
Anti-Ma2 Antibody-Associated Paraneoplastic Neurological Syndromes: A Pilot Study


Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Clinical Features and Outcomes
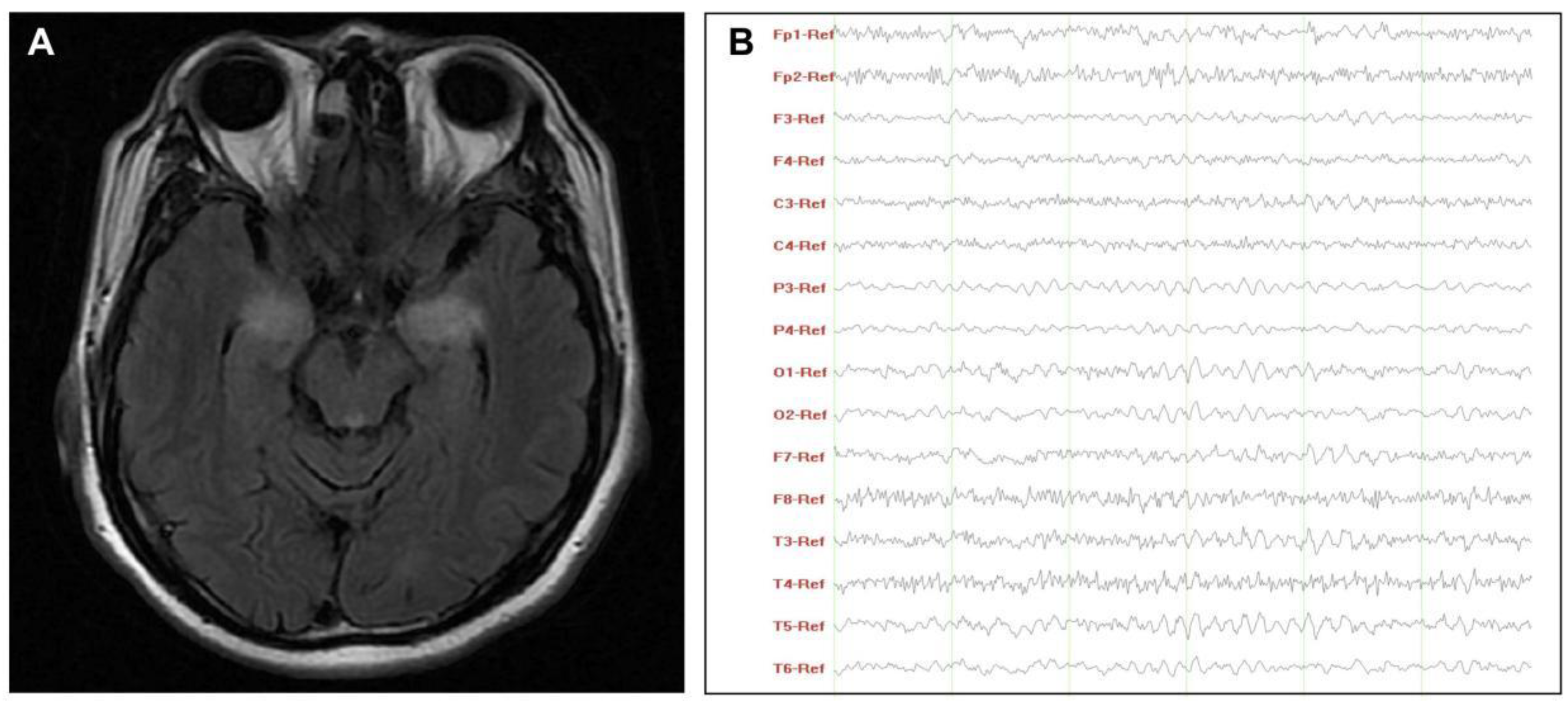
3.2. Paraclinical Findings
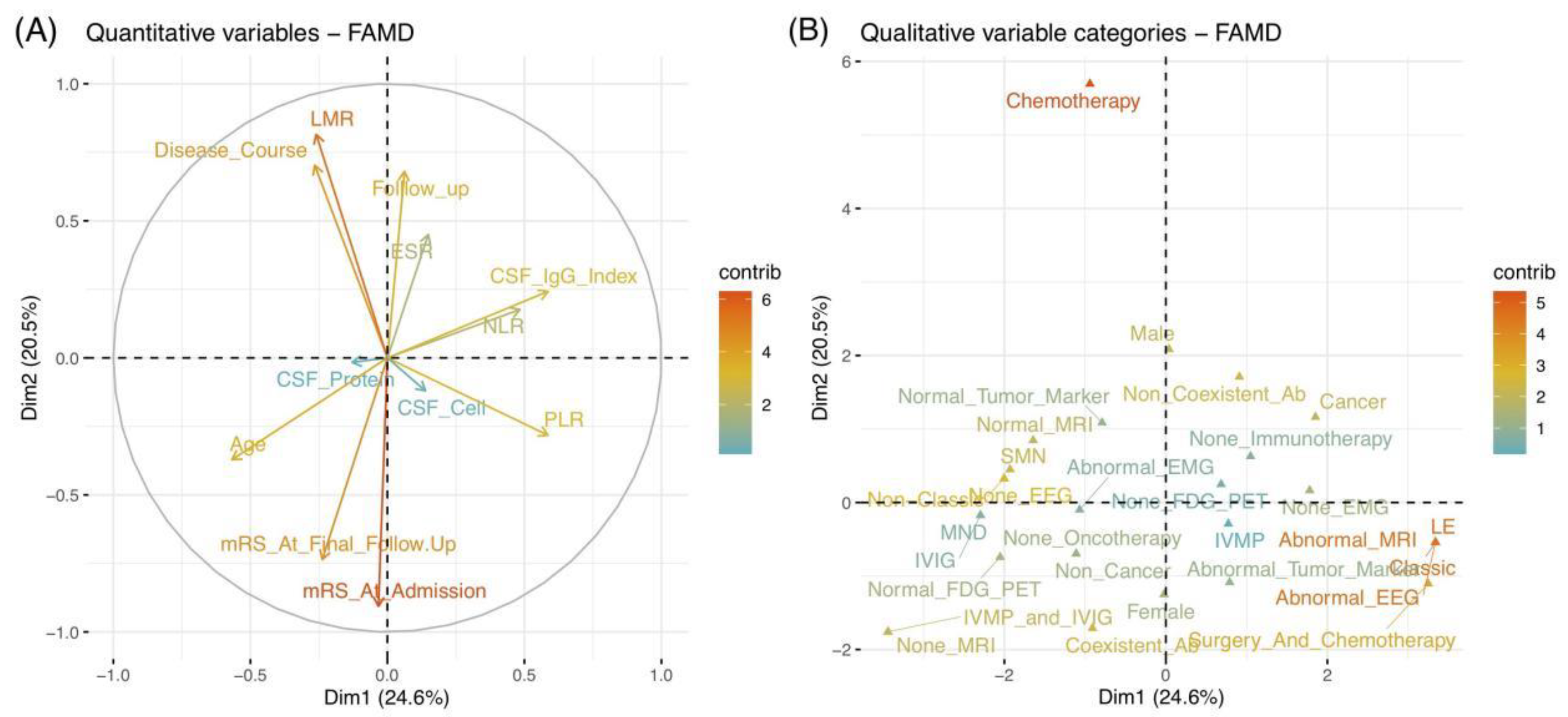
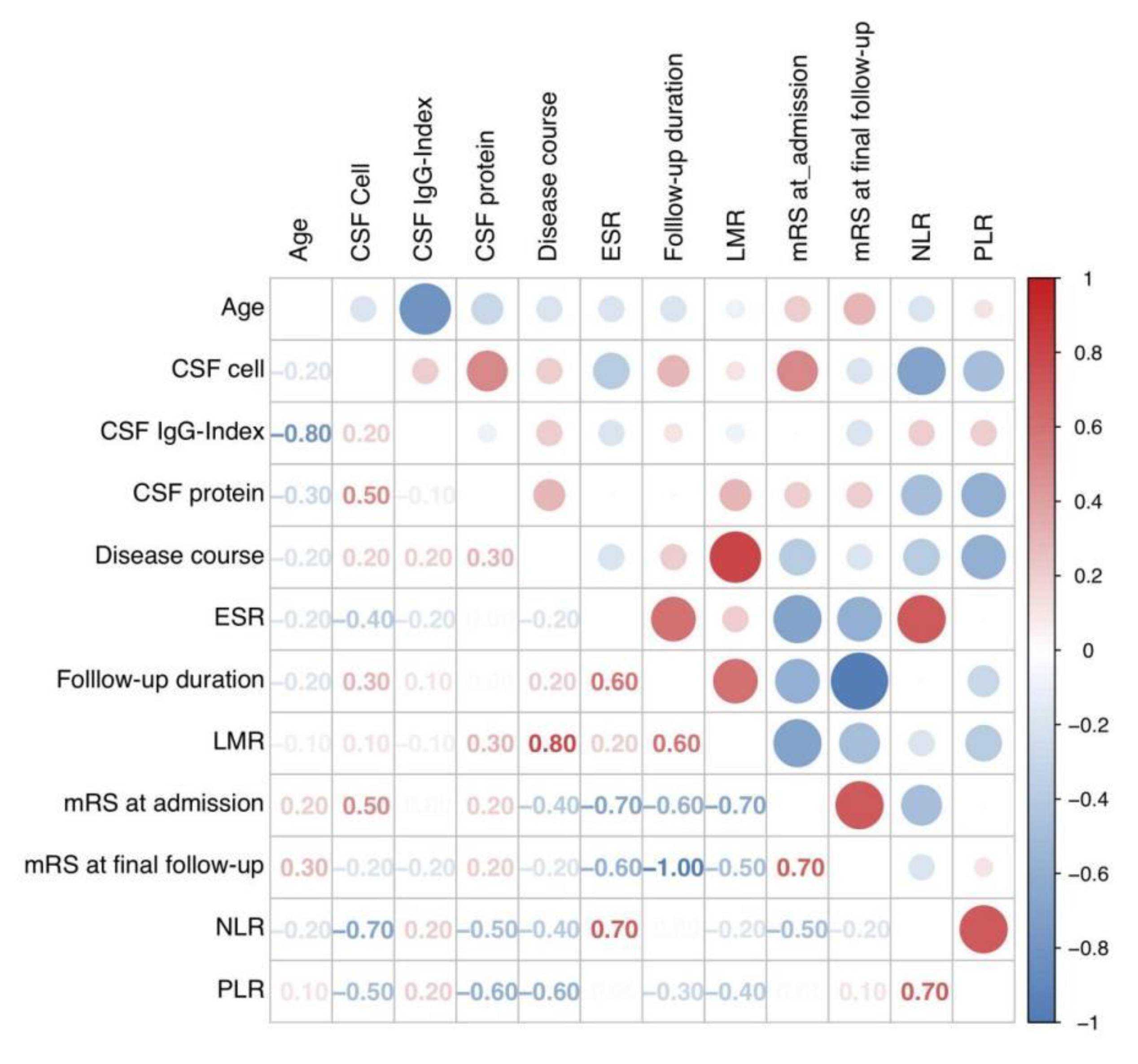
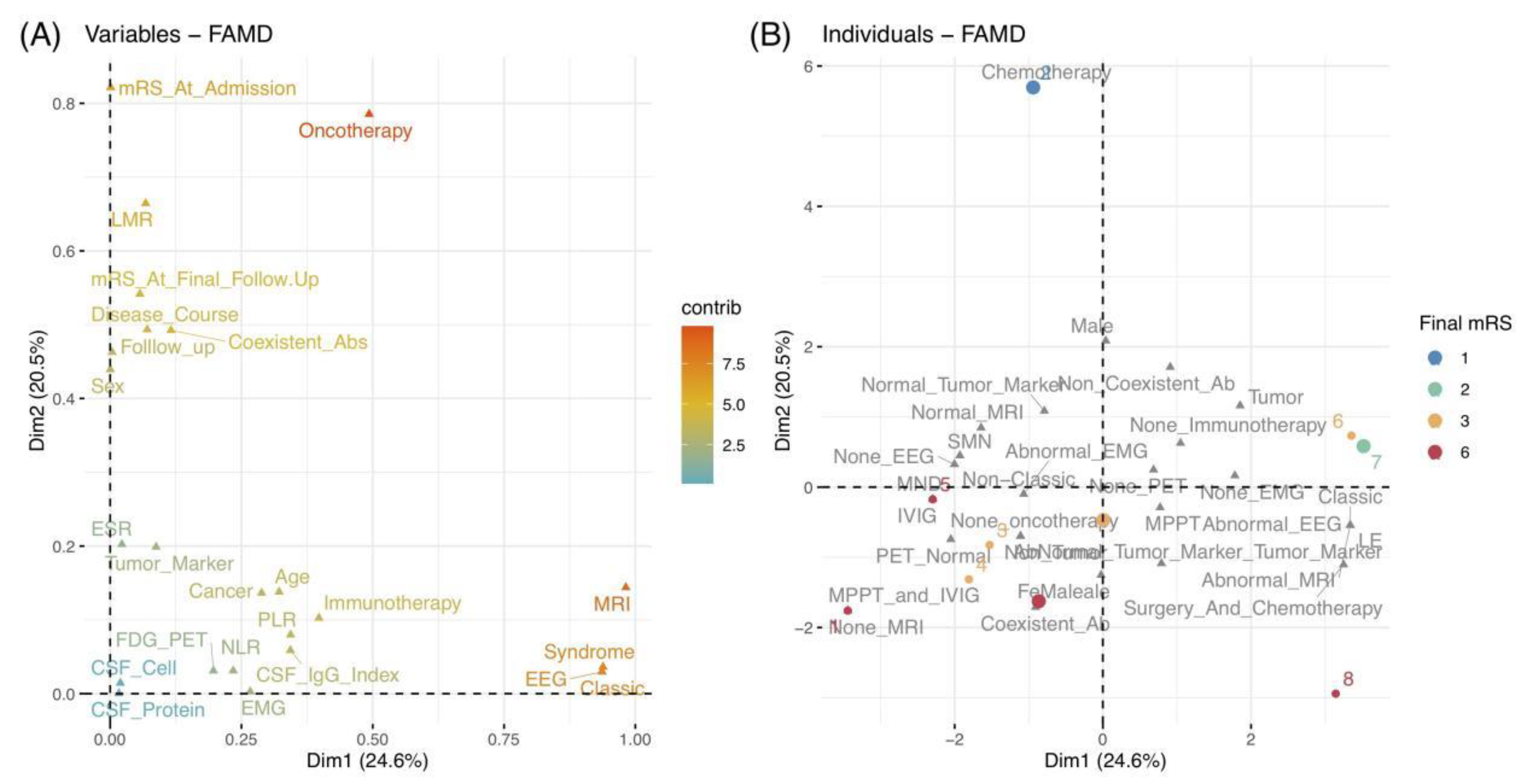
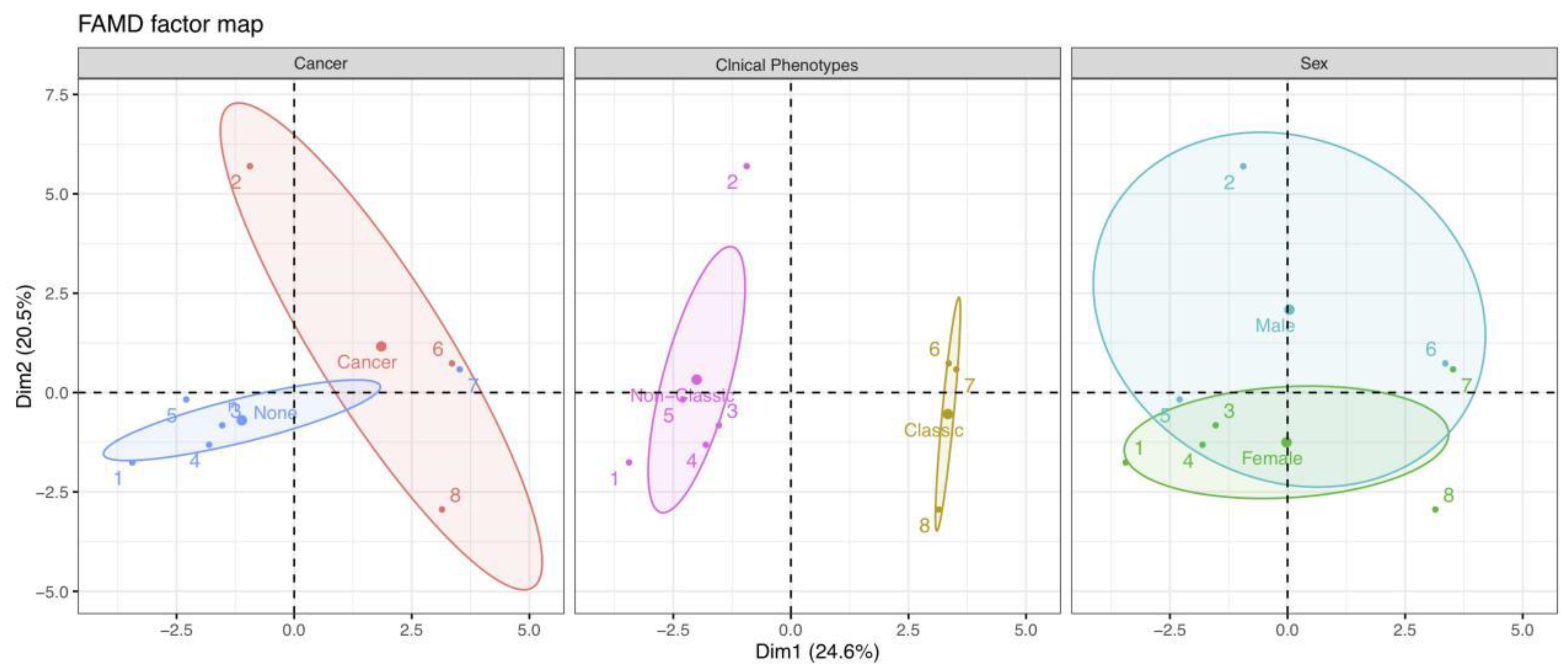
3.3. FAMD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darnell, R.B.; Posner, J.B. Paraneoplastic syndromes involving the nervous system. N. Engl. J. Med. 2003, 349, 1543–1554. [Google Scholar] [CrossRef]
- Honnorat, J.; Antoine, J.C. Paraneoplastic neurological syndromes. Orphanet J. Rare Dis. 2007, 2, 22. [Google Scholar] [CrossRef]
- Graus, F.; Delattre, J.Y.; Antoine, J.C.; Dalmau, J.; Giometto, B.; Grisold, W.; Honnorat, J.; Smitt, P.S.; Vedeler, C.; Verschuuren, J.J.; et al. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, J.; Graus, F.; Villarejo, A.; Posner, J.B.; Blumenthal, D.; Thiessen, B.; Saiz, A.; Meneses, P.; Rosenfeld, M.R. Clinical analysis of anti-Ma2-associated encephalitis. Brain 2004, 127, 1831–1844. [Google Scholar] [CrossRef] [PubMed]
- Ortega Suero, G.; Sola-Valls, N.; Escudero, D.; Saiz, A.; Graus, F. Anti-Ma and anti-Ma2-associated paraneoplastic neurological syndromes. Neurologia (Engl. Ed.) 2018, 33, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Joubert, B.; Maureille, A.; Thomas, L.; Bernard, E.; Streichenberger, N.; Cotton, F.; Ducray, F.; Honnorat, J. Motor neuron involvement in anti-Ma2-associated paraneoplastic neurological syndrome. J. Neurol. 2019, 266, 398–410. [Google Scholar] [CrossRef]
