Internal Carotid Artery Injury in Transsphenoidal Surgery: Tenets for Its Avoidance and Refit—A Clinical Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
- (1)
- Injury during exposure: (a) deviation/displacement of the access trajectory relative to the midline occurred in two cases and (b) durotomy at the sella floor or in the cavernous sinus region occurred in three cases.
- (2)
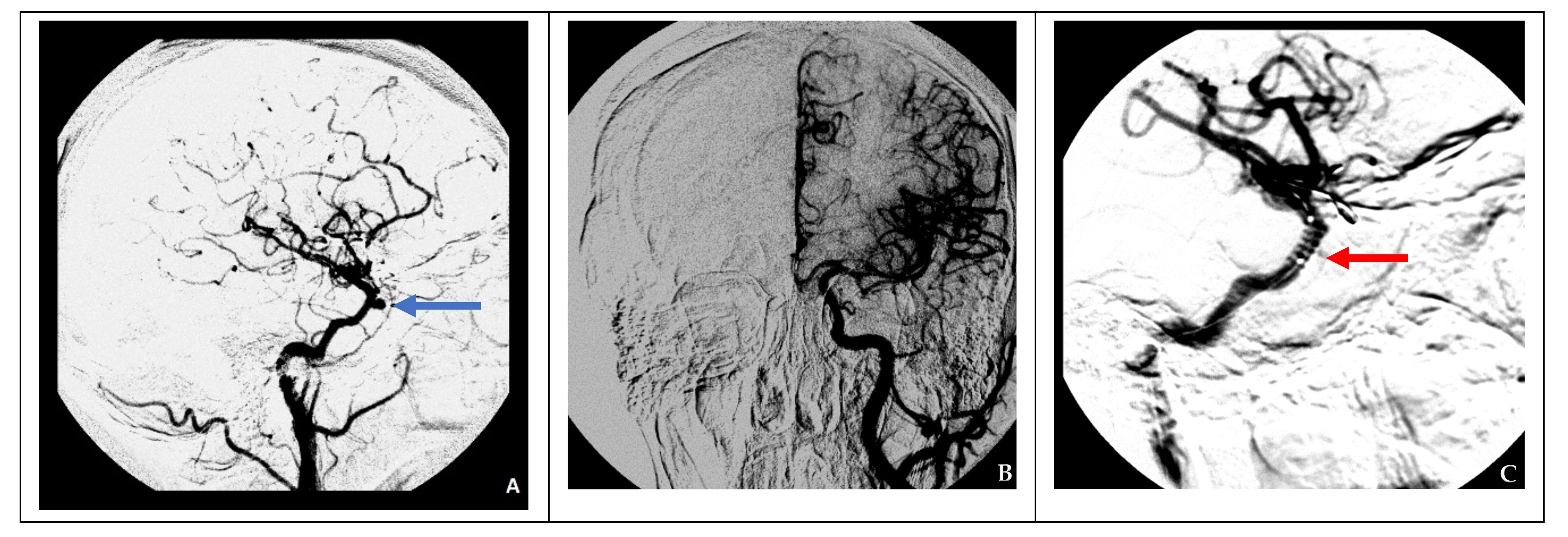
- Injury during tumor removal: Manipulations in the cavernous sinus occurred in three cases. Cerebral DSA was performed in all patients after fixing the ICA injury immediately after surgery. In six cases, a false aneurysm was revealed; in one case, a defect in the ICA wall was not detected. In one patient, ICA occlusion was observed, which was associated with either ICA spasm or excessive tamponade of the removed tumor’s cavity. In one case (no. 4), immediately after carotid artery injury, no changes were detected during angiography; however, during repeat angiography on the eighth day after surgery, a false aneurysm was detected.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kadashev, B.A.; Kutin, M.A.; Fomichev, D.V.; Kalinin, P.L.; Pfaizullaev, R.B. Extended endoscopic endonasal transsphenoidal approaches in skull base surgery. Vopr. Neirokhirurgii Im. N.N. Burdenko 2008, 4, 47–49. [Google Scholar]
- Kalinin, P.L.; Fomichev, D.V.; Kutin, M.A.; Kadashev, B.A.; Astaf’eva, L.I.; Shkarubo, A.N.; Alekseev, S.N.; Fomochkina, L.A. Endoscopic endonasal surgery of pituitary adenomas (experience of 1700 operations). Vopr. Neirokhirurgii Im. N.N. Burdenko 2012, 76, 26–33. [Google Scholar]
