Thalamic Deep Brain Stimulation in Essential Tremor Plus Is as Effective as in Essential Tremor


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Protocol Approval, Registration, and Consent
2.3. Data Acquisition and Tremor Analysis
2.4. Active Contact Location and Stimulation Parameters
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. DBS Effect and Tremor-Scores
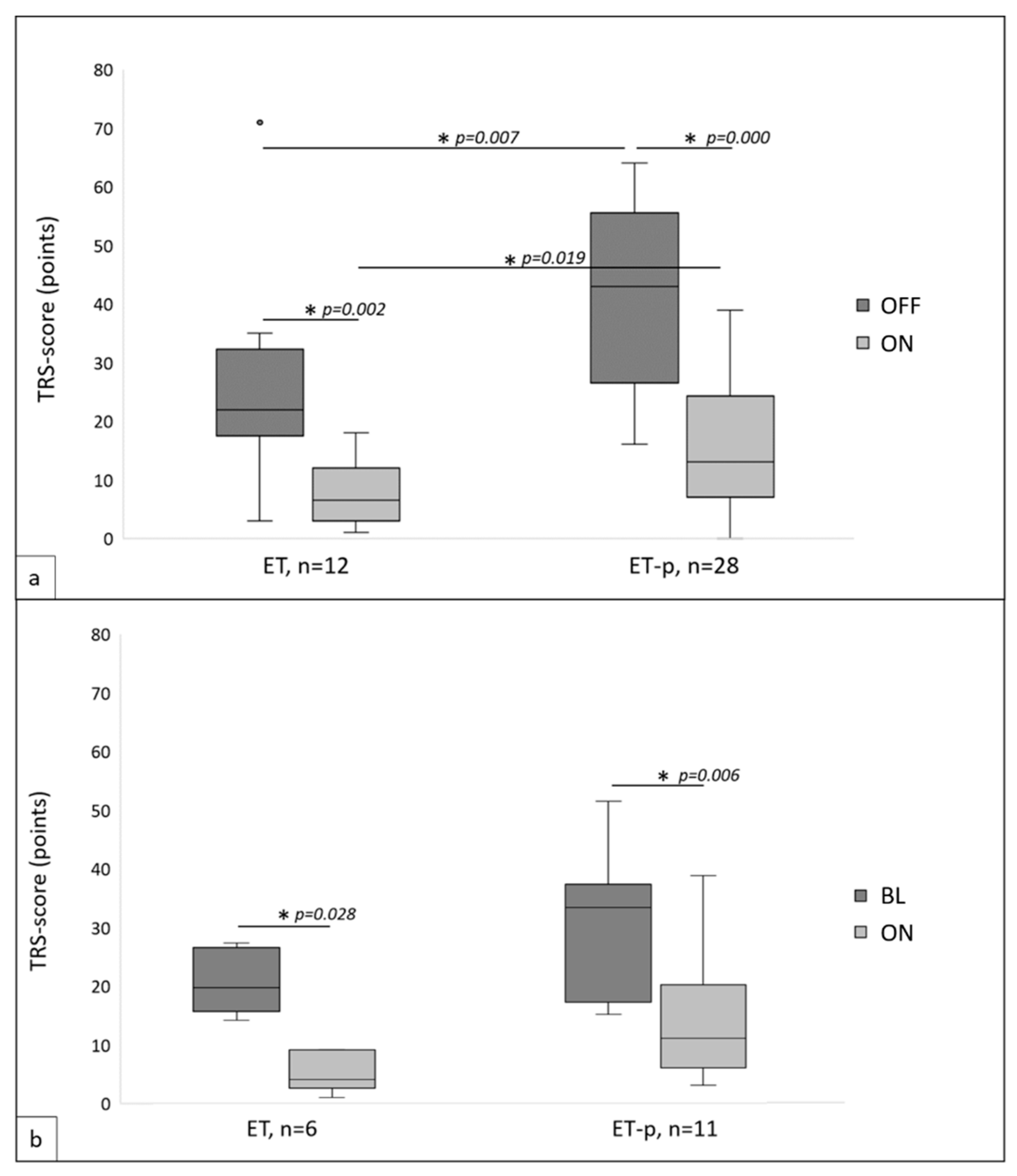
3.2.1. TRS in Stimulation-OFF and -ON
3.2.2. TRS at Baseline and Follow-Up
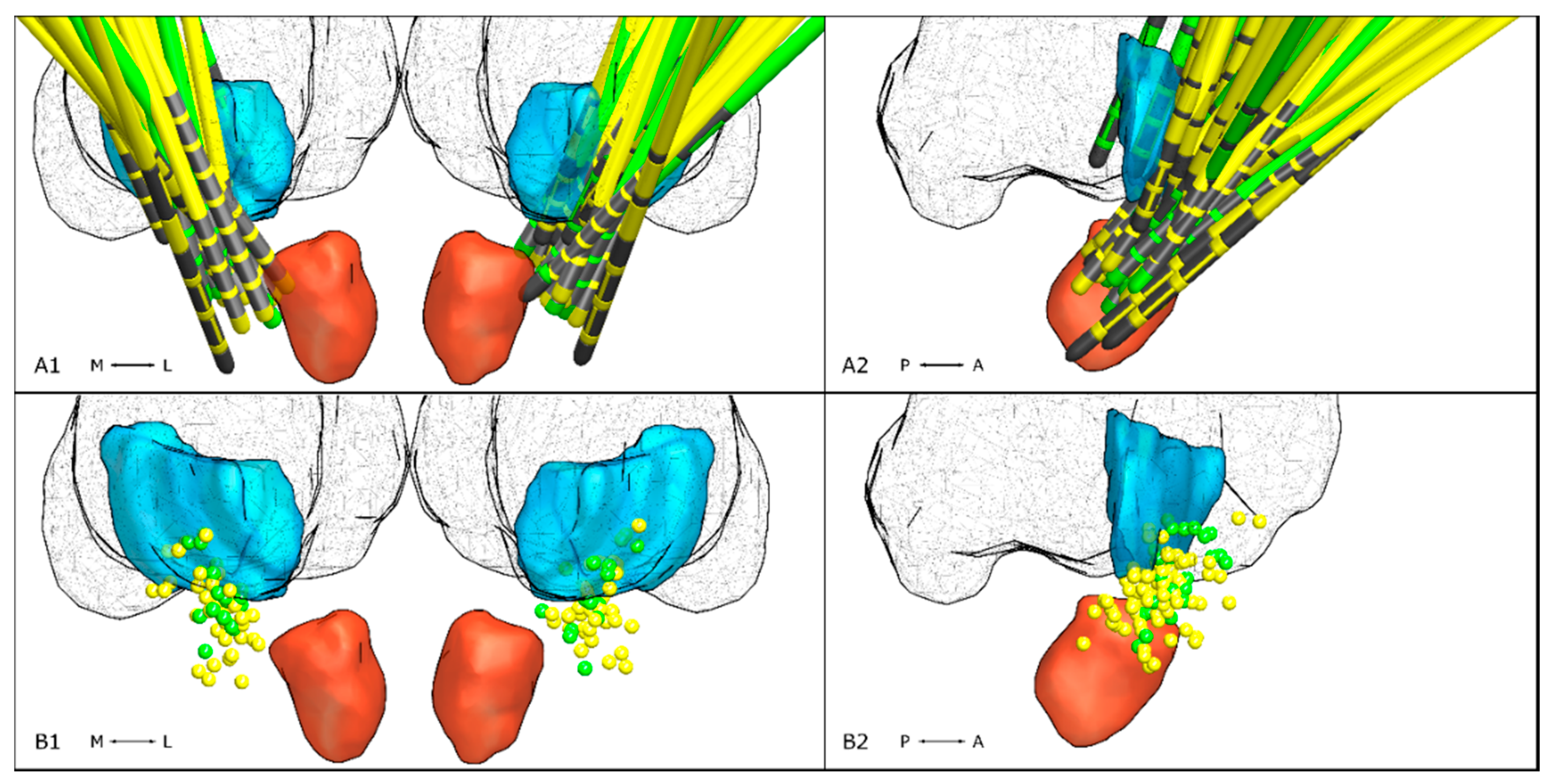
3.2.3. Active Contact Location
3.2.4. Stimulation Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bhatia, K.P.; Bain, P.; Bajaj, N.; Elble, R.J.; Hallett, M.; Louis, E.D.; Raethjen, J.; Stamelou, M.; Testa, C.M.; Deuschl, G.; et al. Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society. Mov. Disord. 2017, 33, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Pal, P.K. Reclassifying essential tremor: Implications for the future of past research. Mov. Disord. 2019, 34, 437. [Google Scholar] [CrossRef] [PubMed]
- Rajalingam, R.; Breen, D.P.; Lang, A.E.; Fasano, A. Essential tremor plus is more common than essential tremor: Insights from the reclassification of a cohort of patients with lower limb tremor. Parkinsonism Relat. Disord. 2018, 56, 109–110. [Google Scholar] [CrossRef] [PubMed]
- Louis, E.D. ‘Essential Tremor Plus’: A Problematic Concept: Implications for Clinical and Epidemiological Studies of Essential Tremor. Neuroepidemiology 2020, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, G.; Raethjen, J.; Hellriegel, H.; Elble, R. Treatment of patients with essential tremor. Lancet Neurol. 2011, 10, 148–161. [Google Scholar] [CrossRef]
