
SIRT1 Contributes as an Invasiveness Marker in Pituitary Adenoma


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. Associations of SIRT1 rs3818292, rs3758391, rs7895833 with PA Development
4.2. Associations of SIRT1 rs3818292, rs3758391, rs7895833 with PA Development by PA’s Hormonal Activity, Invasiveness, and Recurrence
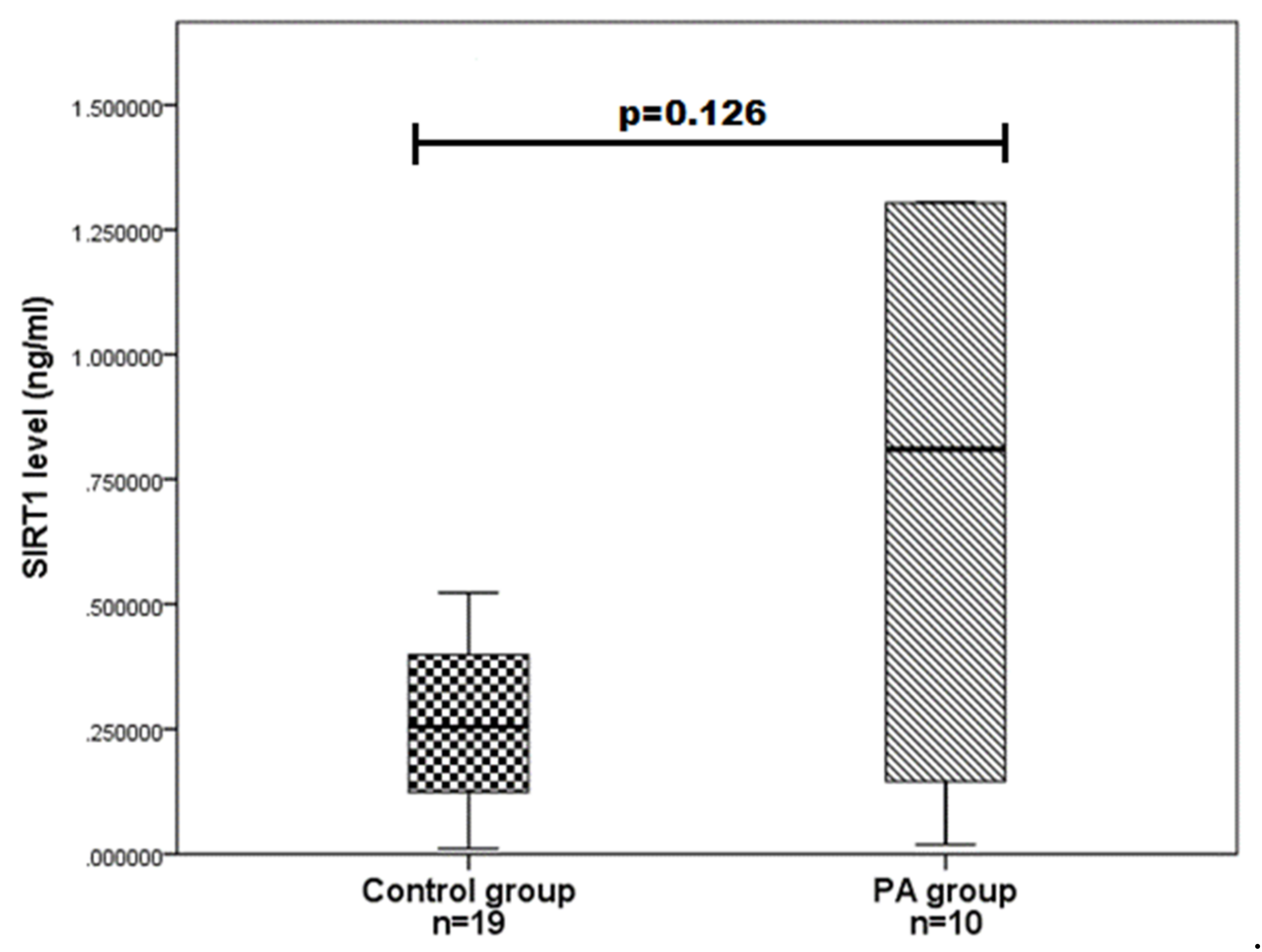
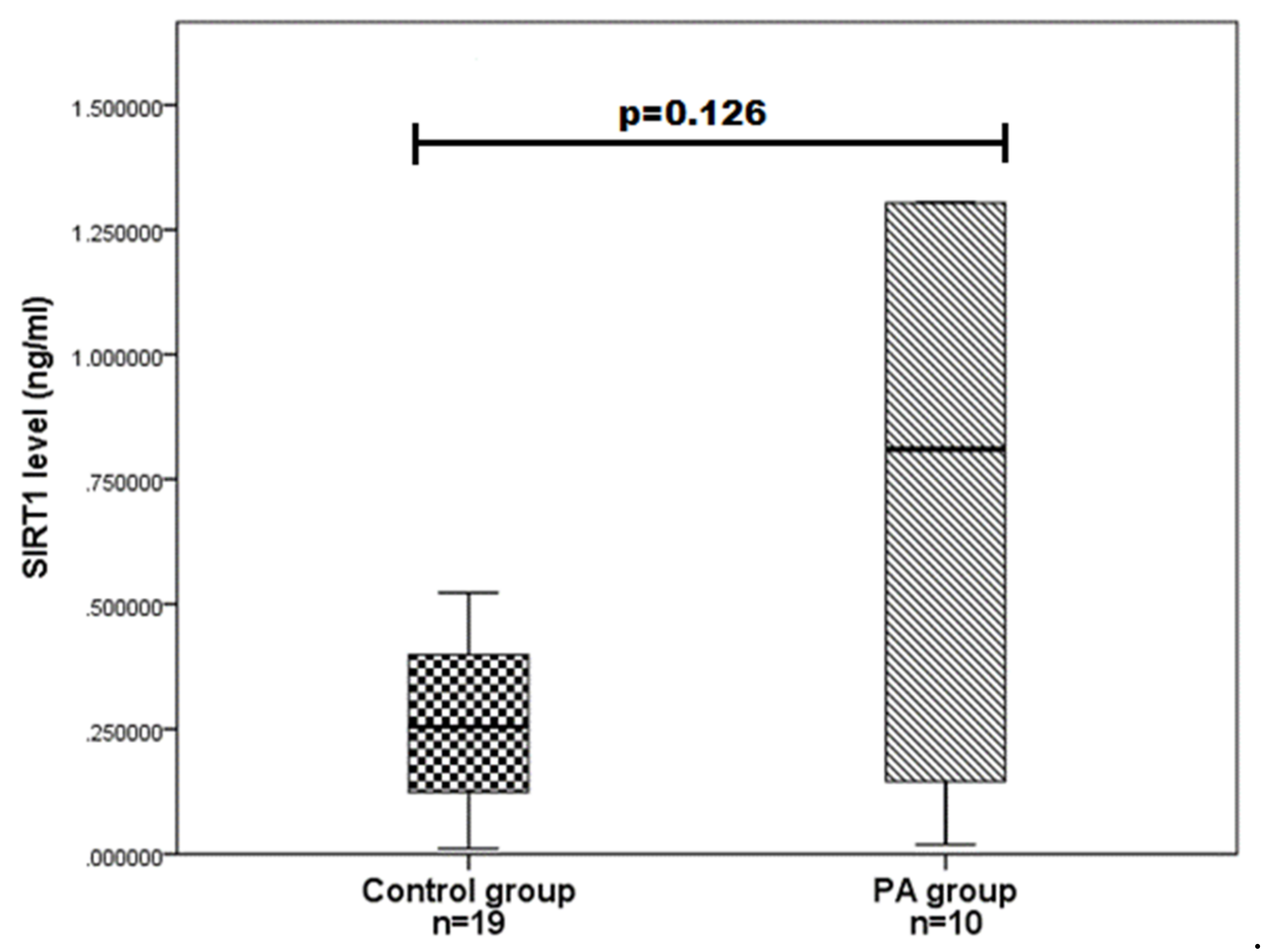
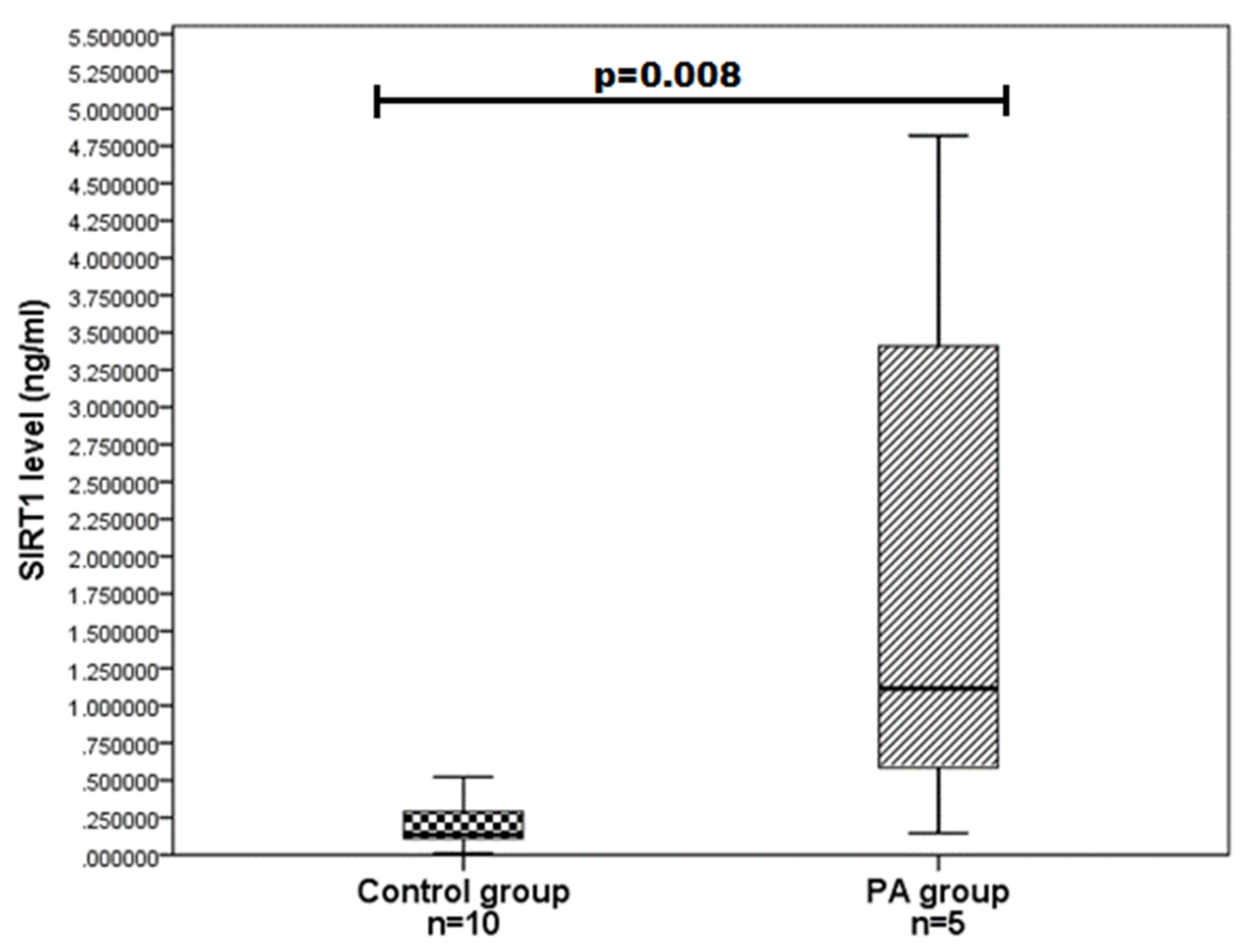
4.3. SIRT1 Serum Levels in PA Patients and Controls
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, G.K.; Payne, S.C.; Jane, J.A. Anatomy, physiology, and laboratory evaluation of the pituitary gland. Otolaryngol. Clin. N. Am. 2016, 49, 21–32. [Google Scholar] [CrossRef]
- Melmed, S. Pathogenesis of pituitary tumors. Nat. Rev. Endocrinol. 2011, 7, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Mete, O.; Lopes, M.B.; Asa, S.L. Spindle cell oncocytomas and granular cell tumors of the pituitary are variants of pituicytoma. Am. J. Surg. Pathol. 2013, 37, 1694–1699. [Google Scholar] [CrossRef]
- Ezzat, S.; Asa, S.L.; Couldwell, W.T.; Barr, C.E.; Dodge, W.E.; Vance, M.L. The prevalence of pituitary adenomas. Cancer 2004, 101, 613–619. [Google Scholar] [CrossRef]
- Carafa, V.; Altucci, L.; Nebbioso, A. Dual tumor suppressor and tumor promoter action of sirtuins in determining malignant phenotype. Front. Pharmacol. 2019, 30, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kan, Y.; Ge, P.; Wang, X.; Xiao, G.; Zhao, H. SIRT1 rs3758391 polymorphism and risk of diffuse large B cell lymphoma in a Chinese population. Cancer Cell Int. 2018, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Grande, I.P.; Amorim, P.V.; Jallad, R.S.; Musolino, N.R.; Cescato, V.A.; da Silva, G.O.; Bronstein, M.D.; Trarbach, E.B. Differential gene expression of sirtuins between somatotropinomas and nonfunctioning pituitary adenomas. Pituitary 2018, 21, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Zhou, R.; Yu, S.; Yu, S.; Cui, Z.; Hu, P.; Liu, J.; Qiao, Q.; Zhang, J. Cytoplasmic SIRT1 inhibits cell migration and invasion by impeding epithelial–mesenchymal transition in ovarian carcinoma. Mol. Cell. Biochem. 