
Activities of Daily Living and Categorization Skills of Elderly with Cognitive Deficit: A Preliminary Study

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Instruments
2.3.1. MoCA
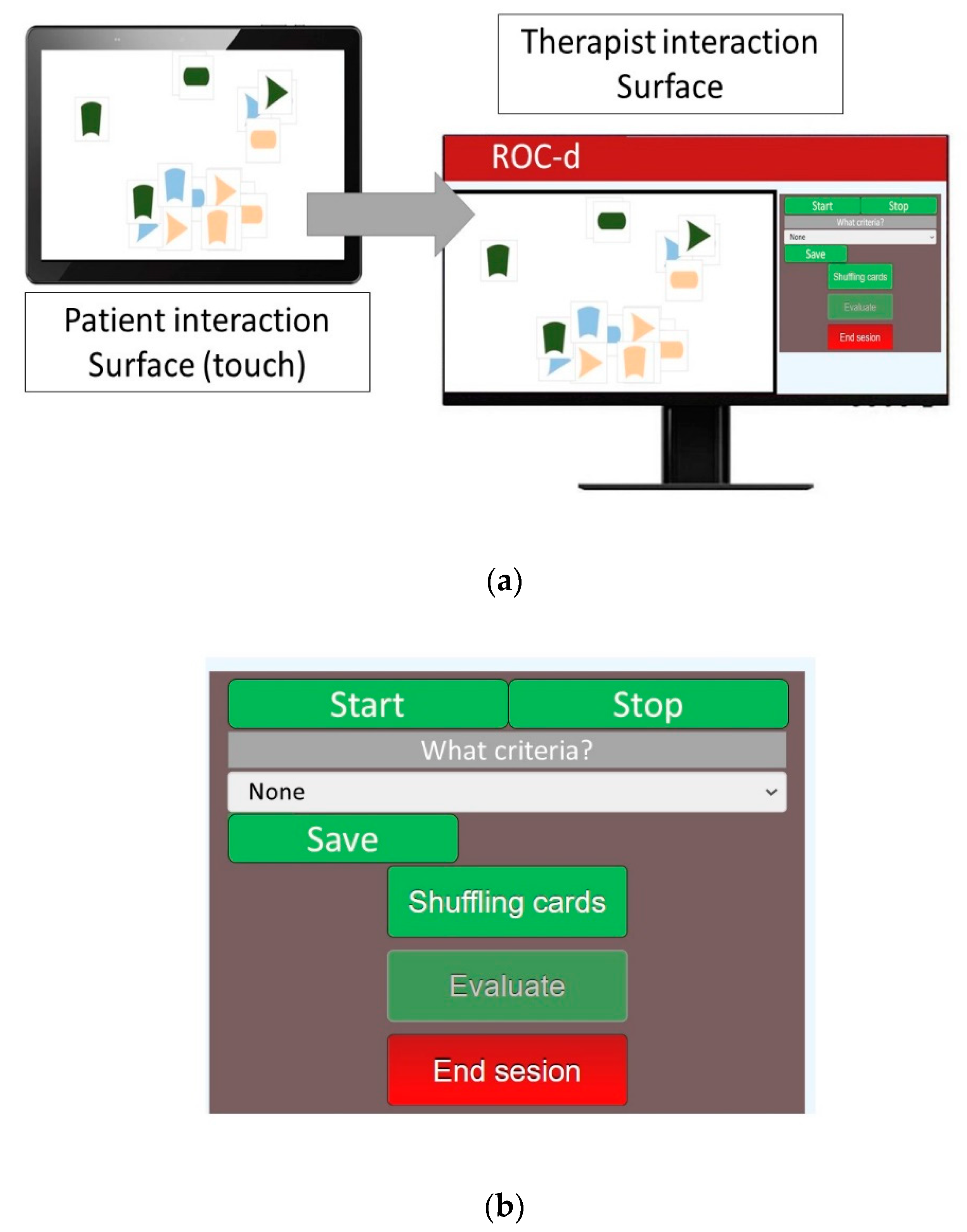
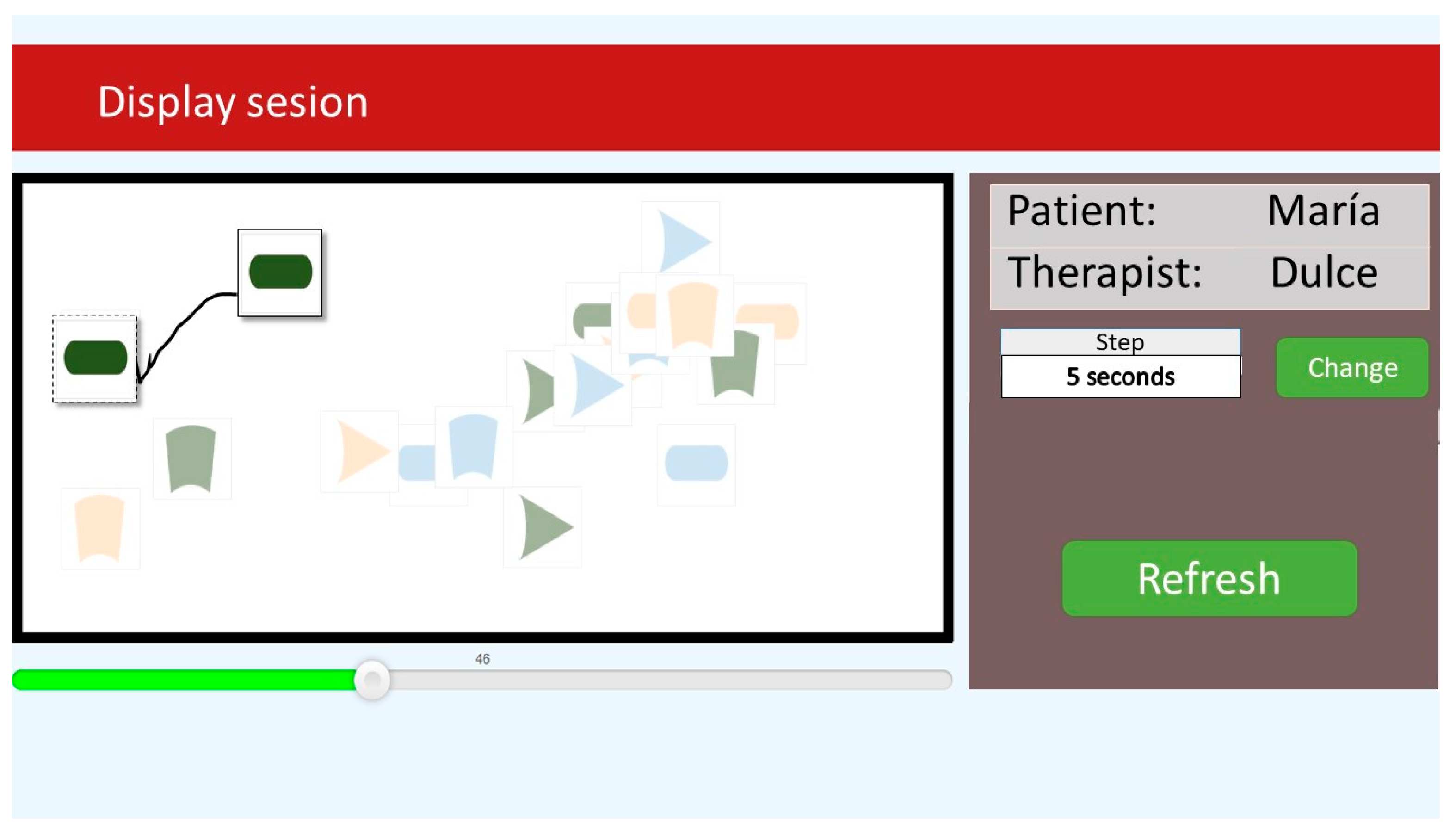
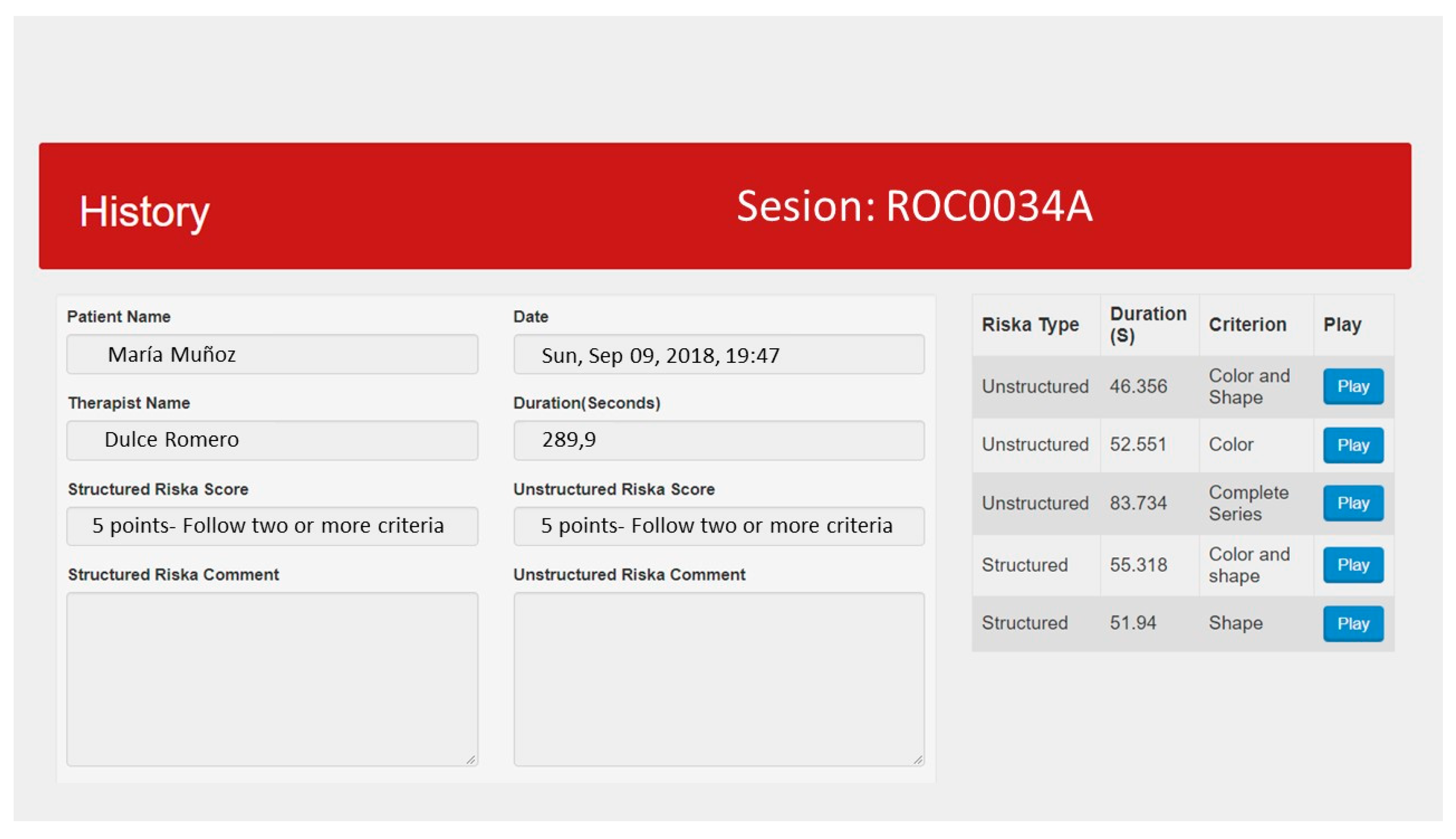
2.3.2. ROC-d
2.3.3. Routine Task Inventory-2
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bonnechère, B.; Sahakian, B.J. Can mobile technology help prevent the burden of dementia in low- and mid-income countries? Front. Public Health 2020, 8, 1–6. [Google Scholar]
- Feger, D.M.; Willis, S.L.; Thomas, K.R.; Marsiske, M.; Rebok, G.W.; Felix, C.; Gross, A.L. Incident instrumental activities of daily living difficulty in older adults: Which comes first? Findings from the advanced cognitive training for independent and vital elderly study. Front. Neurol. 