Effectiveness of Shock Wave Therapy as a Treatment for Spasticity: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Selection of Studies
2.3. Data Extraction
2.4. Analysis of Methodological Quality
3. Results
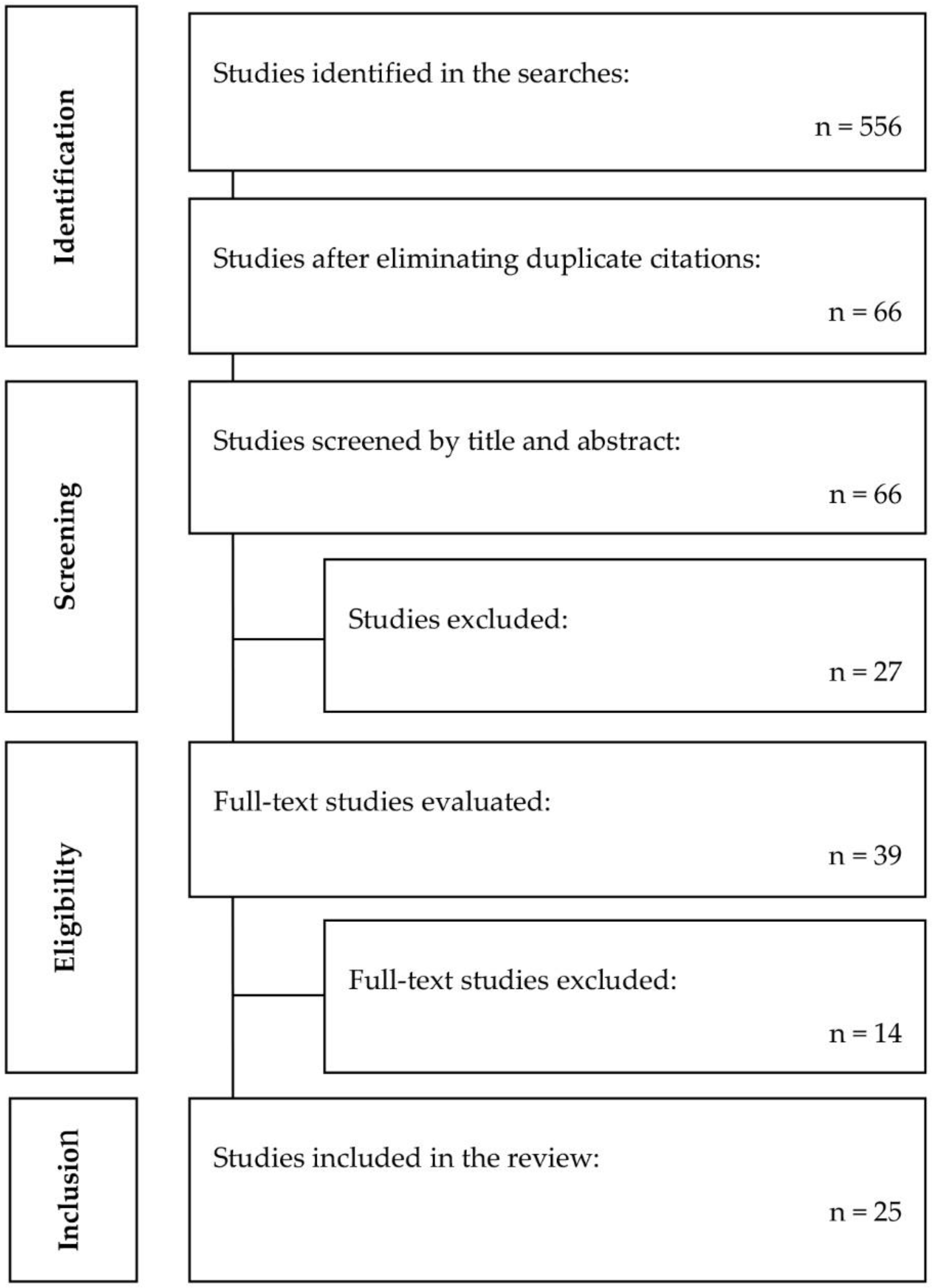
3.1. Results of the Literature Searches and Selection of Studies
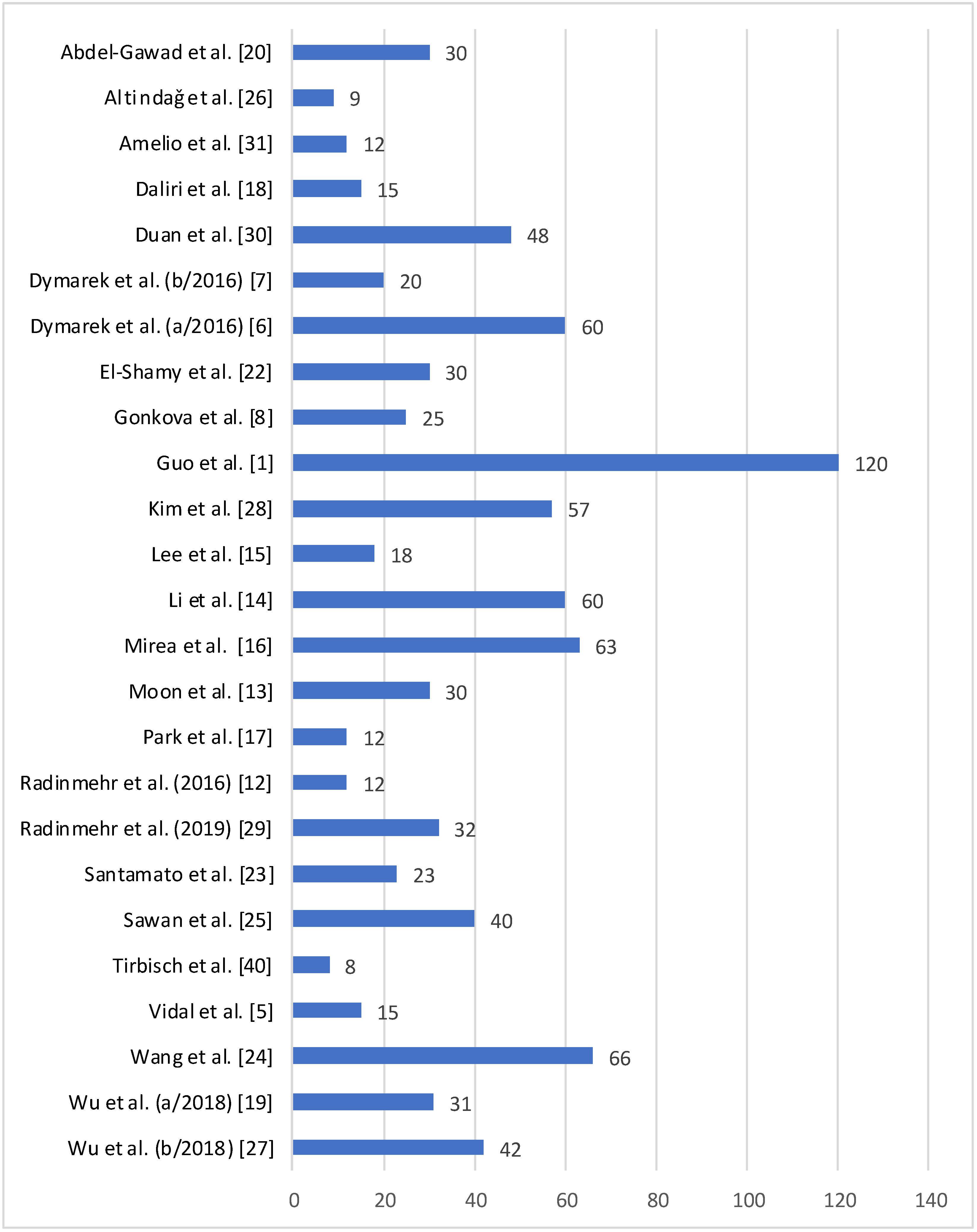
3.2. Characteristics of the Patients in the Studies Included in the Review
3.3. Characteristics of the Studies Included in the Review
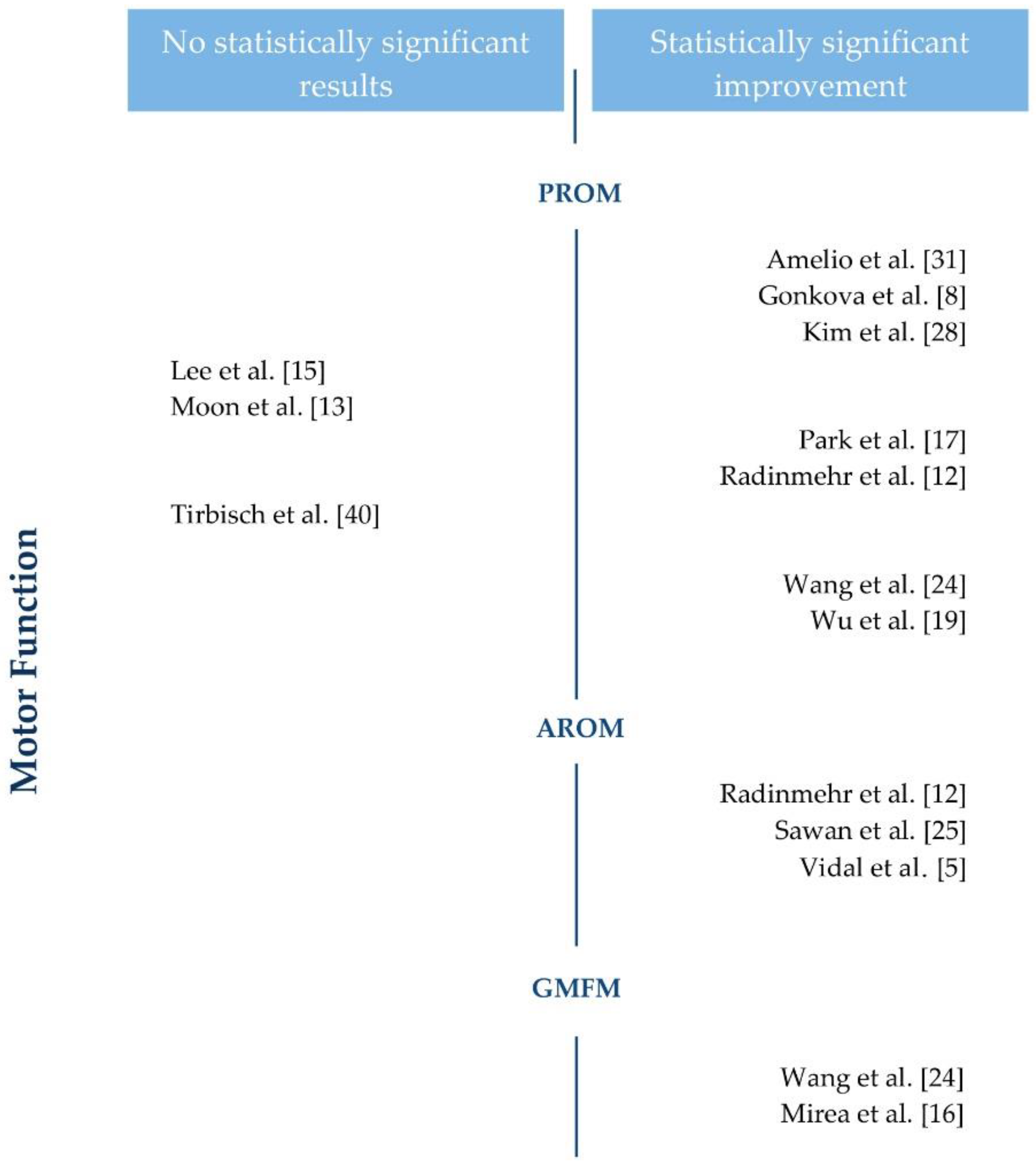
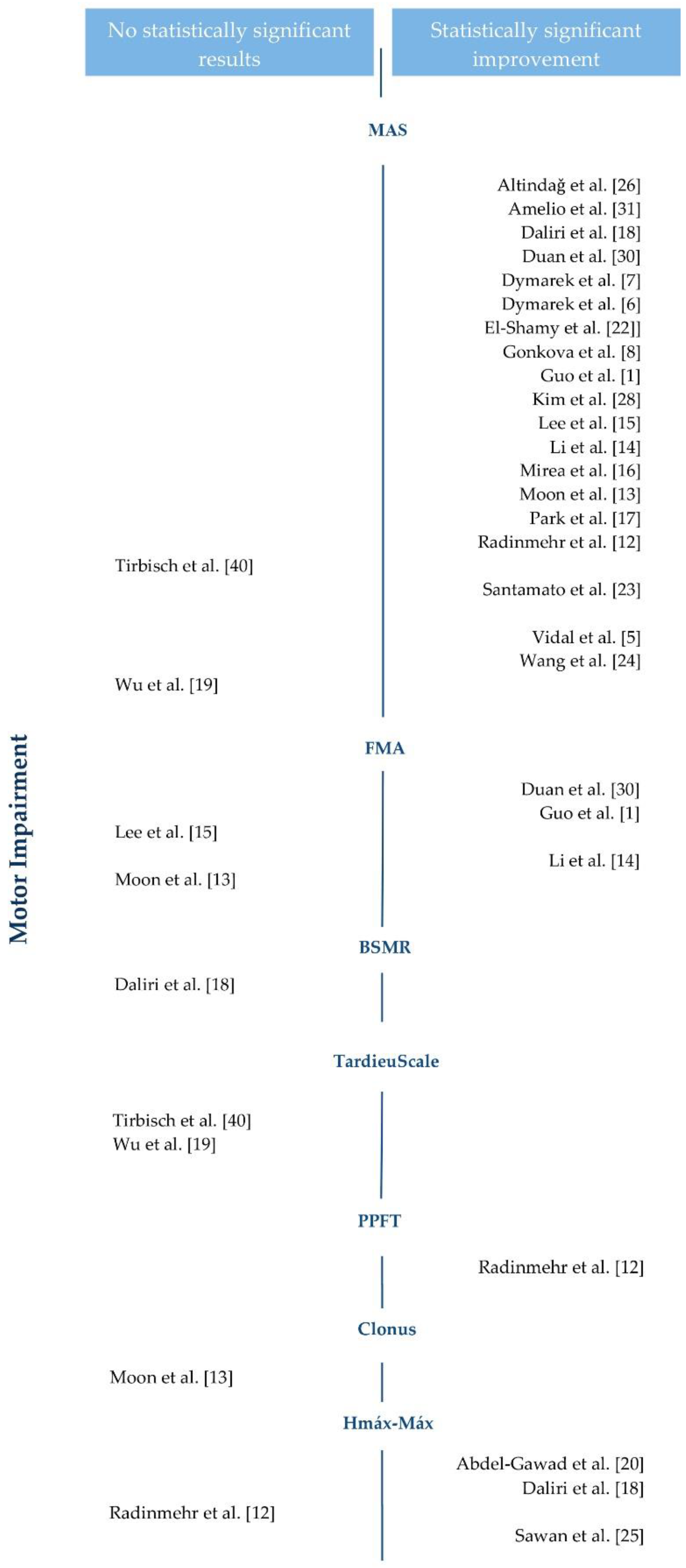
3.4. Results of the Studies Included in the Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Guo, J.; Qian, S.; Wang, Y.; Xu, A. Clinical study of combined mirror and extracorporeal shock wave therapy on upper limb spasticity in poststroke patients. Int. J. Rehabil. Res. 2019, 42, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Vivancos-Matellano, F.; Pascual-Pascual, S.I.; Nardi-Vilardaga, J.; Miquel-Rodríguez, F.; de Miguel-León, I.; Martínez-Garre, M.C.; Martínez-Caballero, I.; Lanzas-Melendo, G.; Garreta-Figuera, R.; García-Ruiz, P.J.; et al. Guía del tratamiento integral de la espasticidad. Rev. Neurol. 2007, 45, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Ashworth, N.L.; Satkunam, L.E.; Deforge, D. Treatment for spasticity in amyotrophic lateral sclerosis/motor neuron disease. Cochrane Database Syst. Rev. 2012, 15, 4156. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.G.; Young, R.R.; Koella, W.P. Spasticity: Disordered Control; Yearbook Medical: Chicago, IL, USA, 1980; pp. 485–494. [Google Scholar]
- Vidal, X.; Morral, A.; Costa, L.; Tur, M. Radial extracorporeal shock wave therapy (rESWT) in thetreatment of spasticity in cerebral palsy: A randomized, placebo-controlled clinical trial. NeuroRehabilitation 2011, 29, 413–419. [Google Scholar] [CrossRef]
- Dymarek, R.; Taradaj, J.; Rosinczuk, J. The effect of radial extracorporeal shock wave stimulation on upper limb spasticity in chronic stroke patients: A single–blind, randomized, placebo-controlled study. Ultrasound Med Biol. 2016, 42, 1862–1875. [Google Scholar] [CrossRef]
