Systematic Review of Level 1 and Level 2 Screening Tools for Autism Spectrum Disorders in Toddlers




Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Overview of the Studies and Measures
3.2. Overview of the Studies and Measures
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Press: Washington, DC, USA, 2013. [Google Scholar]
- Christensen, D.L.; Maenner, M.J.; Bilder, D.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M.; Pettygrove, S.D.; Robinson, C.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 4 Years—Early Autism and Developmental Disabilities Monitoring Network, Seven Sites, United States, 2010, 2012, and 2014. MMWR Surveill. Summ. 2019, 68, 1–19. [Google Scholar]
- Christensen, D.L.; Braun, K.V.N.; Baio, J.; Bilder, D.; Charles, J.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M.; et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveill. Summ. 2018, 65, 1. [Google Scholar]
- Filipek, P.A.; Accardo, P.J.; Ashwal, S.; Baranek, G.T.; Cook, E.H.; Dawson, G.; Gordon, J.S.; Gravel, C.P.; Johnson, R.J.; Kallen, S.E.; et al. Practice parameter: Screening and diagnosis of autism: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Child Neurology Society. Neurology 2000, 55, 468–479. [Google Scholar] [PubMed]
- Marchetti, A.; Castelli, I.; Cavalli, G.; Di Terlizzi, E.; Lecciso, F.; Lucchini, B.; Massaro, D.; Petrocchi, S.; Valle, A. Theory of Mind in typical and atypical developmental settings: Some considerations from a contextual perspective. In Reflective Thinking in Educational Settings: A Cultural Frame Work; Antonietti, A., Confalonieri, E., Eds.; Cambridge University Press: Cambridge, UK, 2014; pp. 102–136. [Google Scholar]
- Falkmer, T.; Anderson, K.; Falkmer, M.; Horlin, C. Diagnostic procedures in autism spectrum disorders: A systematic literature review. Eur. Child Adolesc. Psychiatry 2013, 22, 329–340. [Google Scholar] [PubMed]
- Volkmar, F.; Siegel, M.; Woodbury-Smith, M.; King, B.; McCracken, J.; State, M. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 237–257. [Google Scholar] [PubMed]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. JADD 1994, 24, 659–685. [Google Scholar]
- Lord, C.; Luyster, R.J.; Gotham, K.; Guthrie, W. Autistic Diagnosis Observation Scale 2 Manual; Hogrefe: Florence, Italy, 2013. [Google Scholar]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef]
- Perry, A.; Cummings, A.; Geier, J.D.; Freeman, N.L.; Hughes, S.; LaRose, L.; Managhan, T.; Reitzel, J.A.; Williams, J. Effectiveness of intensive behavioral intervention in a large, community-based program. Res. Autism Spectr. Disord. 2008, 2, 621–642. [Google Scholar] [CrossRef]
- Sallows, G.O.; Graupner, T.D. Intensive behavioral treatment for children with autism: Four-year outcome and predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef]
- Leo, M.; Carcagnì, P.; Del Coco, M.; Spagnolo, P.; Mazzeo, P.L.; Celeste, G.; Distante, C.; Lecciso, F.; Levante, A.; Rosato, A.C.; et al. Towards the Automatic Assessment of Abilities to produce Facial Expressions: The case study of children with ASD. In Proceedings of the 20th Italian National Conference on Photonic Technologies, Lecce, Italy, 23–25 May 2018; p. 4. [Google Scholar]
- Leo, M.; Carcagnì, P.; Distante, C.; Spagnolo, P.; Mazzeo, P.L.; Rosato, A.C.; Petrocchi, S.; Pellegrino, C.; Levante, A.; De Lumè, F.; et al. Computational Assessment of Facial Expression Production in ASD Children. Sensors 2018, 18, 3993. [Google Scholar] [CrossRef]
- Leo, M.; Carcagnì, P.; Distante, C.; Mazzeo, P.L.; Spagnolo, P.; Levante, A.; Petrocchi, S.; Lecciso, F. Computational Analysis of Deep Visual Data for Quantifying Facial Expression Production. Appl. Sci. 2019, 9, 4542. [Google Scholar]
- Daniels, A.M.; Mandell, D.S. Explaining differences in age at autism spectrum disorder diagnostic: A critical review. Autism 2014, 18, 583–597. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.K.; Liang, J.W.; Lord, C. Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. J. Child Psychol. Psychiatry 2014, 55, 485–494. [Google Scholar] [CrossRef]
- Lecciso, F.; Petrocchi, S.; Savazzi, F.; Marchetti, A.; Nobile, M.; Molteni, M. The association between maternal resolution of the diagnosis of autism, maternal mental representations of the relationship with the child, and children’s attachment. Lifesp. Disabil. 2013, 16, 21–38. [Google Scholar]
- Robins, D.L.; Dumont-Mathieu, T.M. Early screening for autism spectrum disorders: Update on the modified checklist for autism in toddlers and other measures. J. Dev. Behav. Pediatrics 2006, 27, S111–S119. [Google Scholar] [CrossRef]
- Lauritsen, M.B.; Pedersen, C.B.; Mortensen, P.B. Effects of familial risk factors and place of birth on the risk of autism: A nationwide register-based study. J. Child Psychol. Psychiatry 2005, 46, 963–971. [Google Scholar] [PubMed]
- Daniels, A.M.; Halladay, A.K.; Shih, A.; Elder, L.M.; Dawson, G. Approaches to enhancing the early detection of autism spectrum disorders: A systematic review of the literature. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 141–152. [Google Scholar] [CrossRef]
- García-Primo, P.; Hellendoorn, A.; Charman, T.; Roeyers, H.; Dereu, M.; Roge, B.; Baduel, S.; Muratori, F.; Narzisi, A.; Van Daalen, E.; et al. Screening for autism spectrum disorders: State of the art in Europe. Eur. Child Adolesc. Psychiatry 2014, 23, 1005–1021. [Google Scholar] [CrossRef]
- McPheeters, M.L.; Weitlauf, A.S.; Vehorn, A.; Taylor, C.; Sathe, N.A.; Krishnaswami, S.; Fonnesbeck, C.; Warren, Z.E. Screening for Autism Spectrum Disorder in Young Children: A Systematic Evidence Review for the U.S. Preventive Services Task Force; Evidence Synthesis No. 129; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2016.