- Pagès, J. Analyse factorielle de donnees mixtes: Principe et exemple d’application. Rev. Stat. Appl. 2004, 52, 93–111. [Google Scholar]
- Pages, J. Factorial Analysis of Mixed Data. In Multiple Factor Analysis by Example Using R, 1st ed.; Chambers, J.M., Hothorn, T., Temple-Lang, D., Wickham, H., Eds.; CRC Press: Boca Raton, FL, USA, 2014; pp. 67–74. [Google Scholar]
- Brigitte, E. Traitement simultané de variables quantitatives et qualitatives en analyse factorielle. Les. Cah. L’anal. Données 1979, 4, 137–146. [Google Scholar]
- Saporta, G. Simultaneous analysis of qualitative and quantitative data. Soc. Ital. Stat. XXXV Riun. Sci. 1990, 1, 63–72. [Google Scholar]
- Jérôme, P. Analyse factorielle de données mixtes. Rev. Stat. Appl. 2002, 52, 93–111. [Google Scholar]
- Kiers, H. Simple Structure in Component Analysis Techniques for Mixtures of Qualitataive and Quantitative Variables. Psychometrika 1991, 56, 197–212. [Google Scholar] [CrossRef]
- Escofier, B.; Pagès, J. Analyses factorielles simples et multiples. Dunod 2008, 318, 27. [Google Scholar]
- Han, L.; Shen, P.; Yan, J.; Huang, Y.; Ba, X.; Lin, W.; Wang, H.; Huang, Y.; Qin, K.; Wang, Y.; et al. Exploring the Clinical Characteristics of COVID-19 Clusters Identified Using Factor Analysis of Mixed Data-Based Cluster Analysis. Front. Med. 2021, 8, 644724. [Google Scholar] [CrossRef] [PubMed]
- Garjito, T.A.; Susanti, L.; Mujiyono, M.; Prihatin, M.T.; Susilo, D.; Nugroho, S.S.; Mujiyanto, M.; Wigati, R.A.; Satoto, T.B.T.; Manguin, S.; et al. Assessment of Mosquito Collection Methods for Dengue Surveillance. Front. Med. 2021, 8, 685926. [Google Scholar] [CrossRef]
