar] [CrossRef]
- Elder, J.H.; Goodman, J.J. Social turn-taking of children with neuropsychiatric impairments and their parents. Compr. Child Adolesc. Nurs. 1996, 19, 249–261. [Google Scholar] [CrossRef]
- Azhari, A.; Leck, W.Q.; Gabrieli, G.; Bizzego, A.; Rigo, P.; Setoh, P.; Bornstein, M.H.; Esposito, G. Parenting Stress Undermines Mother-Child Brain-to-Brain Synchrony: A Hyperscanning Study. Sci. Rep. 2019, 9, 11407. [Google Scholar] [CrossRef]
- Carr, E.G.; Levin, L.; McConnachie, G.; Carlson, J.I.; Kemp, D.C.; Smith, C.E. Communication-Based Intervention for Problem Behavior; Paul H Brookes Publishing: Baltimore, MD, USA, 1994. [Google Scholar]
- Molini, D.; Fernandes, F. Intenção comunicativa e uso de instrumentos em crianças com distúrbios psiquiátricos. Pró-Fono R. Atual. Cient 2003, 149–158. [Google Scholar] [CrossRef]
- Tamarit, J.; De Dios, J.; Dominguez, S.; Escribano, L. Conductas desafiantes y autismo: Un analisis contextualizado. In La Atención a Alumnos con Necesidades Educativas Graves y Permanentes; Gobierno de Navarra: Pamplona, Spain, 1995; Volume 5, pp. 1–10. [Google Scholar]
- Pennington, B.F.; Ozonoff, S. Executive functions and developmental psychopathology. J. Child Psychol. Psychiatry Allied Discip. 1996, 37, 51–87. [Google Scholar] [CrossRef]
- Beisler, J.M.; Tsai, L.Y. A pragmatic approach to increase expressive language skills in young autistic children. J. Autism Dev. Disord. 1983, 13, 287–303. [Google Scholar] [CrossRef] [PubMed]
- Artigas, J. Language in autistic disorders. Rev. Neurol. 1999, 28, 118–123. [Google Scholar]
- Monfort, I. Communicatión y lenguaje: Bidireccionalidad en la interventión en niños con trastorno de espectro autista [Communication and language: Bidirectionality in intervention in children with autism spectrum disorder]. Rev. Neurol. 2009, 48, 53–56. [Google Scholar]
- Moreno-Flagge, N. Trastornos del lenguaje. Diagnóstico y tratamiento [Language disorders Diagnosis and treatment]. Rev. Neurol. 2013, 57, S85–S94. [Google Scholar]
- Golinkoff, R.M.; Can, D.D.; Soderstrom, M.; Hirsh-Pasek, K. (Baby)Talk to Me: The Social Context of Infant-Directed Speech and Its Effects on Early Language Acquisition. Curr. Dir. Psychol. Sci. 2015, 24, 339–344. [Google Scholar] [CrossRef]
- Fernandes, F.D.M. Sugestões de Procedimentos Terapêuticos de Linguagem em Distúrbios do Espectro Autístico [Suggestions for Therapeutic Language Procedures in Autistic Spectrum Disorders]; LIMONGI, S. C. O. (Org.); Guanabara-Koogan: Barueri, Brazil, 2003; pp. 55–65. [Google Scholar]
- Vallejo, M.; Jordán, C. Psicoterapia a través de internet: Recursos tecnológicos en la práctica de la psicoterapia [Psychotherapy through the Internet: Technological resources in the practice of psychotherapy]. Boletín Psicol. 2007, 91, 27–42. [Google Scholar]
- Suler, J. The online disinhibition effect. Cyberpsychol. Behav. 2004, 7, 321–326. [Google Scholar] [CrossRef]
- Suler, J.R. Psychotherapy in cyberspace: A 5-dimensional model of online and computer-mediated psychotherapy. Cyberpsychol. Behav. 2000, 3, 151–159. [Google Scholar] [CrossRef]
- Association, A.P. American Psychiatric Association. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9780890425541. [Google Scholar]
