
Effects of Exercise Training on Neurotrophic Factors and Subsequent Neuroprotection in Persons with Multiple Sclerosis—A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract

1. Introduction
2. Methods
2.1. Literature Search
2.2. Selection Criteria
2.3. Screening Process
2.4. Quality Assessment
2.5. Data Extraction
2.6. Meta-Analysis
3. Results
3.1. Screening Process and Study Selection
3.2. Study Quality
3.3. Participants
3.4. Exercise Interventions
3.5. Physiological and Functional Outcome Measures
3.6. Acute Effects of Exercise on Neurotrophic Factors
3.7. Chronic Effects on Neurotrophic Factors
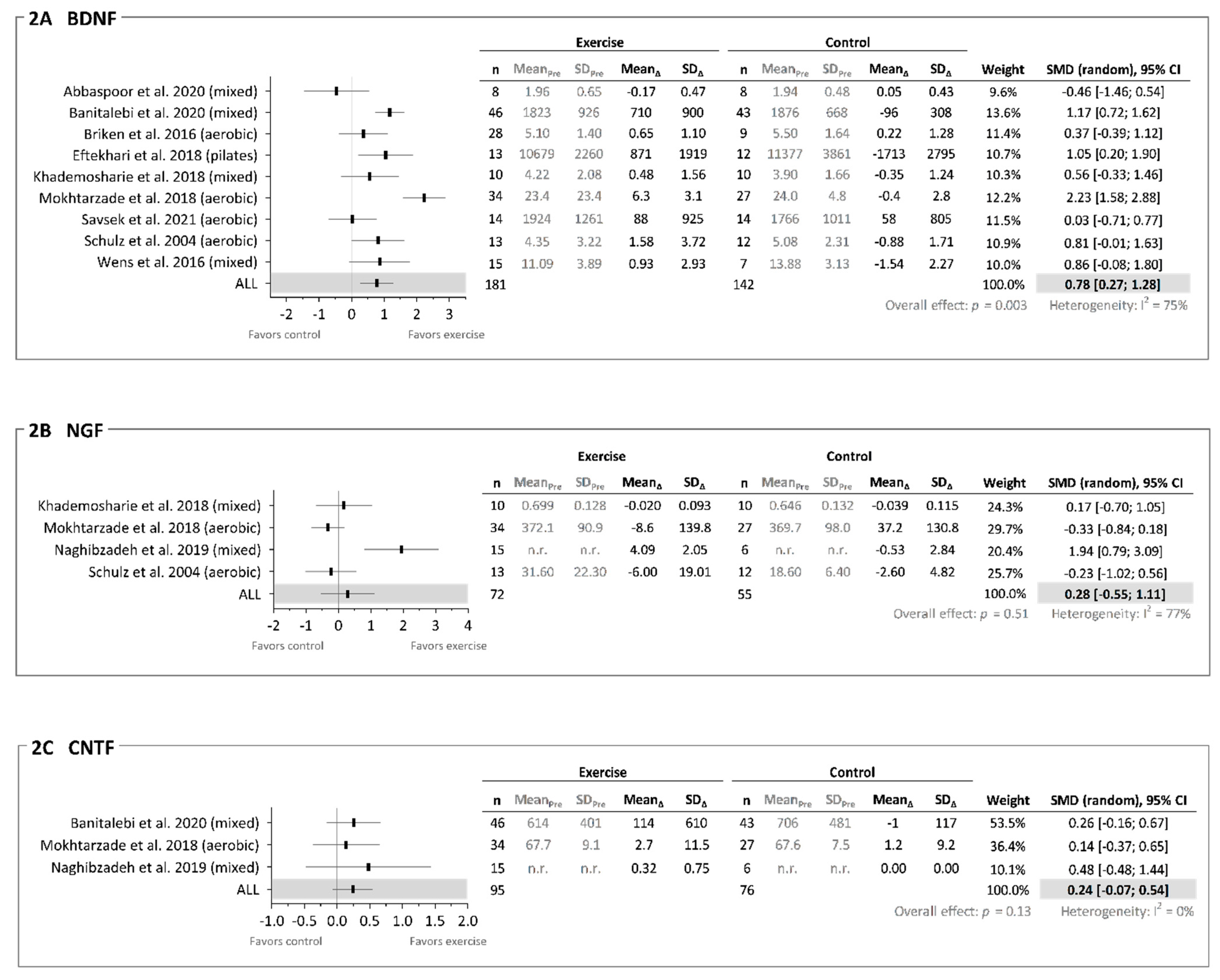
3.7.1. Brain-Derived Neurotrophic Factor (BDNF)
3.7.2. Nerve Growth Factor (NGF)
3.7.3. Ciliary Neurotrophic Factor (CNTF)
3.7.4. Insulin-Like Growth Factor-1 (IGF-1)
3.7.5. Neurotrophin 3 (NT3), 4 (NT4), and 4/5 (NT 4/5)
3.7.6. Glial Cell-Derived Neurotrophic Factor (GDNF)
3.7.7. Platelet-Derived Growth Factor (PDGF)
3.7.8. Vascular Endothelial Growth Factor (VEGF)
3.8. Neuroprotective Effects of Exercise
4. Discussion
4.1. Acute and Chronic Neurotrophic Response to Exercise
4.2. Exercise Modality
4.3. Translation between Neurotrophic Factors and Neuroprotection
4.4. Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2008, 372, 1502–1517. [Google Scholar] [CrossRef]
- Chaudhuri, A. Multiple sclerosis is primarily a neurodegenerative disease. J. Neural Transm. 2013, 120, 1463–1466. [Google Scholar] [CrossRef] [PubMed]
- Lassmann, H. Pathology and disease mechanisms in different stages of multiple sclerosis. J. Neurol. Sci. 2013, 333, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, T.; Signorovitch, J.; Huynh, L.; Galebach, P.; Kelley, C.; DiBernardo, A.; Sasane, R. The natural history of brain volume loss among patients with multiple sclerosis: A systematic literature review and meta-analysis. J. Neurol. Sci. 2015, 357, 8–18. [Google Scholar] [CrossRef]
- White, J.L.; Castellano, V. Exercise and brain health—Implications for multiple sclerosis part 1—Neuronal growth factors. Sports Med. 2008, 38, 91–100. [Google Scholar] [CrossRef]
- Schulz, K.-H.; Gold, S.; Witte, J.; Bartsch, K.; Lang, U.E.; Hellweg, R.; Reer, R.; Braumann, K.-M.; Heesen, C. Impact of aerobic training on immune-endocrine parameters, neurotrophic factors, quality of life and coordinative function in multiple sclerosis. J. Neurol. Sci. 2004, 225, 11–18. [Google Scholar] [CrossRef]
- Pearson, M.; Dieberg, G.; Smart, N. Exercise as a Therapy for Improvement of Walking Ability in Adults with Multiple Sclerosis: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 1339–1348.e7. [Google Scholar] [CrossRef]
- Dalgas, U.; Langeskov-Christensen, M.; Stenager, E.; Riemenschneider, M.; Hvid, L.G. Exercise as Medicine in Multiple Sclerosis-Time for a Paradigm Shift: Preventive, Symptomatic, and Disease-Modifying Aspects and Perspectives. Curr. Neurol. Neurosci. Rep. 2019, 19, 88. [Google Scholar] [CrossRef] [PubMed]