- Sappok, T.; Heinrich, M.; Underwood, L. Screening tools for autism spectrum disorders. Adv. Autism 2015, 1, 12–29. [Google Scholar] [CrossRef]
- Zwaigenbaum, L.; Bauman, M.L.; Fein, D.; Pierce, K.; Buie, T.; Davis, P.A.; Newschaffer, C.; Robins, D.L.; Wetherby, A.; Choueiri, R.; et al. Early screening of autism spectrum disorder: Recommendations for practice and research. Pediatrics 2015, 136, S41–S59. [Google Scholar] [CrossRef]
- Marlow, M.; Servili, C.; Tomlinson, M. A review of screening tools for the identification of autism spectrum disorders and developmental delay in infants and young children: Recommendations for use in low-and middle-income countries. Autism Res. 2019, 12, 176–199. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-García, A.B.; Galindo-Villardón, P.; Nieto-Librero, A.B.; Martín-Rodero, H.; Robins, D.L. Toddler Screening for Autism Spectrum Disorder: A Meta-Analysis of Diagnostic Accuracy. JADD 2019, 49, 1837–1852. [Google Scholar] [CrossRef] [PubMed]
- Thabtah, F.; Peebles, D. Early Autism Screening: A Comprehensive Review. Int. J. Environ. Res. Public Health 2019, 16, 3502. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; De Vet, H.C. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidem. 2010, 63, 737–745. [Google Scholar] [CrossRef]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.; Bouter, L.M.; de Vet, H.C. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef]
- Levante, A.; Petrocchi, S.; Lecciso, F. Systematic review protocol of measures for the early detection of risk of Autism Spectrum Disorder risk in toddlers. Lifesp. Dis. 2019, 22, 55–75. [Google Scholar]
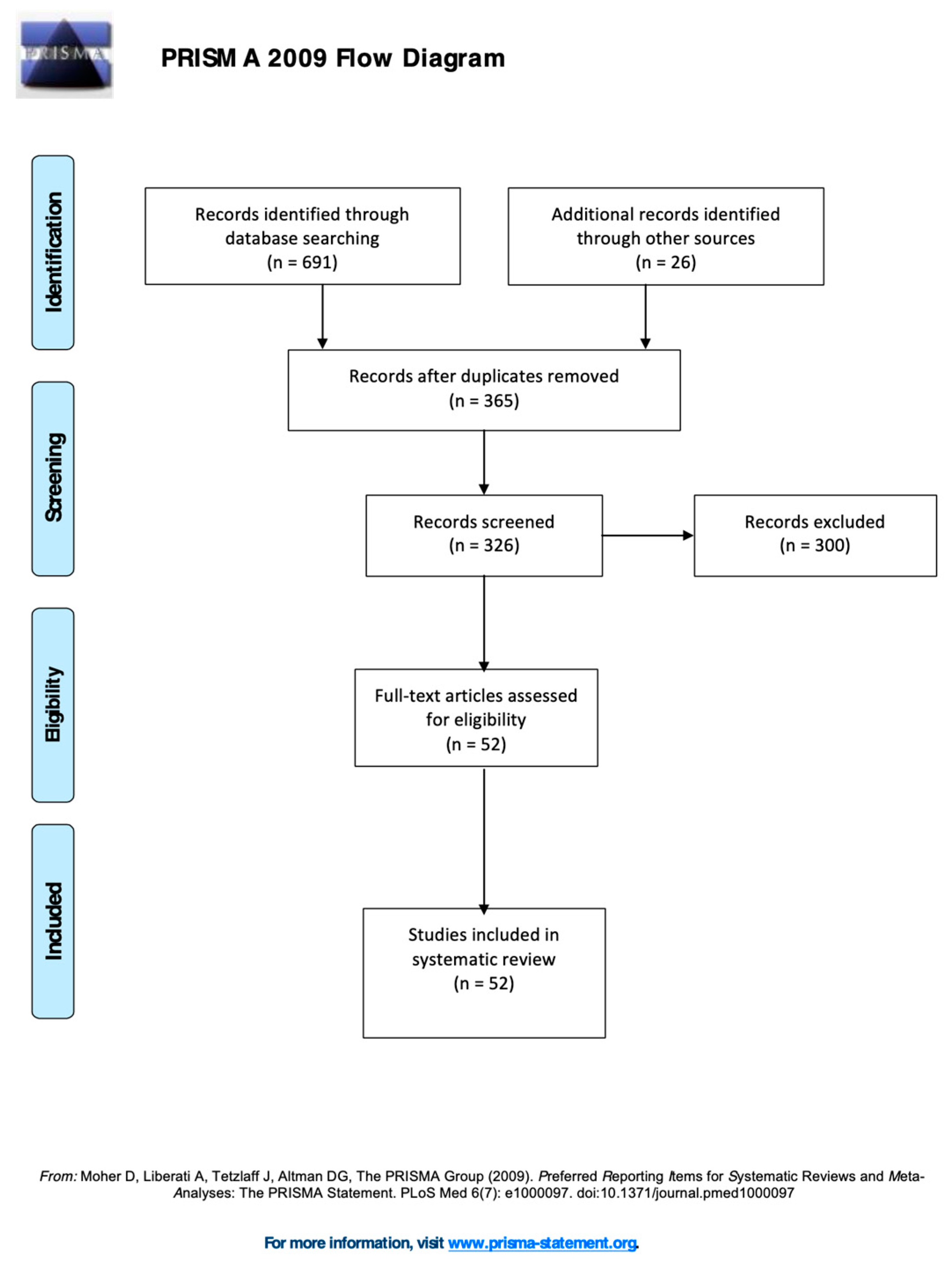
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Hedley, D.; Young, R.; Angelica, M.; Gallegos, J.; Marcin Salazar, C. Cross-cultural evaluation of the Autism Detection in Early Childhood (ADEC) in Mexico. Autism 2010, 14, 93–112. [Google Scholar] [CrossRef]
- Nah, Y.H.; Young, R.L.; Brewer, N. Using the Autism Detection in Early Childhood (ADEC) and Childhood Autism Rating Scales (CARS) to predict long term outcomes in children with autism spectrum disorders. JADD 2014, 44, 2301–2310. [Google Scholar] [CrossRef]
- Nah, Y.H.; Young, R.L.; Brewer, N.; Berlingeri, G. Autism Detection in Early Childhood (ADEC): Reliability and validity data for a level 2 screening tool for autistic disorder. Psychol. Assess. 2014, 26, 215. [Google Scholar] [CrossRef] [PubMed]
- Hedley, D.; Nevill, R.E.; Monroy-Moreno, Y.; Fields, N.; Wilkins, J.; Butter, E.; Mulick, J.A. Efficacy of the ADEC in identifying autism spectrum disorder in clinically referred toddlers in the US. JADD 2015, 45, 2337–2348. [Google Scholar] [CrossRef] [PubMed]
- Bryson, S.E.; Zwaigenbaum, L.; McDermott, C.; Rombough, V.; Brian, J. The Autism Observation Scale for Infants: Scale development and reliability data. JADD 2008, 38, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Brian, J.; Bryson, S.E.; Garon, N.; Roberts, W.; Smith, I.M.; Szatmari, P.; Zwaigenbaum, L. Clinical assessment of autism in high-risk 18-month-olds. Autism 2008, 12, 433–456. [Google Scholar] [CrossRef]
- Gammer, I.; Bedford, R.; Elsabbagh, M.; Garwood, H.; Pasco, G.; Tucker, L.; Volein, A.; Johnson, M.H.; Charman, T.; The BASIS Team. Behavioural markers for autism in infancy: Scores on the Autism Observational Scale for Infants in a prospective study of at-risk siblings. Inf. Behav. Dev. 2015, 38, 107–115. [Google Scholar] [CrossRef]
- Matson, J.L.; Fodstad, J.C.; Dempsey, T. What symptoms predict the diagnosis of autism or PDD-NOS in infants and toddlers with developmental delays using the Baby and Infant Screen for aUtIsm Traits. Dev. Neurorehab. 2009, 12, 381–388. [Google Scholar] [CrossRef]
- Matson, J.L.; Wilkins, J.; Sharp, B.; Knight, C.; Sevin, J.A.; Boisjoli, J.A. Sensitivity and specificity of the Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT): Validity and cutoff scores for autism and PDD-NOS in toddlers. Res. Autism Spectr. Disord. 2009, 3, 924–930. [Google Scholar] [CrossRef]
- Matson, J.L.; Wilkins, J.; Sevin, J.A.; Knight, C.; Boisjoli, J.A.; Sharp, B. Reliability and item content of the Baby and Infant Screen for Children with aUtIsm Traits (BISCUIT): Parts 1–3. Res. Autism Spectr. Disord. 2009, 3, 336–344. [Google Scholar] [CrossRef]
- Matson, J.L.; Boisjoli, J.A.; Hess, J.A.; Wilkins, J. Factor structure and diagnostic fidelity of the Baby and Infant Screen for Children with aUtIsm Traits–Part 1 (BISCUIT–Part 1). Dev. Neurorehab. 2010, 13, 72–79. [Google Scholar] [CrossRef]