- Wing, L. Language, social, and cognitive impairments in autism and severe mental retardation. J. Autism Dev. Disord. 1981, 11, 31–44. [Google Scholar] [CrossRef]
- Wing, L. The Autistic Spectrum; Revised Edition; Hachette: New York, NY, USA, 2012; ISBN 9781472103895. [Google Scholar]
- García Peñas, J.J.; Domínguez Carral, J.; Pereira Bezanilla, E. Alteraciones de la sinaptogénesis en el autismo. Implicaciones etiopatogénicas y terapéuticas [Synaptogenesis disorders in autism. Aetiopathogenic and therapeutic implications]. Rev. Neurol. 2012, 54, 41. [Google Scholar]
- Ermer, J.; Dunn, W. The Sensory Profile: A Discriminant Analysis of Children with and Without Disabilities. Am. J. Occup. Ther. 1998, 52, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Watling, R.L.; Deitz, J.; White, O. Comparison of sensory profile scores of young children with and without autism spectrum disorders. Am. J. Occup. Ther. 2001, 55, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.; Lane, S.J. Diagnostic validity of sensory over-responsivity: A review of the literature and case reports. J. Autism Dev. Disord. 2008, 38, 516–529. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.B.; Dunn, W. Relationship between context and sensory processing in children with autism. Am. J. Occup. Ther. 2010, 64, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Happé, F.; Frith, U. The weak coherence account: Detail-focused cognitive style in autism spectrum disorders. J. Autism Dev. Disord. 2006, 36, 5–25. [Google Scholar] [CrossRef]
- Rumsey, J.M.; Creasey, H.; Stepanek, J.S.; Dorwart, R.; Patronas, N.; Hamburger, S.D.; Duara, R. Hemispheric asymmetries, fourth ventricular size, and cerebellar morphology in autism. J. Autism Dev. Disord. 1988, 18, 127–137. [Google Scholar] [CrossRef]
- Hughes, C.; Russell, J.; Robbins, T.W. Evidence for executive dysfunction in autism. Neuropsychologia 1994, 32, 477–492. [Google Scholar] [CrossRef]
- Ozonoff, S. Components of executive function in autism and other disorders. In Autism as an Executive Disorder; Oxford University Press: New York, NY, USA, 1997; pp. 179–211. ISBN 0198523491. [Google Scholar]
- Baron-Cohen, S.; Leslie, A.M.; Frith, U. Mechanical, behavioural and Intentional understanding of picture stories in autistic children. Br. J. Dev. Psychol. 1986, 4, 113–125. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Ring, H.A.; Wheelwright, S.; Bullmore, E.T.; Brammer, M.J.; Simmons, A.; Williams, S.C.R. Social intelligence in the normal and autistic brain: An fMRI study. Eur. J. Neurosci. 1999, 11, 1891–1898. [Google Scholar] [CrossRef]
- Leslie, A.M.; Frith, U. Autistic children’s understanding of seeing, knowing and believing. Br. J. Dev. Psychol. 1988, 6, 315–324. [Google Scholar] [CrossRef]
- Perner, J.; Frith, U.; Leslie, A.M.; Leekam, S.R. Exploration of the autistic child’s theory of mind: Knowledge, belief, and communication. Child Dev. 1989, 60, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Bruner, J.; Weisser, S. The Invention of Self: Autobiography and Its Forms; Literacy and Orality; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Guidano, V. Complexity of the Self: A developmental Approach to Psychopathology and Therapy; Guilford Press: New York, NY, USA, 1987. [Google Scholar]
