
Reaction Time and Visual Memory in Connection to Hazardous Drinking Polygenic Scores in Schizophrenia, Schizoaffective Disorder and Bipolar Disorder

 ,
,  , , , , , , , , , , , , ,
, , , , , , , , , , , , ,  , , ,
, , ,  and add
Show full author list
and add
Show full author list
Abstract
1. Introduction
- The association of hazardous drinking PGS with reaction time and visual memory in schizophrenia patients;
- The association of hazardous drinking PGS with reaction time and visual memory in schizoaffective disorder patients;
- The association of hazardous drinking PGS with reaction time and visual memory in bipolar disorder patients.
2. Materials and Methods
2.1. Application of STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Checklist for Cross-Sectional Studies
2.2. Study Design
2.3. Timetable
2.4. Participant Number Estimation
2.5. Sample Collection Strategy
2.6. Exclusion Criteria
2.7. Missing Data Handling
2.8. Data Handling
2.9. Data Storage
2.10. Sensitivity Analyses
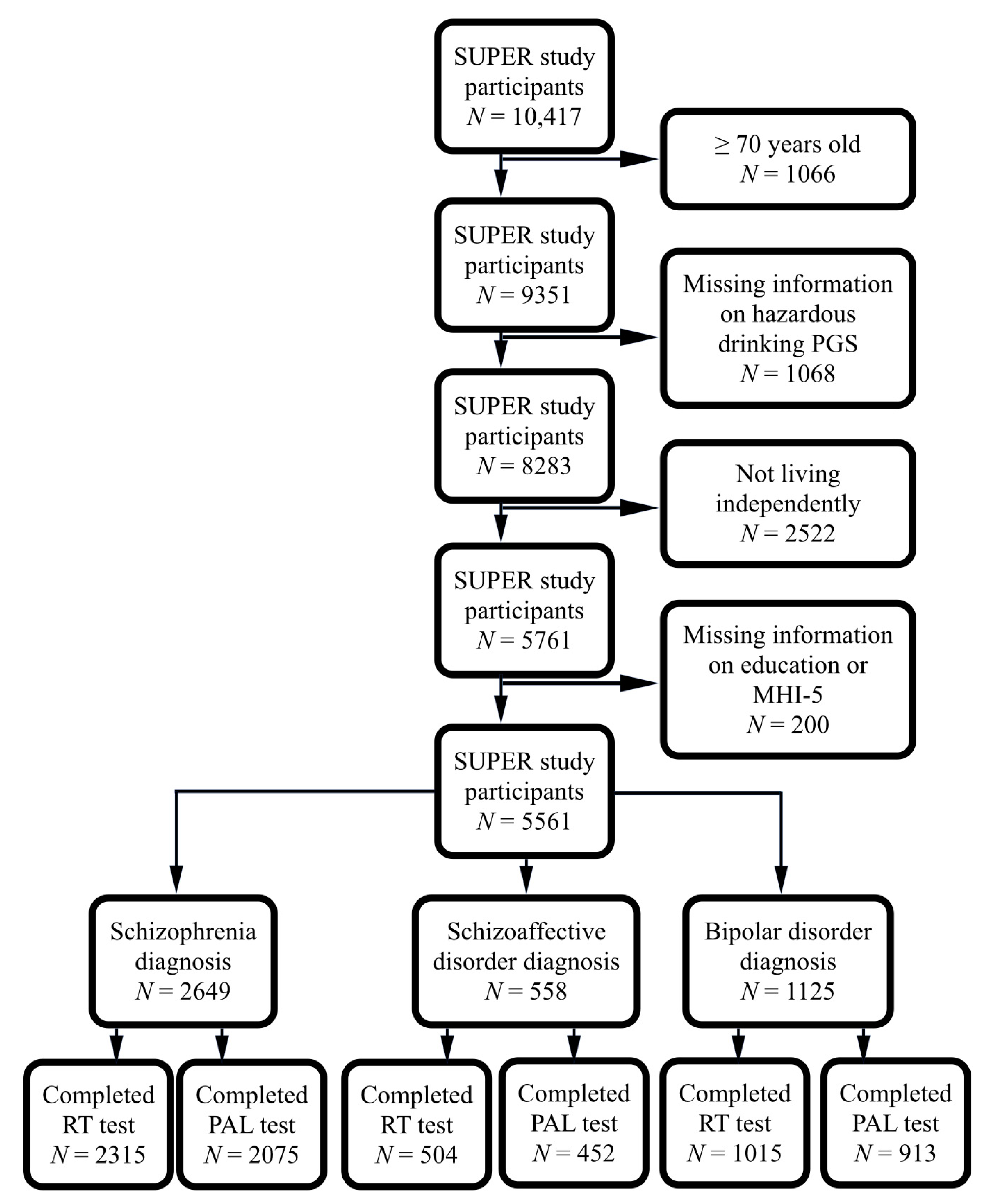
2.11. Participants
2.12. Schizophrenia Diagnoses
2.13. Schizoaffective Disorder Diagnoses
2.14. Bipolar Disorder Diagnoses
2.15. Hazardous Drinking Polygenic Scores
2.16. Cognitive Measures
2.17. Confounding Factors
2.17.1. Age
2.17.2. Age of Onset
2.17.3. Education
2.17.4. Household Pattern
2.17.5. Depressive Symptoms
2.18. Statistical Methods
3. Results
3.1. Background Factors and Hazardous Drinking PGS in Male and Female Schizophrenia Patients
3.2. Background Factors and Hazardous Drinking PGS in Male and Female Schizoaffective Disorder Patients
3.3. Background Factors and Hazardous Drinking PGS in Male and Female Bipolar Disorder Patients
3.4. Association of Hazardous Drinking PGS with RT Test and PAL Test in Male and Female Schizophrenia Patients
3.5. Association of Hazardous Drinking PGS with RT Test and PAL Test in Male and Female Schizoaffective Disorder Patients
3.6. Association of Hazardous Drinking PGS with RT Test and PAL Test in Male and Female Bipolar Disorder Patients
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Studies
4.3. Strengths
4.4. Limitations
4.5. What Is Already Known on This Subject?
4.6. What Does This Study Add?
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanchez-Roige, S.; Palmer, A.A.; Clarke, T.K. Recent Efforts to Dissect the Genetic Basis of Alcohol Use and Abuse. Biol. Psychiatry 2020, 87, 609–618. [Google Scholar] [CrossRef]
- Sanchez-Roige, S.; Palmer, A.A.; Fontanillas, P.; Elson, S.L.; Adams, M.J.; Howard, D.M.; Edenberg, H.J.; Davies, G.; Crist, R.C.; Deary, I.J.; et al. Genome-Wide Association Study Meta-Analysis of the Alcohol Use Disorders Identification Test (AUDIT) in Two Population-Based Cohorts. Am. J. Psychiatry 2019, 176, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Meyers, J.L.; Chorlian, D.B.; Johnson, E.C.; Pandey, A.K.; Kamarajan, C.; Salvatore, J.E.; Aliev, F.; Subbie-Saenz de Viteri, S.; Zhang, J.; Chao, M.; et al. Association of Polygenic Liability for Alcohol Dependence and EEG Con-nectivity in Adolescence and Young Adulthood. Brain Sci. 2019, 9, 280. [Google Scholar] [CrossRef]