- Casson, R.J.; Chidlow, G.; Ebneter, A.; Wood, J.P.; Crowston, J.; Goldberg, I. Translational neuroprotection research in glaucoma: A review of definitions and principles. Clin. Exp. Ophthalmol. 2011, 40, 350–357. [Google Scholar] [CrossRef]
- Kjølhede, T.; Siemonsen, S.; Wenzel, D.; Stellmann, J.-P.; Ringgaard, S.; Pedersen, B.G.; Stenager, E.; Petersen, T.; Vissing, K.; Heesen, C.; et al. Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult. Scler. J. 2017, 24, 1356–1365. [Google Scholar] [CrossRef]
- Chaves, A.R.; Devasahayam, A.J.; Riemenschneider, M.; Pretty, R.W.; Ploughman, M. Walking Training Enhances Corticospinal Excitability in Progressive Multiple Sclerosis—A Pilot Study. Front. Neurol. 2020, 11, 422. [Google Scholar] [CrossRef]
- Stellmann, J.-P.; Maarouf, A.; Schulz, K.-H.; Baquet, L.; Pöttgen, J.; Patra, S.; Penner, I.-K.; Gellißen, S.; Ketels, G.; Besson, P.; et al. Aerobic Exercise Induces Functional and Structural Reorganization of CNS Networks in Multiple Sclerosis: A Randomized Controlled Trial. Front. Hum. Neurosci. 2020, 14, 255. [Google Scholar] [CrossRef]
- Savšek, L.; Stergar, T.; Strojnik, V.; Ihan, A.; Koren, A.; Jazbec, S. Impact of aerobic exercise on clinical and magnetic resonance imaging biomarkers in persons with multiple sclerosis: An exploratory randomized controlled trial. J. Rehabil. Med. 2021, 53, jrm00178. [Google Scholar] [CrossRef]
- Langeskov-Christensen, M.; Hvid, L.G.; Eskildsen, S.F.; Nygaard, M.K.E.; Ringgaard, S.; Jensen, H.B.; Nielsen, H.H.; Petersen, T.; Stenager, E.; Dalgas, U. Efficacy of high-intensity aerobic exercise on brain MRI measures in multiple sclerosis. Neu-Rology 2021, 96, e203–e213. [Google Scholar] [CrossRef]
- Hvid, L.G.; Harwood, D.L.; Eskildsen, S.F.; Dalgas, U. A Critical Systematic Review of Current Evidence on the Effects of Physical Exercise on Whole/Regional Grey Matter Brain Volume in Populations at Risk of Neurodegeneration. Sports Med. 2021, 51, 1651–1671. [Google Scholar] [CrossRef] [PubMed]
- Gentile, A.; Musella, A.; De Vito, F.; Rizzo, F.R.; Fresegna, D.; Bullitta, S.; Vanni, V.; Guadalupi, L.; Bassi, M.A.U.S.; Buttari, F.; et al. Immunomodulatory Effects of Exercise in Experimental Multiple Sclerosis. Front. Immunol. 2019, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.Y.; Lozinski, B.; Yong, V.W. Exercise in multiple sclerosis and its models: Focus on the central nervous system outcomes. J. Neurosci. Res. 2020, 98, 509–523. [Google Scholar] [CrossRef] [PubMed]
- Luo, L. Principles of Neurobiology; Garland Science: New York, NY, USA, 2015. [Google Scholar]
- Souza, P.S.; Gonçalves, E.D.; Pedroso, G.S.; Farias, H.R.; Junqueira, S.C.; Marcon, R.; Dutra, R.C. Physical Exercise Attenuates Experimental Autoimmune Encephalomyelitis by Inhibiting Peripheral Immune Response and Blood-Brain Barrier Disruption. Mol. Neurobiol. 2017, 54, 4723–4737. [Google Scholar] [CrossRef]
