
Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability

 ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. The SSST
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Descriptive Analysis
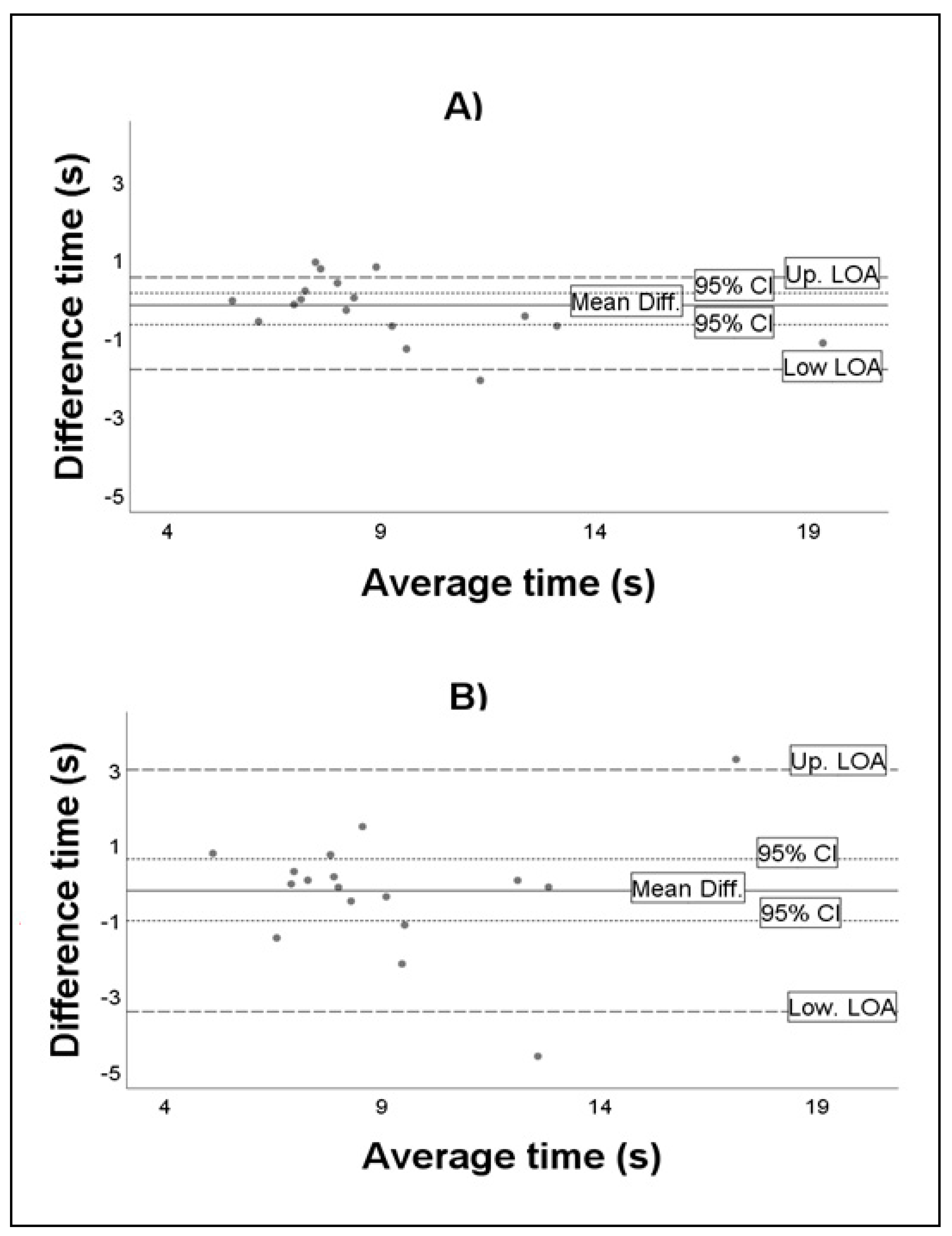
3.2. Test–Retest within-Day and Day-to-Day Reliability Analyses
3.3. Validity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eichstaedt, C.B. Physical Activity for Individuals with Mental Retardation: Infancy through Adulthood; Human Kinetics: Champaign, IL, USA, 1992. [Google Scholar]
- Hale, L.; Miller, R.; Barach, A.; Skinner, M.; Gray, A. Motor Control Test responses to balance perturbations in adults with an intellectual disability. J. Intellect. Dev. Disabil. 2009, 34, 81–86. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Enkelaar, L.; Smulders, E.; Valk, H.V.S.L.-D.; Geurts, A.C.; Weerdesteyn, V. A review of balance and gait capacities in relation to falls in persons with intellectual disability. Res. Dev. Disabil. 2012, 33, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C. Motor proficiency differences among students with intellectual disabilities, autism, and developmental disability. J. Exerc. Rehabil. 2018, 14, 275–281. [Google Scholar] [CrossRef]
- Carmeli, E.; Bar-Yossef, T.; Ariav, C.; Levy, R.; Liebermann, D.G. Perceptual-motor coordination in persons with mild intellectual disability. Disabil. Rehabil. 2008, 30, 323–329. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; García-Soidán, J.L.; García-Liñeira, J. Percentiles and Reference Values for the Accelerometric Assessment of Static Balance in Women Aged 50–80 Years. Sensors 2020, 20, 940. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.M.; Thomas, M.J. Promoting Physical Activity and Exercise in Older Adults with Developmental Disabilities. Top. Geriatr. Rehabil. 2008, 24, 64–73. [Google Scholar] [CrossRef]
- Cleaver, S.; Hunter, D.; Ouellette-Kuntz, H. Physical mobility limitations in adults with intellectual disabilities: A systematic review. J. Intellect. Disabil. Res. 2009, 53, 93–105. [Google Scholar] [CrossRef]
- Anderson-Mooney, A.J.; Schmitt, F.A.; Head, E.; Lott, I.T.; Heilman, K.M. Gait dyspraxia as a clinical marker of cognitive decline in Down syndrome: A review of theory and proposed mechanisms. Brain Cogn. 2016, 104, 48–57. [Google Scholar] [CrossRef]
- Bruce-Keller, A.J.; Ms, R.M.B.; Tudor-Locke, C.; Bs, H.C.F.; Gahan, W.P.; Correa, J.B.; Bs, D.M.N.; Keller, J.N. Assessment of Cognition, Physical Performance, and Gait in the Context of Mild Cognitive Impairment and Dementia. J. Am. Geriatr. Soc. 2012, 60, 176–177. [Google Scholar] [CrossRef]