- Dusick, J.R.; Esposito, F.; Malkasian, D.; Kelly, D.F. Avoidance of carotid artery injuries in transsphenoidal surgery with the doppler probe and micro-hook blades. Oper. Neurosurg. 2007, 60, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Cappabianca, P.; Cavallo, L.M.; Colao, A.; de Divitiis, E. Surgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomas. J. Neurosurg. 2002, 97, 293–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassam, A.B.; Prevedello, D.M.; Carrau, R.L.; Snyderman, C.H.; Thomas, A.; Gardner, P.; Zanation, A.; Duz, B.; Stefko, S.T.; Byers, K.; et al. Endoscopic endonasal skull base surgery: Analysis of complications in the authors’ initial 800 patients. J. Neurosurg. 2011, 114, 1544–1568. [Google Scholar] [CrossRef] [PubMed]
- Mortini, P.; Losa, M.; Barzaghi, R.; Boari, N.; Giovanelli, M. Results of Transsphenoidal Surgery in a Large Series of Patients with Pituitary Adenoma. Neurosurgery 2005, 56, 1222–1233. [Google Scholar] [CrossRef] [PubMed]
- Kalinin, P.L.; Sharipov, O.I.; Shkarubo, A.N.; Fomichev, D.V.; Kutin, M.A.; Alekseev, S.N.; Kadashev, B.A.; Yakovlev, S.B.; Dorohov, E.Y.; Bukharin, E.Y.; et al. Damage to the cavernous segment of internal carotid artery in transsphenoidal endoscopic removal of pituitary adenomas (report of 4 cases). Vopr. Neirokhirurgii Im. N.N. Burdenko 2013, 77, 28–38. [Google Scholar]
- Ebner, F.H.; Kuerschner, V.; Dietz, K.; Bueltmann, E.; Naegele, T.; Honegger, J. Reduced intercarotid artery distance in acromegaly: Pathophysiologic considerations and implications for transsphenoidal surgery. Surg. Neurol. 