- Bonfiglio, T.; Olivero, G.; Vergassola, M.; Mannelli, L.D.C.; Pacini, A.; Iannuzzi, F.; Summa, M.; Bertorelli, R.; Feligioni, M.; Ghelardini, C.; et al. Environmental training is beneficial to clinical symptoms and cortical presynaptic defects in mice suffering from experimental autoimmune encephalomyelitis. Neuropharmacology 2019, 145, 75–86. [Google Scholar] [CrossRef]
- Xie, Y.; Li, Z.; Wang, Y.; Xue, X.; Ma, W.; Zhang, Y.; Wang, J. Effects of moderate- versus high- intensity swimming training on inflammatory and CD4+ T cell subset profiles in experimental autoimmune encephalomyelitis mice. J. Neuroimmunol. 2019, 328, 60–67. [Google Scholar] [CrossRef]
- Mandolesi, G.; Bullitta, S.; Fresegna, D.; De Vito, F.; Rizzo, F.R.; Musella, A.; Guadalupi, L.; Vanni, V.; Bassi, M.S.; Buttari, F.; et al. Voluntary running wheel attenuates motor deterioration and brain damage in cuprizone-induced demyelination. Neurobiol. Dis. 2019, 129, 102–117. [Google Scholar] [CrossRef]
- Lu, Y.; Christian, K.; Lu, B. BDNF: A key regulator for protein synthesis-dependent LTP and long-term memory? Neurobiol. Learn. Mem. 2008, 89, 312–323. [Google Scholar] [CrossRef]
- Begliuomini, S.; Lenzi, E.; Ninni, F.; Casarosa, E.; Merlini, S.; Pluchino, N.; Valentino, V.; Luisi, S.; Luisi, M.; Genazzani, A.R. Plasma brain-derived neurotrophic factor daily variations in men: Correlation with cortisol circadian rhythm. J. Endocrinol. 2008, 197, 429–435. [Google Scholar] [CrossRef]
- Thoenen, H. Neurotrophins and Neuronal Plasticity. Science 1995, 270, 593–598. [Google Scholar] [CrossRef]
- Sakuma, K.; Yamaguchi, A. The recent understanding of the neurotrophin’s role in skeletal muscle adaptation. J. Biomed Bio. 2011, 2011, 201696. [Google Scholar] [CrossRef]
- Pedersen, B.K. Physical activity and muscle–brain crosstalk. Nat. Rev. Endocrinol. 2019, 15, 383–392. [Google Scholar] [CrossRef]
- Wrann, C.D.; White, J.P.; Salogiannnis, J.; Laznik-Bogoslavski, D.; Wu, J.; Ma, D.; Lin, J.D.; Greenberg, M.E.; Spiegelman, B.M. Exercise Induces Hippocampal BDNF through a PGC-1α/FNDC5 Pathway. Cell Metab. 2013, 18, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Negaresh, R.; Motl, R.W.; Zimmer, P.; Mokhtarzade, M.; Baker, J.S. Effects of exercise training on multiple sclerosis biomarkers of central nervous system and disease status: A systematic review of intervention studies. Eur. J. Neurol. 2019, 26, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Poser, C.M.; Paty, D.W.; Scheinberg, L.; McDonald, W.I.; Davis, F.A.; Ebers, G.C.; Johnson, K.P.; Sibley, W.A.; Silberberg, D.H.; Tourtellotte, W.W. New diagnostic criteria for multiple sclerosis: Guidelines for research protocols. Ann Neurol. 1983, 13, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; E Powell, K.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int. J. Evid. Based Healthc. 2015, 13, 9–18. [Google Scholar] [CrossRef]
- Rohatgi, A. Web Plot Digitizer (Version 3.9) [Online Computer Software]. 2015. Available online: https://apps.automeris.io/wpd/. (accessed on 19 October 2021).
