
Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review

 ,
,  ,
,  , ,
, , 
 , ,
, , 


 ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Synthesis
2.4. Study Quality
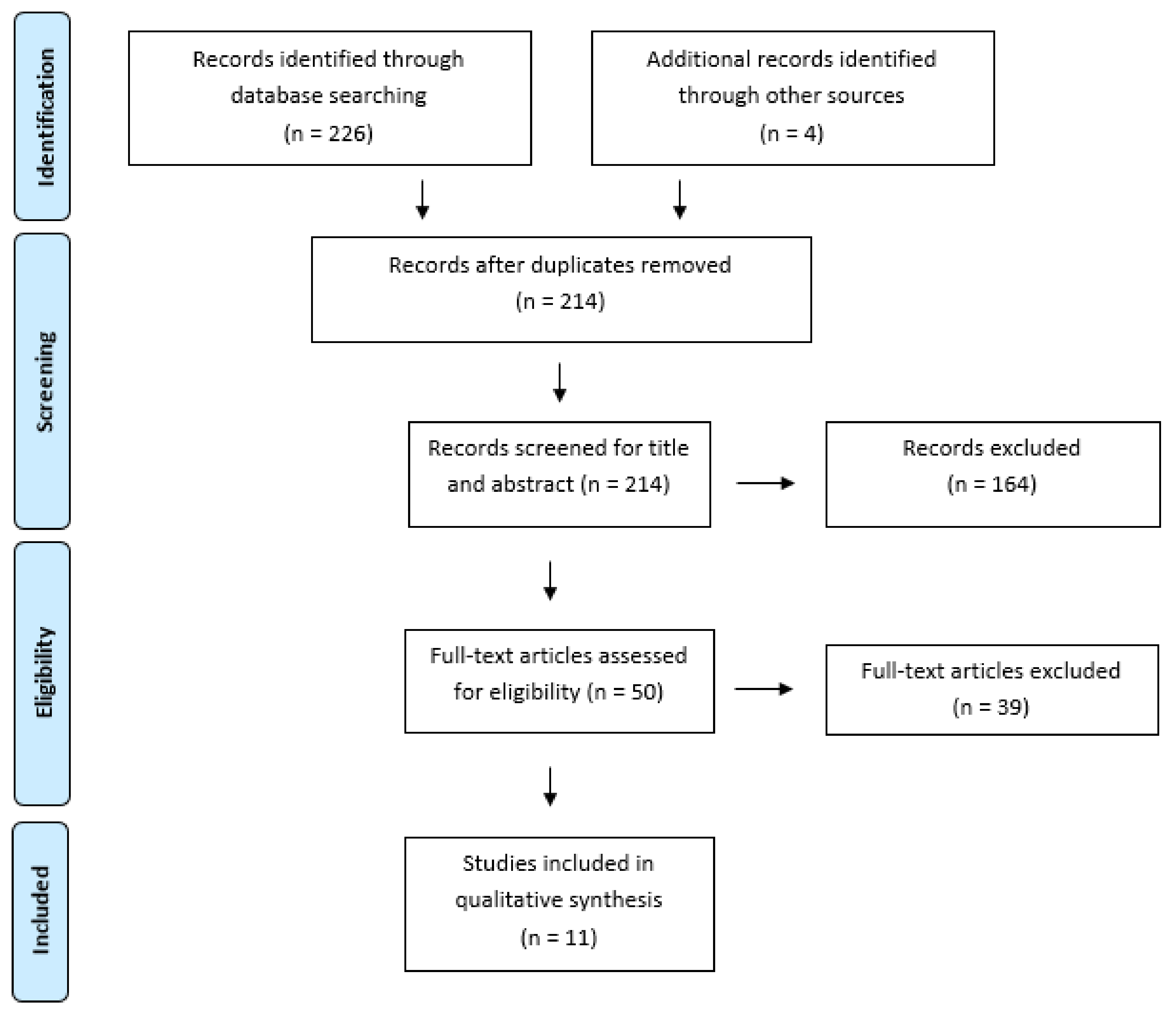
3. Results
3.1. Evidence Synthesis
3.2. Evidence Level and Study Quality of the Included Studies
3.3. Clinical Characteristics of Study Participants
3.4. Robotic Rehabilitation Characteristics
3.5. Main Findings of the Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, X.; Battistuzzo, C.R.; Zoghi, M.; Galea, M.P. Effects of training on upper limb function after cervical spinal cord injury: A systematic review. Clin. Rehabil. 2015, 29, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Stampas, A.; Tansey, K.E. Spinal cord injury medicine and rehabilitation. Semin. Neurol. 2014, 34, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, M.; de Sire, A.; Renò, F.; Cisari, C.; Runza, L.; Baricich, A.; Carda, S.; Fusco, N. Spinal Cord Injury as a Model of Bone-Muscle Interactions: Therapeutic Implications From in vitro and in vivo Studies. Front. Endocrinol. 2020, 11, 204. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Fusco, N. Rethinking the clinical management of volumetric muscle loss in patients with spinal cord injury: Synergy among nutritional supplementation, pharmacotherapy, and rehabilitation. Curr Opin Pharmacol. 2021, 57, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Pickett, G.E.; Campos-Benitez, M.; Keller, J.L.; Duggal, N. Epidemiology of traumatic spinal cord injury in Canada. Spine 2006, 31, 799–805. [Google Scholar] [CrossRef]
- Herrmann, K.H.; Kirchberger, I.; Biering-Sørensen, F.; Cieza, A. Differences in functioning of individuals with tetraplegia and paraplegia according to the International Classification of Functioning, Disability and Health (ICF). Spinal Cord 2011, 49, 534–543. [Google Scholar] [CrossRef]
- Spinal Cord Injury (SCI) Facts and Figures at a Glance. J. Spinal Cord Med. 2016, 42016, 493–494.
- Brogioli, M.; Schneider, S.; Popp, W.; Albisser, U.; Brust, A.K.; Velstra, I.-M.; Gassert, R.; Curt, A.; Starkey, M.L. Monitoring upper limb recovery after cervical spinal cord injury: Insights beyond assessment scores. Front. Neurol. 2016, 7, 142. [Google Scholar] [CrossRef]
- Anderson, K.D. Targeting recovery: Priorities of the spinal cord-injured population. J. Neurotrauma 2004, 21, 1371–1383. [Google Scholar] [CrossRef]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 11, CD006073. [Google Scholar] [CrossRef]
- Edgerton, V.R.; Roy, R.R. Robotic training and spinal cord plasticity. Brain Res. Bull. 2009, 78, 4–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Riener, R. Rehabilitation robotics. Found. Trends Robot. 2013, 3, 1–137. [Google Scholar]
- Morone, G.; Cocchi, I.; Paolucci, S.; Iosa, M. Robot-assisted therapy for arm recovery for stroke patients: State of the art and clinical implication. Expert Rev. Med. Devices 2020, 17, 223–233. [Google Scholar] [CrossRef]