- Matson, J.L.; Wilkins, J.; Fodstad, J.C. The validity of the baby and infant screen for children with autism traits: Part 1 (BISCUIT: Part 1). JADD 2011, 41, 1139–1146. [Google Scholar] [CrossRef]
- Dereu, M.; Warreyn, P.; Raymaekers, R.; Meirsschaut, M.; Pattyn, G.; Schietecatte, I.; Roeyers, H. Screening for Autism Spectrum Disorders in Flemish Day-Care Centres with the Checklist for Early Signs of Developmental Disorders. JADD 2010, 40, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Allen, J.; Gillberg, C. Can autism be detected at 18 months? The needle, the haystack, and the CHAT. Br. J. Psychiatry 1992, 161, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Cox, A.; Baird, G.; Swettenham, J.; Nightingale, N.; Morgan, K.; Drew, A.; Charman, T. Psychological markers in the detection of autism in infancy in a large population. Br. J. Psychiatry 1996, 168, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.M.; Tonge, B.J.; Sweeney, D.J.; Einfeld, S.L. Screening for Autism in young children with developmental delay: An evaluation of the Developmental Behavior Checklist: Early Screen. JADD 2008, 38, 1003–1010. [Google Scholar] [CrossRef]
- Dietz, C.; Swinkels, S.; van Daalen, E.; van Engeland, H.; Buitelaar, J.K. Screening for Autistic Spectrum Disorder in Children Aged 14-15 Months. II: Population Screening with the Early Screening of Autistic Traits Questionnaire (ESAT). Design and General Findings. JADD 2006, 36, 713–722. [Google Scholar] [CrossRef]
- Möricke, E.; Swinkels, S.H.N.; Beuker, K.T.; Buitelaar, J.K. Predictive value of subclinical autistic traits at age 14-15 months for behavioural and cognitive problems at age 3–5 years. Eur. Child Adolesc. Psychiatry 2010, 19, 659–668. [Google Scholar] [CrossRef][Green Version]
- Reznick, J.S.; Baranek, G.T.; Reavis, S.; Watson, L.R.; Crais, E.R. A parent- report instrument for identifying one-year-olds at risk for an eventual diagnosis of autism: The first year inventory. JADD 2007, 37, 1691–1710. [Google Scholar] [CrossRef]
- Ben-Sasson, A.; Carter, A.S. The application of the first year inventory for ASD screening in Israel. JADD 2012, 42, 1906–1916. [Google Scholar] [CrossRef]
- Turner-Brown, L.M.; Baranek, G.T.; Reznick, J.S.; Watson, L.R.; Crais, E.R. The First Year Inventory: A longitudinal follow-up of 12-month-old to 3-year-old children. Autism 2013, 17, 527–540. [Google Scholar] [CrossRef]
- Nygren, G.; Sandberg, E.; Gillstedt, F.; Ekeroth, G.; Arvidsson, T.; Gillberg, C. A new screening program for autism in a general population of Swedish toddlers. Res. Dev. Dis. 2012, 33, 1200–1210. [Google Scholar] [CrossRef]
- Robins, D.L.; Fein, D.; Barton, M.L.; Green, J.A. The Modified Checklist for Autism in Toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. JADD 2001, 31, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Snow, A.V.; Lecavalier, L. Sensitivity and specificity of the Modified Checklist for Autism in Toddlers and the Social Communication Questionnaire in preschoolers suspected of having pervasive developmental disorders. Autism 2008, 12, 627–644. [Google Scholar] [CrossRef] [PubMed]
- Seif Eldin, A.; Habib, D.; Noufal, A.; Farrag, S.; Bazaid, K.; Al-Sharbati, M.; Badr, H.; Moussa, S.; Essali, A.; Gaddour, N. Use of M-CHAT for a multinational screening of young children with autism in the Arab countries. Int. Rev. Psychiatry 2008, 20, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Canal-Bedia, R.; García-Primo, P.; Martín-Cilleros, M.V.; Santos-Borbujo, J.; Guisuraga-Fernández, Z.; Herráez-García, L.; del Mar Herraez-Garcia, M.; Boada-Muños, L.; Fuentes-Biggi, M.; Posada-de La Paz, M. Modified checklist for autism in toddlers: Cross-cultural adaptation and validation in Spain. JADD 2011, 41, 1342–1351. [Google Scholar] [CrossRef]
- Inada, N.; Koyama, T.; Inokuchi, E.; Kuroda, M.; Kamio, Y. Reliability and validity of the Japanese version of the Modified Checklist for autism in toddlers (M- CHAT). Res. Autism Spectr. Disord. 2011, 5, 330–336. [Google Scholar] [CrossRef]
- Albores-Gallo, L.; Roldán-Ceballos, O.; Villarreal-Valdes, G.; Betanzos-Cruz, B.X.; Santos-Sánchez, C.; Martínez-Jaime, M.M.; Lemus-Espinosa, I.; Hilton, C.L. M-CHAT Mexican version validity and reliability and some cultural considerations. ISRN Neurol. 2012, 2012, 408694:1–408694:7. [Google Scholar] [CrossRef]
- Kozlowski, A.M.; Matson, J.L.; Worley, J.A.; Sipes, M.; Horovitz, M. Defining characteristics for young children meeting cutoff on the modified checklist for autism in toddlers. Res. Autism. Spectr. Disord. 2012, 6, 472–479. [Google Scholar] [CrossRef]
