
Impact of SAfinamide on Depressive Symptoms in Parkinson’s Disease Patients (SADness-PD Study): A Multicenter Retrospective Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analyzsis
3. Results
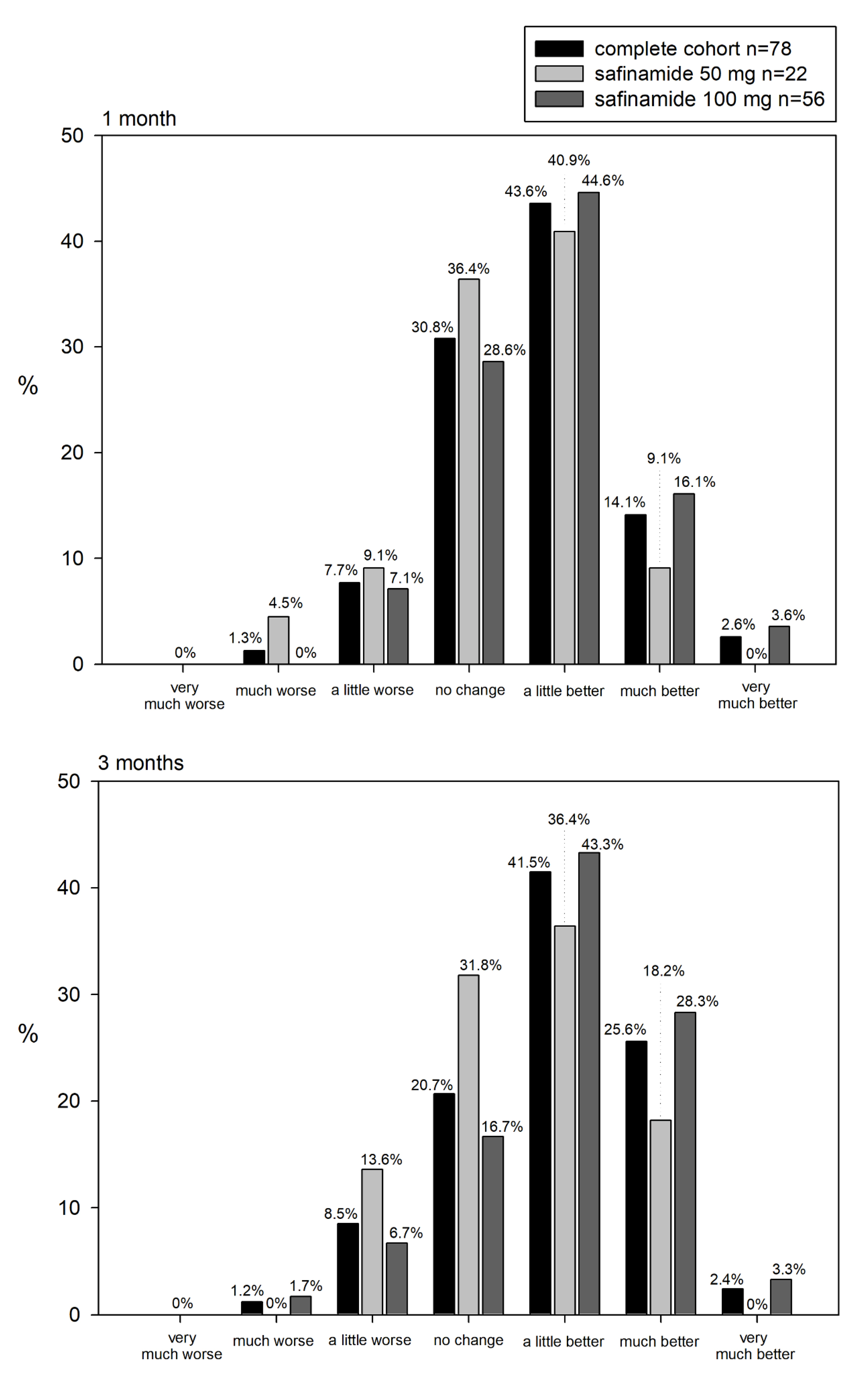
3.1. Effect of Safinamide on Depression in PD Patients
3.2. Safinamide on Motor Symptoms, Motor Complications, and Daily Life Activities in Real Clinical Practice
3.3. Serotonin Syndrome in Patients Concomitantly Treated with Antidepressant Drugs: Other Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stocchi, F.; Torti, M. Adjuvant therapies for Parkinson’s disease: Critical evaluation of safinamide. Drug. Des. Dev. Ther. 2016, 10, 609–618. [Google Scholar] [CrossRef]
- Borgohain, R.; Szasz, J.; Stanzione, P.; Meshram, C.; Bhatt, M.; Chirilineau, D.; Stocchi, F.; Lucini, V.; Iuliani, R.; Forrest, E.; et al. Study 016 Investigators. Randomized trial of safinamide add-on to levodopa in Parkinson’s disease with motor fluctuations. Mov. Disord. 2014, 29, 229–237. [Google Scholar] [CrossRef]
- Borgohain, R.; Szasz, J.; Stanzione, P.; Meshram, C.; Bhatt, M.H.; Chirilineau, D.; Stocchi, F.; Lucini, V.; Giuliani, R.; Forrest, E.; et al. Study 018 Investigators. Two-year, randomized, controlled study of safinamide as add-on to levodopa in mid to late Parkinson’s disease. Mov. Disord. 2014, 29, 1273–1280. [Google Scholar] [CrossRef]
- Schapira, A.H.; Fox, S.H.; Hauser, R.A.; Jankovic, J.; Jost, W.H.; Kenney, C.; Kulisevsky, J.; Pahwa, R.; Poewe, W.; Anand, R. Assessment of Safety and Efficacy of Safinamide as a Levodopa Adjunct in Patients With Parkinson Disease and Motor Fluctuations: A Randomized Clinical Trial. JAMA Neurol. 2017, 74, 216–224. [Google Scholar] [CrossRef]
- Hattori, N.; Tsuboi, Y.; Yamamoto, A.; Sasagawa, Y.; Nomoto, M. Efficacy and safety of safinamide as an add-on therapy to L-DOPA for patients with Parkinson’s disease: A randomized, double-blind, placebo-controlled, phase II/III study. Parkinsonism Relat. Disord. 2020, 75, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, Y.; Hattori, N.; Yamamoto, A.; Sasagawa, Y.; Nomoto, M. Long-term safety and efficacy of safinamide as add-on therapy in levodopa-treated Japanese patients with Parkinson’s disease with wearing-off: Results of an open-label study. J. Neurol. Sci. 2020, 416, 117012. [Google Scholar] [CrossRef] [PubMed]
- Mancini, F.; Di Fonzo, A.; Lazzeri, G.; Borellini, L.; Silani, V.; Lacerenza, M.; Comi, C. Real life evaluation of safinamide effectiveness in Parkinson’s disease. Neurol. Sci. 2020, 39, 733–739. [Google Scholar] [CrossRef]