2020, 11, 550577. [Google Scholar] [CrossRef]
- Connolly, D.; Garvey, J.; McKee, G. Factors associated with ADL/IADL disability in community dwelling older adults in the Irish longitudinal study on ageing (TILDA). Disabil. Rehabil. 2017, 39, 809–816. [Google Scholar] [CrossRef]
- Reppermund, S.; Brodaty, H.; Crawford, J.D.; Kochan, N.A.; Draper, B.; Slavin, M.J.; Trollor, J.N.; Sachdev, P.S. Impairment in instrumental activities of daily living with high cognitive demand is an early marker of mild cognitive impairment: The Sydney memory and ageing study. Psychol. Med. 2013, 43, 2437–2445. [Google Scholar] [CrossRef] [PubMed]
- Chuang, I.C.; Hsu, W.C.; Chen, C.L.; Wu, Y.R.; Chiau, H.Y.; Wu, C.Y. Psychometric Evaluation of an ICF -Based Instrumental Activities of Daily Living Assessment With Older Adults With Cognitive Decline. Am. J. Occup. Ther. 2020, 74, 1–8. [Google Scholar] [CrossRef]
- McAlister, C.; Schmitter-Edgecombe, M. Executive function subcomponents and their relations to everyday functioning in healthy older adults. J. Clin. Exp. Neuropsychol. 2017, 38, 925–940. [Google Scholar] [CrossRef] [PubMed]
- Kounti, F.; Tsolaki, M.; Kiosseoglou, G. Functional cognitive assessment scale (FUCAS): A new scale to assess executive cognitive function in daily life activities in patients with dementia and mild cognitive impairment. Hum. Psychopharmacol. 2006, 21, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, L.; Giovanello, K. Executive function in daily life: Age-related influences of executive processes on instrumental activities of daily living. Psychol. Aging 2010, 25, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Calso, C.; Besnard, J.; Allain, P. Frontal lobe functions in normal aging: Metacognition, autonomy, and quality of life. Exp. Aging Res. 2019, 45, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Goverover, Y. Categorization, deductive reasoning, and self-awareness: Association with everyday competence in persons with acute brain injury. J. Clin. Exp. Neuropsychol. 2004, 26, 737–749. [Google Scholar] [CrossRef]
- Fuentes, P. Funcionalidad y demencia. Rev. Hosp. Clín. Univ. Chile 2008, 19, 324–329. Available online: https://www.redclinica.cl/Portals/0/Users/014/14/14/Publicaciones/Revista/funcionalidad_y_demencia.pdf (accessed on 17 November 2020).
