
DiODe v2: Unambiguous and Fully-Automated Detection of Directional DBS Lead Orientation

 ,
,  ,
, {kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Ethics
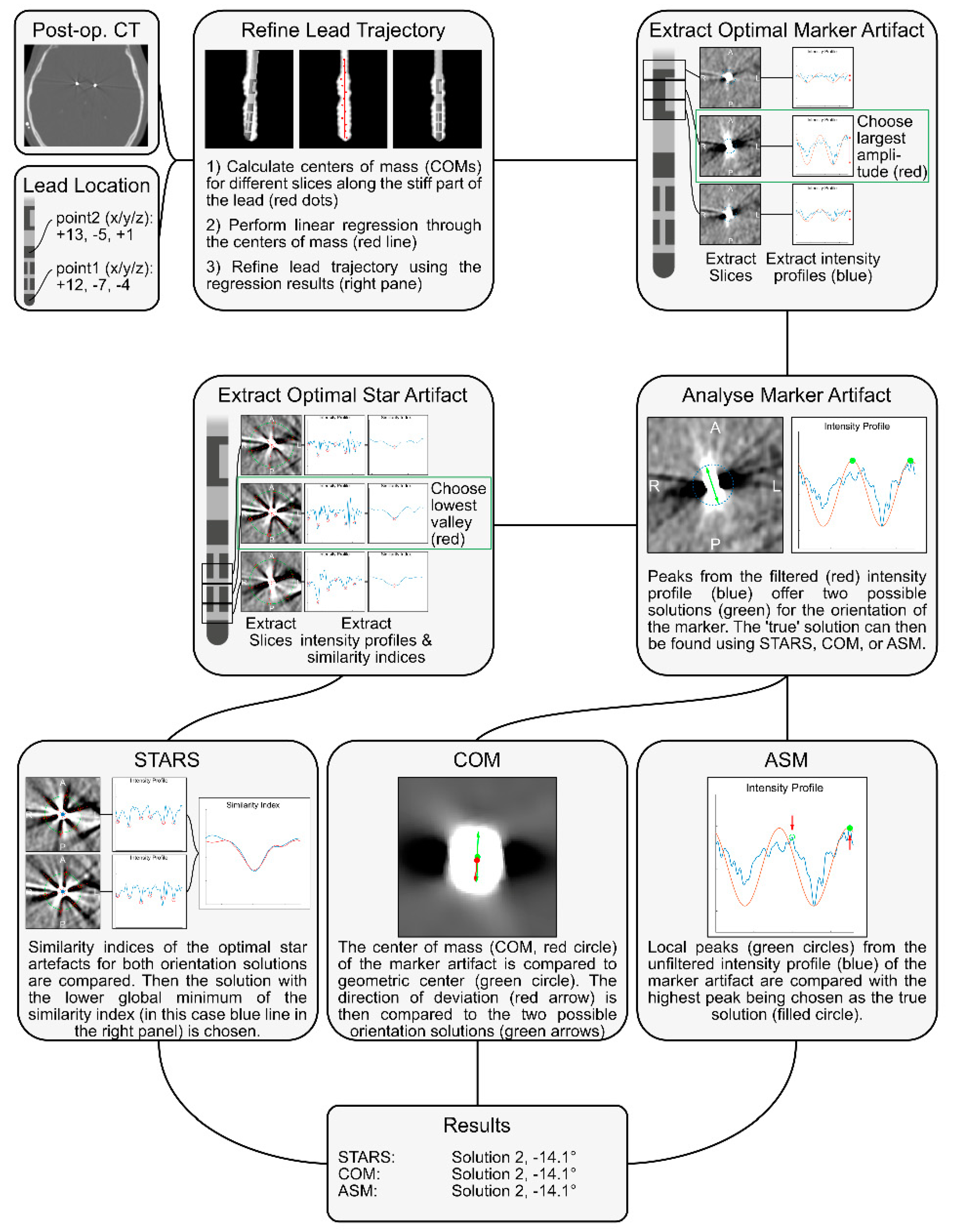
2.2. DiODe v2
2.3. Center of Mass (COM)
2.4. Asymmetric Sampling of the Marker (ASM)
2.5. Star Artifact Symmetry (STARS)
2.6. Dataset
2.7. Analysis
3. Results
4. Discussion
5. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rebelo, P.; Green, A.; Aziz, T.; Kent, A.; Schafer, D.; Venkatesan, L.; Cheeran, B. Thalamic directional deep brain stimulation for tremor: Spend less, get more. Brain Stimul. 2018, 11, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.A.; Reker, P.; Visser-Vandewalle, V.; Wirths, J.; Treuer, H.; Klehr, M.; Roediger, J.; Dafsari, H.S.; Barbe, M.T.; Timmermann, L. Directional DBS increases side-effect thresholds-A prospective, double-blind trial. Mov. Disord. 2017, 32, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Noecker, A.M.; Frankemolle-Gilbert, A.M.; Howell, B.; Petersen, M.V.; Beylergil, S.B.; Shaikh, A.G.; McIntyre, C.C. StimVision v2: Examples and applications in subthalamic deep brain stimulation for Parkinson’s disease. Neuromodul. Technol. Neural Interface 2021, 24, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.A.; Roediger, J.; Horn, A.; Reker, P.; Oehrn, C.R.; Dafsari, H.S.; Li, N.; Kühn, A.A.; Fink, G.R.; Visser-Vandewalle, V.; et al. Probabilistic sweet spots predict motor outcome for deep brain stimulation in Parkinson disease. Ann. Neurol. 2019, 86, 527–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.K.; Nowacki, A.; Debove, I.; Petermann, K.; Tinkhauser, G.; Wiest, R.; Schüpbach, M.; Krack, P.; Pollo, C. Directional stimulation of subthalamic nucleus sweet spot predicts clinical efficacy: Proof of concept. Brain Stimul. 2019, 12, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Petry-Schmelzer, J.N.; Dembek, T.A.; Steffen, J.K.; Jergas, H.; Dafsari, H.S.; Fink, G.R.; Visser-Vandewalle, V.; Barbe, M.T. Selecting the most effective DBS contact in essential tremor patients based on individual tractography. Brain Sci. 2020, 10, 1015. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.; Hoevels, M.; Hellerbach, A.; Horn, A.; Petry-Schmelzer, J.; Borggrefe, J.; Wirths, J.; Dafsari, H.; Barbe, M.; Visser-Vandewalle, V.; et al. Directional DBS leads show large deviations from their intended implantation orientation. Park. Relat. Disord. 