- Aarsland, D.; Påhlhagen, S.; Ballard, C.G.; Ehrt, U.; Svenningsso, P. Depression in Parkinson disease-epidemiology, mechanisms, and management. Nat. Rev. Neurol. 2020, 8, 35–47. [Google Scholar] [CrossRef]
- Carod-Artal, F.J.; Ziomkowski, S.; Mourão Mesquita, H.; Martínez-Martin, P. Anxiety and depression: Main determinants of health-related quality of life in Brazilian patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2008, 14, 102–108. [Google Scholar] [CrossRef]
- Machado-Vieira, R.; Manji, H.K.; Zarate, C.A. The role of the tripartite glutamatergic synapse in the pathophysiology and therapeutics of mood disorders. Neuroscientist 2009, 15, 525–539. [Google Scholar] [CrossRef]
- Allain, H.; Pollak, P.; Neukirch, H.C. Symptomatic effect of selegiline in de novo parkinsonian patients. The French Selegiline Multicenter Trial. Mov. Disord. 1993, 8 (Suppl. S1), S36–S40. [Google Scholar] [CrossRef]
- Barone, P.; Poewe, W.; Albrecht, S.; Debieuvre, C.; Massey, D.; Rascol, O.; Tolosa, E.; Weintraub, D. Pramipexole for the treatment of depressive symptoms in patients with Parkinson’s disease: A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2010, 9, 573–580. [Google Scholar] [CrossRef]
- Rektorova, I.; Balaz, M.; Svatova, J.; Zarubova, K.; Honig, I.; Dostal, V.; Sedlackova, S.; Nestrasil, I.; Mastik, J.; Bares, M.; et al. Effects of ropinirole on nonmotor symptoms of Parkinson disease: A prospective multicenter study. Clin. Neuropharmacol. 2008, 31, 261–266. [Google Scholar] [CrossRef]
- Korchounov, A.; Winter, Y.; Rössy, W. Combined beneficial effect of rasagiline on motor function and depression in de novo PD. Clin. Neuropharmacol. 2012, 35, 121–124. [Google Scholar] [CrossRef]
- Zarate, C.; Machado-Vieira, R.; Henter, I.; Ibrahim, L.; Diazgranados, N.; Salvatore, G. Glutamatergic modulators: The future of treating mood disorders? Harv. Rev. Psychiatry 2010, 18, 293–303. [Google Scholar] [CrossRef]
- Richard, I.H.; Kurlan, R.; Tanner, C.; Factor, S.; Hubble, J.; Suchowersky, O.; Waters, C.; Parkinson Study Group. Serotonin syndrome and the combined use of deprenyl and an antidepressant in Parkinson’s disease. Neurology 1997, 48, 1070–1077. [Google Scholar] [CrossRef]
- Panisset, M.; Chen, J.J.; Rhyee, S.H.; Conner, J.; Mathena, J.; The STACCATO study investigators. Serotonin Toxicity Association with Concomitant Antidepressants and Rasagiline Treatment: Retrospective study (STACCATO). Pharmacotherapy 2014, 34, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Panisset, M.; Schwied, S.; Ondo, W.; Fitzer-Attas, C.; Chen, J.J. Safety of concomitant therapy with rasagiline and antidepressants in Parkinson’s diesease. Mov. Disord. 2007, 22 (Suppl. S16), S104. [Google Scholar] [CrossRef]