- Drobikova, K.; Vallova, S.; Motyka, O.; Mamulova Kutlakova, K.; Placha, D.; Seidlerova, J. Effects of binder choice in converter and blast furnace sludge briquette preparation: Environmental and practical implications. Waste Manag. 2018, 79, 30–37. [Google Scholar] [CrossRef]
- Wahlstrom, V.; Olsson, D.; Ohberg, F.; Olsson, T.; Slunga Jarvholm, L. Underlying Factors Explaining Physical Behaviors among Office Workers-An Exploratory Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9158. [Google Scholar] [CrossRef]
- Lufkin, L.; Budisic, M.; Mondal, S.; Sur, S. A Bayesian Model to Analyze the Association of Rheumatoid Arthritis with Risk Factors and Their Interactions. Front. Public Health 2021, 9, 693830. [Google Scholar] [CrossRef] [PubMed]
- Kongprajug, A.; Denpetkul, T.; Chyerochana, N.; Mongkolsuk, S.; Sirikanchana, K. Human Fecal Pollution Monitoring and Microbial Risk Assessment for Water Reuse Potential in a Coastal Industrial-Residential Mixed-Use Watershed. Front. Microbiol. 2021, 12, 647602. [Google Scholar] [CrossRef] [PubMed]
- Le Marechal, M.; Mailles, A.; Seigneurin, A.; Tattevin, P.; Stahl, J.P.; Epaulard, O. A Prospective Cohort Study to Identify Clinical, Biological, and Imaging Features That Predict the Etiology of Acute Encephalitis. Clin. Infect. Dis. 2021, 73, 264–270. [Google Scholar] [CrossRef]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Lê, S.; Josse, J.; Husson, F. FactoMineR: An R package for multivariate analysis. J. Stat. Softw. 2008, 25, 1–18. [Google Scholar] [CrossRef]