- Turner, D.L.; Ramos-Murguialday, A.; Birbaumer, N.; Hoffmann, U.; Luft, A. Neurophysiology of robot-mediated training and therapy: A perspective for future use in clinical populations. Front. Neurol. 2013, 4, 184. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef]
- Tramontano, M.; Morone, G.; Palomba, A.; De Angelis, S.; Mercuro, A.; Caltagirone, C.; Grasso, M.G. Effectiveness of a sensor-based technology in upper limb motor recovery in post-acute stroke neurorehabilitation: A randomized controlled trial. J. Biol. Regul. Homeost. Agents 2020, 34, 165–174. [Google Scholar]
- Tramontano, M.; Morone, G.; De Angelis, S.; Casagrande Conti, L.; Galeoto, G.; Grasso, M.G. Sensor-based technology for upper limb rehabilitation in patients with multiple sclerosis: A randomised controlled trial. Restor. Neurol. Neurosci. 2020, 38, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Palomba, A.; Cinnera, A.M.; Agostini, M.; Aprile, I.; Arienti, C.; Paci, M.; Casanova, E.; Marino, D.; LA Rosa, G.; et al. “CICERONE” Italian Consensus Conference on Robotic in Neurorehabilitation. Systematic review of guidelines to identify recommendations for upper limb robotic rehabilitation after stroke. Eur. J. Phys. Rehabil. Med. 2021, 57, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Gimigliano, F.; Palomba, A.; Arienti, C.; Morone, G.; Perrero, L.; Agostini, M.; Aprile, I.; Paci, M.; Casanova, E.; Marino, D.; et al. Italian Consensus Conference on Robotics in Neurorehabilitation (CICERONE). Robot-assisted arm therapy in neurological health conditions: Rationale and methodology for the evidence synthesis in the CICERONE Italian Consensus Conference. Eur. J. Phys. Rehabil. Med. 2021, 57, 824–830. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy evidence database (PEDro) scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Zariffa, J.; Kapadia, N.; Kramer, J.L.K.; Taylor, P.; Alizadeh-Meghrazi, M.; Zivanovic, V.; Willms, R.; Townson, A.; Curt, A.; Popovic, M.R.; et al. feasibility and efficacy of upper limb robotic rehabilitation in a subacute cervical spinal cord injury population. Spinal Cord 2012, 50, 220–226. [Google Scholar] [CrossRef]
- Cortes, M.; Elder, J.; Rykman, A.; Murray, L.; Avedissian, M.; Stampas, A.; Thickbroom, G.W.; Pascual-Leone, A.; Krebs, H.I.; Valls-Sole, J.; et al. Improved motor performance in chronic spinal cord injury following upper-limb robotic training. NeuroRehabilitation 2013, 33, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Fitle, K.D.; Pehlivan, A.U.; O’Malley, M.K. A Robotic Exoskeleton for rehabilitation and assessment of the upper limb following incomplete spinal cord injury. In Proceedings of the IEEE International Conference on Robotics and Automation, Seattle, WA, USA, 26–30 May 2015; pp. 4960–4966. [Google Scholar]
- Vanmulken, D.A.; Spooren, A.I.; Bongers, H.M.; Seelen, H.A. Robot-assisted task-oriented upper extremity skill training in cervical spinal cord injury: A feasibility study. Spinal Cord 2015, 53, 547–551. [Google Scholar] [CrossRef]