2019, 459, 157–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.C.; Jeng, Y.M.; Yuan, R.H.; Hsu, H.C.; Chen, Y.L. SIRT1 promotes tumorigenesis and resistance to chemotherapy in hepatocellular carcinoma and its expression predicts poor prognosis. Ann. Surg. Oncol. 2012, 19, 2011–2019. [Google Scholar] [CrossRef]
- Sung, J.Y.; Kim, R.; Kim, J.E.; Lee, J. Balance between SIRT1 and DBC1 expression is lost in breast cancer. Cancer Sci. 2010, 101, 1738–1744. [Google Scholar] [CrossRef]
- Huffman, D.M.; Grizzle, W.E.; Bamman, M.M.; Kim, J.S.; Eltoum, I.A.; Elgavish, A.; Nagy, T.R. SIRT1 is significantly elevated in mouse and human prostate cancer. Cancer Res. 2007, 67, 6612–6618. [Google Scholar] [CrossRef] [Green Version]
- Jang, K.Y.; Kim, K.S.; Hwang, S.H.; Kwon, K.S.; Kim, K.R.; Park, H.S.; Park, B.H.; Chung, M.J.; Kang, M.J.; Lee, D.G.; et al. Expression and prognostic significance of SIRT1 in ovarian epithelial tumours. Pathology 2009, 41, 366–371. [Google Scholar] [CrossRef]
- Cha, E.J.; Noh, S.J.; Kwon, K.S.; Kim, C.Y.; Park, B.H.; Park, H.S.; Lee, H.; Chung, M.J.; Kang, M.J.; Lee, D.G.; et al. Expression of DBC1 and SIRT1 is associated with poor prognosis of gastric carcinoma. Clin. Cancer Res. 2009, 15, 4453–4459. [Google Scholar] [CrossRef] [Green Version]
- Stunkel, W.; Peh, B.K.; Tan, Y.C.; Nayagam, V.M.; Wang, X.; Salto-Tellez, M.; Ni, B.; Entzeroth, M.; Wood, J. Function of the SIRT1 protein deacetylase in cancer. Biotechnol. J. 2007, 2, 1360–1368. [Google Scholar] [CrossRef]
- Liu, G.; Yuan, X.; Zeng, Z.; Tunici, P.; Ng, H.; Abdulkadir, I.R.; Lu, L.; Irvin, D.; Black, K.L.; Yu, J.S. Analysis of gene expression and chemoresistance of CD133+ cancer stem cells in glioblastoma. Mol. Cancer 2006, 5, 67. [Google Scholar] [CrossRef] [Green Version]