- Josse, J.; Husson, F. missMDA: A package for handling missing values in multivariate data analysis. J. Stat. Softw. 2016, 70, 1–31. [Google Scholar] [CrossRef]
- Friendly, M. Corrgrams: Exploratory displays for correlation matrices. Am. Stat. 2002, 56, 316–324. [Google Scholar] [CrossRef]
- Miller, A.; Green, M.; Robinson, D. Simple rule for calculating normal erythrocyte sedimentation rate. Br. Med. J. (Clin. Res. Ed.) 1983, 286, 266. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Cai, M.T.; Yang, F.; Zhou, J.P.; Fang, W.; Shen, C.H.; Zhang, Y.X.; Ding, M.P. IgG Index Revisited: Diagnostic Utility and Prognostic Value in Multiple Sclerosis. Front. Immunol. 2020, 11, 1799. [Google Scholar] [CrossRef] [PubMed]
- Ayrignac, X.; Castelnovo, G.; Landrault, E.; Fayolle, H.; Pers, Y.M.; Honnorat, J.; Campello, C.; Figarella-Branger, D.; Labauge, P. Ma2 antibody and multiple mononeuropathies. Rev. Neurol. 2008, 164, 608–611. [Google Scholar] [CrossRef]
- Hoffmann, L.A.; Jarius, S.; Pellkofer, H.L.; Schueller, M.; Krumbholz, M.; Koenig, F.; Johannis, W.; la Fougere, C.; Newman, T.; Vincent, A.; et al. Anti-Ma and anti-Ta associated paraneoplastic neurological syndromes: 22 newly diagnosed patients and review of previous cases. J. Neurol. Neurosurg. Psychiatry 2008, 79, 767–773. [Google Scholar] [CrossRef]
- Murphy, S.M.; Khan, U.; Alifrangis, C.; Hazell, S.; Hrouda, D.; Blake, J.; Ball, J.; Gabriel, C.; Markarian, P.; Rees, J.; et al. Anti Ma2-associated myeloradiculopathy: Expanding the phenotype of anti-Ma2 associated paraneoplastic syndromes. J. Neurol. Neurosurg. Psychiatry 2012, 83, 232–233. [Google Scholar] [CrossRef][Green Version]