- Smith, K.M.; Eyal, E.; Weintraub, D.; for the ADAGIO Investigators. Combined rasagiline and antidepressant use in Parkinson disease in the ADAGIO study. Effects on nonmotor symptoms and tolerability. JAMA Neurol. 2015, 72, 88–95. [Google Scholar] [CrossRef]
- Aboukarr, A.; Giudice, M. Interaction between Monoamine Oxidase B Inhibitors and Selective Serotonin Reuptake Inhibitors. Can. J. Hosp. Pharm. 2018, 71, 196–207. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1599. [Google Scholar] [CrossRef]
- Torbey, E.; Pachana, N.A.; Dissanayaka, N.N.W. Depression rating scales in Parkinson’s disease: A critical review updating recent literature. J. Affect. Disord. 2015, 184, 216–224. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.R. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Schade, S.; Mollenhauer, B.; Trenkwalder, C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov. Disord. Clin. Pract. 2020, 7, 343–345. [Google Scholar] [CrossRef]
- Stocchi, F.; Borgohain, R.; Onofrj, M.; Schapira, A.H.V.; Bhatt, M.; Lucini, V.; Giuliani, R.; Anand, R. A randomized, double-blind, placebo-controlled trial of safinamide as add-on therapy in early Parkinson’s disease patients. Mov. Disord. 2012, 27, 106–112. [Google Scholar] [CrossRef]
- Cattaneo, C.; Müller, T.; Bonizzoni, E.; Lazzeri, G.; Kottakis, I.; Keywood, C. Long-Term Effects of Safinamide on Mood Fluctuations in Parkinson’s Disease. J. Parkinsons. Dis. 2017, 7, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.L.E.; Riboldazzi, G.; Mauri, M.; Versino, M. Efficacy of safinamide on non-motor symptoms in a cohort of patients affected by idiopathic Parkinson’s disease. Neurol. Sci. 2019, 40, 275–279. [Google Scholar] [CrossRef]
- Alborghetti, M.; Nicoletti, F. Different Generations of Type-B Monoamine Oxidase Inhibitors in Parkinson’s Disease: From Bench to Bedside. Curr. Neuropharmacol. 2019, 17, 861–873. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, C.; Jost, W.H.; Bonizzoni, E. Long-Term Efficacy of Safinamide on Symptoms Severity and Quality of Life in Fluctuating Parkinson’s Disease Patients. J. Parkinsons Dis. 2020, 10, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Abbruzzese, G.; Kulisevsky, J.; Bergmans, B.; Gomez-Esteban, J.C.; Kägi, G.; Raw, J.; Stefani, A.; Warnecke, T.; Jost, W.H.; SYNAPSES Study Investigators Group. A European Observational Study to Evaluate the Safety and the Effectiveness of Safinamide in Routine Clinical Practice: The SYNAPSES Trial. J. Parkinsons Dis. 2020. [Google Scholar] [CrossRef]