- Dymarek, R.; Taradaj, J.; Rosinczuk, J. Extracorporeal Shock Wave Stimulation as Alternative Treatment Modality for Wrist and Fingers Spasticity in Poststroke Patients: A Prospective, Open-Label, Preliminary Clinical Trial. Evid. Based Complement. Alternat. Med. 2016, 4648101. [Google Scholar] [CrossRef]
- Gonkova, M.I.; Ilieva, E.M.; Ferriero, G.; Chavdarov, I. Effect of radial shock wave therapy on muscle spasticity in children with cerebral palsy. Int. J. Rehabil. Res. 2013, 36, 284–290. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B.; Bensmail, D.; Yelnik, A. Non-pharmacological interventions for spasticity in adults: An overview of systematic reviews. Ann. Phys. Rehabil. Med. 2019, 62, 265–273. [Google Scholar] [CrossRef]
- Thompson, A.J.; Jarrett, L.; Lockley, L.; Marsden, J.; Stevenson, V.L. Clinical management of spasticity. J. Neurol. Neurosurg. Psychiatry 2005, 76, 459–463. [Google Scholar] [CrossRef]
- Xiang, J.; Wang, W.; Jiang, W.; Qian, Q. Effects of extracorporeal shock wave therapy on spasticity in post-stroke patients: A systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 2018, 50, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Radinmehr, H.; Ansari, N.N.; Naghdi, S.; Olyaei, G.; Tabatabaei, A. Effects of one session radial extracorporeal shockwave therapy on post-stroke plantar flexor spasticity: A single-blind clinical trial. Disabil. Rehabil. 2016, 39, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.W.; Kim, J.H.; Jung, M.J.; Son, S.; Lee, J.H.; Shin, H.; Lee, E.S.; Yoon, C.H.; Oh, M.K. The Effect of Extracorporeal Shock Wave Therapy on Lower Limb Spasticity in Subacute Stroke Patients. Ann. Rehabil. Med. 2013, 37, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Li, T.Y.; Chang, C.Y.; Chou, Y.C.; Chen, L.C.; Chu, H.Y.; Chiang, S.L.; Wu, Y.T. Effect of radial shock wave therapy on spasticity of the upper limb in patients with chronic stroke. Medicine (Baltimore) 2016, 95, e3544. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Lee, S.U.; Lee, S.H.; Yoo, J.I. Ultrasonographic evaluation for the effect of extracorporeal shock wave therapy on gastrocnemius muscle spasticity in patient with chronic stroke. PM R. 2019, 11, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Mirea, A.; Onose, G.; Padure, L.; Rosulescu, E. Extracorporeal Shockwave Therapy (ESWT) benefits in spastic children with Cerebral Palsy (CP). J. Med. Life 2014, 7, 127–132. [Google Scholar]
- Park, D.S.; Kwon, D.R.; Park, G.Y.; Lee, M.Y. Therapeutic effect of extracorporeal shock wave therapy according to treatment session on gastrocnemius muscle spasticity in children with spastic cerebral palsy: A pilot study. Ann. Rehabil. Med. 2015, 39, 914–921. [Google Scholar] [CrossRef]
- Daliri, S.S.; Forogh, B.; Razavi, S.Z.E.; Ahadi, T.; Madjlesi, F.; Ansari, N.N. A single blind, clinical trial to investigate the effects of a single sesión extracorporeal shock wave therapy on wrist flexor spasticity after stroke. NeuroRehabilitation 2015, 36, 67–72. [Google Scholar] [CrossRef]
- Wu, Y.T.; Chang, C.N.; Chen, Y.M.; Hu, G.C. Comparison of the effect of focused and radial extracorporeal shock waves on spastic equinus in patients with stroke: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 518–525. [Google Scholar]
- AbdelGawad, H.A.; Karim, A.E.A.; Mohammed, A.H. Shock wave therapy for spastic plantar flexor muscles in hemiplegic cerebral palsy children. Egypt. J. Med. Hum. Genet. 2015, 16, 269–275. [Google Scholar] [CrossRef]
- Picelli, A.; Santamato, A.; Chemello, E.; Cinone, N.; Cisari, C.; Gandolfi, M.; Ranieri, M.; Smania, N.; Baricich, A. Adjuvant treatments associated with botulinum toxin injection for managing spasticity: An overview of the literatura. Ann. Phys. Rehabil. Med. 2019, 62, 291–296. [Google Scholar] [CrossRef]