- Scarpa, A.; Reyes, N.M.; Patriquin, M.A.; Lorenzi, J.; Hassenfeldt, T.A.; Desai, V.J.; Kerkering, K.W. The modified checklist for autism in toddlers: Reliability in a diverse rural American sample. JADD 2013, 43, 2269–2279. [Google Scholar] [CrossRef]
- Matson, J.L.; Kozlowski, A.M.; Fitzgerald, M.E.; Sipes, M. True versus false positives and negatives on the Modified Checklist For Autism in Toddlers. Res. Autism Spectr. Disord. 2013, 7, 17–22. [Google Scholar] [CrossRef]
- Stenberg, N.; Bresnahan, M.; Gunnes, N.; Hirtz, D.; Hornig, M.; Lie, K.K.; Lipkin, W.I.; Lord, C.; Magnus, P.; Kjennerud, T.R.; et al. Identifying children with autism spectrum disorder at 18 months in a general population sample. Paed. Perinat. Epidem. 2014, 28, 255–262. [Google Scholar] [CrossRef]
- Seung, H.; Ji, J.; Kim, S.J.; Sung, I.; Youn, Y.A.; Hong, G.; Lee, H.; Lee, Y.H.; Lee, H.; Youm, H.K. Examination of the Korean modified checklist of autism in toddlers: Item responsetheory. JADD 2015, 45, 2744–2757. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Gómez, J.L.; Andrea Manzone, L.; Posada-De-La-Paz, M. Modified checklist for autism in toddler cross-cultural adaptation for Argentina. Int. J. Dev. Dis. 2016, 62, 117–123. [Google Scholar] [CrossRef]
- Baduel, S.; Guillon, Q.; Afzali, M.H.; Foudon, N.; Kruck, J.; Rogé, B. The French version of the modified-checklist for autism in toddlers (M-CHAT): A validation study on a French sample of 24 months old children. JADD 2017, 47, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, J.M.; Robins, D.L.; Ventola, P.E.; Pandey, J.; Boorstein, H.C.; Esser, E.L.; Wilson, L.B.; Rosenthal, M.A.; Sutera, S.; Verbalis, A.D.; et al. The modified checklist for autism in toddlers: A follow-up study investigating the early detection of autism spectrum disorders. JADD 2008, 38, 827–839. [Google Scholar] [CrossRef]
- Chlebowski, C.; Robins, D.L.; Barton, M.L.; Fein, D. Large-scale use of the modified checklist for autism in low-risk toddlers. Pediatrics 2013, 131, e1121–e1127. [Google Scholar] [CrossRef]
- Robins, D.L.; Casagrande, K.; Barton, M.; Chen, C.M.A.; Dumont-Mathieu, T.; Fein, D. Validation of the modified checklist for autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics 2014, 133, 37–45. [Google Scholar] [CrossRef]
- Brennan, L.; Fein, D.; Como, A.; Rathwell, I.C.; Chen, C.M. Use of the Modified Checklist for Autism, Revised with Follow Up-Albanian to Screen for ASD in Albania. JADD 2016, 46, 3392–3407. [Google Scholar] [CrossRef]
- Carakovac, M.; Jovanovic, J.; Kalanj, M.; Rudic, N.; Aleksic–Hil, O.; Aleksic, B.; Villalobos, I.B.; Kasuya, H.; Ozaki, N.; Lecic-Tosevski, D.; et al. Serbian language version of the modified checklist for autism in toddlers, revised, with follow-up: Cross-cultural adaptation and assessment of reliability. Sci. Rep. 2016, 6, 38222. [Google Scholar] [CrossRef]
- Windiani, I.G.A.T.; Soetjiningsih, S.; Adnyana, I.G.A.S.; Lestari, K.A. Indonesian Modified Checklist for Autism in Toddler, Revised with Follow-Up (M- CHAT-R/F) for Autism Screening in Children at Sanglah General Hospital, Bali- Indonesia. Bali Med. J. 2016, 5, 133–137. [Google Scholar] [CrossRef]
- Guo, C.; Luo, M.; Wang, X.; Huang, S.; Meng, Z.; Shao, J.; Zhang, X.; Shao, Z.; Wu, J.; Robins, D.L.; et al. Reliability and Validity of the Chinese Version of Modified Checklist for Autism in Toddlers, Revised, with Follow-Up (M-CHAT-R/F). JADD 2018, 1–12. [Google Scholar] [CrossRef]
- Sangare, M.; Toure, H.B.; Toure, A.; Karembe, A.; Dolo, H.; Coulibaly, Y.I.; Kouyate, M.; Traore, K.; Diakite, S.A.; Coulibaly, S.; et al. Validation of two parent-reported autism spectrum disorders screening tools M-CHAT-R and SCQ in Bamako, Mali. eNeurol. Sci. 2019, 15, 100188. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.A.; Ward, R.A.; Savona, D.; Regehr, K.; Parker, K.; Hudson, M.; Penning, H.; Holden, J.A. Development and Initial Validation of Parent Report Measure of the Behavioral development of infants at risk for Autism Spectrum Disorders. JADD 2012, 42, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Allison, C.; Baron-Cohen, S.; Wheelwright, S.; Charman, T.; Richler, J.; Pasco, G.; Brayne, C. The Q-CHAT (Quantitative CHecklist for Autism in Toddlers): A normally distributed quantitative measure of autistic traits at 18–24 months of age: Preliminary report. JADD 2008, 38, 1414–1425. [Google Scholar] [CrossRef] [PubMed]