- Clarke, T.K.; Smith, A.H.; Gelernter, J.; Kranzler, H.R.; Farrer, L.A.; Hall, L.S.; Fernandez-Pujals, A.M.; MacIntyre, D.J.; Smith, B.H.; Hocking, L.J.; et al. Polygenic risk for alcohol dependence associates with alcohol consumption, cognitive function and social deprivation in a population-based cohort. Addict. Biol. 2016, 21, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L. Alcohol consumption and cognitive impairment in older men: A mendelian randomization study. Neurology 2014, 82, 1038–1044. [Google Scholar] [CrossRef] [PubMed]
- Kumari, M.; Holmes, M.V.; Dale, C.E.; Hubacek, J.A.; Palmer, T.M.; Pikhart, H.; Peasey, A.; Britton, A.; Horvat, P.; Kubinova, R.; et al. Alcohol consumption and cognitive performance: A Mendelian randomization study. Addict. Abingdon Engl. 2014, 109, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- Au Yeung, S.L.; Jiang, C.Q.; Cheng, K.K.; Liu, B.; Zhang, W.S.; Lam, T.H.; Leung, G.M.; Schooling, C.M. Evaluation of moderate alcohol use and cognitive function among men using a Mendelian randomization design in the Guangzhou biobank cohort study. Am. J. Epidemiol. 2012, 175, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Kuźma, E.; Hannon, E.; Zhou, A.; Lourida, I.; Bethel, A.; Levine, D.A.; Lunnon, K.; Thompson-Coon, J.; Hyppönen, E.; Llewellyn, D.J. Which Risk Factors Causally Influence Dementia? A Systematic Review of Mendelian Randomization Studies. J. Alzheimers Dis. 2018, 64, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Hasan, O.; Black, S.E.; Shield, K.D.; Schwarzinger, M. Alcohol use and dementia: A systematic scoping review. Alzheimers Res. Ther. 2019, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Mugavin, J.; MacLean, S.; Room, R.; Callinan, S. Adult low-risk drinkers and abstainers are not the same. BMC Public Health 2020, 20, 37. [Google Scholar] [CrossRef] [PubMed]
- Haber, J.R.; Harris-Olenak, B.; Burroughs, T.; Jacob, T. Residual Effects: Young Adult Diagnostic Drinking Predicts Late-Life Health Outcomes. J. Stud. Alcohol Drugs 2016, 77, 859–867. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saarni, S.I.; Joutsenniemi, K.; Koskinen, S.; Suvisaari, J.; Pirkola, S.; Sintonen, H.; Poikolainen, K.; Lönnqvist, J. Alcohol consumption, abstaining, health utility, and quality of life—A general population survey in Finland. Alcohol Alcohol. 2008, 43, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Fillmore, K.M.; Stockwell, T.; Chikritzhs, T.; Bostrom, A.; Kerr, W. Moderate Alcohol Use and Reduced Mortality Risk: Systematic Error in Prospective Studies and New Hypotheses. Ann. Epidemiol. 2007, 17, s2–s16. [Google Scholar] [CrossRef]
- Gémes, K.; Janszky, I.; Strand, L.B.; László, K.D.; Ahnve, S.; Vatten, L.J.; Dalen, H.; Mukamal, K.J. Light-moderate alcohol consumption and left ventricular function among healthy, middle-aged adults: The HUNT study. BMJ Open 2018, 8, e020777. [Google Scholar] [CrossRef]