- El-shamy, S.M.; Eid, M.A.; El-banna, M.F. Effect of extracorporeal shock wave therapy on gait pattern in hemiplegic cerebral palsy: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2014, 93, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Santamato, A.; Francesca Micello, M.; Panza, F.; Fortunato, F.; Logroscino, G.; Picelli, A.; Manganotti, P.; Smania, N.; Fiore, P.; Ranieri, M. Extracorporeal Shock Wave Therapy for theTreatment of Poststroke Plantar-Flexor Muscles Spasticity: A Prospective Open-Label Study. Top. Stroke Rehabil. 2014, 21, S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Du, L.; Shan, L.; Dong, H.; Feng, J.; Kiessling, M.C.; Angstman, N.B.; Schmitz, C.; Jia, F. A prospective case-control study of radial extracorporeal shock wave therapy for spastic plantar flexor muscles in very young children with cerebral palsy. Medicine (Baltimore) 2016, 95, e3649. [Google Scholar] [CrossRef] [PubMed]
- Sawan, S.; Abd-Allah, F.; Hegazy, M.M.; Farrag, M.A.; El-Den, N.H.S. Effect of shock wave therapy on ankle planter flexors spasticity in stroke patients. NeuroRehabilitation 2017, 40, 115–118. [Google Scholar] [CrossRef]
- Altindaǧ, Ö.; Gursoy, S. Effect of Shock Wave Therapy on Spasticity: A Single- Institution Experience. Turk. J. Phys. Med. Rehabil. 2014, 60, 95–96. [Google Scholar] [CrossRef]
- Wu, Y.T.; Yu, H.K.; Chen, L.R.; Chang, C.N.; Chen, Y.M.; Hu, G.C. Extracorporeal Shock Waves Versus Botulinum Toxin Type A in the Treatment of Poststroke Upper Limb Spasticity: A Randomized Noninferiority Trial. Arch. Phys. Med. Rehabil. 2018, 99, 2143–2150. [Google Scholar] [CrossRef]
- Kim, Y.W.; Shin, J.C.; Yoon, J.G.; Kim, Y.K.; Lee, S.C. Usefulness of radial extracorporeal shock wave therapy for the spasticity of the subscapularis in patients with stroke: A pilot study. Chin. Med. J. (Engl.) 2013, 126, 4638–4643. [Google Scholar]
- Radinmehr, H.; Ansari, N.N.; Naghdi, S.; Tabatabei, A.; Moghim, I.E. Comparison of Therapeutic Ultrasound and Radial Shock Wave Therapy in the Treatment of Plantar Flexor Spasticity After Stroke: A Prospective, Single-blind, Randomized Clinical Trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1546–1554. [Google Scholar] [CrossRef]