- Antoine, J.C.; Camdessanche, J.P. Paraneoplastic neuropathies. Curr. Opin. Neurol. 2017, 30, 513–520. [Google Scholar] [CrossRef]
- Pellkofer, H.; Schubart, A.S.; Hoftberger, R.; Schutze, N.; Pagany, M.; Schuller, M.; Lassmann, H.; Hohlfeld, R.; Voltz, R.; Linington, C. Modelling paraneoplastic CNS disease: T-cells specific for the onconeuronal antigen PNMA1 mediate autoimmune encephalomyelitis in the rat. Brain 2004, 127, 1822–1830. [Google Scholar] [CrossRef]
- Kyle, R.A.; Gertz, M.A.; Witzig, T.E.; Lust, J.A.; Lacy, M.Q.; Dispenzieri, A.; Fonseca, R.; Rajkumar, S.V.; Offord, J.R.; Larson, D.R.; et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin. Proc. 2003, 78, 21–33. [Google Scholar] [CrossRef]
- Adams, D.; Lozeron, P.; Lacroix, C. Amyloid neuropathies. Curr. Opin. Neurol. 2012, 25, 564–572. [Google Scholar] [CrossRef]
- Kelly, J.J., Jr.; Kyle, R.A.; O’Brien, P.C.; Dyck, P.J. The natural history of peripheral neuropathy in primary systemic amyloidosis. Ann. Neurol. 1979, 6, 1–7. [Google Scholar] [CrossRef]
- Kyle, R.A.; Bayrd, E.D. Amyloidosis: Review of 236 cases. Medicine 1975, 54, 271–299. [Google Scholar] [CrossRef] [PubMed]
- Muchtar, E.; Dispenzieri, A.; Gertz, M.A.; Kumar, S.K.; Buadi, F.K.; Leung, N.; Lacy, M.Q.; Dingli, D.; Ailawadhi, S.; Bergsagel, P.L.; et al. Treatment of AL Amyloidosis: Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) Consensus Statement 2020 Update. Mayo Clin. Proc. 2021, 96, 1546–1577. [Google Scholar] [CrossRef]
- Duddy, M.E.; Baker, M.R. Stiff person syndrome. Front. Neurol. Neurosci. 2009, 26, 147–165. [Google Scholar] [PubMed]