- Kiiskinen, T.; Mars, N.J.; Palviainen, T.; Koskela, J.; Rämö, J.T.; Ripatti, P.; Ruotsalainen, S.; Palotie, A.; Madden, P.; Rose, R.J.; et al. Genomic prediction of alcohol-related morbidity and mortality. Transl. Psychiatry 2020, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.C.; Sanchez-Roige, S.; Acion, L.; Adams, M.J.; Bucholz, K.K.; Chan, G.; Chao, M.J.; Chorlian, D.B.; Dick, D.M.; Edenberg, H.J.; et al. Polygenic contributions to alcohol use and alcohol use disorders across population-based and clinically ascertained samples. Psychol Med. 2020, 51, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.H.; Whitfield, J.B.; Liu, M.; Medland, S.E.; Hickie, I.B.; Martin, N.G.; Verhulst, B.; Heath, A.C.; Madden, P.A.; Statham, D.J.; et al. Associations between polygenic risk for tobacco and alcohol use and liability to tobacco and alcohol use, and psychiatric disorders in an independent sample of 13,999 Australian adults. Drug Alcohol Depend. 2019, 205, 107704. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D. Domains of cognition and their assessment. Dialogues Clin. Neurosci. 2019, 21, 227–237. [Google Scholar] [CrossRef]
- Reilly, M.T.; Noronha, A.; Goldman, D.; Koob, G.F. Genetic studies of alcohol dependence in the context of the addiction cycle. Neuropharmacology 2017, 122, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Vilhjálmsson, B.J.; Yang, J.; Finucane, H.K.; Gusev, A.; Lindström, S.; Ripke, S.; Genovese, G.; Loh, P.R.; Bhatia, G.; Do, R.; et al. Modeling Linkage Disequilibrium Increases Accuracy of Polygenic Risk Scores. Am. J. Hum. Genet. 2015, 97, 576–592. [Google Scholar] [CrossRef] [PubMed]
- Van Hooren, S.A.H.; Valentijn, A.M.; Bosma, H.; Ponds, R.W.H.M.; Van Boxtel, M.P.J.; Jolles, J. Cognitive functioning in healthy older adults aged 64–81: A cohort study into the effects of age, sex, and education. Aging Neuropsychol. Cogn. 2007, 14, 40–54. [Google Scholar] [CrossRef] [PubMed]
- Biddle, K.D.; Jacobs, H.I.L.; Uquillas, F.D.; Zide, B.S.; Kirn, D.R.; Properzi, M.R.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; Donovan, N.J. Associations of Widowhood and β-Amyloid with Cognitive Decline in Cognitively Unimpaired Older Adults. JAMA Netw. Open 2020, 3, e200121. [Google Scholar] [CrossRef] [PubMed]
- Roux, P.; Raust, A.; Cannavo, A.S.; Aubin, V.; Aouizerate, B.; Azorin, J.M.; Bellivier, F.; Belzeaux, R.; Bougerol, T.; Cussac, I.; et al. Associations between residual depressive symptoms, cognition, and functioning in patients with euthymic bipolar dis-order: Results from the FACE-BD cohort. Br. J. Psychiatry 2017, 211, 381–387. [Google Scholar] [CrossRef]
- Andersson, C.; Marklund, K.; Walles, H.; Hagman, G.; Miley-Akerstedt, A. Lifestyle Factors and Subjective Cognitive Impairment in Patients Seeking Help at a Memory Disorder Clinic: The Role of Negative Life Events. Dement. Geriatr. Cogn. Disord. 2020, 48, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, A.Y.; Trygg, T.; Pitkälä, K.H.; Strandberg, T.E. Alcohol consumption in midlife and old age and risk of frailty: Alcohol paradox in a 30-year follow-up study. Age Ageing 2018, 47, 248–254. [Google Scholar] [CrossRef]
- Bora, E.; Pantelis, C. Meta-analysis of Cognitive Impairment in First-Episode Bipolar Disorder: Comparison with First-Episode Schizophrenia and Healthy Controls. Schizophr. Bull. 2015, 41, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Frangou, S. Cognitive function in early onset schizophrenia: A selective review. Front. Hum. Neurosci. 2009, 3, 79. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, T.; Bauer, I.E.; Meyer, T.D.; Kapczinski, F.; Soares, J.C. Neuroprogression and Cognitive Functioning in Bipolar Disorder: A Systematic Review. Curr. Psychiatry Rep. 2015, 17, 75. [Google Scholar] [CrossRef] [PubMed]