2009, 72, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Sharipov, O.I.; Fomichev, D.V.; Kutin, M.A.; Kalinin, P.L. Intraoperative Doppler ultrasound of the cavernous part of the internal carotid artery in endoscopic transsphenoidal removal of the laterosellar tumors. Russ. J. Neurosurg. 2019, 21, 27–34. [Google Scholar] [CrossRef]
- Ciric, I.; Ragin, A.; Baumgartner, C.; Pierce, D. Complications of Transsphenoidal Surgery: Results of a National Survey, Review of the Literature, and Personal Experience. Neurosurgery 1997, 40, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Tabaee, A.; Anand, V.K.; Barrón, Y.; Hiltzik, D.H.; Brown, S.M.; Kacker, A.; Mazumdar, M.; Schwartz, T.H. Endoscopic pituitary surgery: A systematic review and meta-analysis. J. Neurosurg. 2009, 111, 545–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, P.A.; Tormenti, M.J.; Pant, H.; Fernandez-Miranda, J.C.; Snyderman, C.H.; Horowitz, M.B. Carotid Artery Injury During Endoscopic Endonasal Skull Base Surgery: Incidence and Outcomes. Oper. Neurosurg. 2013, 73, ons261–ons270. [Google Scholar] [CrossRef] [PubMed]
- Yakovlev, S.B.; Tissen, T.P.; Bocharov, A.V.; Bukharin, E.Y. Use of a stent graft in endovascular neurosurgery. Vopr. Neirokhirurgii Im. N.N. Burdenko 2006, 53–56. [Google Scholar]
- Konovalov, A.N.; Filatov, Y.M.; Tissen, T.P.; Eliava, S.S.; Yakovlev, S.B.; Pronin, I.N.; Usachev, D.Y.; Golanov, A.V.; Lukshin, V.A.; Arustamyan, S.R.; et al. Surgical treatment of cerebral vascular diseases. Zhurnal Nevrol. i Psikhiatrii im. S.S. Korsakova 2015, 115, 4. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, J.-K.; Lawton, M.T. Practice Trends in Intracranial Bypass Surgery in a 21-Year Experience. World Neurosurg. 