2019, 67, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.A.; Asendorf, A.L.; Wirths, J.; Barbe, M.T.; Visser-Vandewalle, V.; Treuer, H. Temporal stability of lead orientation in directional deep brain stimulation. Ster. Funct. Neurosurg. 2021, 99, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Rau, A.; Urbach, H.; Coenen, V.A.; Egger, K.; Reinacher, P.C. Deep brain stimulation electrodes may rotate after implantation—An animal study. Neurosurg. Rev. 2021, 44, 2349–2353. [Google Scholar] [CrossRef] [PubMed]
- Lange, F.; Steigerwald, F.; Engel, D.; Malzacher, T.; Neun, T.; Fricke, P.; Volkmann, J.; Matthies, C.; Capetian, P. Longitudinal assessment of rotation angles after implantation of directional deep brain stimulation leads. Ster. Funct. Neurosurg. 2021, 99, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Reinacher, P.; Krüger, M.; Coenen, V.; Shah, M.; Roelz, R.; Jenkner, C.; Egger, K. Determining the orientation of directional deep brain stimulation electrodes using 3D rotational fluoroscopy. Am. J. Neuroradiol. 2017, 38, 1111–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunsche, S.; Neudorfer, C.; El Majdoub, F.; Maarouf, M.; Sauner, D. Determining the rotational orientation of directional deep brain stimulation leads employing flat-panel computed tomography. Oper. Neurosurg. 2018, 16, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Yalaz, M.; Noor, M.S.; McIntyre, C.C.; Butz, M.; Schnitzler, A.; Deuschl, G.; Höft, M. DBS electrode localization and rotational orientation detection using SQUID-based magnetoencephalography. J. Neural Eng. 2021, 18, 026021. [Google Scholar] [CrossRef] [PubMed]
- Hellerbach, A.; Dembek, T.A.; Hoevels, M.; Holz, J.A.; Gierich, A.; Luyken, K.; Barbe, M.T.; Wirths, J.; Visser-Vandewalle, V.; Treuer, H. DiODe: Directional orientation detection of segmented deep brain stimulation leads: A sequential algorithm based on CT imaging. Ster. Funct. Neurosurg. 2018, 96, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Sitz, A.; Hoevels, M.; Hellerbach, A.; Gierich, A.; Luyken, K.; Dembek, T.A.; Klehr, M.; Wirths, J.; Visser-Vandewalle, V.; Treuer, H. Determining the orientation angle of directional leads for deep brain stimulation using computed tomography and digital X-ray imaging: A phantom study. Med. Phys. 2017, 44, 4463–4473. [Google Scholar] [CrossRef] [PubMed]