- Higgins, T.D.J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. In Wiley Cochrane Series; John Wiley & Sons: Chichester, UK, 2008. [Google Scholar]
- Kinney, A.R.; Eakman, A.M.; Graham, J.E. Novel Effect Size Interpretation Guidelines and an Evaluation of Statistical Power in Rehabilitation Research. Arch. Phys. Med. Rehabil. 2020, 101, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Abbaspoor, E.; Zolfaghari, M.; Ahmadi, B.; Khodaei, K. The effect of combined functional training on BDNF, IGF-1, and their association with health-related fitness in the multiple sclerosis women. Growth Horm. IGF Res. 2020, 52, 101320. [Google Scholar] [CrossRef] [PubMed]
- Banitalebi, E.; Ghahfarrokhi, M.M.; Negaresh, R.; Kazemi, A.; Faramarzi, M.; Motl, R.W.; Zimmer, P. Exercise improves neurotrophins in multiple sclerosis independent of disability status. Mult. Scler. Relat. Disord. 2020, 43, 102143. [Google Scholar] [CrossRef] [PubMed]
- Briken, S.; Rosenkranz, S.C.; Keminer, O.; Patra, S.; Ketels, G.; Heesen, C.; Hellweg, R.; Pless, O.; Schulz, K.-H.; Gold, S. Effects of exercise on Irisin, BDNF and IL-6 serum levels in patients with progressive multiple sclerosis. J. Neuroimmunol. 2016, 299, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, E.; Etemadifar, M. Interleukin-10 and brain-derived neurotrophic factor responses to the Mat Pilates training in women with multiple sclerosis. Sci. Med. 2018, 28, ID31668. [Google Scholar] [CrossRef]
- Khademosharie, M.; Tadibi, V.; Reza Hamedinia, M. The effect of 12-weeks resistance and endurance training on the serum levels NGF, BDNF, and VDBP in women with multiple sclerosis. Int. J. Appl. Exerc. Physiol. 2018, 7, 76–86. [Google Scholar] [CrossRef]
- Naghibzadeh, A.; Mohammadi, G.; Darlington, P.J.; Rezaei Namjoo, F.; Rashidlamir, A. Aquatic exercise with Swedish massage increases neurotrophic factors and decreases interleukin-6 (IL-6) in relapsing remitting multiple sclerosis. Bio Exerc. 2019, 15, 171–186. [Google Scholar]
- Ozkul, C.; Guclu-Gunduz, A.; Irkec, C.; Fidan, I.; Aydin, Y.; Ozkan, T.; Yazici, G. Effect of combined exercise training on serum brain-derived neurotrophic factor, suppressors of cytokine signaling 1 and 3 in patients with multiple sclerosis. J. Neuroimmunol. 2018, 316, 121–129. [Google Scholar] [CrossRef]
- Wens, I.; Keytsman, C.; Deckx, N.; Cools, N.; Dalgas, U.; Eijnde, B.O. Brain derived neurotrophic factor in multiple sclerosis: Effect of 24 weeks endurance and resistance training. Eur. J. Neurol. 2016, 23, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Askari, A.; Rashid Lamir, A.; Bijeh, N.; Momeni Moghadam, M. Effect of 8-Week Aquatic Training and Resistance Training on Plasma NT-4 Levels and NT-4 Expression in Peripheral Blood Mononuclear Cells in Women with Multiple Sclerosis. Med. Lab. J. 2017, 11, 1–6. [Google Scholar] [CrossRef][Green Version]
- Jørgensen, M.; Kjølhede, T.; Dalgas, U.; Hvid, L. Plasma brain-derived neurotrophic factor (BDNF) and sphingosine-1-phosphat (S1P) are NOT the main mediators of neuroprotection induced by resistance training in persons with multiple sclerosis—A randomized controlled trial. Mult. Scler. Relat. Disord. 2019, 31, 106–111. [Google Scholar] [CrossRef]
- Mokhtarzade, M.; Motl, R.; Negaresh, R.; Zimmer, P.; Khodadoost, M.; Baker, J.S.; Patel, D.; Majdinasab, N.; Ranjbar, R. Exercise-induced changes in neurotrophic factors and markers of blood-brain barrier permeability are moderated by weight status in multiple sclerosis. Neuropeptides 2018, 70, 93–100. [Google Scholar] [CrossRef]
- Rezaee, S.; Kahrizi, S.; Nabavi, S.M.; Hedayati, M. VEGF and TNF-α Responses to Acute and Chronic Aerobic Exercise in the Patients with Multiple Sclerosis. Asian J. Sports Med. 2020, 11, 98312. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Lanctôt, K.L. The effect of acute exercise on blood concentrations of brain-derived neurotrophic factor in healthy adults: A meta-analysis. Eur. J. Neurosci. 2017, 46, 1635–1646. [Google Scholar] [CrossRef]
- Szuhany, K.L.; Bugatti, M.; Otto, M.W. A meta-analytic review of the effects of exercise on brain-derived neurotrophic factor. J. Psychiatr. Res. 2015, 60, 56–64. [Google Scholar] [CrossRef]