- Akbari, S.; Lyden, P.D.; Kamali, M.; Fahimi, M.A. Correlations among impairment, daily activities and thinking operations after stroke. NeuroRehabilitation 2013, 33, 153–160. [Google Scholar] [CrossRef]
- Ojeda, N.; del Pino, R.; Ibarrtxe-Bilbao, N.; Schretlen, D.; Peña, J.; Álvarez, D. Montreal cognitive assessment test: Nor-malization and standardization for Spanish population. Rev. Neurol. 2016, 63, 488–496. [Google Scholar]
- Regev, S.; Josman, N. Evaluation of executive functions and everyday life for people with severe mental illness: A systematic review. Schizophr. Res. Cogn. 2020, 21, 100178. [Google Scholar] [CrossRef] [PubMed]
- Santiago, J. del conocimiento, L.O. Procesos Psicológicos Básicos, 2nd ed.; McGraw-Hill: Madrid, Spain, 2006; pp. 123–145. [Google Scholar]
- Fernández-Abascal, E.; Martín-Díaz, M.; Domínguez-Sánchez, J. Procesos Psicológicos; Pirámide Ediciones: Madrid, Spain, 2004. [Google Scholar]
- Smith, E.E.; Kosslyn, S.M. Procesos cognitivos. In Modelos Y Bases Neurales; Prentice Hall: Madrid, Spain, 2007. [Google Scholar]
- Jutten, R.J.; Harrison, J.; de Jong, F.J.; Aleman, A.; Ritchie, C.W.; Scheltens, P.; Sikkes, S.A. A composite measure of cognitive and functional progression in Alzheimer’s disease: Design of the capturing changes in cognition study. Alzheimers Dement Transl. Res. Clin. Interv. 2017, 3, 130–138. [Google Scholar] [CrossRef]
- Katz, N.; Itzkovich, M.; Averbuch, S.; Elazar, B. Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) battery for brain-injured patients: Reliability and validity. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 1989, 43, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Josman, N. Reliability and validity of the toglia category assessment test. Can. J. Occup. Ther. 1999, 66, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Muramatsu, T. Wisconsin Card Sorting Test (WCST). Nihon Rinsho. 2011, 69, 435–438. [Google Scholar]
- Nyhus, E.; Barceló, F. The Wisconsin card sorting test and the cognitive assessment of prefrontal executive functions: A critical update. Brain Cogn. 2009, 71, 437–451. [Google Scholar] [CrossRef]
- de la Fuente, Á.; Doménech, R. El nivel educativo de la población en España y sus regiones: 1960–2011. Investig. Reg. 2016, 2016, 73–94. [Google Scholar]
- Domingo-Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C. Propuestas de clase social neoweberiana y neomarxista a partir de la Clasificación nacional de ocupaciones 2011. Gac. Sanit. 2013, 27, 263–272. [Google Scholar] [CrossRef]
- Gil-Berrozpe, G.J.; Sánchez-Torres, A.M.; García de Jalón, E.; Moreno-Izco, L.; Fañanás, L.; Peralta, V.; Cuesta, M.J.; Ballesteros, A.; Hernández, R.; Janda, L.; et al. Utility of the MoCA for cognitive impairment screening in long-term psychosis patients. Schizophr. Res. 2020, 216, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Josman, N.; Katz, N. Relationships of categorization on tests and daily tasks in patients with schizophrenia, post-stroke patients and healthy controls. Psychiatry Res. 2006, 141, 15–28. [Google Scholar] [CrossRef]
- Su, C.Y.; Chen, W.L.; Tsai, P.C.; Tsai, C.Y.; Su, W.L. Psychometric properties of the loewenstein occupational therapy cognitive assessment-second edition in Taiwanese persons with schizophrenia. Am. J. Occup. Ther. 2007, 61, 108–118. [Google Scholar] [CrossRef][Green Version]
- Tesoriero, R. Distributing user interfaces. In Proceedings of the 2014 Workshop on Distributed User Interfaces and Multimodal Interaction, Toulouse, France, 1 July 2014. [Google Scholar]
- McAnanama, E.; Rogosin-Rose, M.; Scott, E.; Joffe, R.; Kelner, M. Discharge planning in mental health: The relevance of cognition to community living. Am. J. Occup. Ther. 1999, 53, 129–135. [Google Scholar] [CrossRef][Green Version]
- Martínez-González, M.; Sánchez-Villegas, A.; Toledo-Atucha, E.; Faulin-Fajardo, J. Bioestadística Amigable, 4th ed.; Elsevier: Barcelona, España, 2020. [Google Scholar]
- Chen, H.; Cohen, P.; Chen, S. How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Commun. Stat. Simul. Comput. 2010, 39, 860–864. [Google Scholar] [CrossRef]
- Gold, D.A. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2012, 34, 11–34. [Google Scholar] [CrossRef] [PubMed]
- Levy, L. Cognitive aging in perspective: Information processing, cognition and memory. In Cognition and Occupation across the Life Span Models for Intervention in Occupational Therapy; American Occupational Therapy Association Press: Bethesda, MD, USA, 2005; pp. 327–346. [Google Scholar]
- Tomaszewski Farias, S.; Giovannetti, T.; Payne, B.R.; Marsiske, M.; Rebok, G.W.; Schaie, K.W.; Thomas, K.R.; Willis, S.R.; Dzierzewski, J.M.; Unverzagt, F.; et al. Self-perceived difficulties in everyday function precede cognitive decline among older adults in the active study. J. Int. Neuropsychol. Soc. 2018, 24, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Read, J.C. Serious games in education. EAI Endorsed Trans. Serious Games 2015, 2. Available online: https://search.proquest.com/docview/2306502487?accountid=14542 (accessed on 10 February 2021).