- Oppewal, A.; Hilgenkamp, T.I.M.; Van Wijck, R.; Evenhuis, H.M. Feasibility and outcomes of the Berg Balance Scale in older adults with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 2743–2752. [Google Scholar] [CrossRef]
- Blomqvist, S.; Wester, A.; Sundelin, G.; Rehn, B. Test–retest reliability, smallest real difference and concurrent validity of six different balance tests on young people with mild to moderate intellectual disability. Physiotherapy 2012, 98, 313–319. [Google Scholar] [CrossRef]
- Hale, L.; Bray, A.; Littmann, A. Assessing the balance capabilities of people with profound intellectual disabilities who have experienced a fall. J. Intellect. Disabil. Res. 2007, 51, 260–268. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; García-Soidán, J.L.; Romo-Pérez, V. Analyzing the Use of Accelerometers as a Method of Early Diagnosis of Alterations in Balance in Elderly People: A Systematic Review. Sensors 2019, 19, 3883. [Google Scholar] [CrossRef]
- Nieuwenhuis, M.M.; Van Tongeren, H.; Sørensen, P.S.; Ravnborg, M. The Six Spot Step Test: A new measurement for walking ability in multiple sclerosis. Mult. Scler. J. 2006, 12, 495–500. [Google Scholar] [CrossRef]
- Callesen, J.; Richter, C.; Kristensen, C.; Sunesen, I.; Næsby, M.; Dalgas, U.; Skjerbæk, A.G. Test–retest agreement and reliability of the Six Spot Step Test in persons with multiple sclerosis. Mult. Scler. J. 2017, 25, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Fritz, N.E.; Jiang, A.; Keller, J.; Zackowski, K.M. Utility of the Six-Spot Step Test as a Measure of Walking Performance in Ambulatory Individuals with Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2016, 97, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Lindvall, M.A.; Anderzén-Carlsson, A.; Appelros, P.; Forsberg, A. Validity and test–retest reliability of the six-spot step test in persons after stroke. Physiother. Theory Pr. 2018, 36, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Kreutzfeldt, M.; Andersen, H.; Jensen, H.B.; Markvardsen, L.H.; Sindrup, S.H.; Ravnborg, M. The six-spot-step test—A new method for monitoring walking ability in patients with chronic inflammatory polyneuropathy. J. Peripher. Nerv. Syst. 2017, 22, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Spanish Institute of Statistics. Survey on Disabilities, Personal Autonomy and Dependency Situations; Spanish Institute of Statistics: Madrid, Spain, 2020. [Google Scholar]
- Langford, Z. The Four Square Step Test. J. Physiother. 2015, 61, 162. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Christopher, A.; Kraft, E.; Olenick, H.; Kiesling, R.; Doty, A. The reliability and validity of the Timed Up and Go as a clinical tool in individuals with and without disabilities across a lifespan: A systematic review. Disabil. Rehabil. 2019, 1, 1–15. [Google Scholar] [CrossRef]