- Francisco, G.E.; Yozbatiran, N.; Berliner, J.; O’Malley, M.K.; Pehlivan, A.U.; Kadivar, Z.; Fitle, K.; Boake, C. Robot-Assisted Training of Arm and Hand Movement Shows Functional Improvements for Incomplete Cervical Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2017, 96, S171–S177. [Google Scholar] [CrossRef] [PubMed]
- Frullo, J.M.; Elinger, J.; Pehlivan, A.U.; Fitle, K.; Nedley, K.; Francisco, G.E.; Sergi, F.; O’Malley,, M.K. Effects of Assist-As-Needed Upper Extremity Robotic Therapy after Incomplete Spinal Cord Injury: A Parallel-Group Controlled Trial. Front. Neurorobot. 2017, 11, 26. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, B.S.; Lee, H.-J.; Kim, H.-R.; Cho, D.-Y.; Lim, J.-E.; Kim, J.-J.; Kim, H.Y.; Han, Z.-A. Clinical efficacy of upper limb robotic therapy in people with tetraplegia: A pilot randomised controlled trial. Spinal Cord 2019, 57, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Unger, J.; Zariffa, J.; Pakosh, M.; Jaglal, S.; Craven, B.C.; Musselman, K.E. Robot-assisted upper extremity rehabilitation for cervical spinal cord injuries: A systematic scoping review. Disabil. Rehabil. Assist. Technol. 2018, 13, 704–715. [Google Scholar] [CrossRef] [PubMed]
- Yozbatiran, N.; Francisco, G.E. Robot-assisted Therapy for the Upper Limb after Cervical Spinal Cord Injury. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 367–384. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Lee, H.J.; Cho, D.Y.; Lim, J.-E.; Lee, B.S.; Kwon, S.H.; Kim, H.Y.; Lee, S.J. Effects of Combined Upper Limb Robotic Therapy in Patients with Tetraplegic Spinal Cord Injury. Ann. Rehabil. Med. 2019, 43, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Osuagwu, B.A.; Timms, S.; Peachment, R.; Dowie, S.; Thrussell, H.; Cross, S.; Shirley, R.; Segura-Fragoso, A.; Taylor, J. Home-based rehabilitation using a soft robotic hand glove device leads to improvement in hand function in people with chronic spinal cord injury:a pilot study. J. Neuroeng. Rehabil. 2020, 17, 40. [Google Scholar] [CrossRef]
- Calafiore, D.; Negrini, F.; Tottoli, N.; Ferraro, F.; Ozyemisci Taskiran, O.; de Sire, A. Efficacy of robotic exoskeleton for gait rehabilitation in patients with subacute stroke: A systematic review with meta-analysis. Eur J Phys Rehabil Med. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Cattaneo, D.; Abuarqub, S.; Ferrarin, M. Robot-based rehabilitation of the upper limbs in multiple sclerosis: Feasibility and preliminary results. J. Rehabil. Med. 2009, 41, 966–970. [Google Scholar] [CrossRef]
- Vanoglio, F.; Bernocchi, P.; Mulè, C.; Garofali, F.; Mora, C.; Taveggia, G.; Scalvini, S.; Luisa, A. Feasibility and efficacy of a robotic device for hand rehabilitation in hemiplegic stroke patients: A randomised pilot controlled study. Clin. Rehabil. 