- Ferris, L.T.; Williams, J.S.; Shen, C.-L. The Effect of Acute Exercise on Serum Brain-Derived Neurotrophic Factor Levels and Cognitive Function. Med. Sci. Sports Exerc. 2007, 39, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Mattiuzzi, C.; Sanchis-Gomar, F. Updated overview on interplay between physical exercise, neurotrophins, and cognitive function in humans. J. Sport Heal. Sci. 2020, 9, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Liu, C.S.; Sherman, C.; Chan, S.; Lanctôt, K.L. The Effect of Exercise Training on Resting Concentrations of Peripheral Brain-Derived Neurotrophic Factor (BDNF): A Meta-Analysis. PLoS ONE 2016, 11, e0163037. [Google Scholar]
- Schmolesky, M.; Webb, D.L.; Hansen, R.A. The Effects of Aerobic Exercise Intensity and Duration on Levels of Brain-Derived Neurotrophic Factor in Healthy Men. J. Sports Sci. Med. 2013, 12, 502–511. [Google Scholar]
- Reycraft, J.T.; Islam, H.; Townsend, L.K.; Hayward, G.C.; Hazell, T.J.; Macpherson, R.E.K. Exercise Intensity and Recovery on Circulating Brain-derived Neurotrophic Factor. Med. Sci. Sports Exerc. 2020, 52, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Church, D.D.; Hoffman, J.R.; Mangine, G.T.; Jajtner, A.R.; Townsend, J.; Beyer, K.S.; Wang, R.; La Monica, M.B.; Fukuda, D.; Stout, J.R. Comparison of high-intensity vs. high-volume resistance training on the BDNF response to exercise. J. Appl. Physiol. 2016, 121, 123–128. [Google Scholar] [CrossRef]
- El-Sayes, J.; Harasym, D.; Turco, C.V.; Locke, M.B.; Nelson, A.J. Exercise-Induced Neuroplasticity: A Mechanistic Model and Prospects for Promoting Plasticity. Neuroscientist 2018, 25, 65–85. [Google Scholar] [CrossRef] [PubMed]
- Taul-Madsen, L.; Connolly, L.; Dennett, R.; Freeman, J.; Dalgas, U.; Hvid, L.G. Is Aerobic or Resistance Training the Most Effective Exercise Modality for Improving Lower Extremity Physical Function and Perceived Fatigue in People With Multiple Sclerosis? A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2021, 102, 2032–2048, in press. [Google Scholar] [CrossRef]
- Zimmer, P.; Bloch, W.; Schenk, A.; Oberste, M.; Riedel, S.; Kool, J.; Langdon, D.; Dalgas, U.; Kesselring, J.; Bansi, J. High-intensity interval exercise improves cognitive performance and reduces matrix metalloproteinases-2 serum levels in persons with multiple sclerosis: A randomized controlled trial. Mult. Scler. J. 2017, 24, 1635–1644. [Google Scholar] [CrossRef]
- Prosperini, L.; Di Filippo, M. Beyond clinical changes: Rehabilitation-induced neuroplasticity in MS. Mult. Scler. J. 2019, 25, 1348–1362. [Google Scholar] [CrossRef] [PubMed]
- Preziosa, P.; Rocca, M.A.; Filippi, M. Current state-of-art of the application of serum neurofilaments in multiple sclerosis diagnosis and monitoring Expert. Rev. Neurother. 2020, 20, 747–769. [Google Scholar] [CrossRef]
- Högel, H.; Rissanen, E.; Barro, C.; Matilainen, M.; Nylund, M.; Kuhle, J.; Airas, L. Serum glial fibrillary acidic protein correlates with multiple sclerosis disease severity. Mult. Scler. 2020, 26, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Joisten, N.; Rademacher, A.; Warnke, C.; Proschinger, S.; Schenk, A.; Walzik, D.; Knoop, A.; Thevis, M.; Steffen, F.; Bittner, S.; et al. Exercise Diminishes Plasma Neurofilament Light Chain and Reroutes the Kynurenine Pathway in Multiple Sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2021, 29, e982. [Google Scholar] [CrossRef] [PubMed]
- Ercan, Z.; Bilek, F.; Demir, C.F. The effect of aerobic exercise on Neurofilament light chain and glial Fibrillary acidic protein level in patients with relapsing remitting type multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 55, 103219. [Google Scholar] [CrossRef] [PubMed]
- Gejl, A.K.; Enevold, C.; Bugge, A.; Andersen, M.S.; Nielsen, C.H.; Andersen, L.B. Associations between serum and plasma brain-derived neurotrophic factor and influence of storage time and centrifugation strategy. Sci. Rep. 2019, 9, 9655. [Google Scholar] [CrossRef]
- Polacchini, A.; Metelli, G.; Francavilla, R.; Baj, G.; Florean, M.; Mascaretti, L.G.; Tongiorgi, E. A method for reproducible measurements of serum BDNF: Comparison of the performance of six commercial assays. Sci. Rep. 2015, 5, 17989. [Google Scholar] [CrossRef] [PubMed]
- Vrijen, C.; Schenk, H.M.; Hartman, C.A.; Oldehinkel, A.J. Measuring BDNF in saliva using commercial ELISA: Results from a small pilot study. Psychiatry Res. 2017, 254, 340–346. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Study | Study Quality | Sub-Total | Study Reporting | Sub-Total | Total | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||||
| Abbaspoor et al., 2020 (mixed) | 1 | 0 | 0 | 1 | 1 | 3 | 0 | 0 | 2 | 1 | 0 | 1 | 1 | 5 | 8 |