- Schouws, S.N.; Comijs, H.C.; Stek, M.L.; Dekker, J.; Oostervink, F.; Naarding, P.; van der Velde, I.; Beekman, A.T. Cognitive impairment in early and late bipolar disorder. Am. J. Geriatr. Psychiatry 2009, 17, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Krahn, D.; Freese, J.; Hauser, R.; Barry, K.; Goodman, B. Alcohol use and cognition at mid-life: The importance of adjusting for baseline cognitive ability and educational attainment. Alcohol. Clin. Exp. Res. 2003, 27, 1162–1166. [Google Scholar] [CrossRef]
- Donovan, N.J.; Okereke, O.I.; Vannini, P.; Amariglio, R.E.; Rentz, D.M.; Marshall, G.A.; Johnson, K.A.; Sperling, R.A. Association of Higher Cortical Amyloid Burden with Loneliness in Cognitively Normal Older Adults. JAMA Psychiatry 2016, 73, 1230–1237. [Google Scholar] [CrossRef]
- Elovanio, M.; Hakulinen, C.; Pulkki-Råback, L.; Aalto, A.M.; Virtanen, M.; Partonen, T.; Suvisaari, J. General Health Questionnaire (GHQ-12), Beck Depression Inventory (BDI-6), and Mental Health Index (MHI-5): Psychometric and predictive properties in a Finnish population-based sample. Psychiatry Res. 2020, 289, 112973. [Google Scholar] [CrossRef]
- Voyer, D.; Voyer, S.D.; Saint-Aubin, J. Sex differences in visual-spatial working memory: A meta-analysis. Psychon. Bull. Rev. 2017, 24, 307–334. [Google Scholar] [CrossRef] [PubMed]
- Herlitz, A.; Dekhtyar, S.; Asperholm, M.; Weber, D. Gender Differences in Memory and Cognition. In Encyclopedia of Geropsychology; Pachana, N., Ed.; Springer: Singapore, 2016. [Google Scholar]
- Taylor, M.; Simpkin, A.J.; Haycock, P.C.; Dudbridge, F.; Zuccolo, L. Exploration of a Polygenic Risk Score for Alcohol Consumption: A Longitudinal Analysis from the ALSPAC Cohort. PLoS ONE 2016, 11, e0167360. [Google Scholar] [CrossRef] [PubMed]
- Mistry, S.; Escott-Price, V.; Florio, A.D.; Smith, D.J.; Zammit, S. Investigating associations between genetic risk for bipolar disorder and cognitive functioning in childhood. J. Affect. Disord. 2019, 259, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Dima, D.; de Jong, S.; Breen, G.; Frangou, S. The polygenic risk for bipolar disorder influences brain regional function relating to visual and default state processing of emotional information. NeuroImage Clin. 2016, 12, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Tesli, M.; Kauppi, K.; Bettella, F.; Brandt, C.L.; Kaufmann, T.; Espeseth, T.; Mattingsdal, M.; Agartz, I.; Melle, I.; Djurovic, S.; et al. Altered Brain Activation during Emotional Face Processing in Relation to Both Diagnosis and Polygenic Risk of Bipolar Disorder. PLoS ONE 2015, 10, e0134202. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zhang, X.; Li, A.; Zhu, M.; Liu, S.; Qin, W.; Li, J.; Yu, C.; Jiang, T.; Liu, B. Polygenic risk for five psychiatric disorders and cross-disorder and disorder-specific neural connectivity in two independent populations. NeuroImage Clin. 2017, 14, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Whalley, H.C.; Papmeyer, M.; Sprooten, E.; Romaniuk, L.; Blackwood, D.H.; Glahn, D.C.; Hall, J.; Lawrie, S.M.; Sussmann, J.; McIntosh, A.M. The influence of polygenic risk for bipolar disorder on neural activation assessed using fMRI. Transl. Psychiatry 2012, 2, e130. [Google Scholar] [CrossRef]