- Solcoff, K.D.V. (Ed.) Memoria autobiográfica y espectro autista. In Autismo: Enfoques Actuales. Una guía para Padres y Profesionales de la Salud y la Educación; Intellectus Partners: San Francisco, CA, USA, 2001; pp. 151–194. [Google Scholar]
- Solcoff, K. ¿Fenomenología experimental de la memoria? La memoria autobiográfica entre el contexto y el significado [Autobiographical memory and autism spectrum]. Estud. Psicol. 2001, 22, 319–344. [Google Scholar] [CrossRef]
- Solcoff, K. La edad de la memoria. El recuerdo biográfico y la representación de estados mentales autorreferenciales [Experimental phenomenology of memory? Autobiographical memory between context and meaning]. Propues. Educ. 2002, 25, 31–34. [Google Scholar]
- Schoen, S.A.; Miller, L.J.; Brett-Green, B.A.; Nielsen, D.M. Physiological and behavioral differences in sensory processing: A comparison of children with Autism Spectrum Disorder and Sensory Modulation Disorder. Front. Integr. Neurosci. 2009, 3, 29. [Google Scholar] [CrossRef] [PubMed]
- Ben-Sasson, A.; Hen, L.; Fluss, R.; Cermak, S.A.; Engel-Yeger, B.; Gal, E. A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Delacato, C.H. The Ultimate Stranger: The Autistic Child; Doubleday & Co.: New York, NY, USA, 1974; ISBN 0385010745. [Google Scholar]
- Mulligan, S. An analysis of score patterns of children with attention disorders on the sensory integration and praxis tests. Am. J. Occup. Ther. 1996, 50, 647–654. [Google Scholar] [CrossRef]
- Dunn, W. The impact of sensory processing abilities on the daily lives of young children and their families: A conceptual model. Infants Young Child. 1997, 9, 23–35. [Google Scholar] [CrossRef]
- Dunn, W. Sensory Profile; Texas Psicol. Corp.: San Antonio, TX, USA, 1999. [Google Scholar]
- Miller, L.J.; Reisman, J.; McIntosh, D.N.; Simon, J. An ecological model of sensory modulation: Performance of children with fragile X syndrome, autism, attention-deficit/hyperactivity disorder and sensory modulation dysfunction. In Understanding the Nature of Sensory Integration with Diverse Populations; Academic Press: New York, NY, USA, 2001; pp. 57–88. [Google Scholar]
- Iandolo, G.; Esposito, G.; Venuti, P. Cohesión, micro-organización, estructura narrativa y competencias verbales entre tres y once años: El desarrollo narrativo formal. Estud. Psicol. 2013, 34, 141–160. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H.; Leventhal, B.L.; Dilavore, P.C.; Pickles, A.; Rutter, M. The Autism Diagnostic Observation Schedule-Generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Services (WPS): Torrance, CA, USA, 2012. [Google Scholar]
- Morales-Hidalgo, P.; Roigé-Castellví, J.; Hernández-Martínez, C.; Voltas, N.; Canals, J. Prevalence and Characteristics of Autism Spectrum Disorder Among Spanish School-Age Children. J. Autism Dev. Disord. 2018, 48, 3176–3190. [Google Scholar] [CrossRef]
- Banach, R.; Thompson, A.; Szatmari, P.; Goldberg, J.; Tuff, L.; Zwaigenbaum, L.; Mahoney, W. Brief report: Relationship between non-verbal IQ and gender in autism. J. Autism Dev. Disord. 2009, 39, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Werling, D.M.; Geschwind, D.H. Sex differences in autism spectrum disorders. Curr. Opin. Neurol. 2013, 26, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Elliott, C.D. Differential Abilities Scale (DAS); TX Psychol. Corp.: San Antonio, TX, USA, 1990. [Google Scholar]