- Ahmed, M.A.A. A systematic review and meta-analysis of safety and efficacy of safinamide for motor fluctuations in patients with Parkinson’s disease. F1000Resarch 2019, 8, 2078. [Google Scholar] [CrossRef] [PubMed]
- Gloria Martí-Andrés, G.; Jiménez-Bolaños, R.; Arbelo-González, J.M.; Pagonabarraga, J.; Carmen Duran-Herrera, C.; Valenti-Azcarate, R.; Luquin, M.R. Safinamide in Clinical Practice: A Spanish Multicenter Cohort Study. Brain. Sci. 2019, 9, 272. [Google Scholar] [CrossRef]
- Baldo, B.A.; Rose, M.A. The anesthetists, opioid analgesic drugs, and serotonin toxicity: A mechanistic and clinical review. Br. J. Anaesth 2020, 124, 44e62. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | n (%) | Complete cohort | 82 |
| Safinamide-only group | 38 (46.3%) | ||
| Safinamide + antidepressants group | 44 (53.7%) | ||
| Age (years) | Mean (SD) [range] | Complete cohort | 68.33 (11.41) [41–90] |
| Ssafinamide-only group | 70.13 (9.83) [41–87] | ||
| Safinamide + antidepressants group | 66.77 (12.51) [42–90] | ||
| Gender (male/female) | n (%)/n (%) | Complete cohort | 37 (45.1%)/45 (54.9%) |
| Safinamide-only group | 21 (55.3%)/17 (44.7%) | ||
| Safinamide + antidepressants group | 16 (36.4%)/28 (63.6%) | ||
| Disease duration (years) | Mean (SD) | Complete cohort | 8.67 (8.55) |
| Safinamide-only group | 7.84 (9.65) | ||
| Safinamide + antidepressants group | 9.39 (7.51) | ||
| UPDRS | |||
| I | Mean (SD) | Complete cohort | 4.56 (1.82) |
| Safinamide-only group | 3.82 (1.90) | ||
| Safinamide + antidepressants group | 5.20 (1.49) | ||
| II | Mean (SD) | Complete cohort | 13.59 (6.67) |
| Safinamide-only group | 13.55 (7.07) | ||
| Safinamide + antidepressants group | 13.61 (6.38) | ||
| III | Mean (SD) | Complete cohort | 22.91 (8.68) |
| Safinamide-only group | 22.47 (9.90) | ||
| Safinamide + antidepressants group | 23.30 (7.57) | ||
| IV | Mean (SD) | Complete cohort | 3.51 (2.83) |
| Safinamide-only group | 2.61 (2.52) | ||
| Safinamide + antidepressants group | 4.30 (2.87) | ||
| HAMD-17 | Mean (SD) | Complete cohort | 19.49 (4.03) |
| Safinamide-only group | 18.39 (3.58) | ||
| Safinamide + antidepressants group | 20.43 (4.20) | ||
| LEDD (mg) | Mean (SD) | Complete cohort | 810.26 (368.45) |
| Safinamide-only group | 681.25 (218.15) | ||
| Safinamide + antidepressants group | 921.68 (432.86) |
| Antidepressant Drug | Range of Doses (mg/day) | n (%) |
|---|---|---|
| DULOXETINE | 30–120 | 11 (25.0%) |
| ESCITALOPRAM | 5–15 | 7 (15.9%) |
| MIRTAZAPINE | 15–30 | 5 (11.4%) |
| SERTRALINE | 50–100 | 5 (11.4%) |
| VENLAFAXINE | 75–150 | 5 (11.4%) |
| TRAZODONE | 50–100 | 4 (9.1%) |
| AMITRIPTILINE | 25 | 1 (2.3%) |
| CLORIMIPRAMINE | 25 | 1 (2.3%) |