- Putcha, D.; Tremont, G. Predictors of independence in instrumental activities of daily living: Amnestic versus nonamnestic MCI. J. Clin. Exp. Neuropsychol. 2016, 38, 991–1004. [Google Scholar] [CrossRef]
- Zur, B.M.; Rudman, D.L.; Johnson, A.M.; Roy, E.A.; Wells, J.L. Components of cognitive competence predictive of occupational competence in persons with dementia: A delphi study. Can. J. Occup. Ther. 2013, 80, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Graff, M.J.L.; Vernooij-Dassen, M.J.M.; Thijssen, M.; Dekker, J.; Hoefnagels, W.H.L.; Olderikkert, M.G.M. Effects of community occupational therapy on quality of life, mood, and health status in dementia patients and their caregivers: A randomized controlled trial. J. Gerontol. Ser. Biol. Sci. Med. Sci. 2007, 62, 1002–1009. [Google Scholar] [CrossRef]
- Yuill, N.; Hollis, V. A systematic review of cognitive stimulation therapy for older adults with mild to moderate dementia: An occupational therapy perspective. Occup. Ther. Int. 2011, 18, 163–186. [Google Scholar] [CrossRef] [PubMed]
- Pimouguet, C.; Le Goff, M.; Wittwer, J.; Dartigues, J.F.; Helmer, C. Benefits of occupational therapy in dementia patients: Findings from a real-world observational study. J. Alzheimers Dis. 2017, 56, 509–517. [Google Scholar] [CrossRef]
- Cano, S.J.; Posner, H.B.; Moline, M.L.; Hurt, S.W.; Swartz, J.; Hsu, T.; Hobart, J.C. The ADAS-cog in Alzheimer’s disease clinical trials: Psychometric evaluation of the sum and its parts. J. Neurol. Neurosurg. Psychiatry 2010, 81, 1363–1368. [Google Scholar] [CrossRef]
- Rabin, L.A.; Wang, C.; Katz, M.J.; Derby, C.A.; Buschke, H.; Lipton, R.B. Predicting Alzheimer’s disease: Neuropsychological tests, self-reports, and informant reports of cognitive difficulties. J. Am. Geriatr. Soc. 2012, 60, 1128–1134. [Google Scholar] [CrossRef]
- Romero Ayuso, D.M. Actividades de la vida diaria. An. Psicol. Ann. Psychol. 2007, 23, 264–271. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Taylor, R.R.; Kielhofner, G. Kielhofner’s Model of Human Occupation: Theory and Application; Wolters Kluwer Health: Philadelphia, PA, USA, 2017. [Google Scholar]
- Law, M.; Cooper, B.; Strong, S.; Stewart, D.; Rigby, P.; Letts, L. The person-environment-occupation model: A transactive approach to occupational performance. Can. J. Occup. Ther. 1996, 63, 9–23. [Google Scholar] [CrossRef]
- Hernández Escobar, A.A.; Ramos Rodríguez, M.P.; Placencia López, B.M.; Indacochea Ganchozo, B.; Quimis Gómez, A.J.; Moreno Ponce, L.A. Metodología De La Investigación Científica; 3Ciencias: Alcoy, Spain, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Male | 16 | 31.4 |
| Female | 35 | 68.6 |
| Educational Level | ||