| Askari et al., 2017 (aerobic + resistance) | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 2 | 1 | 0 | 1 | 1 | 5 | 6 |
| Banitalebi et al., 2020 (mixed) | 1 | 0 | 1 | 0 | 1 | 3 | 2 | 0 | 2 | 1 | 0 | 1 | 1 | 7 | 10 |
| Briken et al., 2016 (aerobic) | 1 | 1 | 1 | 0 | 0 | 3 | 2 | 0 | 1 | 1 | 0 | 1 | 1 | 6 | 9 |
| Eftekhari et al., 2018 (Pilates) | 1 | 1 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 4 | 6 |
| Joergensen et al., 2019 (resistance) | 1 | 0 | 1 | 1 | 0 | 3 | 3 | 0 | 2 | 1 | 0 | 1 | 1 | 8 | 11 |
| Khademosharie et al., 2018 (mixed) | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 2 | 1 | 0 | 1 | 1 | 5 | 6 |
| Mokhtarzade et al., 2018 (aerobic) | 1 | 0 | 1 | 0 | 1 | 3 | 2 | 0 | 2 | 1 | 0 | 1 | 1 | 7 | 10 |
| Naghibzadeh et al., 2019 (mixed) | 1 | 0 | 0 | 0 | 1 | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 3 |
| Ozkul et al., 2018 (mixed) | 1 | 1 | 1 | 1 | 1 | 5 | 3 | 0 | 1 | 1 | 0 | 1 | 1 | 7 | 12 |
| Rezaee et al., 2020 (aerobic) | 1 | 0 | 0 | 1 | 0 | 2 | 1 | 0 | 2 | 1 | 0 | 0 | 1 | 5 | 7 |
| Savsek et al., 2021 (aerobic) | 1 | 0 | 0 | 1 | 1 | 3 | 2 | 0 | 2 | 1 | 0 | 1 | 1 | 7 | 10 |
| Schulz et al., 2004 (aerobic) | 1 | 0 | 1 | 1 | 0 | 3 | 0 | 0 | 2 | 1 | 0 | 0 | 1 | 4 | 7 |
| Wens et al., 2016 (mixed) | 1 | 1 | 1 | 1 | 0 | 4 | 3 | 0 | 2 | 1 | 0 | 1 | 1 | 8 | 12 |
| Total (across sub-scores) | 14 | 4 | 7 | 7 | 6 | 18 | 0 | 24 | 13 | 0 | 11 | 13 | Median = 8.5 | ||
| Study | MS Participants | Intervention | Type of Training | Neurotrophic Factors Primary Outcome | Physiological and/or Functional Adaptations | |
|---|---|---|---|---|---|---|
| MS type (RR/SP/PP) Number of participants (m/f%) EDSS (mean/median score or range) Age (mean years or range) TSD (mean years) | Duration (weeks) Sessions/week (s/wk) Session duration (min) Intensity | (yes/no/not reported) Methods for Assessing Neurotrophic Factors Neurotrophic Factor(s) Adaptations | Neuroprotective Adaptations (yes/no/not reported) | |||
| Abbaspoor et al., 2020 | RR n = 16 (0/100%) Age: 35.4 EDSS: 3.0 TSD: 10.1 | 1: MIX 2: Control | 8 weeks, 3 s/wk AT (rhythmic): 15–20 min, 55–70% of HRmax 3 s/wk TRX or elastic band or body weight training: 1–2 × 8–14 reps, 1 s/wk | Not reported | Grip strength ↑BG Finger pinch strength 2 min walking distance (↑BG) Walking speed ↑BG Knee ext strength Not reported | |
| Methods: Blood samples 48 h before and after intervention. Serum analyzed by ELISA kit (BDNF: Shanghai Crystal Day Biotech Co, China; IGF-1: Mediagnost, Germany). Centrifugation 3000 g for 10 min. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF IGF-1 ↑BG | |||||
| Askari et al., 2017 | MS type not reported n = 30 (0/100%) Age: 35.1 EDSS: not reported TSD: not reported | 1: AT 2: RT 3: Control NB: results from AT and RT are pooled into a MIX group. | 8 weeks, 3 s/wk AT (aquatic): 30 min, no intensity reported RT: 30–45 min, 40–70% of 1RM, machines, 2–3 × 10–14 reps | Not reported | Not reported Not reported | |
| Methods: Blood samples 48 h before and after intervention. Plasma analyzed with ELISA kit (NT4: Chongqing Biospes Co, China). Centrifugation not reported. Storage −70 °C. | ||||||
| Acute: | Chronic: NT4 ↑BG (AT and RT vs control) | |||||
| Banitalebi et al., 2020 | RR n = 89 (0/100%) Age: not reported EDSS 0–4: n = 45 EDSS 4.5–6.0: n = 25 EDSS 6.5–8.0: n = 19 TSD: Not reported | 1: MIX 2: Control | 12 weeks, 3 s/wk 100 min (in total) AT (bike or run): 50–70% of HRmax RT (whole body): 40–70% of 1RM, 3 × 12 reps Balance: static + weight shift, no further details reported Pilates: no details reported Stretching: to pain threshold, no further details reported | Not reported | Knee ext strength ↑BG VO2max ↑BG Body fat % ↓BG Not reported | |
| Methods: Blood samples before and after intervention (after overnight fasting). Serum analyzed by ELISA kit (BDNF, NT3, NT4/5, GDNF: Boster Bio, CA, US; CNTF: Stabiopharm, Singapore). Centrifugation 500 g for 12 min at 4 °C. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF ↑BG NT3 ↑BG NT4/5 ↑BG GDNF CNTF | |||||
| Briken et al., 2016 | SP/PP (31/11) n = 42 (42.9/57.1%) EDSS: 4.9 Age: 50.0 TSD: 16.3 | 1: AT (arm ergometry) 2: AT (bicycle) 3: AT (rowing) 4: Control | 9 weeks, 2–3 s/wk 15–45 min (in total) AT: 120–130% of anaerobic threshold | No (primary outcome: Vo2max) | Vo2max ↑BG (bicycle vs control) 6 min walking distance ↑BG (arm and bicycle vs control) Not reported | |