| BUPROPION | 150 | 1 (2.3%) |
| CITALOPRAM | 20 | 1 (2.3%) |
| PAROXETINE + AMITRIPTILINE | 10 + 25 | 1 (2.3%) |
| VENLAFAXINE + MIRTAZAPINE | 75 + 15 | 1 (2.3%) |
| VORTIOXETINE | 10 | 1 (2.3%) |
| Baseline Mean (SD) | 1 Month Mean Difference from Baseline (SD) | p-Value | 3 Months Mean Difference from Baseline (SD) | p-Value | ||
|---|---|---|---|---|---|---|
| HAMD-17 | Complete cohort | 19.49 (4.03) n = 82 | −6 (5.10) n = 78 | p < 0.0001 | −7.27 (5.48) n = 82 | p < 0.0001 |
| Safinamide 50 mg | 18.50 (2.69) n = 22 | −3.32 (4.54) n = 22 | p = 0.0003 | −4.73 (4.49) n = 22 | p < 0.0001 | |
| Safinamide 100 mg | 19.85 (4.39) n = 60 | −7.03 (5.19) n = 56 | p < 0.0001 | −8.02 (5.73) n = 60 | p < 0.0001 | |
| UPDRS I | Complete cohort | 4.56 (1.82) n = 82 | −1.32 (1.99) n = 78 | p < 0.0001 | −1.5 (2.03) n = 82 | p < 0.0001 |
| Safinamide 50 mg | 4.59 (1.47) n = 22 | −0.64 (1.91) n = 22 | p = 0.0157 | −0.91 (1.76) n = 22 | p = 0.0045 | |
| Safinamide 100 mg | 4.55 (1.94) n = 60 | −1.59 (1.97) n = 56 | p < 0.0001 | −1.72 (2.08) n = 60 | p < 0.0001 | |
| UPDRS II | Complete cohort | 13.59 (6.67) n = 82 | −2.51 (6.30) n = 78 | p < 0.0001 | −2.47 (6.11) n = 82 | p < 0.0001 |
| Safinamide 50 mg | 11.50 (5.20) n = 22 | −0.36 (5.44) n = 22 | p = 0.4064 | −0.23 (5.23) n = 22 | p = 0.4966 | |
| Safinamide 100 mg | 14.35 (7.02) n = 60 | −3.30 (6.65) n = 56 | p < 0.0001 | −3.28 (6.45) n = 60 | p < 0.0001 | |
| UPDRS III | Complete cohort | 22.91 (8.68) n = 82 | −3.58 (8.56) n = 78 | p < 0.0001 | −4.03 (8.95) n = 82 | p < 0.0001 |
| Safinamide 50 mg | 22.00 (8.12) n = 22 | −0.41 (8.88) n = 22 | p = 0.7722 | +0.50 (9.42) n = 22 | p = 0.6723 | |
| Safinamide 100 mg | 23.25 (8.92) n = 60 | −4.8 (8.34) n= 56 | p < 0.0001 | −5.70 (8.47) n = 60 | p < 0.0001 | |
| UPDRS IV | Complete cohort | 3.51 (2.83) n = 82 | −0.61 (2.61) n = 78 | p = 0.0003 | −0.8 (2.53) n = 82 | p < 0.0001 |
| Safinamide 50 mg | 4.64 (2.59) n = 22 | −0.32 (2.38) n = 22 | p = 0.1839 | −0.28 (2.50) n = 22 | p = 0.2482 | |
| Safinamide 100 mg | 3.10 (2.82) n = 60 | −0.76 (2.50) n = 56 | p = 0.0007 | −1.00 (2.28) n = 60 | p < 0.0001 |
| 1 Month | 3 Months | |||||||
|---|---|---|---|---|---|---|---|---|
| Safinamide + Antidepressants Group n = 42 | Safinamide-only Group n = 36 | p-Value | Safinamide + Antidepressants Group n = 44 | Safinamide-only Group n = 38 | p-Value | |||
| Major symptoms | Confusion | n (%) | 2 (2.6%) | 0 (0%) | p = 0.564 | 1 (1.2%) | 0 (0%) | p = 1.251 |
| Emotional lability | 2 (2.6%) | 1 (1.3%) | p = 1.021 | 3 (3.7%) | 1 (1.2%) | p = 0.627 | ||
| Fever | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | ||