- Zhang, K.; Bhatia, S.; Oh, M.Y.; Cohen, D.; Angle, C.; Whiting, D. Long-term results of thalamic deep brain stimulation for essential tremor. J. Neurosurg. 2009, 112, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Koller, W.C.; Lyons, K.E.; Wilkinson, S.B.; Troster, A.I.; Pahwa, R. Long-term safety and efficacy of unilateral deep brain stimulation of the thalamus in essential tremor. Mov. Disord. 2001, 16, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, G.; Bain, P.; Brin, M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov. Disord. 1998, 13 (Suppl. 3), 2–23. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Smith, E.G.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment: Clinical Characterization and Outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Fahn, S.; Tolosa, E.; Concepcion, M. Clinical Rating Scale for Tremor. In Parkinson’s Disease and Movement Disorders; Jankovic, J., Tolosa, E., Eds.; Williams & Wilkins: Philadelphia, PA, USA, 1993. [Google Scholar]
- Horn, A.; Li, N.; Dembek, T.A.; Kappel, A.; Boulay, C.; Ewert, S.; Tietze, A.; Husch, A.; Perera, T.; Neumann, W.J.; et al. Lead-DBS v2: Towards a comprehensive pipeline for deep brain stimulation imaging. Neuroimage 2019, 184, 293–316. [Google Scholar] [CrossRef] [PubMed]
- Dembek, T.A.; Roediger, J.; Horn, A.; Reker, P.; Oehrn, C.; Dafsari, H.S.; Li, N.; Kühn, A.A.; Fink, G.R.; Visser-Vandewalle, V.; et al. Probabilistic sweet spots predict motor outcome for deep brain stimulation in Parkinson disease. Ann. Neurol. 2019, 86, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Koss, A.M.; Alterman, R.L.; Tagliati, M.; Shils, J.L. Calculating total electrical energy delivered by deep brain stimulation systems. Ann. Neurol. 2005, 58, 168. [Google Scholar] [CrossRef]