- Dite, W.; Temple, V.A. A clinical test of stepping and change of direction to identify multiple falling older adults. Arch. Phys. Med. Rehabil. 2002, 83, 1566–1571. [Google Scholar] [CrossRef]
- Whitney, S.L.; Marchetti, G.F.; Morris, L.O.; Sparto, P.J. The Reliability and Validity of the Four Square Step Test for People With Balance Deficits Secondary to a Vestibular Disorder. Arch. Phys. Med. Rehabil. 2007, 88, 99–104. [Google Scholar] [CrossRef]
- Moore, M.; Barker, K. The validity and reliability of the four square step test in different adult populations: A systematic review. Syst. Rev. 2017, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cabeza-Ruiz, R.; Alcántara-Cordero, F.J.; Ruiz-Gavilán, I.; Sánchez-López, A.M. Feasibility and Reliability of a Physical Fitness Test Battery in Individuals with Down Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 2685. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional Reach: A New Clinical Measure of Balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Katz-Leurer, M.; Fisher, I.; Neeb, M.; Schwartz, I.; Carmeli, E. Reliability and validity of the modified functional reach test at the sub-acute stage post-stroke. Disabil. Rehabil. 2009, 31, 243–248. [Google Scholar] [CrossRef]
- Merchán-Baeza, J.A.; González-Sánchez, M.; Cuesta-Vargas, A.I. Reliability in the Parameterization of the Functional Reach Test in Elderly Stroke Patients: A Pilot Study. BioMed. Res. Int. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Brauer, S.G.; Burns, Y.; Galley, P. Lateral reach: A clinical measure of medio-lateral postural stability. Physiother. Res. Int. 1999, 4, 81–88. [Google Scholar] [CrossRef]
- Berg, K. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Berg, K.O.; Maki, B.E.; Williams, J.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar]
- Godi, M.; Franchignoni, F.; Caligari, M.; Giordano, A.; Turcato, A.M.; Nardone, A. Comparison of Reliability, Validity, and Responsiveness of the Mini-BESTest and Berg Balance Scale in Patients with Balance Disorders. Phys. Ther. 2013, 93, 158–167. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Atkinson, G.; Nevill, A.M. Statistical Methods for Assessing Measurement Error (Reliability) in Variables Relevant to Sports Medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- McManus, I.C. The misinterpretation of the standard error of measurement in medical education: A primer on the problems, pitfalls and peculiarities of the three different standard errors of measurement. Med. Teach. 