- Duan, H.; Li, Z.; Xu, G.; Liu, F.; Yan, Z. Efficacy of extracorporeal shock wave in treatment of spasticity of bíceps brachii in stroke patients. J. Jilin Univ. Med. 2017, 43, 151–154. [Google Scholar]
- Amelio, E.; Manganotti, P. Effect of shock wave stimulation on hypertonic plantar flexor muscles in patients with cerebral palsy: A placebo-controlled study. J. Rehabil. Med. 2010, 42, 339–343. [Google Scholar] [CrossRef]
- Dymarek, R.; Ptaszkowski, K.; Słupska, L.; Halski, T.; Taradaj, J.; Rosińczuk, J. Effects of extracorporeal shock wave on upper and lower limb spasticity in post-stroke patients: A narrative review. Top. Stroke Rehabil. 2016, 23, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Gao, F.; Zhao, T.; Sun, W.; Wang, B.; Li, Z. Positive Effects of Extracorporeal Shock Wave Therapy on Spasticity in Poststroke Patients: A Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 2470–2476. [Google Scholar] [CrossRef] [PubMed]
- Cabanas-Valdés, R.; Serra-Llobet, P.; Rodriguez-Rubio, P.R.; López-de–Celis, C.; Llauró-Fores, M.; Calvo-Sanz, J. The effectiveness of extracorporeal shock wave therapy for improving upper limb spasticity and functionality in stroke patients: A systematic review and meta-analysis. Clin. Rehabil. 2019, 34, 1141–1156. [Google Scholar] [CrossRef] [PubMed]
- Corrado, B.; Di Luise, C.; Servodio Iammarrone, C. Management of Muscle Spasticity in Children with Cerebral Palsy by Means of Extracorporeal Shockwave Therapy: A Systematic Review of the Literature. Dev. Neurorehabil. 2019, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Handbook for Systematic reviews of Interventions; Prisma. Version 5.1.0 [updatedMarch 2011]; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blind ing necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Murad, H.M.; Asi, N.; Alsawas, M.; Alahdab, F. New evidence pyramid. Evid. Based Med. 2016, 21, 125–127. [Google Scholar] [CrossRef]
- National Heart Lung and Blood Institute. Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group. 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 October 2020).