- Jang, K.Y.; Hwang, S.H.; Kwon, K.S.; Kim, K.R.; Choi, H.N.; Lee, N.R.; Kwak, J.Y.; Park, B.H.; Park, H.S.; Chung, M.J.; et al. SIRT1 expression is associated with poor prognosis of diffuse large B-cell lymphoma. Am. J. Surg. Pathol. 2008, 32, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Rizk, S.M.; Shahin, N.N.; Shaker, O.G. Association between SIRT1 gene polymorphisms and breast cancer in Egyptians. PLoS ONE 2016, 11, e0151901. [Google Scholar] [CrossRef] [Green Version]
- Shafieian, Z.; Bahari, G.; Hashemi, M.; Nakhaee, A. SIRT1 Gene Polymorphisms Are Associated with Urinary Bladder Cancer in an Iranian Population. Rep. Biochem. Mol. Biol. 2019, 8, 194–199. [Google Scholar] [PubMed]
- Lv, Y.; Lin, S.; Peng, F. SIRT1 gene polymorphisms and risk of lung cancer. Cancer Manag. Res. 2017, 9, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Shaker, O.G.; Wadie, M.S.; Ali RM, M.; Yosry, A. SIRT1 gene polymorphisms and its protein level in colorectal cancer. Gene Rep. 2017, 7, 164–168. [Google Scholar] [CrossRef]
- Glebauskiene, B.; Vilkeviciute, A.; Liutkeviciene, R.; Jakstiene, S.; Kriauciuniene, L.; Zemaitiene, R.; Zaliuniene, D. Association of FGFR2 rs2981582, SIRT1 rs12778366, STAT3 rs744166 gene polymorphisms with pituitary adenoma. Oncol. Lett. 2017, 13, 3087–3099. [Google Scholar] [CrossRef]
- Liutkeviciene, R.; Vilkeviciute, A.; Morkunaite, G.; Glebauskiene, B.; Kriauciuniene, L. SIRT1 (rs3740051) role in pituitary adenoma development. BMC Med. Genet. 2019, 20, 185. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, H.; Dessain, S.K.; Ng Eaton, E.; Imai, S.I.; Frye, R.A.; Pandita, T.K.; Guarente, L.; Weinberg, R.A. hSIR2(SIRT1) functions as an NAD-dependent p53 deacetylase. Cell 2001, 107, 149–159. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.Y.; Wang, D.H.; Yen, R.C.; Luo, J.; Gu, W.; Baylin, S.B. Tumor suppressor HIC1 directly regulates SIRT1 to modulate p53-dependent DNA-damage responses. Cell 2005, 123, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Huang, Q.; Zeng, Z.; Wu, J.; Zhang, Y.; Chen, Z. Sirt1 inhibits oxidative stress in vascular endothelial cells. Oxid. Med. Cell. Longev. 2017, 2017, 7543973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, H.Y.; Miller, C.; Bitterman, K.J.; Wall, N.R.; Hekking, B.; Kessler, B.; Howitz, K.T.; Gorospe, M.; de Cabo, R.; Sinclair, D.A. Calorie restriction promotes mammalian cell survival by inducing the SIRT1 deacetylase. Science 2004, 305, 390–392. [Google Scholar] [CrossRef] [Green Version]
- Motta, M.C.; Divecha, N.; Lemieux, M.; Kamel, C.; Chen, D.; Gu, W.; Bultsma, Y.; McBurney, M.; Guarente, L. Mammalian SIRT1 represses forkhead transcription factors. Cell 2004, 116, 551–563. [Google Scholar] [CrossRef] [Green Version]
- Akieda-Asai, S.; Zaima, N.; Ikegami, K.; Kahyo, T.; Yao, I.; Hatanaka, T.; Iemura, S.I.; Sugiyama, R.; Yokozeki, T.; Eishi, Y.; et al. SIRT1 regulates thyroid-stimulating hormone release by enhancing PIP5Kγ activity through deacetylation of specific lysine residues in mammals. PLoS ONE 2010, 5, e11755. [Google Scholar] [CrossRef]
- Elibol, B.; Kilic, U. High levels of SIRT1 expression as a protective mechanism against disease-related conditions. Front. Endocrinol. 2018, 9, 614. [Google Scholar] [CrossRef]
- Kannan, V.; Brouwer, N.; Hanisch, U.K.; Regen, T.; Eggen, B.J.; Boddeke, H.W. Histone deacetylase inhibitors suppress immune activation in primary mouse microglia. J. Neurosci. Res. 2013, 91, 1133–1142. [Google Scholar] [CrossRef]