- Taylor, A.; Pickering, K.; Lord, C.; Pickles, A. Mixed and multi-level models for longitudinal data: Growth curve models of language development. In Statistical Analysis of Medical Data: New Developments; Hodder Education Publishers: London, UK, 1998; pp. 127–142. [Google Scholar]
- Anderson, D.K.; Lord, C.; Risi, S.; DiLavore, P.S.; Shulman, C.; Thurm, A.; Welch, K.; Pickles, A. Patterns of Growth in Verbal Abilities Among Children With Autism Spectrum Disorder. J. Consult. Clin. Psychol. 2007, 75, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.; Kamphaus, R. Reynolds Intellectual Assessment Scale (RIAS). Lutz, FL Psychol. Assess. Resour. 2003, 25, 402–408. [Google Scholar]
- Sánchez-Sánchez, F.; Fernández-Pinto, I.; Santamaría, P.; Carrasco, M.Á.; Del Barrio, V. SENA, Sistema de Evaluación de Niños y Adolescentes [ENA, Child and Adolescent Assessment System]. Rev. Psicol. Clínica Niños Adolesc. 2016, 3, 23–34. [Google Scholar]
- Bornstein, M.H.; Tamis-LeMonda, C.S. The Bear Family. Cognitive Coding Handbook; Unpublished Manual; National Institute of Child Health and Human Development: Bethesda, MD, USA, 1985. [Google Scholar]
- Esposito, G.; Venuti, P.; Iandolo, G.; de Falco, S.; Gabrieli, G.; Wei, C.; Bornstein, M.H. Microgenesis of typical storytelling. Early Child Dev. Care 2020, 190, 1991–2001. [Google Scholar] [CrossRef]
- Iandolo, G.; Esposito, G.; Venuti, P. The bears family projective test: Evaluating stories of children with emotional difficulties. Percept. Mot. Skills 2012, 114, 883–902. [Google Scholar] [CrossRef]
- Iandolo, G. El Desarrollo de las Competencias Narrativas: Forma, Cohesión y Equilibrio de Contenido a Través del Test Proyectivo de la Familia de los Osos [The development of narrative competences: Form, cohesion and balance of content through the Projective Test of the Bear Family]. PhD. Thesis, Universidad Autónoma de Madrid, Madrid, Spain, 2011. [Google Scholar]
- Venuti, P. L’osservazione del Comportamento: Ricerca Psicologica e Pratica Clinica [Observation of behavior: Psychological research and clinical practice]; Carocci: Roma, Italy, 2001; ISBN 8843018175. [Google Scholar]
- Bentenuto, A. Studio della Relazione Genitore—Bambino in Soggetti con Disturbo dello Spettro Autistico [Observation of behavior: Psychological research and clinical practice]. PhD Thesis, University of Trento, Trento, Italy, 2012. [Google Scholar]
- Bizzego, A.; Battisti, A.; Gabrieli, G.; Esposito, G.; Furlanello, C. Pyphysio: A physiological signal processing library for data science approaches in physiology. SoftwareX 2019, 10, 100287. [Google Scholar] [CrossRef]
- Iandolo, G.; López-Florit, L.; Venuti, P.; Neoh, M.J.Y.; Bornstein, M.H.; Esposito, G. Story contents and intensity of the anxious symptomatology in children and adolescents with Autism Spectrum Disorder. Int. J. Adolesc. Youth 2020, 25, 725–740. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, R.A.; Pastre, C.M.; Vanderlei, L.C.M.; Godoy, M.F. Poincaré plot indexes of heart rate variability: Relationships with other nonlinear variables. Auton. Neurosci. Basic Clin. 2013, 177, 271–274. [Google Scholar] [CrossRef]
- Taelman, J.; Vandeput, S.; Spaepen, A.; Van Huffel, S. Influence of mental stress on heart rate and heart rate variability. In Proceedings of the IFMBE, Antwerp, Belgium, 23–27 November 2008; Volume 22, pp. 1366–1369. [Google Scholar]