- Tirbisch, L. Effets des ondes de choc radiales sur la spasticité du triceps sural de patients hémiplégiques en phase subaiguë: Un essai contrôlé randomisé. Kinesither. Revue 2015, 15, 62–69. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, S.N.; Lee, I.S.; Jung, H.; Lee, K.S.; Koh, S.E. Effects of extracorporeal shock wave therapy on spasticity in patients after brain injury: A meta-analysis. J. Phys. Ther. Sci. 2014, 26, 1641–1647. [Google Scholar] [CrossRef]
- Branco Mills, P.; Finlayson, H.; Sudol, M.; O’Connor, R. Systematic review of adjunct therapies to improve outcomes following botulinum toxin injection for treatment of limb spasticity. Clin. Rehabil. 2015, 30, 537–548. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year | Study Design | Participants | Intervention | Comparative | Outcomes Variable (Tool) |
| AbdelGawad et al. (2015) [20] | Randomized Controlled Trial | Dx: CP Age (mean ± standard deviation years): (I) 5.75 ± 0.51 (C) 5.83 ± 0.34 Sex: 60% F, 40% M Inclusion criteria: No BTA, MAS 1-2, standing | n = 15 Shock wave therapy and conventional rehabilitation programme | n = 15 conventional rehabilitation programme | Motor impairment (Hmax–Mmax) Functional independence (gait analysis) |
| Altindaǧ et al. (2014) [26] | Case series | Dx: Stroke, CP, SPI Age (years): 36.6 ± 23.37 Sex: 44% F, 56% M Inclusion criteria: no BTA, MAS > 2 | n = 9 Shock wave therapy and conventional rehabilitation programme | Motor impairment (MAS) | |
| Amelio et al. (2010) [31] | Quasi-experimental pre-post | Dx: CP Age (years): 5.83 ± 2.31 Sex: 50% F, 50% M Inclusion criteria: no BTA, gait | n = 12 1st session placebo and 2nd session shock wave therapy | Motor Function (PROM) Motor impairment (MAS) Functional independence (podobarometry) | |
| Daliri et al. (2015) [18] | Quasi-experimental pre-post | Dx: Stroke Age (years): 54.4 ± 9.4 Sex: 20% F, 80% M Inclusion criteria: no BTA, Stroke > 6 months | n = 15 1st session placebo and 2nd session shock wave therapy | Motor impairment (MAS, BMRS, Hmax-Mmax) | |
| Duan et al. (2016) [30] | Randomized Controlled Trial | Dx: Stroke Age (years) (I) 48.29 ± 12.30 (C) 50.67 ± 14.27 Sex: 48% F, 52% M Inclusion criteria: no BTA | n = 24 Shock wave therapy and conventional rehabilitation programme | n = 24 conventional rehabilitation programme | Motor impairment (MAS, FMA) |
| Dymarek et al. (b/2016) [7] | Quasi-experimental pre-post | Dx: Stroke Age (years): 63.15 ± 12.60 Sex: 65% F, 35% M Inclusion criteria: no BTA, MAS > 1+, Stroke > 9 months | n = 20 Shock wave therapy | Motor impairment (MAS) Electrodiagnostic (EMG, IRT) | |
| Dymarek et al. (a/2016) [6] | Randomized Controlled Trial | Dx: Stroke Age (years) (I) 61.43 ± 12.74 (C) 60.87 ± 9.51 Sex: 43% F, 57% M Inclusion criteria: no BTA, MAS > 1+, Stroke > 9 months | n = 30 Shock wave therapy | n = 30 Placebo | Motor impairment (MAS) Electrodiagnostic (EMG, IRT) |
| El-Shamy et al. (2014) [22] | Randomized Controlled Trial | Dx: CP Age (years) (I) 6.93 ± 0.8 (C) 6.8 ± 0.77 Sex: 40% F, 60% M Inclusion criteria: No BTA, independent gait | n = 15 Shock wave therapy and conventional rehabilitation programme | n = 15 conventional rehabilitation programme | Motor impairment (MAS) Functional independence (gait analysis) |
| Gonkova et al. (2013) [8] | Quasi-experimental pre-post | Dx: CP Age (years): 4.84 ± 3.11 Sex: 36% F, 64% M Inclusion criteria: no BTA | n = 25 1st session placebo and 2nd session radial shock wave therapy | Motor Function (PROM) Motor impairment (MAS) Functional independence (podobarometry) | |
| Guo et al. (2019) [1] | Randomized Controlled Trial | Dx: Stroke Age (years) (I–A) 66.79 ± 11.02 (I–B) 67.15 ± 11.23 (I–C) 68.72.0 ± 10.56 (C) 69.72 ± 11.13 Sex: 44% F, 56% M Inclusion criteria: no BTA, MAS > 1, <4, Stroke > 6 months | Group A: n = 30 Shock wave therapy and conventional rehabilitation programme Group B: n = 30 Mirror therapy and conventional rehabilitation programme Group C: n = 30 Mirror therapy, shock wave and conventional rehabilitation programme | n = 30 conventional rehabilitation programme | Motor impairment (MAS, FMA) |
| Kim et al. (2013) [28] | Quasi-experimental pre-post | Dx: stroke Age (years): 55.4 ± 13.2 Sex: 42% F, 58% M Inclusion criteria: no BTA, MAS > 1, Stroke > 9 months | n = 57 Radial shock wave therapy and conventional rehabilitation programme | Motor function (PROM) Motor impairment (MAS) Pain (VAS) | |