- Bartholow, B.D.; Fleming, K.A.; Wood, P.K.; Cowan, N.; Saults, J.S.; Altamirano, L.; Miyake, A.; Martins, J.; Sher, K.J. Alcohol effects on response inhibition: Variability across tasks and individuals. Exp. Clin. Psychopharmacol. 2018, 26, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Mayhugh, R.E.; Moussa, M.N.; Simpson, S.L.; Lyday, R.G.; Burdette, J.H.; Porrino, L.J.; Laurienti, P.J. Moderate-Heavy Alcohol Consumption Lifestyle in Older Adults Is Associated with Altered Central Executive Network Community Structure during Cognitive Task. PLoS ONE 2016, 11, e0160214. [Google Scholar] [CrossRef]
- Carrilho, P.E.; Santos, M.B.; Piasecki, L.; Jorge, A.C. Marchiafava-Bignami disease: A rare entity with a poor outcome. Rev. Bras. Ter. Intensiva 2013, 25, 68–72. [Google Scholar] [CrossRef]
- Kim, J.W.; Lee, D.Y.; Lee, B.C.; Jung, M.H.; Kim, H.; Choi, Y.S.; Choi, I.G. Alcohol and cognition in the elderly: A review. Psychiatry Investig. 2012, 9, 8–16. [Google Scholar] [CrossRef]
- Reas, E.T.; Laughlin, G.A.; Kritz-Silverstein, D.; Barrett-Connor, E.; McEvoy, L.K. Moderate, Regular Alcohol Consumption is Associated with Higher Cognitive Function in Older Community-Dwelling Adults. J. Prev. Alzheimers Dis. 2016, 3, 105–113. [Google Scholar] [CrossRef]
- Panza, F.; Frisardi, V.; Seripa, D.; Logroscino, G.; Santamato, A.; Imbimbo, B.P.; Scafato, E.; Pilotto, A.; Solfrizzi, V. Alcohol consumption in mild cognitive impairment and dementia: Harmful or neuroprotective? Int. J. Geriatr. Psychiatry 2012, 27, 1218–1238. [Google Scholar] [CrossRef] [PubMed]
- Bond, G.E.; Burr, R.; McCurry, S.M.; Graves, A.B.; Larson, E.B. Alcohol, aging, and cognitive performance in a cohort of Japanese Americans aged 65 and older: The Kame project. Int. Psychogeriatr. 2001, 13, 207–223. [Google Scholar] [CrossRef] [PubMed]
- Spencer, R.L.; Hutchison, K.E. Alcohol, aging, and the stress response. Alcohol Res. Health 1999, 23, 272–283. [Google Scholar] [PubMed]
- Moussa, M.N.; Simpson, S.L.; Mayhugh, R.E.; Grata, M.E.; Burdette, J.H.; Porrino, L.J.; Laurienti, P.J. Long-term moderate alcohol consumption does not exacerbate age-related cognitive decline in healthy, community-dwelling older adults. Front. Aging Neurosci. 2015, 6, 341. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Elbaz, A.; Britton, A.; Bell, S.; Dugravot, A.; Shipley, M.; Kivimaki, M.; Singh-Manoux, A. Alcohol consumption and cognitive decline in early old age. Neurology 2014, 82, 332–339. [Google Scholar] [CrossRef]