2012, 34, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Pavan, K.; Tilbery, C.P.; Lianza, S.; Marangoni, B.E.M. Validation of the “Six Step Spot Test” for gait among patients with multiple sclerosis in Brazil. Arq. Neuro-Psiquiatr. 2010, 68, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Brincks, J.; Callesen, J.; Dalgas, U.; Johnsen, E. Test–retest reliability and limits of agreement of the Six-Spot Step Test in people with Parkinson’s disease. Clin. Rehabil. 2019, 33, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Lexell, J.; Flansbjer, U.-B.; Holmbäck, A.M.; Downham, D.; Patten, C. Reliability of Gait Performance Tests in Men and Women with Hemiparesis after Stroke. J. Rehabil. Med. 2005, 37, 75–82. [Google Scholar] [CrossRef]
- Valet, M.; Lejeune, T.; Devis, M.; Van Pesch, V.; El Sankari, S.; Stoquart, G. Timed Up-and-Go and 2-Minute Walk Test in patients with multiple sclerosis with mild disability: Reliability, responsiveness and link with perceived fatigue. Eur. J. Phys. Rehabil. Med. 2019, 55, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Motl, R.W.; Sosnoff, J.J.; Pula, J.H. Further validation of the Six-Spot Step Test as a measure of ambulation in multiple sclerosis. Gait Posture 2015, 41, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.L.; Stratford, P.W. Interpreting Validity Indexes for Diagnostic Tests: An Illustration Using the Berg Balance Test. Phys. Ther. 1999, 79, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, R.; Kröger, I.; Taraldsen, K.; Mellone, S.; Ihlen, E.A.; Vereijken, B.; Helbostad, J.; Becker, C.; Mikolaizak, A.S. Predicting Advanced Balance Ability and Mobility with an Instrumented Timed Up and Go Test. Sensors 2020, 20, 4987. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 18) | Men (n = 11) | Women (n = 7) |
|---|---|---|---|
| Age (years) | 31.8 ± 9.9 | 30.5 ± 9.3 | 34.1 ± 10.7 |
| Height (cm) | 163.7 ± 0.1 | 165.6 ± 0.1 | 162 ± 0.1 |
| Weight (kg) | 74.1 ± 24.5 | 65.6 ± 14.4 * | 88.4 ± 31.9 * |
| BMI (kg/m2) | 27.4 ± 8 | 23.7 ± 3.9 * | 33 ± 9.6 * |
| MMSE (points) | 25.2 ± 6 | 27.9 ± 6.4 | 23.4 ± 5.7 |
| TUG (s) | 8.4 ± 2.4 | 7.7 ± 2.6 | 9.3 ± 2.1 |
| FST (s) | 9.3 ± 3.7 | 8.1 ± 2.9 | 11.2 ± 4.4 |
| FRT (cm) | 22.2 ± 11.5 | 22.8 ± 12.4 | 21.2 ± 11.1 |
| LRT–R (cm) | 11.8 ± 5.2 | 13.6 ± 4.4 | 8.5 ± 5.4 |
| LRT–L (cm) | 12.6 ± 5.1 | 14.3 ± 4.9 | 10 ± 4.8 |
| BBS (points) | 49.9 ± 6.4 | 50.8 ± 6.8 | 48.6 ± 6.2 |
| ICAP–GF (points) | 81.4 ± 6.8 | 81.1 ± 7.1 | 81.9 ± 6.4 |
| All (n = 18) | Men (n = 11) | Women (n = 7) | ||||
|---|---|---|---|---|---|---|
| ± SD | 95% CI | ± SD | 95% CI | ± SD | 95% CI | |
| Chronometer | ||||||
| First test | 9.1 ± 3.2 | [7.4–10.7] | 8.3 ± 2.1 | [6.8–9.9] | 10.1 ± 4.2 | [6.2–14] |