2019, 125, e717–e722. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, C.; Li, P.; Chen, L.; Wang, Y. High-Flow Extracranial–Intracranial Bypass for Giant Cavernous Carotid Aneurysm. J. Craniofac. Surg. 2018, 29, 1042–1046. [Google Scholar] [CrossRef]
- Tantongtip, D.; Fratianni, A.; Jenkner, J.; Arnold, S.; Spetzger, U. Surgical Treatment of Inadvertent Internal Carotid Artery Lesion by Extraintracranial High-flow Bypass. A Case Report and Review of the Literature. J. Neurol. Surg. Rep. 2015, 76, e100–e104. [Google Scholar] [CrossRef] [Green Version]
- Amin-Hanjani, S. Cerebral revascularization: Extracranial-intracranial bypass. J. Neurosurg. Sci. 2011, 55, 107–116. [Google Scholar] [PubMed]
- Rangel-Castilla, L.; McDougall, C.G.; Spetzler, R.F.; Nakaji, P. Urgent Cerebral Revascularization Bypass Surgery for Iatrogenic Skull Base Internal Carotid Artery Injury. Oper. Neurosurg. 2014, 10, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J. Early neurological deterioration in acute stroke: Clinical characteristics and impact on outcome. QJM 2006, 99, 625–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age/Sex | Tumor | ICA Damage Cause | Angiography | Treatment | Outcome |
|---|---|---|---|---|---|---|
| 1 | 55 yo/F | Pituitary adenoma | Access deviation relative to the midline | ICA occlusion | Conservative therapy | Lethal |
| 2 | 61 yo/M | Pituitary adenoma | Durotomy at the bottom of the sella turcica (with medial ICA displacement) | False aneurysm | Balloon ICA occlusion at the damage site | Lethal |
| 3 | 40 yo/F | Pituitary adenoma | Access deviation relative to the midline | False aneurysm | Balloon ICA occlusion at the damage site | No complications |