- Magiati, I.; Goh, D.A.; Lim, S.J.; Gan, D.Z.Q.; Leong, J.C.L.; Allison, C.; Baron-Cohen, S.; Rifkin-Graboi, A.; Broekman, B.F.P.; Saw, S.M.; et al. The psychometric properties of the Quantitative-Checklist for Autism in Toddlers (Q-CHAT) as a measure of autistic traits in a community sample of Singaporean infants and toddlers. Mol. Autism 2015, 6, 40. [Google Scholar] [CrossRef]
- Ruta, L.; Chiarotti, F.; Arduino, G.M.; Apicella, F.; Leonardi, E.; Maggio, R.; Carozza, C.; Chericoni, N.; Costanzo, V.; Turco, N.; et al. Validation of the Quantitative CHecklist for Autism in Toddlers (Q-CHAT) in an Italian clinical sample of young children with Autism and Other Developmental Disorders. Front. Psychiatry 2019, 10, 488. [Google Scholar] [CrossRef]
- Rutaa, L.; Arduino, G.M.; Gagliano, A.; Apicella, F.; Leonardi, E.; Famà, F.I.; Chericoni, N.; Costanzo, V.; Turco, N.; Tartarisco, G.; et al. Psychometric properties, factor structure and cross-cultural validity of the quantitative CHecklist for autism in toddlers (Q-CHAT) in an Italian community setting. Res. Autism Spectr. Disord. 2019, 64, 39–48. [Google Scholar] [CrossRef]
- Lecciso, F.; Levante, A.; Signore, F.; Petrocchi, S. Preliminary evidence of the Structural Validity and measurement invariance of the Quantitative-CHecklist for Autism in Toddler (Q-CHAT) on Italian unselected children. EJASA 2019, 12, 320–340. [Google Scholar] [CrossRef]
- Persson, B.; Nordstrom, B.; Petersson, K.; Månsson, M.E.; Sivberg, B. Screening for infants with developmental deficits and/or autism: A Swedish pilotstudy. J. Pediatric Nurs. 2006, 21, 313–324. [Google Scholar] [CrossRef]
- Oner, P.; Oner, O.; Munir, K. Three-Item Direct Observation Screen (TIDOS) for autism spectrum disorder. Autism 2014, 18, 733–742. [Google Scholar] [CrossRef]
- Honda, H.; Shimizu, Y.; Nitto, Y.; Imai, M.; Ozawa, T.; Iwasa, M.; Shiga, K.; Hira, T. Extraction and refinement strategy for detection of autism in 18-month-old: A guarantee of higher sensivity and specificity in the process of mass screening. J. Child Psychol. Psychiatry 2009, 50, 972–981. [Google Scholar] [CrossRef]
- Prinsen, C.A.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; De Vet, H.C.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Sirigatti, S.; Stefanile, C. MMPI-2: Aggiornamento all’ Adattamento Italiano; Giunti OS Organizzazioni Speciali: Florence, Italy, 2011. [Google Scholar]
- Petrocchi, S.; Iannello, P.; Lecciso, F.; Levante, A.; Antonietti, A.; Schulz, P.J. Interpersonal Trust in Doctor-Patient Relation: Evidence from Dyadic Analysis and Association with Quality of Dyadic Communication. Soc. Sci. Med. 2019, 235, 112391. [Google Scholar] [CrossRef] [PubMed]
- Reichow, B.; Barton, E.E.; Boyd, B.A.; Hume, K. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD). Cochrane Database Syst. Rev. 2012, 10, CD009260. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measure Name (Short Name) | Short Description of the Dimension(s) Measured | Admin. Age (Months) | Number of Items | Type of Answer | Admin. Time (Minute) | Admin. Method | Cut-Off | N° of Validation Studies Included |
|---|---|---|---|---|---|---|---|---|
| Autism Detection in Early Childhood (ADEC) | Social interaction behaviors and social communication behaviors. | 12–36 | 16 | 3-point Likert scale | 10 | Observational checklist for professionals | 11 | 4 |
| Autism Observation Scale for Infants (AOSI) | Social communication behaviors, non- social behaviors, | 6–18 | 18 | 3-point Likert scale | 15-20 | Observational checklist for professionals | n.s. | 3 |
| Baby and Infants Screen for Children with aUtIsm Traits (BISCUIT) | Part 1 ASD symptoms; Part 2 comorbid psychopathology; Part 3 behavioral problems. | 17–37 | Part 1: 62; Part 2: 65; Part 3: 17. | 3-point Likert scale | 15 | Parent-interview | Part 1: 17; Part 2: 39; Part 3: 17. | 5 |
| Checklist for Early Signs of Developmental Disorders | Language and social functioning. | 3–39 | 25 | Yes/No | Not declared | Parent-reported questionnaire | 2 | 1 |
| CHecklist for Autism in Toddlers (CHAT) | Social play, social interest, pretend play, joint-attention, proto-declarative pointing, imitation; B functional play, proto-imperative pointing, motor development, rough and tumble play. | 18 | Part A: 9; Part B: 5 | Yes/No | 15 | Part A: parent- reported questionnaire; Part B: professionals- reported questionnaire | 3 key item | 2 |
| Developmental Behavior Checklist: Early Screen (DBC-ES) | Social, verbal, and non-verbal communication, restricted and repetitive behaviors and interests | 18–48 | 17 | 3-point Likert scale | 5–10 | Parent-reported questionnaire | 11 | 1 |