- Dishman, R.K.; Nakamura, Y.; Garcia, M.E.; Thompson, R.W.; Dunn, A.L.; Blair, S.N. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int. J. Psychophysiol. 2000, 37, 121–133. [Google Scholar] [CrossRef]
- Rosales-Soto, G.; Corsini-Pino, R.; Monsálves-Álvarez, M.; Yáñez-Sepúlveda, R. Respuesta del balance simpático-parasimpático de la variabilidad de la frecuencia cardíaca durante una semana de entrenamiento aeróbico en ciclistas de ruta [Response of the sympathetic-parasympathetic balance of heart rate variability during a week of aerobic training in road cyclists]. Rev. Andal. Med. Deport. 2016, 9, 143–147. [Google Scholar]
- Gutiérrez Sotelo, O. Variabilidad de la frecuencia cardíaca en individuos sanos costarricenses [Heart rate variability in healthy Costa Rican individuals]. Rev. Costarric. Cardiol 2000, 2, 3–10. [Google Scholar]
- Rodríguez-Ruiz, S.; Ruiz-Padial, E.; Vera, N.; Fernández, C.; Anllo-Vento, L.; Vila, J. Effect of heart rate variability on defensive reaction and eating disorder symptomatology in chocolate cravers. J. Psychophysiol. 2009, 23, 95–103. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, A.R. The somatic marker hypothesis: A neural theory of economic decision. Games Econ. Behav. 2005, 52, 336–372. [Google Scholar] [CrossRef]
- Nilsen, E.S.; Graham, S.A. The relations between children’s communicative perspective-taking and executive functioning. Cogn. Psychol. 2009, 58, 220–249. [Google Scholar] [CrossRef]
- Paula-Pérez, I. Coocurrencia entre ansiedad y autismo. las hipótesis del error social y de la carga alostática [Co-occurrence between anxiety and autism. the social error and allostatic load hypotheses]. Rev. Neurol. 2013, 56 (Suppl. 1), 45–59. [Google Scholar]
- Paula, I. La Ansiedad en el Autismo [Anxiety in autism]; Alianza Editorial: Madrid, Spain, 2015; p. 296. [Google Scholar]
- Zelazo, P.D.; Müller, U.; Frye, D.; Marcovitch, S.; Argitis, G.; Boseovski, J.; Chiang, J.K.; Hongwanishkul, D.; Schuster, B.V.; Sutherland, A. The development of executive function in early childhood. Monogr. Soc. Res. Child Dev. 2003, 68, 7–137. [Google Scholar] [CrossRef]
- Muñoz-Céspedes, J.M.; Tirapu-Ustárroz, J. Rehabilitación de las funciones ejecutivas [Rehabilitation of executive functions]. Rev. Neurol. 2004, 38, 656–663. [Google Scholar] [PubMed]
- Bernard-Opitz, V. Pragmatic analysis of the communicative behavior of an autistic child. J. Speech Hear. Disord. 1982, 47, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, F.D.M. Aspectos funcionais da comunicaçäo de crianças autistas [Functional aspects of the communication of autistic children]. Temas Desenvolv 2000, 9, 25–35. [Google Scholar]
- Garay, A.; Iñiguez, L.; Martínez, L.M. La perspectiva discursiva en psicología social [The discursive perspective in social psychology]. Subj. Procesos Cogn. 2005, 7, 105–130. [Google Scholar]
- Nigg, J.T.; Hinshaw, S.P.; Huang-Pollock, C. Disorders of Attention and Impulse Regulation. In Developmental Psychopathology, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2006; Volume 3, pp. 358–403. ISBN 9780470939406. [Google Scholar]
- Miilher, L.P.; Fernandes, F.D.M. Analyses of the communicative functions expressed by language therapists and patients of the autistic spectrum. Pro. Fono. 2006, 18, 239–248. [Google Scholar] [CrossRef]