2017, 31, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Yozbatiran, N.; Keser, Z.; Davis, M.; Argyrios, S.; O’Malley, M.; Cooper-Hay, C.; Joel, F.; Fregni, F.; Gerard, F.E. Transcranial direct current stimulation (tDCS) of the primary motor cortex and robot-assisted arm training in chronic incomplete cervical spinal cord injury: A proof of concept sham-randomised clinical study. NeuroRehabilitation 2016, 39, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Pehlivan, A.U.; Celik, O.; O’Malley, M.K. Mechanical design of a distal arm exoskeleton for stroke and spinal cord injury rehabilitation. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011. [Google Scholar]


{kind=link}
| S | PI | D | E | R |
|---|---|---|---|---|
| Sample | Phenomenon of Interest | Design | Evaluation | Research Type |
| Spinal Cord Injury | Robotic rehabilitation for upper limb motor recovery | Research article | Functional and/or rehabilitative outcomes | Qualitative |
| (Spinal Cord Injury[Title/Abstract]) OR Spinal Cord Injuries[MeSH Terms] | ((((robot[Title/Abstract]) OR exoskeleton[Title/Abstract]) OR end-effector[Title/Abstract]) OR robotics[MeSH Terms]) OR Exoskeleton Device[MeSH Terms] AND (((((((upper limb[Title/Abstract]) OR upper extremity[Title/Abstract]) OR hand[Title/Abstract]) OR arm[Title/Abstract]) OR upper extremity[MeSH Terms])) | (((function[Title/Abstract]) OR rehabilitation [Title/Abstract]) OR recovery [Title/Abstract]) |
| Article | Nation | Design | Aim | Number Participants (Drop-Outs) | Gender and Age | SCI Stage | SCI According to AIS | SCI Level | Methodological Quality | CBIM |
|---|---|---|---|---|---|---|---|---|---|---|
| Zariffa 2012 [25] | Canada | Case Series | To assess the feasibility and efficacy of upper limb robotic rehabilitation device in subacute cervical SCI | 15 (3) | 14 M, 1 F 19–75 years | Subacute | AIS A (n = 2) AIS B (n = 4) AIS C (n = 1) AIS D (n = 5) | C4–C6 | n/a | 4 |
| Cortes 2013 [26] | USA | Case Series | To assess feasibility, safety, and effectiveness of robotic-assisted training in chronic SCI | 10 (0) | 8 M, 2 F 17–70 years | Chronic | AIS A (n = 3) AIS B (n = 4) AIS C (n = 1) AIS D (n = 2) | C4–C6 | n/a | 4 |
| Fitle 2015 [27] | USA | Case series | To assess feasibility and effectiveness of a robotic exoskeleton designed to train elbow, forearm and wrist movements | 10 (2) | 8 M, 2 F, age: NR | Chronic | AIS C–D (n = 2) | C2–C6 | n/a | 4 |
| Vanmulken 2015 [28] | Netherlands | Case Series | To assess feasibility and effectiveness (arm-hand function and performance) of haptic robot technology | 5 (2) | 4 M, 1 F 25–70 years | Chronic | AIS A (n = 1) AIS B (n = 2) | C3–C7 | n/a | 4 |
| Francisco 2017 [29] | USA | Case Series | To assess feasibility, tolerability, and effectiveness of robotic-assisted arm training | 10 (2) | 8 M, 2 F, 19–76 years | Chronic | AIS C (n = 4) AIS D (n = 4) | C2–C7 | n/a | 4 |
| Frullo 2017 [30] | USA | Parallel group controlled trial | To assess feasibility of subject-adaptive robotic-assisted therapy: AAN vs. ST training modality | 17 (3) | 12 M and 2 F, 3 NR 53.5 years | Chronic | AIS C–D (n = 17) | C3–C8 | n/a | 4 |