| Early Screening of Autistic Traits Questionnaire (ESAT) | Social- communication skills, stereotyped behaviors, reactions | 14–15 | 14 | Yes/No | 5–10 | Parent-reported questionnaire | 3 | 2 |
| First Year Inventory (FYI) | Social communication and sensory regulatory domains. | 12 | 63 | 4 point Likert scale; multiple choice; two open-ended question. | 10 | Parent-reported questionnaire | 30 (95th); 40 (98th); 50 (99th) [73] (Reznick et al., 2007); 22.55 (95th); 28.14 (98th) [39]; 19.2 (96th) [84]. | 3 |
| Joint Attention OBServation (JA- OBS) | Joint attention | 20–48 | 5 | Yes/No | 10 | Observational checklist for professionals | 2 | 1 |
| Modified Checklist for Autism in Toddlers (M- CHAT) | Social interest, pretend and functional play, joint-attention, proto-declarative pointing, imitation, motor development, rough and tumble play. | 16–30 | 23 | Yes/No | 5–10 | Parent-reported questionnaire | 2 for the critical items (2–7–9–13–14–15) or 3 for the total score | 13 |
| Modified Checklist for Autism in Toddlers-Revised with Follow-up (M-CHAT-R/F) | Social interest, pretend and functional play, joint-attention, proto-declarative pointing, imitation, motor development, rough and tumble play. | 16–30 | 20 | Yes/No | 5–10 | Parent-reported interview | 0–2: low risk 3–7: moderate risk 8–20: high risk | 7 |
| Parent Observation of Early Markers Scale (POEMS) | Social and communicative development, restricted interests, behavioral and emotional problems. | 1–24 | 61 | 4-point Likert Scale | 30 | Parent-reported questionnaire | 70 | 1 |
| Quantitative CHecklist for Autism in Toddlers (Q- CHAT) | Social communication, behavior, and language. | 18–24 | 25 | 5-point Likert scale | 5–10 | Parent-reported questionnaire | n.s. | 2 |
| Screening for Infants with Developmental Deficits and/or Autism (SEEK) | I: sleep, eating, and parent-child interaction; II: regulation, parent-child interaction, communication, and coordination stability. | 8 | SEEK I: 6; SEEK II: 33 | Yes/No | 3–-40 | Parent-reported questionnaire and observational checklist for professionals | n.s. | 1 |
| Three-Item Direct Observation Screen (TIDOS) | Joint attention, eye contact and response to name. | 18–60 | 3 | Yes/no | 15–20 | Observational checklist for professionals | 1 | 1 |
| Young Autism and other developmental disorders CHeckup Tool: 18-month-olds’ version (YACHT-18) | Motor functions, communication and social interaction, pointing, and language comprehension. | 18 | I: questionnaire (11 items); II: interview (6 questions); II: picture card test. | I: yes/no; III: pass/fail | 10 | Professionals - reported questionnaire; interview with caregivers, child observation | n.s. | 1 |
| Measure | Author(s) (Year) | Study Design | Population and Subgroups | Application Level (1, 2, or “Hybrid”) | Sens. | Spec. | PPV(NPV) |
|---|---|---|---|---|---|---|---|
| ADEC | [34] | Cross sect. | Study 1 N = 19 ASD N = 13 ODD N = 29 gen pop. Study 2 N = 34 PDD N = 15 gen. pop. N = 5 ODD | hybrid | range: 79%–94% | range: 88%–100% | Study 1: 0.75 (0.90) Study 2: 1 (0.71) |
| [35] | Long. | N = 55 ASD | Hybrid | 100% | 89% | 0.84 (1 *) | |
| [36] | Cross sect. | N = 70 ASD N = 24 PDD-NOS N = 57 ODD N = 64 gen. pop. | Hybrid | 100% | range: 74%–90% | 0.84 (1) | |
| [37] | Cross-sect. | N = 96 DC | 2 | range: 93%–94% | range: 62%–64% | 0.83 (0.81) | |
| AOSI | [38] | Cross sect. | N = 101 GR | 2 | N/A | N/A | N/A |
| [39] | Long. | N = 115 GR N = 73 DC | 2 | N/A | N/A | N/A | |
| [40] | Cross sect. | N = 54 GR N = 50 DC | 2 | N/A | N/A | N/A | |
| BISCUIT | [41] | Cross-sect. | Study 1 N = 957 DC Study 2 N = 171 ASD N = 144 PDD-NOS | 2 | Part 1: 84.7%; Part 2: 84.4%; Part 3: 93.4% | Part 1: 86.4%; Part 2: 83.3%; Part 3: 86.6% | N/A |
| [42] | Cross-sect. | N = 178 ASD N = 152 PDD-NOS N = 677 gen. pop. | Hybrid | N/A | N/A | N/A | |
| [43] | Cross-sect. | N = 276 DC | 2 | N/A | N/A | N/A | |
| [44] | Cross-sect. | Study 1 N = 405 ASD Study 2 N = 405 ASD N = 882 gen. pop. | Hybrid | N/A | N/A | N/A | |
| [45] | Cross-sect. | N = 178 ASD N = 152 PDD-NOS N = 677 gen. pop. | Hybrid | N/A | N/A | N/A | |
| CESDD | [46] | Long. | Wave 1 N = 6.808 gen. pop. Wave 2 N = 255 at risk Wave 3 N = 20 ASD N = 40 ODD | 1 | 80% | 94% | 0.07 (0.99) |
| CHAT | [47] | Cross-sect. | N = 50 gen. pop. N = 41 GR | 2 | N/A | N/A | N/A |
| [48] | Long. | Wave 1 N = 16.000 gen. pop. Wave 2 N = 10 ASD N = 17 ODD N = 23 TD | 1 | N/A | N/A | N/A | |