- Prozorovski, T.; Ingwersen, J.; Lukas, D.; Göttle, P.; Koop, B.; Graf, J.; Schneider, R.; Franke, K.; Schumacher, S.; Britsch, S.; et al. Regulation of sirtuin expression in autoimmune neuroinflammation: Induction of SIRT1 in oligodendrocyte progenitor cells. Neurosci. Lett. 2019, 704, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Dong, Y.T.; Xiang, J.; Xu, Y.; Hong, W.; Song, H.; Guan, Z.Z. Reduced expression of SIRT1 and SOD-1 and the correlation between these levels in various regions of the brains of patients with Alzheimer’s disease. J. Clin. Pathol. 2018, 71, 1090–1099. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.J.; Baek, H.A.; Park, H.S.; Jang, K.Y.; Moon, W.S.; Kang, M.J.; Lee, D.G.; Kim, M.H.; Lee, J.H.; Chung, M.J. Expression of SIRT1 and cortactin is associated with progression of non-small cell lung cancer. Pathol. Res. Pract. 2013, 209, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Byles, V.; Zhu, L.; Lovaas, J.D.; Chmilewski, L.K.; Wang, J.; Faller, D.V.; Dai, Y. SIRT1 induces EMT by cooperating with EMT transcription factors and enhances prostate cancer cell migration and metastasis. Oncogene 2012, 31, 4619–4629. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.X.; Li, H.; Chen, X.M.; Yang, X.H.; Wang, Q.; Wu, M.L.; Kong, Q.Y.; Li, Z.X.; Liu, J. Expression patterns and potential roles of SIRT1 in human medulloblastoma cells in vivo and in vitro. Neuropathology 2013, 33, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Mindermann, T.; Wilson, C.B. Age-related and gender-related occurrence of pituitary adenomas. Clin. Endocrinol. 1994, 41, 359–364. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | Group | p-Value | |
|---|---|---|---|
| PA, n (%) (n = 108) | Control, n (%) (n = 216) | ||
| Males | 43 (39.8) | 83 (38.4) | 1.0 |
| Females | 65 (60.2) | 133 (61.6) | 1.0 |
| Age, median, (min.–max.) | 54 (18–84) | 56 (19–94) | 0.792 |
| Hormonal activity * Active Non-active | 53 (53) 47 (47) | - | - |
| Recurrence * Non-recurrent With recurrence | 78 (78) 22 (22) | - | - |
| Invasiveness * Invasive Non-invasive | 65 (63.1) 38 (36.9) | - | - |
| SNP | Genotype/Allele | Frequency | p-Value | ||