| Kim 2019 [31] | Republic of Korea | RCT | To assess the clinical efficacy of upper limb robotic therapy in people with tetraplegia | 34 (4) RT: 17 (2) CT: 17 (2) | 28 M, 6 F, RT: 56.7 ± 13.6 years CT: 47.1 ± 14.9 years | Subacute/Chronic | AIS A (n = 8) AIS B (n = 6) AIS C (n = 4) AIS D (n = 16) | C2–C8 | 8/10 | 2 |
| Singh 2018 [32] | Canada | Systematic review | To summarize feasibility and outcomes of robotic-assisted upper extremity training for patients with cervical SCI | 73 (11) | 46 M, 8 F, 7 NR 17–75 years | Subacute/Chronic | AIS A-B (n = 16) AIS C-D (n = 46) | C2–C8 | Critically low quality | 3 |
| Yozbatiran 2019 [33] | USA | Systematic review | To summarize the current evidence of robot-assisted rehabilitation in patients with tetraplegia | 88 (13) | 69 M, 13 F, 6 NR 17–76 years | Subacute/Chronic | AIS A–B (n = 14) AIS C–D (n = 58) 3 NR | C2–C7 | Low quality | 3 |
| Jung 2019 [34] | Republic of Korea | RCT | To assess the effects of combined upper limb robotic therapy (RT) as compared to conventional occupational therapy (OT) in SCI patients | 38 (8) RT: 22 (5) CT: 16 (3) | 24 M, 6 F RT: 47.23 ± 14 CT: 53 ± 13.5 | Subacute | AIS A (n = 3) AIS B (n = 4) AIS C (n = 7) AIS D (n = 16) | C2–C7 | 4/10 | 3 |
| Osuagwu 2020 [35] | UK | Interventional longitudinal clinical trial design | To investigate the therapeutic effect of a self-administered home-based hand rehabilitation programme for people with cervical SCI using the soft extra muscle (SEM) Glove | 15 (0) | 11 M, 4 F 50.3 (33–60) | Chronic | AIS C (n = 3) AIS D (n = 11) Untested (n = 1) | C2–C5 | n/a | 4 |
| Zariffa 2012 [25] | Canada | Case Series | To assess the feasibility and efficacy of upper limb robotic rehabilitation device in subacute cervical SCI | 15 (3) | 14 M, 1 F 19–75 years | Subacute | AIS A (n = 2) AIS B (n = 4) AIS C (n = 1) AIS D (n = 5) | C4–C6 | n/a | 4 |
| Cortes 2013 [26] | USA | Case Series | To assess feasibility, safety, and effectiveness of robotic-assisted training in chronic SCI | 10 (0) | 8 M, 2 F 17–70 years | Chronic | AIS A (n = 3) AIS B (n = 4) AIS C (n = 1) AIS D (n = 2) | C4–C6 | n/a | 4 |
| Fitle 2015 [27] | USA | Case series | To assess feasibility and effectiveness of a robotic exoskeleton designed to train elbow, forearm and wrist movements | 10 (2) | 8 M, 2 F, age: NR | Chronic | AIS C-D (n = 2) | C2–C6 | n/a | 4 |
| Vanmulken 2015 [28] | Netherlands | Case Series | To assess feasibility and effectiveness (arm-hand function and performance) of haptic robot technology | 5 (2) | 4 M, 1 F 25–70 years | Chronic | AIS A (n = 1) AIS B (n = 2) | C3–C7 | n/a | 4 |
| Francisco 2017 [29] | USA | Case Series | To assess feasibility, tolerability, and effectiveness of robotic-assisted arm training | 10 (2) | 8 M, 2 F, 19–76 years | Chronic | AIS C (n = 4) AIS D (n = 4) | C2–C7 | n/a | 4 |
| Frullo 2017 [30] | USA | Parallel group controlled trial | To assess feasibility of subject-adaptive robotic-assisted therapy: AAN vs. ST training modality | 17 (3) | 12 M and 2 F, 3 NR 53.5 years | Chronic | AIS C–D (n = 17) | C3–C8 | n/a | 4 |