- Kurtev-Rittstieg, R.; Achatz, S.; Nourinia, A.; Mittermeyer, S. Orientation of directional deep brain stimulation leads on CT: Resolving the ambiguity. bioRxiv 2020. [Google Scholar] [CrossRef]
- Horn, A.; Li, N.; Dembek, T.A.; Kappel, A.; Boulay, C.; Ewert, S.; Tietze, A.; Husch, A.; Perera, T.; Neumann, W.-J.; et al. Lead-DBS v2: Towards a comprehensive pipeline for deep brain stimulation imaging. NeuroImage 2019, 184, 293–316. [Google Scholar] [CrossRef] [PubMed]
- Avants, B.; Epstein, C.; Grossman, M.; Gee, J. Symmetric diffeomorphic image registration with cross-correlation: Evaluating automated labeling of elderly and neurodegenerative brain. Med. Image Anal. 2008, 12, 26–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husch, A.; Petersen, M.; Gemmar, P.; Goncalves, J.; Hertel, F. PaCER-A fully automated method for electrode trajectory and contact reconstruction in deep brain stimulation. NeuroImage Clin. 2018, 17, 80–89. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dembek, T.A.; Hellerbach, A.; Jergas, H.; Eichner, M.; Wirths, J.; Dafsari, H.S.; Barbe, M.T.; Hunsche, S.; Visser-Vandewalle, V.; Treuer, H. DiODe v2: Unambiguous and Fully-Automated Detection of Directional DBS Lead Orientation. Brain Sci. 2021, 11, 1450. https://doi.org/10.3390/brainsci11111450
Dembek TA, Hellerbach A, Jergas H, Eichner M, Wirths J, Dafsari HS, Barbe MT, Hunsche S, Visser-Vandewalle V, Treuer H. DiODe v2: Unambiguous and Fully-Automated Detection of Directional DBS Lead Orientation. Brain Sciences. 2021; 11(11):1450. https://doi.org/10.3390/brainsci11111450
Chicago/Turabian StyleDembek, Till A., Alexandra Hellerbach, Hannah Jergas, Markus Eichner, Jochen Wirths, Haidar Salimi Dafsari, Michael T. Barbe, Stefan Hunsche, Veerle Visser-Vandewalle, and Harald Treuer. 2021. "DiODe v2: Unambiguous and Fully-Automated Detection of Directional DBS Lead Orientation" Brain Sciences 11, no. 11: 1450. https://doi.org/10.3390/brainsci11111450
APA StyleDembek, T. A., Hellerbach, A., Jergas, H., Eichner, M., Wirths, J., Dafsari, H. S., Barbe, M. T., Hunsche, S., Visser-Vandewalle, V., & Treuer, H. (2021). DiODe v2: Unambiguous and Fully-Automated Detection of Directional DBS Lead Orientation. Brain Sciences, 11(11), 1450. https://doi.org/10.3390/brainsci11111450