| DBC-ES | [49] | Cross-sect. | N = 142 ASD or PDD N = 65 ODD | Hybrid | 83% | 48% | 0.78(0.56) |
| ESAT | [50] | Long. | Wave 1 N = 31.724 gen. pop Wave 2 N = 255 at risk Wave 3 N = 18 ASD N = 55 ODD. | 1 | N/A | N/A | N/A |
| [51] | Long. | Wave 1 N = 4.107 gen. pop. Wave 2 N = 103 at risk | 1 | N/A | N/A | N/A | |
| FYI | [52] | Cross-sect. | N = 1300 gen. pop. | 1 | N/A | N/A | N/A |
| [53] | Long. | Wave 1 N = 471 gen. pop. Wave 2 N = 17 at risk | 1 | N/A | N/A | N/A | |
| [54] | Long. | Wave 1 N = 699 gen. pop. Wave 2 N = 9 ASD | 1 | N/A | N/A | N/A | |
| JA-OBS | [55] | Long. | Wave 1 N = 3999 Wave 2 N = 64 at risk Wave 3 N = 48 ASD N = 3 TD N = ODD | 1 | 86% | N/A | 0.90 (N/A) |
| M-CHAT | [56] | Long. | Wave 1 N = 1.122 gen. pop.; Wave 2 N = 171 at risk | 1 | 87% | 99% | 0.80 (0.99) |
| [57] | Cross-sect. | N = 36 ASD N = 18 PDD-NOS N = 28 ODD | Hybrid | Critic items: 79%; Total score: 88% | Critic items: 38%; Total score: 38% | 0.79(0.28) | |
| [58] | Cross-sect. | N = 122 ASD N = 106 gen. pop. | Hybrid | 86% | 80% | 0.81(0.93) | |
| [59] | Long. | Study 1 Wave 1 N = 2480 gen. pop.; Wave 2 N = 23 ASD N = 63 ODD Study 2: Wave 1 N = 2055 gen. pop. Wave 2 N = 6 ASD N = ODD | 1 | 100% | 98% | Study 1: 0.35 (1) Study 2: 0.19 (1) | |
| [60] | Cross-sect. | N = 24 gen. pop. N = 25 DC | 2 | Critic items: 75%; Total score: 65% | Critic items: 89%; Total score: 88% | 0.21(0.98) | |
| [61] | Cross-sect. | N = 117 ASD N = 339 gen. pop. | Hybrid | N/A | N/A | N/A | |
| [62] | Cross-sect. | N = 141 ASD N = 102 ODD | Hybrid | range: 70%–97% | range: 38%–99% | N/A | |
| [63] | Cross-sect. | N = 447 gen. pop. | 1 | ||||
| [64] | Cross-sect. | N = 552 DC | 2 | range: 70%–97% | range: 38%–99% | N/A | |
| [65] | Long. | Wave 1 N = 51.853 gen. pop. Wave 2 N = 173 ASD | 1 | Critic items: 20.8%; total score: 34.1% | Critic items: 97.9%; total score: 92.7% | Critic items: 0.33 (N/A); total score: 0.15 (N/A) | |
| [66] | Cross-sect. | N = 2048 gen. pop. | 1 | N/A | N/A | N/A | |
| [67] | Long. | Wave 1 N = 420 gen. pop. Wave 2 N = 2 ASD | 1 | N/A | N/A | N/A | |
| [68] | Long. | Wave 1 N = 1250 DC Wave 2 N = 18 ASD N = 17 ODD N = 1 TD | 2 | 67% | With FUI: 99%; Without FUI: 94% | With FUI: 0.60 (0.99) Without FUI: 0.14 (0.99) | |
| M-CHAT-R/F | [69] | Long. | Study 1 N = 3309 DC N = 484 GR; Study 2 Wave 1: N = 1.160 DC N = 256 = GR Wave 2 N = 80 ASD N = 51 ODD | 2 | N/A | N/A | N/A |
| [70] | Cross-sect. | N = 207 DC | 2 | N/A | N/A | N/A | |
| [71] | Long. | Wave 1 N = 16.115 gen. pop. Wave 2 N = 123 ASD N = 140 ODD | 1 | 94% | 83% | 0.50 (0.99) | |
| [72] | Long. | Wave 1 N = 2594 gen. pop. Wave 2 N = 253 at risk Wave 3 N = 17 ASD | 1 | N/A | N/A | N/A | |
| [73] | Cross-sect. | N = 20 DC N = 128 TD | 2 | N/A | N/A | N/A | |
| [74] | Long. | Wave 1 N = 110 gen. pop. Wave 2 N = 18 ASD | 1 | 88.9% | 94.6% | 0.76 (0.97) | |
| [75] | Long. | Wave 1 N = 7928 gen. pop. Wave 2 N = 1140 at risk Wave 3 N = 72 ASD | 1 | 96% | 86% | 0.69 (1) | |
| [76] | Cross-sect. | N = 947 gen. pop. | 1 | 50% | 100% | 100(0.87) | |
| POEMS | [77] | Cross-sect. | N = 108 GR | 2 | 74% | 73% | 0.21 (N/A) |
| Q-CHAT | [78] | Cross sect. | N = 779 gen. pop. N = 160 ASD | Hybrid | N/A | N/A | N/A |
| [79] | Cross-sect. | N = 764 gen. pop. | 1 | N/A | N/A | N/A | |
| [80] | Cross-sect. | N = 139 ASD N = 50 PDD N = 126 TD | 2 | 73–83% | 76–78% | N/A | |
| [81] | Cross-sect. | N = 2400 | 1 | N/A | N/A | N/A | |
| [82] | Cross-sect. | N = 545 | 1 | N/A | N/A | N/A | |
| SEEK | [83] | Cross-sect. | N = 312 gen. pop. | 1 | N/A | N/A | N/A |
| TIDOS | [84] | Cross-sect. | N = 86 ASD N = 76 ODD N = 97 gen. pop. | Hybrid | 95% | 85% | 0.91(0.90) |
| YACHT-18 | [85] | Cross-sect. | N = 2.814 gen. pop. | 1 | 60% | 86.3% | N/A |
| Measures | Author(s), (Years) | Psychometric Properties | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Internal Consistency | Reliability | Measurement Error | Content Validity | Structural Validity | Hypothesis Testing | Cross-Cultural Validity | Criterion Validity | Responsiveness | ||
| ADEC | [34] | 0 unidimensionality, sample | + missing item, sample, time interval | 0 sample | 0 sample | 0 sample | ||||
| [35] | + missing item | + missing item | ||||||||
| [36] | 0 unidimensionality | 0 time interval | + missing item | + missing item | + missing item | |||||
| [37] | 0 unidimensionality | + missing item, hypothesis | + missing item | |||||||
| AOSI | [38] | + sample, missing item | +++ | |||||||
| [39] | + missing item | + missing item | ||||||||