- Calvin, C.M.; Deary, I.J.; Webbink, D.; Smith, P.; Fernandes, C.; Lee, S.H.; Luciano, M.; Visscher, P.M. Multivariate genetic analyses of cognition and academic achievement from two population samples of 174,000 and 166,000 school children. Behav. Genet. 2012, 42, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.M.; Wright, M.J.; Luciano, M.; Martin, N.G.; de Geus, E.J.; van Beijsterveldt, C.E.; Bartels, M.; Posthuma, D.; Boomsma, D.I.; Davis, O.S.; et al. The heritability of general cognitive ability increases linearly from childhood to young adulthood. Mol. Psychiatry 2010, 15, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Enoch, M.A.; Goldman, D. The genetics of alcoholism and alcohol abuse. Curr. Psychiatry Rep. 2001, 3, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Emberson, J.R.; Bennett, D.A. Effect of alcohol on risk of coronary heart disease and stroke: Causality, bias, or a bit of both? Vasc. Health Risk Manag. 2006, 2, 239–249. [Google Scholar] [CrossRef]
- Taylor, A.E.; Lu, F.; Carslake, D.; Hu, Z.; Qian, Y.; Liu, S.; Chen, J.; Shen, H.; Smith, G.D. Exploring causal associations of alcohol with cardiovascular and metabolic risk factors in a Chinese population using Mendelian randomization analysis. Sci. Rep. 2015, 5, 14005. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, T.; Donath, S.; Cooper-Stanbury, M.; Chikritzhs, T.; Catalano, P.; Mateo, C. Under-reporting of alcohol consumption in household surveys: A comparison of quantity-frequency, graduated-frequency and recent recall. Addict. Abingdon Engl. 2004, 99, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.C.; Waterton, J.J. Under-reporting of alcohol consumption in sample surveys: The effect of computer interviewing in fieldwork. Br. J. Addict. 1984, 79, 303–308. [Google Scholar] [CrossRef]
- Xue, A.; Jiang, L.; Zhu, Z.; Wray, N.R.; Visscher, P.M.; Zeng, J.; Yang, J. Genome-wide analyses of behavioural traits are subject to bias by misreports and longitudinal changes. Nat. Commun. 2021, 12, 20211. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.M.; Kaptoge, S.; Butterworth, A.S.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.S.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: Combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef]
- Peña, S.; Mäkelä, P.; Härkänen, T.; Heliövaara, M.; Gunnar, T.; Männistö, S.; Laatikainen, T.; Vartiainen, E.; Koskinen, S. Measurement error as an explanation for the alcohol harm paradox: Analysis of eight cohort studies. Int. J. Epidemiol. 2020, 49, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Shen, L.; Miles, T.; Shen, Y.; Cordero, J.; Qi, Y.; Liang, L.; Li, C. Association of Low to Moderate Alcohol Drinking with Cognitive Functions from Middle to Older Age Among US Adults. JAMA Netw. Open 2020, 3, e207922. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Male | Female | |
|---|---|---|
| N = 1433 | N = 1216 | |
| Age (mean (SD)) | 44.75 (12.32) | 46.76 (12.63) |
| Age of onset (mean (SD)) | 26.37 (7.74) | 27.07 (9.00) |
| Completing matriculation examination (%) | 423 (29.5) | 474 (39.0) |
| Living with spouse (%) | 145 (10.1) | 297 (24.4) |
| Having depressive symptoms Ω (%) | 913 (63.7) | 790 (65.0) |
| Currently on psychotropic medications (%) | 1403 (97.9) | 1194 (98.2) |
| Currently on antipsychotics (%) | 1365 (95.3) | 1141 (93.8) |
| Currently on benzodiazepines (%) | 354 (24.7) | 318 (26.2) |
| Currently on antidepressant (%) | 483 (33.7) | 427 (35.1) |
| Currently on mood stabilizer (%) | 222 (15.5) | 241 (19.8) |
| On some other psychotropics/missing data (%) | 22 (1.5) | 23 (1.9) |