- Eye, P.G.; Wang, B.; Keung, E.S.; Tagg, N.T. Anti-ZIC4 associated paraneoplastic cerebellar degeneration in a patient with both diffuse large B-cell lymphoma and incidental smoldering multiple myeloma. J. Neurol. Sci. 2018, 384, 36–37. [Google Scholar] [CrossRef]
- Erre, G.L.; Paliogiannis, P.; Castagna, F.; Mangoni, A.A.; Carru, C.; Passiu, G.; Zinellu, A. Meta-analysis of neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in rheumatoid arthritis. Eur. J. Clin. Investig. 2019, 49, e13037. [Google Scholar] [CrossRef] [PubMed]
- Mandaliya, H.; Jones, M.; Oldmeadow, C.; Nordman, I.I. Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): Neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI). Transl. Lung Cancer Res. 2019, 8, 886–894. [Google Scholar] [CrossRef]
- Sacdalan, D.B.; Lucero, J.A.; Sacdalan, D.L. Prognostic utility of baseline neutrophil-to-lymphocyte ratio in patients receiving immune checkpoint inhibitors: A review and meta-analysis. Onco. Targets Ther. 2018, 11, 955–965. [Google Scholar] [CrossRef]
- Velasco, A.; Rodriguez-Revuelta, J.; Olie, E.; Abad, I.; Fernandez-Pelaez, A.; Cazals, A.; Guillaume, S.; de la Fuente-Tomas, L.; Jimenez-Trevino, L.; Gutierrez, L.; et al. Neutrophil-to-lymphocyte ratio: A potential new peripheral biomarker of suicidal behavior. Eur. Psychiatry 2020, 63, e14. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Vogrig, A.; Muñiz-Castrillo, S.; Antoine, J.G.; Desestret, V.; Dubey, D.; Giometto, B.; Irani, S.R.; Joubert, B.; Leypoldt, F.; et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e1014. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Sex | Age at Onset, y | Clinical Symptoms | Syndromes | Associated Cancer/Diagnostic Time | Oncotherapy | Immunotherapy | Follow-Up Duration, m | mRs Score on Admission/at Final Follow-Up |