- Garland, E.L.; Fredrickson, B.; Kring, A.M.; Johnson, D.P.; Meyer, P.S.; Penn, D.L. Upward spirals of positive emotions counter downward spirals of negativity: Insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clin. Psychol. Rev. 2010, 30, 849–864. [Google Scholar] [CrossRef]
- Delaherche, E.; Chetouani, M.; Mahdhaoui, A.; Saint-Georges, C.; Viaux, S.; Cohen, D. Interpersonal synchrony: A survey of evaluation methods across disciplines. IEEE Trans. Affect. Comput. 2012, 3, 349–365. [Google Scholar] [CrossRef]
- Adelantado, N. Diferencias Individuales en el Fraccionamiento Direccional de las Respuestas Electrodérmicas y Cardíacas Ante Estímulos con Diferente Carga Emocional [Individual Differences in Directional Fractionation of Electrodermal and Cardiac Responses to Stimuli with Different Emotional Charges]. PhD. Thesis, Universidad de Murcia, Murcia, Spain, 1988. [Google Scholar]
- López-de-la-Nieta, O.; Koeneke Hoenicka, M.A.; Martinez-Rubio, J.L.; Shinohara, K.; Esposito, G.; Iandolo, G. Exploration of the Spanish Version of the Attachment Style Questionnaire: A Comparative Study between Spanish, Italian, and Japanese Culture. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 113–128. [Google Scholar] [CrossRef]
- Koegel, R.L.; O’Dell, M.C.; Koegel, L.K. A natural language teaching paradigm for nonverbal autistic children. J. Autism Dev. Disord. 1987, 17, 187–200. [Google Scholar] [CrossRef]
- Koegel, L.K. Interventions to facilitate communication in autism. J. Autism Dev. Disord. 2000, 30, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Biringen, Z.; Damon, J.; Grigg, W.; Mone, J.; Pipp-Siegel, S.; Skillern, S.; Stratton, J. Emotional availability: Differential predictions to infant attachment and kindergarten adjustment based on observation time and context. Infant Ment. Health J. 2005, 26, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Siller, M.; Sigman, M. The Behaviors of Parents of Children with Autism Predict the Subsequent Development of Their Children’s Communication. J. Autism Dev. Disord. 2002, 32, 77–89. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Min | Max | Average | SD | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|
| Chronological age—years | 6 | 18 | 12.0 | 3.00 | −0.12 | −0.13 |
| Equivalent age (IQ-RIAS)—years | 4.6 | 18 | 12.50 | 3.29 | −0.45 | 0.08 |
| General IQ (IG-RIAS) ① | 62 | 120 | 96.38 | 16.01 | −0.25 | −0.64 |
| Verbal IQ (IV-RIAS) ① | 59 | 125 | 94.92 | 21.50 | −0.34 | −1.01 |
| Non-verbal IQ (INV-RIAS) ① | 66 | 120 | 97.81 | 15.06 | −0.40 | −0.86 |
| Verbal memory IQ (IM-RIAS) ① | 60 | 120 | 97.23 | 14.48 | −0.49 | 0.82 |
| ADOS/ ADOS-2 module ② | 2 | 4 | ||||
| Total ADOS/ ADOS-2 score ② | 7 | 12 | 10 | 1.37 | 0.43 | −0.36 |
| Number of propositions (Bears Family story) | 0 | 75 | 23.08 | 23.58 | 1.37 | 0.42 |
| Number of episodes (Bears Family story) | 0 | 40 | 11.00 | 10.53 | 1.86 | 3.36 |
| Cohesion index (Bears Family story) ③ | 0 | 10 | 5.00 | 2.87 | −0.10 | −1.11 |
| Structure index (Bears Family story) ④ | 0 | 6 | 3.17 | 2.12 | 0.12 | −1.56 |
| Global problem index (SENA-self report) ⑤ | 39 | 81 | 55.48 | 10.80 | 0.39 | 0.09 |
| Emotional problems (SENA-self report) ⑤ | 40 | 76 | 55.35 | 12.09 | 0.33 | −1.55 |