| Second test | 9.4 ± 3.6 | [7.5–11.2] | 8.9 ± 2.6 | [7–10.7] | 10.1 ± 4.8 | [5.6–14.5] |
| Third test | 9.3 ± 3 | [7.8–10.9] | 9.3 ± 3 | [7.2–11.5] | 9.3 ± 3.3 | [6.2–12.3] |
| Video Camera | ||||||
| First test | 8.4 ± 3.3 | [6.7–10.1] | 7.8 ± 2.4 | [6.1–9.5] | 9.2 ± 4.4 | [5.2–13.3] |
| Second test | 8.5 ± 3.2 | [6.9–10.1] | 8.2 ± 2.4 | [6.2–10.2] | 8.9 ± 3.8 | [5.4–12.3] |
| Third test | 8.8 ± 3.1 | [7.1–10.4] | 8.7 ± 3 | [6.5–10.8] | 9 ± 3.5 | [5.3–12.6] |
| ICC | 95% CI | CV (%) | SEM | Mean Difference | 95% CI | Upper LOA | Lower LOA | |
|---|---|---|---|---|---|---|---|---|
| Chronometer | ||||||||
| Within-day agreement | 0.97 | 0.92–0.99 | 4.69 | 0.59 | −0.3 | −0.4–0.11 | 1.26 | −1.85 |
| Day-to-day agreement | 0.86 | 0.66–0.95 | 7.3 | 1.16 | −0.26 | −1.1–0.59 | 2.96 | −3.47 |
| Video Camera | ||||||||
| Within-day agreement | 0.96 | 0.9–0.99 | 6.71 | 0.62 | −0.99 | −0.59–0.4 | 0.83 | −2.8 |
| Day-to-day agreement | 0.88 | 0.71–0.96 | 6.79 | 1.07 | −0.32 | −1.17–0.52 | 2.77 | −3.42 |
| Chronometer | Video Camera | ||
|---|---|---|---|
| First Test | Second Test | Third Test | |
| First test | 0.976 * | 0.941 * | 0.876 * |
| Second test | 0.973 * | 0.975 * | 0.930 * |
| Third test | 0.844 * | 0.928 * | 0.984 * |
| Variables Included | Chronometer | Video | ||||
|---|---|---|---|---|---|---|
| B | SE | R2 | B | SE | R2 | |
| TUG | 0.652 | 0.302 | 0.25 * | 0.731 | 0.307 | 0.29 * |
| FSST | 0.765 | 0.123 | 0.76 *** | 0.837 | 0.107 | 0.83 *** |
| FRT | −0.143 | 0.06 | 0.27 * | −0.148 | 0.064 | 0.26 * |
| LRT–R | −0.329 | 0.133 | 0.29 * | −0.283 | 0.149 | 0.19 |
| LRT–L | −0.068 | 0.16 | 0.01 | −0.082 | 0.168 | 0.02 |
| BBS | −0.303 | 0.1 | 0.38 ** | −0.315 | 0.105 | 0.33 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reguera-García, M.M.; Leirós-Rodríguez, R.; Fernández-Baro, E.; Álvarez-Barrio, L. Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability. Brain Sci. 2021, 11, 201. https://doi.org/10.3390/brainsci11020201
Reguera-García MM, Leirós-Rodríguez R, Fernández-Baro E, Álvarez-Barrio L. Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability. Brain Sciences. 2021; 11(2):201. https://doi.org/10.3390/brainsci11020201
Chicago/Turabian StyleReguera-García, María Mercedes, Raquel Leirós-Rodríguez, Eva Fernández-Baro, and Lorena Álvarez-Barrio. 2021. "Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability" Brain Sciences 11, no. 2: 201. https://doi.org/10.3390/brainsci11020201
APA StyleReguera-García, M. M., Leirós-Rodríguez, R., Fernández-Baro, E., & Álvarez-Barrio, L. (2021). Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability. Brain Sciences, 11(2), 201. https://doi.org/10.3390/brainsci11020201