|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 59 | Limb numbness and weakness | Chronic SMN | - | - | IVMP + IVIG | 20.0 | 4/6 |
| 2 | M | 53 | Limb numbness and pain | Chronic SMN | Multiple myeloma (IIIb)/16 m after onset | Chemotherapy | None | 57.5 | 1/1 |
| 3 | F | 69 | Limb numbness and weakness | Chronic SMN | - | - | None | 41.1 | 4/3 |
| 4 | F | 68 | Limb numbness and weakness | Subacute SMN | - | - | IVMP | 44.5 | 4/3 |
| 5 | M | 47 | Muscle weakness and atrophy | MND | - | - | IVIG | 7.0 | 4/6 |
| 6 | M | 34 | Drowsy, memory loss, hallucinations | LE | Mixed germ cell tumors */2 m after onset | Surgery + chemotherapy | IVMP | 42.8 | 4/3 |
| 7 | F | 29 | Psychiatric symptoms | LE | - | - | None | 46.8 | 3/2 |
| 8 | F | 64 | Memory loss | LE | Thymoma (IIIb) */2 y before onset | Surgery + chemotherapy | None | 0.0 | 4/6 |
| No | Tumor Marker | Coexistent Antibodies | ESR, mm/h | NLR | PLR | LMR | CSF | MRI | FDG-PET | EEG | EMG | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cells/mL | Protein, mg/dL | IgG Index | |||||||||||
| 1 | Normal | Anti-ATG, anti-TPO, anti-TG | 21.0 | 1.5 | 84.9 | 3.9 | 3 | 103 | 0.11 | - | - | - | Demyelinating |
| 2 | Normal | Monoclonal protein, IgG, Kappa light | 30.0 ^ | 2.6 | 125.0 | 6.8 | 0 | 43.3 | 0.48 | Normal | - | - | Demyelinating |
| 3 | CA125 | Anti-β2GPI | 19.0 | 1.4 | 93.0 | 2.9 | 6 | 43.5 | 0.31 | Normal | - | - | - |