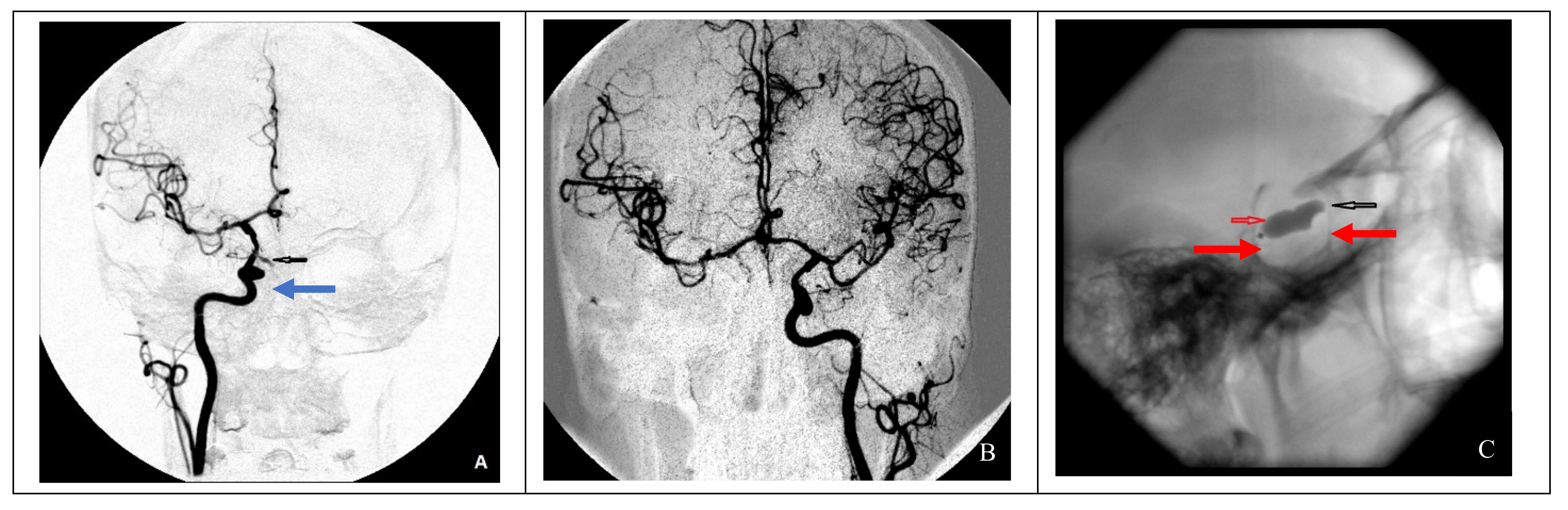
| 4 | 46 yo/M | Pituitary adenoma | Manipulation inside the cavernous sinus | False aneurysm | Installation of a stent-graft at the damage site | No complications |
| 5 | 66 yo/F | Pituitary adenoma | Manipulation inside the cavernous sinus | False aneurysm | Occlusion of ICA with micro coils at the damage site + single extra-intracranial anastomosis between the superficial temporal artery and the middle cerebral artery | Hemiparesis |
| 6 | 24 yo/F | Chordoma | Durotomy in the cavernous sinus area | ICA defect not detected | Intraoperative muscle tamponade of the defect | No complications |
| 7 | 25 yo/F | Trigeminal neuroma | Durotomy in the cavernous sinus area | False aneurysm | Occlusion of microcoils at the damage site | Transient paresis of CN VI |
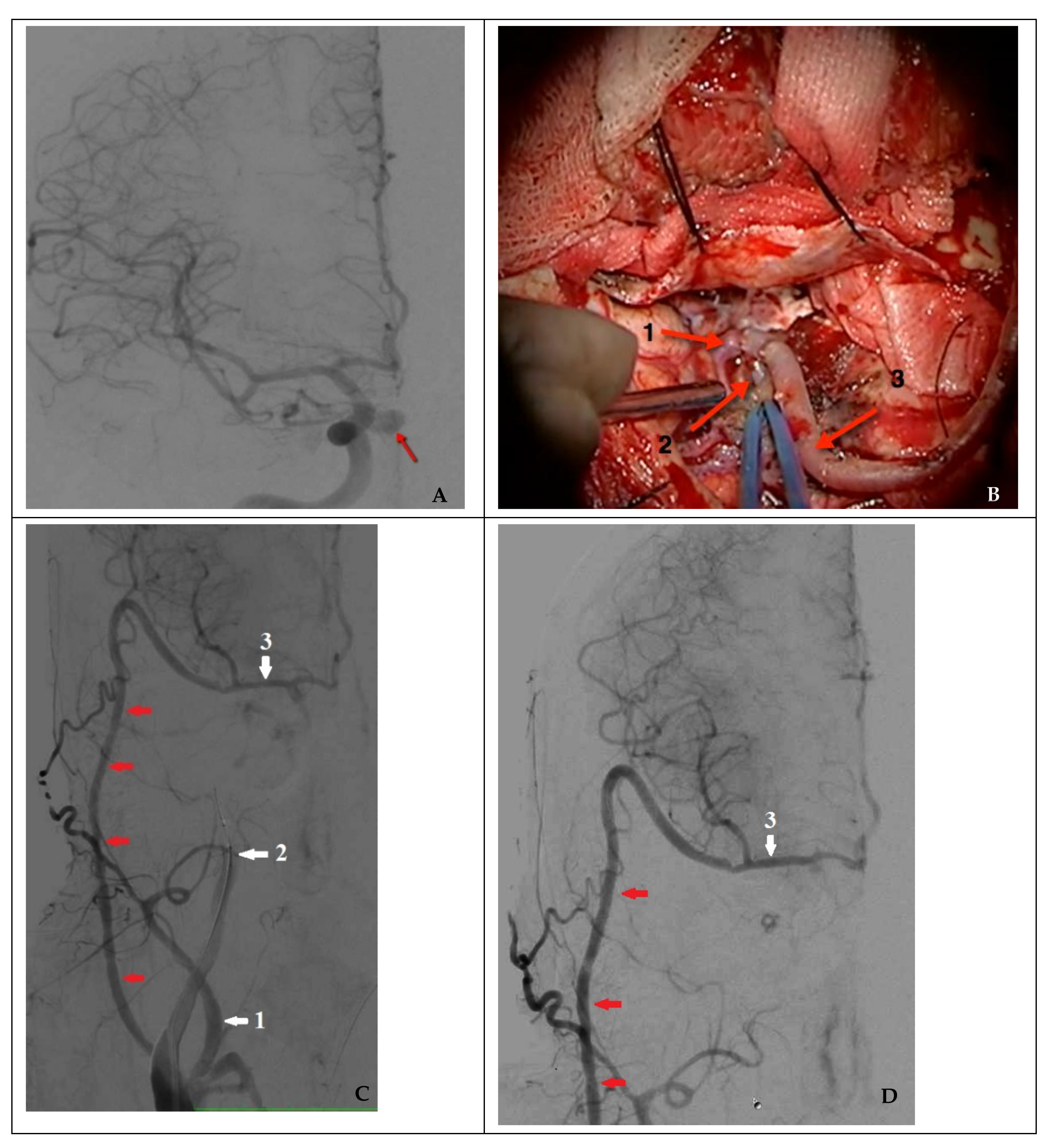
| 8 | 41 yo/M * | Pituitary adenoma | Manipulation in the region of the cavernous sinus | False aneurysm | High-flow bypass + occlusion of the ICA with microcoils at the damage site | Visual field defect, transient hemihypesthesia |
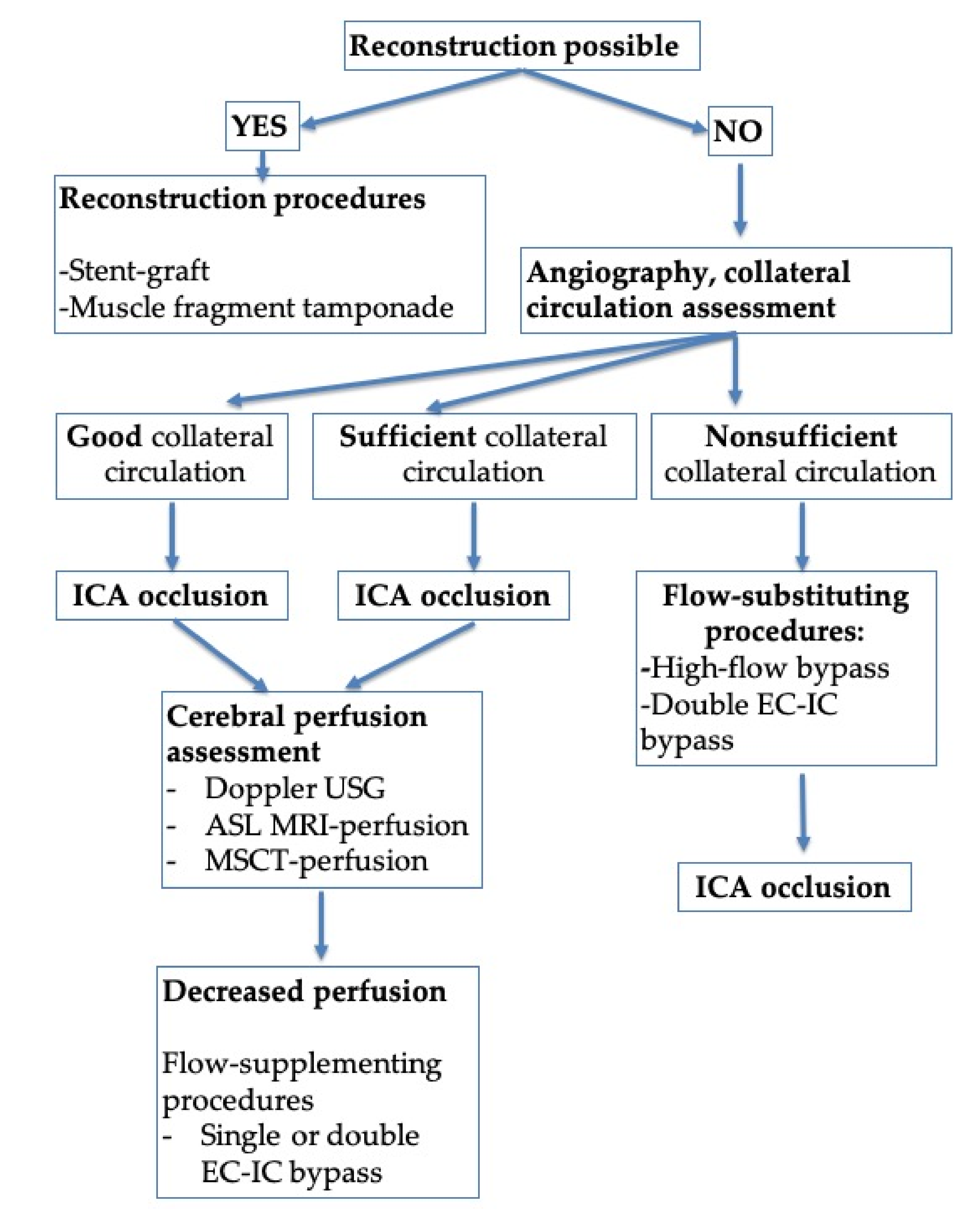
| Case | Degree of Collateral Circulation | Defect Closure Approach |
|---|---|---|
| 1 | Good | Conservative therapy |
| 2 | Good | ICA occlusion with a balloon at the site of injury |
| 3 | Good | ICA occlusion with a balloon at the site of injury |
| 4 | Nonsufficient | Stent-graft |
| 5 | Sufficient | ICA occlusion with microcoils at the site of injury + single extra-intracranial bypass (flow-supplementing surgery) |
| 6 | Good | No endovascular treatment needed |