| Hazardous drinking PGS (mean (SD)) | 7.95 × 10−7 (9.66 × 10−7) | 7.63 × 10−7 (9.96 × 10−7) |
| Male | Female | |
|---|---|---|
| N = 196 | N = 362 | |
| Age (mean (SD)) | 41.53 | 42.72 |
| Age of onset (mean (SD)) | 29.52 | 30.01 |
| Completing matriculation examination (%) | 84 (42.9) | 167 (46.1) |
| Living with spouse (%) | 40 (20.4) | 126 (34.8) |
| Having depressive symptoms Ω (%) | 140 (71.4) | 247 (68.2) |
| Currently on psychotropic medications (%) | 190 (96.9) | 353 (97.5) |
| Currently on antipsychotics (%) | 185 (94.4) | 336 (92.8) |
| Currently on benzodiazepines (%) | 56 (28.6) | 107 (29.6) |
| Currently on antidepressant (%) | 69 (35.2) | 148 (40.9) |
| Currently on mood stabilizer (%) | 82 (41.8) | 111 (30.7) |
| On some other psychotropics/missing data (%) | 2 (1.0) | 4 (1.1) |
| Hazardous drinking PGS (mean (SD)) | 7.71 × 10−7 (10.29 × 10−7) | 7.77 × 10−7 (9.27 × 10−7) |
| Male | Female | |
|---|---|---|
| N = 419 | N = 706 | |
| Age (mean (SD)) | 45.38 (12.96) | 44.41 (12.70) |
| Age of onset (mean (SD)) | 36.78 (11.57) | 36.05 (11.51) |
| Completing matriculation examination (%) | 143 (34.1) | 324 (45.9) |
| Living with spouse (%) | 152 (36.3) | 302 (42.8) |
| Having depressive symptoms Ω (%) | 295 (70.4) | 520 (73.7) |
| Currently on psychotropic medications (%) | 397 (94.7) | 671 (95.0) |
| Currently on antipsychotics (%) | 345 (82.3) | 557 (78.9) |
| Currently on benzodiazepines (%) | 100 (23.9) | 196 (27.8) |
| Currently on antidepressant (%) | 124 (29.6) | 297 (42.1) |
| Currently on mood stabilizer (%) | 198 (47.3) | 263 (37.3) |
| On some other psychotropics/missing data (%) | 11 (2.6) | 16 (2.3) |
| Hazardous drinking PGS (mean (SD)) | 7.81 × 10−7 (9.29 × 10−7) | 8.17 × 10−7 (9.44 × 10−7) |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| RT Test | eβ (95% CI) | p-Value | R2 | eβ (95% CI) | p-Value | R2 |
| Median | ||||||
| Crude | 0.97 (0.93, 1.02) | 0.212 | 0.00 | 1.00 (0.94, 1.05) | 0.883 | 0.00 |
| Adjusted | 0.97 (0.93, 1.02) | 0.260 | 0.08 | 0.99 (0.94, 1.04) | 0.599 | 0.08 |
| SD | ||||||
| Crude | 1.00 (0.95, 1.04) | 0.856 | 0.00 | 1.00 (0.95, 1.06) | 0.931 | 0.00 |
| Adjusted | 1.00 (0.95, 1.05) | 0.968 | 0.10 | 0.99 (0.95, 1.04) | 0.685 | 0.10 |
| PAL FTMS | β (95% CI) | p-Value | R2 | β (95% CI) | p-Value | R2 |
| Crude | 0.04 (−0.02, 0.09) | 0.121 | 0.00 | −0.05 (−0.11, 0.01) | 0.089 | 0.00 |
| Adjusted | 0.04 (−0.01, 0.09) | 0.155 | 0.17 | −0.03 (−0.09, 0.02) | 0.214 | 0.18 |
| PAL TEAS | OR (95% CI) | p-Value | Cohens’ D | OR (95% CI) | p-Value | Cohens’ D |
| Crude | 1.02 (0.87–1.20) | 0.828 | 0.01 | 0.90 (0.77, 1.05) | 0.190 | 0.11 |
| Adjusted | 1.02 (0.86–1.21) | 0.829 | 0.93 (0.78, 1.11) | 0.429 |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| RT Test | eβ (95% CI) | p-Value | R2 | eβ (95% CI) | p-Value | R2 |
| Median | ||||||
| Crude | 0.94 (0.83, 1.07) | 0.356 | 0.00 | 0.93 (0.85, 1.02) | 0.117 | 0.00 |
| Adjusted | 0.93 (0.82, 1.05) | 0.228 | 0.07 | 0.94 (0.86, 1.02) | 0.129 | 0.09 |
| SD | ||||||
| Crude | 1.08 (0.94, 1.24) | 0.259 | 0.00 | 0.96 (0.88, 1.04) | 0.266 | 0.00 |
| Adjusted | 1.07 (0.94, 1.21) | 0.328 | 0.10 | 0.96 (0.89, 1.04) | 0.298 | 0.09 |