| Kim 2019 [31] | Republic of Korea | RCT | To assess the clinical efficacy of upper limb robotic therapy in people with tetraplegia | 34 (4) RT: 17 (2) CT: 17 (2) | 28 M, 6 F, RT: 56.7 ± 13.6 years CT: 47.1 ± 14.9 years | Subacute/Chronic | AIS A (n = 8) AIS B (n = 6) AIS C (n = 4) AIS D (n = 16) | C2–C8 | 8/10 | 2 |
| Singh 2018 [32] | Canada | Systematic review | To summarize feasibility and outcomes of robotic-assisted upper extremity training for patients with cervical SCI | 73 (11) | 46 M, 8 F, 7 NR 17–75 years | Subacute/Chronic | AIS A-B (n = 16) AIS C–D (n = 46) | C2–C8 | Critically low quality | 3 |
| Yozbatiran 2019 [33] | USA | Systematic review | To summarize the current evidence of robot-assisted rehabilitation in patients with tetraplegia | 88 (13) | 69 M, 13 F, 6 NR 17–76 years | Subacute/Chronic | AIS A–B(n = 14) AIS C–D (n = 58) 3 NR | C2–C7 | Low quality | 3 |
| Jung 2019 [34] | Republic of Korea | RCT | To assess the effects of combined upper limb robotic therapy (RT) as compared to conventional occupational therapy (OT) in SCI patients | 38 (8) RT: 22 (5) CT: 16 (3) | 24 M, 6 F RT: 47.23 ± 14 CT: 53 ± 13.5 | Subacute | AIS A (n = 3) AIS B (n = 4) AIS C (n = 7) AIS D (n = 16) | C2–C7 | 4/10 | 3 |
| Osuagwu 2020 [35] | UK | Interventional longitudinal clinical trial design | To investigate the therapeutic effect of a self-administered home-based hand rehabilitation programme for people with cervical SCI using the soft extra muscle (SEM) Glove | 15 (0) | 11 M, 4 F 50.3 (33–60) | Chronic | AIS C (n = 3) AIS D (n = 11) Untested (n = 1) | C2–C5 | n/a | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morone, G.; de Sire, A.; Martino Cinnera, A.; Paci, M.; Perrero, L.; Invernizzi, M.; Lippi, L.; Agostini, M.; Aprile, I.; Casanova, E.; et al. Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review. Brain Sci. 2021, 11, 1630. https://doi.org/10.3390/brainsci11121630
Morone G, de Sire A, Martino Cinnera A, Paci M, Perrero L, Invernizzi M, Lippi L, Agostini M, Aprile I, Casanova E, et al. Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review. Brain Sciences. 2021; 11(12):1630. https://doi.org/10.3390/brainsci11121630
Chicago/Turabian StyleMorone, Giovanni, Alessandro de Sire, Alex Martino Cinnera, Matteo Paci, Luca Perrero, Marco Invernizzi, Lorenzo Lippi, Michela Agostini, Irene Aprile, Emanuela Casanova, and et al. 2021. "Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review" Brain Sciences 11, no. 12: 1630. https://doi.org/10.3390/brainsci11121630
APA StyleMorone, G., de Sire, A., Martino Cinnera, A., Paci, M., Perrero, L., Invernizzi, M., Lippi, L., Agostini, M., Aprile, I., Casanova, E., Marino, D., La Rosa, G., Bressi, F., Sterzi, S., Giansanti, D., Battistini, A., Miccinilli, S., Filoni, S., Sicari, M., ... Straudi, S., on behalf of Working Group Upper Limb “CICERONE” Italian Consensus Conference on Robotic Rehabilitation. (2021). Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review. Brain Sciences, 11(12), 1630. https://doi.org/10.3390/brainsci11121630