|---|---|---|---|---|---|
| Control Group, n (%) | HWE p Value | PA, n (%) | |||
| rs3818292 | Genotype | ||||
| A/A | 190 (88) | 0.366 | 91 (88.3) | 0.865 | |
| A/G | 25 (11.6) | 11 (10.7) | |||
| G/G | 1 (0.4) | 1 (1) | |||
| All | 216 (100) | 103 (100) | |||
| Allele | |||||
| A | 405 (93.8) | 193 (93.7) | 0.976 | ||
| G | 27 (6.2) | 13 (6.3) | |||
| rs3758391 | Genotype | ||||
| C/C | 127 (58.8) | 0.941 | 52 (50.5) | 0.240 | |
| C/T | 77 (35.6) | 47 (45.6) | |||
| T/T | 12 (5.6) | 4 (3.9) | |||
| All | 216 (100) | 103 (100) | |||
| Allele | |||||
| C | 331 (76.6) | 151 (73.3) | 0.362 | ||
| T | 101 (23.4) | 55 (26.7) | |||
| rs7895833 | Genotype | ||||
| A/A | 156 (72.2) | 0.064 | 75 (72.8) | 0.178 | |
| A/G | 59 (27.3) | 25 (24.3) | |||
| G/G | 1 (0.5) | 3 (2.9) | |||
| All | 216 (100) | 103 (100) | |||
| Allele | |||||
| A | 371 (85.9) | 175 (84.9) | 0.755 | ||
| G | 61 (14.1) | 31 (15.1) | |||
| SNP | Genotype/Allele | Frequency | |||||
|---|---|---|---|---|---|---|---|
| Non-Active PA, n (%) n = 47 | Control Group, n (%) n = 216 | p-Value | Active PA, n (%) n = 53 | Control Group, n (%) n = 216 | p-Value | ||
| rs3818292 | Genotype | ||||||
| A/A | 43 (91.5) | 190 (88) | 0.833 | 45 (84.9) | 190 (88) | 0.449 | |
| A/G | 4 (8.5) | 25 (10.6) | 7 (13.2) | 25 (10.6) | |||
| G/G | 0 (0) | 1 (0.4) | 1 (1.9) | 1 (0.4) | |||
| Allele | |||||||
| A | 90 (95.7) | 405 (93.8) | 0.457 | 97 (91.5) | 405 (93.8) | 0.408 | |
| G | 4 (4.3) | 27 (6.2) | 9 (8.5) | 27 (6.2) | |||
| rs3758391 | Genotype | ||||||
| C/C | 22 (46.8) | 127 (58.8) | 0.115 | 28 (52.8) | 127 (58.8) | 0.693 | |
| C/T | 24 (51.1) | 77 (35.6) | 22 (41.5) | 77 (35.6) | |||
| T/T | 1 (2.1) | 12 (5.6) | 3 (5.7) | 12 (5.6) | |||
| Allele | |||||||
| C | 68 (72.3) | 331 (76.6) | 0.379 | 78 (73.6) | 331 (76.6) | 0.512 | |
| T | 26 (27.7) | 101 (23.4) | 28 (26.4) | 101 (23.4) | |||
| rs7895833 | Genotype | ||||||