| Behavioral problems (SENA-self report) ⑤ | 41 | 88 | 55.35 | 15.03 | 1.02 | −0.03 |
| Executive functions problems (SENA-self report) ⑤ | 39 | 79 | 53.70 | 10.99 | 0.45 | −0.15 |
| Personal resources (SENA-self report) ⑤ | 15 | 54 | 38.65 | 9.75 | −0.58 | 0.58 |
| Self-esteem (SENA-self report) ⑤ | 21 | 62 | 44.70 | 9.67 | −0.29 | 0.40 |
| Global problem index (SENA-family report) ⑤ | 44 | 82 | 63.12 | 11.73 | 0.33 | −1.16 |
| Emotional problems (SENA-family report) ⑤ | 36 | 84 | 61.88 | 15.85 | −0.33 | −1.11 |
| Behavioral problems (SENA-family report) ⑤ | 40 | 90 | 57.80 | 13.97 | 0.85 | 0.26 |
| Executive functions problems (SENA-family report) ⑤ | 53 | 83 | 65.16 | 10.37 | 0.58 | −1.12 |
| Personal resources (SENA-family report) ⑤ | 21 | 50 | 34.64 | 8.32 | 0.02 | −0.44 |
| Global problem index (SENA-teacher report) ⑤ | 44 | 83 | 56.56 | 12.45 | 1.32 | 0.87 |
| Emotional problems (SENA-teacher report) ⑤ | 46 | 64 | 53.63 | 6.37 | 0.27 | −1.44 |
| Behavioral problems (SENA-teacher report) ⑤ | 44 | 88 | 54.69 | 14.30 | 1.75 | 2.36 |
| Executive functions (SENA-teacher report) ⑤ | 50 | 84 | 59.31 | 12.43 | 1.25 | 0.14 |
| Personal resources (SENA-teacher report) ⑤ | 13 | 46 | 32.50 | 10.48 | −0.11 | −1.21 |
| Group | SD2 Mean/SD |
|---|---|
| Group 1 (Low Sympathetic Activity –Low Stress Level) | 334,754/58,964 |
| Group 2 (High Sympathetic Activity –High Stress Level) | 92,518/38,868 |
| Online Therapy Session | Min | Max | Average | SD | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| Session duration (seconds) | 773 | 3000 | 1851.92 | 667.01 | 0.01 | −1.17 |
| Number of turn-taking events (frequency) | 38 | 202 | 117.69 | 51.06 | −0.15 | −1.22 |
| Ratio—session duration (seconds)/total number of turn-taking events (frequency) | 11 | 29 | 16.96 | 4.75 | 0.94 | 0.30 |
| Patient’s Characteristics | Child Accepts (NA) | Child Expands (NAm) | Patient Does Not Share (NNcC) | Patient Does Not Accept (NNA) | Patient Does Not Share and Proposes (NNcP) |
|---|---|---|---|---|---|
| Chronological age | r = −0.50 p = 0.05 | r = 0.40 p = 0.05 | |||
| Number of propositions (Bears Family story) | r = 0.46 p = 0.05 | ||||
| Cohesion index (Bears Family story) | r = −0.51 p = 0.01 | ||||
| Self-esteem (SENA-self report) | r = −0.57 p = 0.01 | ||||
| Personal resources (SENA-parental report) | r = −0.47 p = 0.05 |
| Therapist’s Behavior | Group | Mean | SD |
|---|---|---|---|
| Therapist ends (TT) - behavioral frequency - | Group 1 (Low Sympathetic Activity—Low Stress) | 1.2 | 0.63 |
| Group 2 (High Sympathetic Activity—High Stress) | 0.56 | 0.51 |
| Behavior | Mean | Median | Variance | Std. Dev. | Min. | Max. | Range | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|---|---|
| Co-oriented therapist | 327.32 | 318.31 | 23,587.96 | 153.58 | 21.34 | 813.49 | 792.16 | 0.42 | −0.05 |
| Therapist expands (TA) | 332.71 | 332.81 | 20,231.79 | 142.24 | 21.34 | 891.48 | 870.15 | 0.06 | −0.05 |
| Therapist directs attention (TDAt) | 411.73 | 462.02 | 18,996.30 | 137.83 | 135.46 | 625.71 | 490.24 | −0.56 | −0.99 |
| Therapist directs action (TDAc) | 429.52 | 451.02 | 18,178.90 | 134.83 | 37.02 | 719.27 | 682.25 | −1.34 | 2.11 |
| Therapist interrupts (TI) | 458.45 | 518.71 | 15,643.51 | 125.07 | 248.08 | 630.02 | 381.94 | −0.92 | −0.59 |