| Lee et al. (2019) [15] | Randomized Controlled Trial | Dx: stroke Age (years): (I) 50.89 ± 8.81 (C) 44.11 ± 4.07 Sex: 11% F, 89% M Inclusion criteria: No BTA | n = 9 Radial shock wave therapy | n = 9 Placebo | Motor function (PROM) Motor impairment (MAS, FMA) Electrodiagnostic (echography) |
| Li et al. (2016) [14] | Randomized Controlled Trial | Dx: stroke Age (years): (I–A) 55.35 ± 3.05 (I–B) 56.80 ± 3.00 (C) 55.95 ± 2.64 Sex: 31% F, 69% M Inclusion criteria: no BTA, MAS > 1, Stroke > 9 months | Group A: n = 20 3 sessions of radial shock wave therapy Group B: n = 20 1 session of shock wave therapy | n = 20 Placebo | Motor impairment (MAS, FMA) |
| Mirea et al. (2014) [16] | Quasi-experimental pre-post | Dx: CP Age (months): 99.57 ± 53.74 Sex: 41% F, 59% M Inclusion criteria: no BTA, MAS 1−3 | n = 63 Shock wave therapy | Motor function (GMFM) Motor impairment (MAS) Pain (QPS) | |
| Moon et al. (2013) [13] | Quasi-experimental pre-post | Dx: stroke Age (years): 52.6 ± 14.9 Sex: 43% F, 57% M Inclusion criteria: no BTA, MAS > 1+, Stroke > 1 month. | n = 30 1 placebo session and 3 sessions of shock wave therapy | Motor function (PROM) Motor impairment (MAS, FMA, clonus) Functional independence (dynamometric isocentric parameters) | |
| Park et al. (2015) [17] | Randomized Controlled Trial | Dx: CP Age (years): (I) 7.0 ± 3.1 (C) 6.8 ± 2.3 Sex: 41% F, 59% M Inclusion criteria: no BTA, gait | n = 6 3 sessions of shock wave therapy and conventional rehabilitation programme | n = 6 1 shock wave session and 2 placebo sessions and conventional rehabilitation programme | Motor function (PROM) Motor impairment (MAS) |
| Radinmehr et al. (2016) [12] | Randomized Controlled Trial | Dx: stroke Age (years): 59 ± 13 Sex: 41% F, 59% M Inclusion criteria: no BTA, independent gait, MAS > 1, Stroke > 1 month | n = 12 Radial shock wave therapy | Motor function (PROM, AROM) Motor impairment (MAS, PPFT, Hmax–Mmax) Functional independence (TUG) | |
| Radinmehr et al. (2019) [29] | Randomized Controlled Trial | Dx: stroke Age (years): (I) 56.0 ± 12.3 (C) 56.2 ± 8.4 Sex: 40% F, 60% M Inclusion criteria: no BTA, gait, MAS > 1, Stroke > 1 month | n = 16 Radial shock wave therapy | n = 16 Ultrasounds | Motor function (PROM, AROM) Motor impairment (MAS, PPFT, Hmax–Mmax) Functional independence (TUG) |
| Santamato et al. (2014) [23] | Quasi-experimental pre-post | Dx: stroke Age (years): 57.6 ± 10.8 Sex: 34% F, 66% M Inclusion criteria: no BTA, MAS > 1 <4 | n = 23 Shock wave therapy | Motor impairment (MAS) | |
| Sawan et al. (2017) [25] | Quasi experimental | Dx: stroke Age (years): (I) 50.6 ± 6.7 (C) 84.8 ± 5.9 Inclusion criteria: no BTA, MAS 1−2 | n = 20 Shock wave therapy and conventional rehabilitation programme | n = 20 Placebo and conventional rehabilitation programme | Motor function (AROM) Motor impairment (Hmax–Mmax) Functional independence (Timed 10 m walk test) |
| Tirbisch et al. (2015) [40] | Randomized Controlled Trial | Dx: stroke Inclusion criteria: no BTA, MAS > 1+ | n = 4 Radial shock wave therapy and conventional rehabilitation programme | n = 4 conventional rehabilitation programme | Motor function (PROM) Motor impairment (MAS, Tardieu Scale) |
| Vidal et al. (2011) [5] | Randomized Controlled Trial | Dx: CP Age (years): 31 Sex: 20% F, 80% M Inclusion criteria: no BTA | n = 5 Radial shock wave therapy on spastic agonists. n = 5 Radial shock wave therapy on spastic agonists and antagonists | n = 5 Placebo | Motor function (AROM) Motor impairment (MAS) |
| Wang et al. (2016) [24] | Case-control | Dx: CP Age (months): (I) 26.9 ± 13.1 (C) 27.0 ± 14.2 Sex: 33% F, 67% M Inclusion criteria: no BTA, MAS 1−4 | n = 34 Shock wave therapy and conventional rehabilitation programme | n = 32 Conventional rehabilitation programme | Motor function (PROM, GMFM) Motor impairment (MAS) |
| Wu et al. (a/2018) [19] | Randomized Controlled Trial | Dx: stroke Age (years): (I) 59.6 ± 11.3 (C) 60.3 ± 9.9 Sex: 41% F, 59% M Inclusion criteria: no BTA, gait, MAS 1-4, Stroke > 6 months | n = 16 Radial shock wave therapy | n = 15 Focused shock wave therapy | Motor function (PROM) Motor impairment (MAS, Tardieu Scale) Functional independence (Timed 10 m walk test, plantar contact area) |