| PAL FTMS | β (95% CI) | p-Value | R2 | β (95% CI) | p-Value | R2 |
| Crude | −0.10 (−0.24, 0.04) | 0.143 | 0.01 | 0.08 (−0.03, 0.20) | 0.163 | 0.00 |
| Adjusted | −0.09 (−0.21, 0.03) | 0.155 | 0.28 | 0.06 (−0.05, 0.17) | 0.300 | 0.11 |
| PAL TEAS | OR (95% CI) | p-Value | Cohens’ D | OR (95% CI) | p-Value | Cohens’ D |
| Crude | 0.82 (0.58, 1.15) | 0.256 | 0.21 | 1.10 (0.84, 1.46) | 0.492 | 0.01 |
| Adjusted | 0.85 (0.56, 1.29) | 0.456 | 1.06 (0.79, 1.43) | 0.698 |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| RT Test | eβ (95% CI) | p-Value | R2 | eβ (95% CI) | p-Value | R2 |
| Median | ||||||
| Crude | 1.01 (0.92, 1.10) | 0.872 | 0.00 | 1.04 (0.98, 1.10) | 0.186 | 0.00 |
| Adjusted | 0.99 (0.91, 1.07) | 0.781 | 0.11 | 1.04 (0.98, 1.10) | 0.208 | 0.06 |
| SD | ||||||
| Crude | 1.00 (0.91, 1.10) | 0.981 | 0.00 | 1.02 (0.95, 1.08) | 0.649 | 0.00 |
| Adjusted | 0.99 (0.91, 1.07) | 0.745 | 0.15 | 0.99 (0.94, 1.05) | 0.773 | 0.13 |
| PAL FTMS | β (95% CI) | p-Value | R2 | β (95% CI) | p-Value | R2 |
| Crude | −0.03 (−0.15, 0.08) | 0.562 | 0.00 | −0.01 (−0.08, 0.07) | 0.820 | 0.00 |
| Adjusted | −0.02 (−0.12, 0.08) | 0.679 | 0.24 | 0.00 (−0.06, 0.07) | 0.935 | 0.17 |
| PAL TEAS | OR (95% CI) | p-Value | Cohens’ D | OR (95% CI) | p-Value | Cohens’ D |
| Crude | 0.93 (0.72, 1.21) | 0.590 | 0.10 | 0.99 (0.83, 1.19) | 0.890 | 0.01 |
| Adjusted | 0.96 (0.71, 1.28) | 0.758 | 1.01 (0.83, 1.21) | 0.956 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazumder, A.H.; Barnett, J.; Isometsä, E.T.; Lindberg, N.; Torniainen-Holm, M.; Lähteenvuo, M.; Lahdensuo, K.; Kerkelä, M.; Ahola-Olli, A.; Hietala, J.; et al. Reaction Time and Visual Memory in Connection to Hazardous Drinking Polygenic Scores in Schizophrenia, Schizoaffective Disorder and Bipolar Disorder. Brain Sci. 2021, 11, 1422. https://doi.org/10.3390/brainsci11111422
Mazumder AH, Barnett J, Isometsä ET, Lindberg N, Torniainen-Holm M, Lähteenvuo M, Lahdensuo K, Kerkelä M, Ahola-Olli A, Hietala J, et al. Reaction Time and Visual Memory in Connection to Hazardous Drinking Polygenic Scores in Schizophrenia, Schizoaffective Disorder and Bipolar Disorder. Brain Sciences. 2021; 11(11):1422. https://doi.org/10.3390/brainsci11111422
Chicago/Turabian StyleMazumder, Atiqul Haq, Jennifer Barnett, Erkki Tapio Isometsä, Nina Lindberg, Minna Torniainen-Holm, Markku Lähteenvuo, Kaisla Lahdensuo, Martta Kerkelä, Ari Ahola-Olli, Jarmo Hietala, and et al. 2021. "Reaction Time and Visual Memory in Connection to Hazardous Drinking Polygenic Scores in Schizophrenia, Schizoaffective Disorder and Bipolar Disorder" Brain Sciences 11, no. 11: 1422. https://doi.org/10.3390/brainsci11111422
APA StyleMazumder, A. H., Barnett, J., Isometsä, E. T., Lindberg, N., Torniainen-Holm, M., Lähteenvuo, M., Lahdensuo, K., Kerkelä, M., Ahola-Olli, A., Hietala, J., Kampman, O., Kieseppä, T., Jukuri, T., Häkkinen, K., Cederlöf, E., Haaki, W., Kajanne, R., Wegelius, A., Männynsalo, T., ... Veijola, J. (2021). Reaction Time and Visual Memory in Connection to Hazardous Drinking Polygenic Scores in Schizophrenia, Schizoaffective Disorder and Bipolar Disorder. Brain Sciences, 11(11), 1422. https://doi.org/10.3390/brainsci11111422