| Sweating | 3 (3.8%) | 1 (1.3%) | p = 0.627 | 3 (3.7%) | 0 (0%) | p = 0.266 | ||
| Myoclonus | 0 (0%) | 0 (0%) | - | 2 (2.4%) | 0 (0%) | p = 0.565 | ||
| Minor symptoms | Agitation | n (%) | 2 (2.6%) | 1 (1.3%) | p = 1.021 | 1 (1.2%) | 0 (0%) | p = 1.251 |
| Sleep disorders | 13 (16.7%) | 4 (5.1%) | p = 0.053 | 13 (15.9%) | 4 (4.9%) | p = 0.054 | ||
| Nervousness | 15 (19.2%) | 4 (5.1%) | p = 0.017 | 13 (15.9%) | 5 (6.1%) | p = 0.108 | ||
| Tachycardia | 2 (2.6%) | 1 (1.3%) | p = 1.021 | 3 (3.7%) | 0 (0%) | p = 0.266 | ||
| Hyperventilation | 0 (0%) | 1 (1.3%) | p = 0.897 | 0 (0%) | 1 (1.2%) | p = 0.894 | ||
| Dyspnea | 1 (1.3%) | 2 (2.6%) | p = 0.642 | 2 (2.4%) | 3 (3.7%) | p = 0.666 | ||
| Diarrhea | 0 (0%) | 1 (1.3%) | p = 0.897 | 1 (1.2%) | 0 (0%) | p = 1.251 | ||
| Hypertension | 0 (0%) | 1 (1.3%) | p = 0.897 | 0 (0%) | 1 (1.2%) | p = 0.894 | ||
| Hypotension | 0 (0%) | 0 (0%) | - | 0 (0%) | 0 (0%) | - | ||
| Ataxia | 0 (0%) | 1 (1.3%) | p = 0.897 | 0 (0%) | 1 (1.2%) | p = 0.894 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña, E.; Borrué, C.; Mata, M.; Martínez-Castrillo, J.C.; Alonso-Canovas, A.; Chico, J.L.; López-Manzanares, L.; Llanero, M.; Herreros-Rodríguez, J.; Esquivel, A.; et al. Impact of SAfinamide on Depressive Symptoms in Parkinson’s Disease Patients (SADness-PD Study): A Multicenter Retrospective Study. Brain Sci. 2021, 11, 232. https://doi.org/10.3390/brainsci11020232
Peña E, Borrué C, Mata M, Martínez-Castrillo JC, Alonso-Canovas A, Chico JL, López-Manzanares L, Llanero M, Herreros-Rodríguez J, Esquivel A, et al. Impact of SAfinamide on Depressive Symptoms in Parkinson’s Disease Patients (SADness-PD Study): A Multicenter Retrospective Study. Brain Sciences. 2021; 11(2):232. https://doi.org/10.3390/brainsci11020232
Chicago/Turabian StylePeña, Esteban, Carmen Borrué, Marina Mata, Juan Carlos Martínez-Castrillo, Araceli Alonso-Canovas, Juan Luis Chico, Lydia López-Manzanares, Marcos Llanero, Jaime Herreros-Rodríguez, Alberto Esquivel, and et al. 2021. "Impact of SAfinamide on Depressive Symptoms in Parkinson’s Disease Patients (SADness-PD Study): A Multicenter Retrospective Study" Brain Sciences 11, no. 2: 232. https://doi.org/10.3390/brainsci11020232
APA StylePeña, E., Borrué, C., Mata, M., Martínez-Castrillo, J. C., Alonso-Canovas, A., Chico, J. L., López-Manzanares, L., Llanero, M., Herreros-Rodríguez, J., Esquivel, A., Maycas-Cepeda, T., & Ruíz-Huete, C. (2021). Impact of SAfinamide on Depressive Symptoms in Parkinson’s Disease Patients (SADness-PD Study): A Multicenter Retrospective Study. Brain Sciences, 11(2), 232. https://doi.org/10.3390/brainsci11020232