| 4 * | β-hCG | Anti-ATG | 14.0 | 1.8 | 163.1 | 3.8 | 4 | 31.5 | 0.43 | Normal | Normal | - | Demyelinating and axonal |
| 5 | Normal | Normal | 4.0 | 1.6 | 120.7 | 3.3 | - | - | - | Normal | Normal | - | Denervation of multiple muscles in cervical, thoracic, and lumbosacral regions |
| 6 * | AFP, PSA | Normal | 9.0 | 1.1 | 115.1 | 4.8 | 10 | 87.8 | 0.90 | BMTL | - | Slow wave | - |
| 7 | Normal | Normal | 33.0 ^ | 3.3 | 160.4 | 2.3 | 2 | 47.6 | - | BMTL | - | Slow wave | - |
| 8 | CEA, CA211, SCC * | Anti-ATG, anti-TPO | 15.0 | 2.9 | 225.8 | 2.1 | 0 | 27.5 | - | BMTL | - | Slow wave | Decremental response on slow RNS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Cai, M.-T.; Lai, Q.-L.; Zheng, Y.; Shen, C.-H.; Zhang, Y.-X. Anti-Ma2 Antibody-Associated Paraneoplastic Neurological Syndromes: A Pilot Study. Brain Sci. 2021, 11, 1577. https://doi.org/10.3390/brainsci11121577
Guo Y, Cai M-T, Lai Q-L, Zheng Y, Shen C-H, Zhang Y-X. Anti-Ma2 Antibody-Associated Paraneoplastic Neurological Syndromes: A Pilot Study. Brain Sciences. 2021; 11(12):1577. https://doi.org/10.3390/brainsci11121577
Chicago/Turabian StyleGuo, Yi, Meng-Ting Cai, Qi-Lun Lai, Yang Zheng, Chun-Hong Shen, and Yin-Xi Zhang. 2021. "Anti-Ma2 Antibody-Associated Paraneoplastic Neurological Syndromes: A Pilot Study" Brain Sciences 11, no. 12: 1577. https://doi.org/10.3390/brainsci11121577
APA StyleGuo, Y., Cai, M.-T., Lai, Q.-L., Zheng, Y., Shen, C.-H., & Zhang, Y.-X. (2021). Anti-Ma2 Antibody-Associated Paraneoplastic Neurological Syndromes: A Pilot Study. Brain Sciences, 11(12), 1577. https://doi.org/10.3390/brainsci11121577