| 7 | Good | ICA occlusion with microcoils at the site of injury |
| 8 | Nonsufficient | High-flow bypass (flow-substituting surgery) + ICA occlusion with microcoils at the site of injury. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usachev, D.; Sharipov, O.; Abdali, A.; Yakovlev, S.; Lukshin, V.; Kutin, M.; Fomichev, D.; Dorokhov, P.; Bukharin, E.; Shkarubo, A.; et al. Internal Carotid Artery Injury in Transsphenoidal Surgery: Tenets for Its Avoidance and Refit—A Clinical Study. Brain Sci. 2021, 11, 99. https://doi.org/10.3390/brainsci11010099
Usachev D, Sharipov O, Abdali A, Yakovlev S, Lukshin V, Kutin M, Fomichev D, Dorokhov P, Bukharin E, Shkarubo A, et al. Internal Carotid Artery Injury in Transsphenoidal Surgery: Tenets for Its Avoidance and Refit—A Clinical Study. Brain Sciences. 2021; 11(1):99. https://doi.org/10.3390/brainsci11010099
Chicago/Turabian StyleUsachev, Dmitry, Oleg Sharipov, Ashraf Abdali, Sergei Yakovlev, Vasiliy Lukshin, Maksim Kutin, Dmitry Fomichev, Pavel Dorokhov, Evgeny Bukharin, Alexey Shkarubo, and et al. 2021. "Internal Carotid Artery Injury in Transsphenoidal Surgery: Tenets for Its Avoidance and Refit—A Clinical Study" Brain Sciences 11, no. 1: 99. https://doi.org/10.3390/brainsci11010099
APA StyleUsachev, D., Sharipov, O., Abdali, A., Yakovlev, S., Lukshin, V., Kutin, M., Fomichev, D., Dorokhov, P., Bukharin, E., Shkarubo, A., Chernov, I., Panteleyev, A., Yağmurlu, K., Chaurasia, B., & Kalinin, P. (2021). Internal Carotid Artery Injury in Transsphenoidal Surgery: Tenets for Its Avoidance and Refit—A Clinical Study. Brain Sciences, 11(1), 99. https://doi.org/10.3390/brainsci11010099