| Method: Blood samples before and after intervention (at rest). Serum analyzed by ELISA kit (BDNF: Promega, WI, US). Centrifugation not reported. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF | |||||
| Eftekhari et al., 2018 | RR (Interferon-β) n = 25 (0/100%) EDSS: 2.0–6.0 Age: 33 TSD: not reported | 1: Pilates (mat) 2: Control (waitlist) | 8 weeks, 3 s/wk 30–40 min Pilates: main exercises included hundred, roll-up/-down, single leg circle movements, 1–2 × 3–10 reps (10s per rep) | Not reported | Not reported Not reported | |
| Method: Blood samples before and 48h after intervention (in the morning). Serum analyzed by ELISA kit (BDNF: Boster Bio, CA, US). Centrifugation not reported. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF ↑BG | |||||
| Joergensen et al., 2019 | RR (Interferon-α or -β) n = 30 (26.7/73.3%) EDSS: 3.0 Age: 44.5 TSD: 7.0 | 1: RT 2: Control (habitual lifestyle) | 24 weeks, 2 s/wk 30 min RT (whole body): 3–5 × 10 reps at 15RM progressing to 6 reps at 6RM | No (primary outcome: total brain volume) | Knee ext + flex EMG ↑BG Knee ext + flex strength ↑BG Brain structure: Total brain volume (↑BG) Cortical thickness ↑BG (4 of 74 subregions) T2 lesion volume + count From Kjolhede et al. 2018 | |
| Method: Acute blood samples before and 0, 15, 45, 75, 120 min after one RT session (RT group) or 30 min rest (control group); Chronic blood samples before and after intervention (after overnight fasting at rest in supine position). Plasma analyzed by ELISA kit (BDNF: MyBioSource, CA, US). Centrifugation 1200 g for 10 min at 4 °C. Storage −80 °C. | ||||||
| Acute: BDNF | Chronic: BDNF | |||||
| Khademosharie et al., 2018 | SP/PP n = 20 (0/100%) EDSS: 3.2 Age: 20–50 TSD: not reported | 1: MIX 2: Control (habitual lifestyle) | 12 weeks, 3 s/wk (2 AT, 1 RT) RT (whole body): 60–80% of 1RM, 2–4 × 8–14 reps AT (rhythmic + jogging): 15–60 min, 40–55% of HRreserve | Not reported | Disability (EDSS) ↓BGBody fat % ↓BG Not reported | |
| Method: Blood samples before and 48 h after intervention (after overnight fasting). Serum analyzed by ELISA kit (BDNF: Boster Bio, CA, US; NGF: Eastibiopharm, CA, US). Centrifugation not reported. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF(↑BG) NGF | |||||
| Mokhtarzade et al., 2018 | RR n = 61 (34.4/65.6%) EDSS: 1.6 Age: 31 TSD: 7.5 | 1: AT (OW_I) 2: AT (NW_I) 3: Control (OW_C) 4: Control (NW_C) | 8 weeks, 3 s/wk AT (bicycle): 42–66 min, 3 × 10 min upper limbs + 3 × 10 min lower limbs, 60–75% peak power | Not reported | VO2max ↑BG Total body mass BMI Brain structure (blood–brain barrier): S100b ↓BG (NW_I vs control) NSE | |
| Method: Blood samples before and after intervention (after overnight fasting). Serum analyzed by ELISA kit (BDNF, NGF: R&D Systems, MN, US; CNTF, PDGF: IBL International, Germany). Centrifugation 3000 g for 12 min at 4 °C. Storage −80 °C. | ||||||
| Acute: | Chronic: PDGF ↑BG BDNF ↑BG (NW_I vs control) NGF CNTF | |||||
| Naghibzadeh et al., 2019 | RR n = 26 (0/100%) EDSS: 2–4 Age: 33.4 TSD: not reported | 1: MIX 2: Control 3: Swedish massage 4: AT + Swedish massage | 8 weeks, 3 s/wk AT (aquatic): 30 min, walking and jumping, balance etc., no intensity reported | Not reported | Knee flex strength ↑BG (all AT groups vs control) Knee ext strength ↑BG (all AT groups vs control) Grip strength Not reported | |
| Method: Blood samples 48 h before and 48 h after intervention. Plasma analyzed by ELISA kit (BDNF: Boster Bio, CA, US; NGF, CNTF: Chongqing Biospes Co, China). Centrifugation not reported. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF NGF ↑BG CNTF | |||||
| Ozkul et al., 2018 | RR n = 36 MS (22.2/77.8%) EDSS: 1 Age: 33.8 TSD: 4 | 1: MIX 2: Control 3: Healthy controls (n = 18) | 8 weeks, 3 s/wk AT (treadmill walk): 20–60 min, 60–80% HRmax Pilates: 60 min, multiple exercises, 10–20 reps per exercise | Yes (with suppressors of cytokine signaling proteins) | Postural stability * 6 min walking distance * ↑BG Fatigue severity scale * ↓BG Not reported | |
| Method: Blood samples before and after intervention (at rest). Serum analyzed by ELISA kit (BDNF: Shanghai Sunred Biological technology, China). Centrifugation 3000 g for 10 min. Storage −40 °C. | ||||||
| Acute: | Chronic: BDNF * | |||||
| Rezaee et al., 2020 | RR n = 20 (60/40%) EDSS: 2.4 Age: 28.7 TSD: not reported | 1: AT 2: Control | 6 weeks, 3 s/wk AT (bicycle): 30 min, 60% of VO2max | Yes (with tumor necrosis factor alpha) | Not reported Not reported | |