| Illiterate | 14 | 27.5 |
| Primary education | 16 | 31.4 |
| Secondary education | 14 | 27.5 |
| Higher education | 7 | 13.7 |
| Socioeconomic status | ||
| Level I | 8 | 15.7 |
| Level II | 3 | 5.9 |
| Level III | 40 | 78.4 |
| ROCUS | |
|---|---|
| Score | Criteria |
| 1 | Exact identification |
| 2 | Follows an incomplete criterion |
| 3 | Follows a criterion with spatial preparation |
| 4 | Follows a criterion with random disposition |
| 5 | Follows two or more criteria simultaneously |
| ROC | |
| Score | Criteria |
| 1 | Exact identification |
| 2 | Follows an incomplete criterion |
| 3 | Follows a criterion |
| 4 | Follows two or more criteria simultaneously only |
| at the second attempt | |
| 5 | Follows two or more criteria simultaneously at the |
| first attempt | |
| No Cognitive Impairment (n = 20) | Cognitive Impairment (n = 31) | p-Value | |||
|---|---|---|---|---|---|
| % (n) | % (n) | ||||
| Gender | 0.360 * | ||||
| Male | 40 (8) | 25.8 (8) | |||
| Female | 60 (12) | 74.2 (23) | |||
| Educational Level | <0.001 ** | ||||
| Illiterate | 0 (0) | 45.2 (14) | |||
| Primary education | 30 (6) | 31.4 (16) | |||
| Secondary education | 35 (7) | 27.5 (14) | |||
| Higher education | 35 (7) | 13.7 (7) | |||
| Socioeconomic status | 0.004 * | ||||
| Level I | 35 (7) | 3.2 (1) | |||
| Level II | 10 (2) | 3.2 (1) | |||
| Level III | 55 (11) | 93.5 (29) | |||
| Mean (SD) | Median (25–75% interquartile range) | Mean (SD) | Median (25–75% interquartile range) | ||
| Age | 62.40 (5.51) | 62 (58.50–64.50) | 76.97 (10.66) | 81 (64–86) | <0.001 *** |
| MoCA Score | 27.20 (1.20) | 27 (26–28) | 15.84 (6.05) | 16 (10–22) | <0.001 *** |
| ROC | 4.55 (0.95) | 5 (5–5) | 2.97 (1.02) | 3 (2–3) | <0.001 *** |
| ROCUS | 4.95 (0.22) | 5(5–5) | 3.10 (1.14) | 3 (2–4) | <0.001 *** |
| ROC-d (s) | 501.05 (161.30) | 484 (366–610) | 667.76 (338.42) | 642 (327–909) | 0.150 *** |
| Physical ADLs-RTI-2 | 5.13 (0.04) | 5.14 (5.14–5.14) | 4.35 (0.77) | 4.43 (3.86–5) | <0.001 *** |
| Grooming | 5 (0) | 5 (5–5) | 4.32 (0.83) | 5 (4–5) | <0.001 *** |
| Dressing | 5 (0) | 5 (5–5) | 4.39 (0.96) | 5 (4–5) | 0.002 *** |
| Bathing | 5 (0) | 5 (5–5) | 4.16 (1.19) | 5 (4–5) | <0.001 *** |
| Walking/Exercising | 4.90 (0.31) | 5 (5–5) | 4.06 (1.12) | 4 (4–5) | 0.001 *** |
| Eating | 5 (0) | 5 (5–5) | 4.45 (0.57) | 4 (4–5) | <0.001 *** |
| Toileting | 5 (0) | 5 (5–5) | 4.68 (0.48) | 5 (4–5) | 0.005 *** |
| Taking Medication | 6 (0) | 6 (6–6) | 4.35 (1.31) | 4 (3–6) | <0.001 *** |
| IADLs-RTI-2 | 5.31 (0.78) | 5.64 (4.93–5.86) | 3.42 (1.22) | 2.86 (2.43–4.29) | <0.001 *** |
| Housekeeping | 4.30 (1.38) | 5 (4.25–5) | 2.81(1.66) | 3 (1–5) | 0.002 *** |
| Preparing and securing food | 5.10 (1.65) | 6 (4.50–6) | 3.23 (1.67) | 2 (2–5) | 0.001 *** |