| Therapist proposes (T*) | 537.27 | 580.35 | 15,435.04 | 124.24 | 367.92 | 686.61 | 318.69 | −0.51 | −1.57 |
| Behavior | Mean | Median | Variance | Std. Dev. | Min. | Max. | Range | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|---|---|
| Patient expands (NAm) | 329.97 | 321.05 | 23,810.13 | 154.31 | 21.34 | 813.49 | 792.16 | 0.39 | −0.12 |
| Patient shares (NC) | 334.62 | 335.04 | 20,277.21 | 142.40 | 21.34 | 891.48 | 870.15 | 0.07 | −0.01 |
| Patient does not share (NNcC) | 368.53 | 407.46 | 25,309.95 | 159.09 | 42.17 | 719.27 | 677.10 | −0.48 | −0.88 |
| Patient does not share and proposes (NNcP) | 383.77 | 394.58 | 13,807.32 | 117.50 | 198.01 | 557.53 | 359.53 | −0.29 | −1.22 |
| Patient accepts (NA) | 461.70 | 440.47 | 6395.40 | 79.97 | 367.92 | 605.74 | 237.82 | 0.61 | −0.98 |
| Patient does not accept (NNA) | 618.49 | 614.61 | 1983.16 | 44.53 | 563.59 | 686.61 | 123.02 | 0.20 | −1.39 |
| Kolmogorov-Smirnov | Shapiro-Wilk | |||||||
|---|---|---|---|---|---|---|---|---|
| Statistic | df | Sig. | Statistic | df | Sig. | |||
| Therapist | SD2 | M* | 0.251 | 15 | 0.012 | 0.823 | 15 | 0.007 |
| MA | 0.023 | 1808 | 0.025 | 0.994 | 1808 | 0.000 | ||
| MC | 0.047 | 1300 | 0.000 | 0.983 | 1300 | 0.000 | ||
| MDAc | 0.189 | 86 | 0.000 | 0.868 | 86 | 0.000 | ||
| MDAt | 0.176 | 113 | 0.000 | 0.904 | 113 | 0.000 | ||
| MI | 0.229 | 22 | 0.004 | 0.807 | 22 | 0.001 | ||
| Patient | SD2 | NA | 0.185 | 22 | 0.048 | 0.886 | 22 | 0.016 |
| NAm | 0.045 | 1318 | 0.000 | 0.984 | 1318 | 0.000 | ||
| NC | 0.023 | 1729 | 0.039 | 0.994 | 1729 | 0.000 | ||
| NNA | 0.133 | 10 | 0.200 | 0.935 | 10 | 0.501 | ||
| NNcC | 0.126 | 185 | 0.000 | 0.936 | 185 | 0.000 | ||
| NNcP | 0.116 | 80 | 0.009 | 0.913 | 80 | 0.000 | ||
| Therapist SD2 (HRV) Grouped by Therapist’s Turn-Taking Interactive Behavior. (TMC, TA, TDAt, TDAc, TI, T*) | Therapist SD2 (HRV) Grouped by Patient’s Turn-Taking Interactive Behavior. (NAm, NC, NNcC, NNcP, NA, NNA) | |
|---|---|---|
| Chi-Square Statistical | 124.710 | 75.292 |
| Asymp. Sig. | 0.001 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Florit, L.; García-Cuesta, E.; Gracia-Expósito, L.; García-García, G.; Iandolo, G. Physiological Reactions in the Therapist and Turn-Taking during Online Psychotherapy with Children and Adolescents with Autism Spectrum Disorder. Brain Sci. 2021, 11, 586. https://doi.org/10.3390/brainsci11050586
López-Florit L, García-Cuesta E, Gracia-Expósito L, García-García G, Iandolo G. Physiological Reactions in the Therapist and Turn-Taking during Online Psychotherapy with Children and Adolescents with Autism Spectrum Disorder. Brain Sciences. 2021; 11(5):586. https://doi.org/10.3390/brainsci11050586
Chicago/Turabian StyleLópez-Florit, Laura, Esteban García-Cuesta, Luis Gracia-Expósito, German García-García, and Giuseppe Iandolo. 2021. "Physiological Reactions in the Therapist and Turn-Taking during Online Psychotherapy with Children and Adolescents with Autism Spectrum Disorder" Brain Sciences 11, no. 5: 586. https://doi.org/10.3390/brainsci11050586
APA StyleLópez-Florit, L., García-Cuesta, E., Gracia-Expósito, L., García-García, G., & Iandolo, G. (2021). Physiological Reactions in the Therapist and Turn-Taking during Online Psychotherapy with Children and Adolescents with Autism Spectrum Disorder. Brain Sciences, 11(5), 586. https://doi.org/10.3390/brainsci11050586