| Wu et al. (b/2018) [27] | Randomized Controlled Trial | Dx: stroke Age (years): (I) 60.0 ± 11.1 (C) 62.0 ± 10.2 Sex: 33% F, 67% M Inclusion criteria: no BTA, Stroke > 6 months | n = 21 Shock wave therapy | n = 21 BTA | Motor function (PROM) Motor impairment (MAS, FMA) |
| Authors | Type of Shock Waves | Number of Sessions | Treatment Time | Number of Shots | Energy | Frequency | Anatomic Area |
| AbdelGawad et al. [20] | Not specified | 3 | 1 week | 2100 | 0.32 mJ/mm2 | Soleus and gastrocnemius | |
| Altindaǧ et al. [26] | Not specified | 3 | 2 weeks | 2000 | 0.1 mJ/mm2 2 bar | Soleus and gastrocnemius | |
| Amelio et al. [31] | Not specified | 1 | 8 weeks | 1500 | 0.03 mJ/mm2 1.5 bar | Soleus and gastrocnemius | |
| Daliri et al. [18] | Not specified | 1 | 2 weeks | 1500 | 0.03 mJ/mm2 1.5 bar | Flexor carpi radialis and flexor carpi ulnaris | |
| Duan et al. [30] | Not specified | 1 week | Biceps brachii | ||||
| Dymarek et al. (b/2016) [7] | Not specified | 1 | 1 week | 1500 | 0.03 mJ/mm2 1.5 bar | 4 Hz | Flexor carpi radialis and flexor carpi ulnaris |
| Dymarek R et al. (a/2016) [6] | Not specified | 1 | 1 week | 1500 | 0.03 mJ/mm2 1.5 bar | 5 Hz | Flexor carpi radialis and flexor carpi ulnaris |
| El-Shamy et al. [22] | Not specified | 12 | 3 months | 1500 | 0.03 mJ/mm2 1.5 bar | 5 Hz | Soleus and gastrocnemius |
| Gonkova et al. [8] | Radials | 1 | 5 weeks | 1500 | 0.03 mJ/mm2 1.5 bar | 5 Hz | Soleus and gastrocnemius |
| Guo et al. [1] | Not specified | 20 | 4 weeks | 2000 | 2–3 bar | 8 Hz | Intrinsic and flexor digitorum |
| Kim et al. [28] | Radials | 5 | 2 weeks | 3000 | 0.63 mJ/mm2 1.6 bar | 8 Hz | Subscapularis |
| Lee et al. [15] | Radials | 1 | 1 week | 2000 | 0.1 mJ/mm2 2 bar | 4 Hz | Soleus and gastrocnemius |
| Li et al. [14] | Radials | 3 | 3 weeks | 1500 4000 | 3.5 bar 3 bar | 5 Hz 5 Hz | Flexor carpi radialis and flexor carpi ulnaris, intrinsic and flexor digitorum |
| Mirea et al. [16] | Not specified | 3 | 3 weeks | 500 | 0.15 mJ/mm2 1.5 bar | 10 Hz | Soleus and gastrocnemius, biceps brachii, Flexor carpi radialis and flexor carpi ulnaris |
| Moon et al. [13] | Not specified | 3 | 4 weeks | 1500 | 0.089 mJ/mm2 | 4 Hz | Soleus and gastrocnemius |
| Park et al. [17] | Not specified | 1/3 | 1 week | 1500 | 0.03 mJ/mm2 2.5 bar | 4 Hz | Soleus and gastrocnemius |
| Radinmehr et al. (2016) [12] | Radials | 1 | 1 week | 2000 | 0.34 mJ/mm2 1 bar | 5 Hz | Soleus and gastrocnemius |
| Radinmehr et al. (2019) [29] | Radials | 1 | 1 week | 2000 | 0.34 mJ/mm2 1 bar | 5 Hz | Soleus and gastrocnemius |
| Santamato et al. [23] | Not specified | 1 | 1 week | 1500 | 0.1 mJ/mm2 2 bar | Soleus and gastrocnemius | |
| Sawan et al. [25] | Not specified | 6 | 6 weeks | 1500 | 0.34 mJ/mm2 1 bar | 5 Hz | Soleus and gastrocnemius |
| Tirbisch et al. [40] | Radials | 9 | 3 weeks | 0.03 mJ/mm2 | 10 Hz | Soleus and gastrocnemius | |
| Vidal et al. [5] | Radials | 3 | 1 week | 4000 | 0.10 mJ/mm2 2 bar | 8 Hz | Agonists and antagonists |
| Wang et al. [24] | Radials | 12 | 3 months | 3000 | 0.03 mJ/mm2 0.6 bar | 8 Hz | Soleus and gastrocnemius |
| Wu et al. (a/2018) [19] | Radials Focused | 3 3 | 1 week 1 week | 3000 3000 | 2 bar 0.10 mJ/mm2 | 5 Hz 5 Hz | Soleus and gastrocnemius Soleus and gastrocnemius |
| Wu YT et al. (b/2018) [27] | Not specified | 3 | 1 week | 3000 | 3.5 bar | 5Hz | Flexor carpi radialis and flexor carpi ulnaris and biceps brachii. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez, I.M.; Sempere-Rubio, N.; Navarro, O.; Faubel, R. Effectiveness of Shock Wave Therapy as a Treatment for Spasticity: A Systematic Review. Brain Sci. 2021, 11, 15. https://doi.org/10.3390/brainsci11010015
Martínez IM, Sempere-Rubio N, Navarro O, Faubel R. Effectiveness of Shock Wave Therapy as a Treatment for Spasticity: A Systematic Review. Brain Sciences. 2021; 11(1):15. https://doi.org/10.3390/brainsci11010015
Chicago/Turabian StyleMartínez, Isabel María, Nuria Sempere-Rubio, Olga Navarro, and Raquel Faubel. 2021. "Effectiveness of Shock Wave Therapy as a Treatment for Spasticity: A Systematic Review" Brain Sciences 11, no. 1: 15. https://doi.org/10.3390/brainsci11010015
APA StyleMartínez, I. M., Sempere-Rubio, N., Navarro, O., & Faubel, R. (2021). Effectiveness of Shock Wave Therapy as a Treatment for Spasticity: A Systematic Review. Brain Sciences, 11(1), 15. https://doi.org/10.3390/brainsci11010015