| Spending Money | 5.35 (1.35) | 6 (6–6) | 3.61(1.52) | 3 (3–6) | <0.001 *** |
| Shopping | 5.80 (0.89) | 6 (6–6) | 3.26 (1.53) | 2 (2–4) | <0.001 *** |
| Doing Laundry | 5.25 (1.25) | 6 (4.25–6) | 3.77 (1.23) | 3 (3–5) | <0.001 *** |
| Traveling | 5.45 (0.95) | 6 (5–6) | 3.32 (1.40) | 3 (2–4) | <0.001 *** |
| Telephoning | 5.95 (0.22) | 6 (6–6) | 3.97 (1.45) | 3 (3–6) | <0.001 *** |
| IADL-RTI-2 | Physical ADL-RTI-2 | MoCA | ROCUS | |
|---|---|---|---|---|
| Physical ADL-RTI-2 | 0.818 ** | |||
| MoCA | 0.740 ** | 0.798 ** | ||
| ROCUS | 0.510 ** | 0.547 ** | 0.732 ** | |
| ROC | 0.463 ** | 0.586 ** | 0.653 ** | 0.661 ** |
| Score | No Cognitive Impairment n% | Cognitive Impairment n% | p-Value Crude Model | p-Value Adjusted for Age, Educational Level and Socioeconomic Status | OR Adjusted for Age, Educational Level, and Socioeconomic Status (CI 95%) | |||
|---|---|---|---|---|---|---|---|---|
| Physical ADL-RTI-2 | ≤5 | 2 | 10.0% | 25 | 80.6% | <0.001 | 0.179 | 4.25 (0.52–35.08) |
| >5 | 18 | 90.0% | 6 | 19.4% | ||||
| IADL-RTI-2 | ≤4.3 | 3 | 15.0% | 25 | 80.6% | <0.001 | 0.998 | 2.27 × 1013 (0–∞) |
| >4.3 | 17 | 85.0% | 6 | 19.4% | ||||
| ROCUS | 2–4 | 1 | 5.0% | 26 | 83.9% | <0.001 | 0.006 | 58.31 (3.24–1049.43) |
| 5 | 19 | 95.0% | 5 | 16.1% | ||||
| ROC | 1–3 | 4 | 20.0% | 25 | 80.6% | <0.001 | 0.139 | 4.14 (0.63–27.15) |
| 4–5 | 16 | 80.0% | 6 | 19.4% | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Ayuso, D.; Cuerda, C.; Morales, C.; Tesoriero, R.; Triviño-Juárez, J.M.; Segura-Fragoso, A.; Gallud, J.A. Activities of Daily Living and Categorization Skills of Elderly with Cognitive Deficit: A Preliminary Study. Brain Sci. 2021, 11, 213. https://doi.org/10.3390/brainsci11020213
Romero-Ayuso D, Cuerda C, Morales C, Tesoriero R, Triviño-Juárez JM, Segura-Fragoso A, Gallud JA. Activities of Daily Living and Categorization Skills of Elderly with Cognitive Deficit: A Preliminary Study. Brain Sciences. 2021; 11(2):213. https://doi.org/10.3390/brainsci11020213
Chicago/Turabian StyleRomero-Ayuso, Dulce, Cristian Cuerda, Carmen Morales, Ricardo Tesoriero, José Matías Triviño-Juárez, Antonio Segura-Fragoso, and José A. Gallud. 2021. "Activities of Daily Living and Categorization Skills of Elderly with Cognitive Deficit: A Preliminary Study" Brain Sciences 11, no. 2: 213. https://doi.org/10.3390/brainsci11020213
APA StyleRomero-Ayuso, D., Cuerda, C., Morales, C., Tesoriero, R., Triviño-Juárez, J. M., Segura-Fragoso, A., & Gallud, J. A. (2021). Activities of Daily Living and Categorization Skills of Elderly with Cognitive Deficit: A Preliminary Study. Brain Sciences, 11(2), 213. https://doi.org/10.3390/brainsci11020213