| A/A | 36 (72) | 156 (72.2) | 0.767 | 36 (67.9) | 156 (72.2) | 0.02 | |
| A/G | 11 (27.5) | 59 (27.3) | 14 (26.4) | 59 (27.3) | |||
| G/G | 0 (0) | 1 (0.5) | 3 (5.7) | 1 (0.5) | |||
| Allele | |||||||
| A | 83 (88.3) | 371 (85.9) | 0.536 | 86 (81.1) | 371 (85.9) | 0.221 | |
| G | 11 (11.7) | 61 (14.1) | 20 (18.9) | 61 (14.1) | |||
| rs7895833 | ||||
|---|---|---|---|---|
| Genetic Model | Genotype/Allele | OR (95 % CI) | p Value | AIK |
| Codominant | A/A | 1 | 265.173 | |
| A/G | 1.028 (0.518–2.042) | 0.937 | ||
| G/G | 13 (1.314–128.632) | 0.028 | ||
| Dominant | A/A | 1 | 268.605 | |
| A/G + G/G | 1.228 (0.642–2.350) | 0.536 | ||
| Recessive | A/A + A/G | 1 | 263,179 | |
| G/G | 12.9 (1.314–126.624) | 0.028 | ||
| Overdominant | A/A + G/G | 1 | 268.966 | |
| A/G | 0.955 (0.484–1.886) | 0.895 | ||
| Additive | G | 1.451 (0.812–2.592) | 0.209 | 267.452 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaiciulis, D.; Vilkeviciute, A.; Gedvilaite, G.; Glebauskiene, B.; Kriauciuniene, L.; Liutkeviciene, R. SIRT1 Contributes as an Invasiveness Marker in Pituitary Adenoma. Brain Sci. 2021, 11, 1638. https://doi.org/10.3390/brainsci11121638
Vaiciulis D, Vilkeviciute A, Gedvilaite G, Glebauskiene B, Kriauciuniene L, Liutkeviciene R. SIRT1 Contributes as an Invasiveness Marker in Pituitary Adenoma. Brain Sciences. 2021; 11(12):1638. https://doi.org/10.3390/brainsci11121638
Chicago/Turabian StyleVaiciulis, Domantas, Alvita Vilkeviciute, Greta Gedvilaite, Brigita Glebauskiene, Loresa Kriauciuniene, and Rasa Liutkeviciene. 2021. "SIRT1 Contributes as an Invasiveness Marker in Pituitary Adenoma" Brain Sciences 11, no. 12: 1638. https://doi.org/10.3390/brainsci11121638
APA StyleVaiciulis, D., Vilkeviciute, A., Gedvilaite, G., Glebauskiene, B., Kriauciuniene, L., & Liutkeviciene, R. (2021). SIRT1 Contributes as an Invasiveness Marker in Pituitary Adenoma. Brain Sciences, 11(12), 1638. https://doi.org/10.3390/brainsci11121638