| [40] | + missing item | + missing item | + missing item | + missing item | ||||||
| BISCUIT | [41] | 0 comparator instrument | 0 statistical methods | |||||||
| [42] | + missing item, hypothesis, comparator instrument | + missing item | ||||||||
| [43] | 0 unidimensionality | |||||||||
| [44] | + missing item | +++ | + missing item | + missing item | 0 statistical method | |||||
| [45] | 0 unidimensionality | + missing item, hypothesis | 0 no gold standard | |||||||
| CESDD | [46] | + hypothesis | + missing item | |||||||
| CHAT | [47] | +++ | + ++ | 0 comparator instrument | 0 no gold standard | |||||
| [48] | + missing item | + missing item | ||||||||
| DBC-ES | [49] | 0 unidimensionality | 0 only one measurement | + missing item, hypothesis | + missing item | |||||
| ESAT | [50] | 0 time interval | + missing item, hypothesis | + missing item | ||||||
| [51] | + missing item | + missing item | ||||||||
| FYI | [52] | +++ | +++ | 0 statistical method | ++ | +++ | ||||
| [53] | 0 statistical method | ++ | 0 statistical method | ++ | ||||||
| [54] | 0 time interval, measurement condition | + sample | + missing item, sample | + missing item, statistical method | ||||||
| JA-OBS | [55] | 0 only one measurement | + missing item | |||||||
| M-CHAT | [56] | +++ | . | + missing item, sample | 0 missing item | |||||
| [57] | 0 unidimensionality | ++ | ++ | |||||||
| [58] | + missing item | |||||||||
| [59] | + missing item, hypothesis | 0 missing item, translation | + missing item | |||||||
| [60] | 0 sample, unidimensionality | 0 sample | 0 sample, hypothesis | 0 sample, comparator instrument | ||||||
| [61] | 0 unidimensionality | + missing item, hypothesis | + missing item | |||||||
| [62] | +++ | 0 statistical method | ||||||||
| [63] | 0 measurement not independent | 0 comparator instrument | ||||||||
| [64] | 0 only one measurement | 0 comparison instrument | ||||||||
| [65] | + time interval | + sample, hypothesis | 0 missing item | |||||||
| [66] | +++ | |||||||||
| [67] | + missing item | 0 statistical method | ||||||||
| [68] | 0 missing item, hypothesis | 0 missing item, sample | ||||||||
| M-CHAT-R/F | [69] | 0 unidimensionality | 0 measurement not indipendent | + missing item | 0 statistical method | 0 statistical method | ||||
| [70] | + missing item | |||||||||
| [71] | 0 unidimensionality | 0 administration not similar, statistical method | + hypothesis | +++ | ||||||
| [72] | 0 sample, unidimensionality | 0 time interval, statistical method | ++ | 0 expertise translator, statistcal method | 0 sample | |||||
| [73] | 0 sample, undimensionality | 0 missing, sample, time interval, statistical method | 0 statistical method | |||||||
| [74] | + missing item | 0 comparator instrument | + translation | 0 no golden standard | ||||||
| [75] | 0 undimensionality | 0 statistical method | 0 hypothesis | 0 no pilot study, statistical method | +++ | |||||
| [76] | 0 comparator instrument | |||||||||
| POEMS | [77] | 0 unidimensionality | ++ | +++ | 0 hypothesis | 0 statistical methods | ||||
| Q-CHAT | [78] | +++ | + measurement condition | +++ | + hypothesis | |||||
| [79] | +++ | 0 time interval | +++ | + hypothesis | 0 comparator instrument | |||||
| [80] | +++ | 0 comparator instrument | +++ | |||||||
| [81] | +++ | +++ | 0 comparator instrument | 0 statistical method | ||||||
| [82] | + missing item | + missing item | + missing item | 0 no pilot study; statistical method | ||||||
| SEEK | [83] | +++ | ||||||||
| TIDOS | [84] | +++ | + missing item | + missing item | ||||||
| YACHT- 18 | [85] | + missing item | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrocchi, S.; Levante, A.; Lecciso, F. Systematic Review of Level 1 and Level 2 Screening Tools for Autism Spectrum Disorders in Toddlers. Brain Sci. 2020, 10, 180. https://doi.org/10.3390/brainsci10030180
Petrocchi S, Levante A, Lecciso F. Systematic Review of Level 1 and Level 2 Screening Tools for Autism Spectrum Disorders in Toddlers. Brain Sciences. 2020; 10(3):180. https://doi.org/10.3390/brainsci10030180
Chicago/Turabian StylePetrocchi, Serena, Annalisa Levante, and Flavia Lecciso. 2020. "Systematic Review of Level 1 and Level 2 Screening Tools for Autism Spectrum Disorders in Toddlers" Brain Sciences 10, no. 3: 180. https://doi.org/10.3390/brainsci10030180
APA StylePetrocchi, S., Levante, A., & Lecciso, F. (2020). Systematic Review of Level 1 and Level 2 Screening Tools for Autism Spectrum Disorders in Toddlers. Brain Sciences, 10(3), 180. https://doi.org/10.3390/brainsci10030180