| Method: Acute/chronic blood samples before (in the morning) and immediately after 1st and 18th AT session. Serum analyzed by ELISA kit (VEGF: ZellBio GmbH, Germany). Centrifugation 3000 g for 15 min at 4 °C. Storage −80 °C. | ||||||
| Acute: VEGF ↑BG | Chronic: VEGF | |||||
| Savsek et al., 2021 | RR n = 28 (82.1/17.9%) EDSS: 2.8 Age: 41 TSD: 11.6 | 1: AT 2: Control (habitual lifestyle) | 12 weeks, 2 s/wk AT (aerobics): 30–40 min (60 min including warm-up and cool-down), 60–70% HRreserve | No (primary outcomes: brain structures) | Disability (EDSS) # Modified fatigue impact scale # Walking speed # ↑BG Brain structure: Total brain volume Gray matter brain volume T2 lesion volume + count Cortical lesion volume + count Active lesion volume + count * ↑BG Substructures ↑BG (5 of 15 substructures) | |
| Method: Blood samples before and after intervention (in the morning at rest). Serum analyzed by ELISA kit (BDNF: R&D Systems, MN, US). Centrifugation 3500 g for 5 min. Storage −20 °C. | ||||||
| Acute: | Chronic: BDNF # (↑BG) | |||||
| Schulz et al., 2004 | RR/SP/PP n = 28 (32/68%) EDSS: 2.3 Age: 39.5 TSD: 11.4 | 1: AT 2: Control (waitlist) | 8 weeks, 2 s/wk AT (bicycle): 30 min, 75% of Wattmax | Not reported | VO2max Not reported | |
| Method: Blood samples before and after intervention. Serum analyzed by ELISA kit (BDNF: Promega, WI, US; NGF: sensitive and specific two-site enzyme immunoassay). Centrifugation not specified. Storage −80 °C. | ||||||
| Acute: | Chronic: NGF (↓BG) BDNF | |||||
| Wens et al., 2016 | RR n = 22 (36.4/63.6%) EDSS: 2.6 Age: 43 TSD: not reported | 1: MIX 2: Control (sedentary) 3: HC (n = 19) | 24 weeks, 5 s/2 wk 45–75 min (in total) AT (bicycle or treadmill): 1–3 × 10 min, 12–14 on BORG20 Scale RT: 1–4 × 10–15 reps, 12–14 on BORG20 Scale | Yes | Knee flex strength ↑BG Knee ext strength ↑BG Fat mass Total body mass Not reported | |
| Method: Blood samples before and 48h after intervention (at rest). Serum analyzed by Elisa kit (BDNF: Meso Scale Discovery, MD, US). Centrifugation 3000 g for 10 mn. Storage −80 °C. | ||||||
| Acute: | Chronic: BDNF ↑BG | |||||
| Summary | n = 473 (n = 366 women) (23/77%) Median EDSS: 2.6 Mean TSD: 9.7 years Mean age: 37.4 years | RT: 1 AT: 5 MIX: 7 Pilates: 1 | 8–24 weeks 2–5 s/wk RT and AT: low-to-high intensity | No. of studies reporting on neurotrophic factors (and ↑BG): Acute: BDNF 1/14 (↑BG in 0/1), VEGF 1/14 (↑BG in 1/1) Chronic: BDNF 12/14 (↑BG in 6/12), IGF-1 1/14 (↑BG in 1/1), NT4 1/14 (↑BG in 1/1), NT3 1/14 (↑BG in 1/1), NT4/5 1/14 (↑BG in 1/1), GDNF 1/14 (↑BG in 0/1), CNTF 3/14 (↑BG in 0/3), NGF 4/14 (↑BG in 1/4), PDGF 1/14 (↑BG in 1/1), VEGF 1/14 (↑BG in 1/1) | No. of studies reporting on physiological/functional outcomes (and ↑BG): 11/14 (↑BG in 10/11; one or more outcomes) No. of studies reporting parallel ↑BG (one or more outcomes) in physiological/functional outcomes and acute neurotrophic factors: 1/2 or chronic neurotrophic factors: 8/11 No. of studies reporting parallel ↑BG (one or more outcomes) in neuroprotection and acute neurotrophic factors: 0/1 or chronic neurotrophic factors: 2/3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diechmann, M.D.; Campbell, E.; Coulter, E.; Paul, L.; Dalgas, U.; Hvid, L.G. Effects of Exercise Training on Neurotrophic Factors and Subsequent Neuroprotection in Persons with Multiple Sclerosis—A Systematic Review and Meta-Analysis. Brain Sci. 2021, 11, 1499. https://doi.org/10.3390/brainsci11111499
Diechmann MD, Campbell E, Coulter E, Paul L, Dalgas U, Hvid LG. Effects of Exercise Training on Neurotrophic Factors and Subsequent Neuroprotection in Persons with Multiple Sclerosis—A Systematic Review and Meta-Analysis. Brain Sciences. 2021; 11(11):1499. https://doi.org/10.3390/brainsci11111499
Chicago/Turabian StyleDiechmann, Mette D., Evan Campbell, Elaine Coulter, Lorna Paul, Ulrik Dalgas, and Lars G. Hvid. 2021. "Effects of Exercise Training on Neurotrophic Factors and Subsequent Neuroprotection in Persons with Multiple Sclerosis—A Systematic Review and Meta-Analysis" Brain Sciences 11, no. 11: 1499. https://doi.org/10.3390/brainsci11111499
APA StyleDiechmann, M. D., Campbell, E., Coulter, E., Paul, L., Dalgas, U., & Hvid, L. G. (2021). Effects of Exercise Training on Neurotrophic Factors and Subsequent Neuroprotection in Persons with Multiple Sclerosis—A Systematic Review and Meta-Analysis. Brain Sciences, 11(11), 1499. https://doi.org/10.3390/brainsci11111499