- Huang, H.; Yang, X.; Zhao, Q.; Ning, P.; Shen, Q.; Wang, H.; Xie, D.; Lu, H.; Xu, Y. Clinical characteristics of patients with essential tremor or essential tremor plus. Acta Neurol. Scand. 2020, 141, 335–341. [Google Scholar] [CrossRef]
- Paschen, S.; Forstenpointner, J.; Becktepe, J.; Heinzel, S.; Hellriegel, H.; Witt, K.; Helmers, A.-K.; Deuschl, G. Long-term efficacy of deep brain stimulation for essential tremor: An observer-blinded study. Neurology 2019, 92, e1378–e1386. [Google Scholar] [CrossRef] [PubMed]
- Herzog, J.; Hamel, W.; Wenzelburger, R.; Pötter, M.; Pinsker, M.O.; Bartussek, J.; Morsnowski, A.; Steigerwald, F.; Deuschl, G.; Volkmann, J. Kinematic analysis of thalamic versus subthalamic neurostimulation in postural and intention tremor. Brain 2007, 130, 1608–1625. [Google Scholar] [CrossRef]
- Barbe, M.T.; Liebhart, L.; Runge, M.; Deyng, J.; Florin, E.; Wojtecki, L.; Schnitzler, A.; Allert, N.; Sturm, V.; Fink, G.R.; et al. Deep brain stimulation of the ventral intermediate nucleus in patients with essential tremor: Stimulation below intercommissural line is more efficient but equally effective as stimulation above. Exp. Neurol. 2011, 230, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Sandvik, U.; Koskinen, L.-O.; Lundquist, A.; Blomstedt, P. Thalamic and Subthalamic Deep Brain Stimulation for Essential Tremor: Where Is the Optimal Target? Neurosurgery 2012, 70, 840–846. [Google Scholar] [PubMed]
- Barbe, M.T.; Franklin, J.; Kraus, D.; Reker, P.; Dembek, T.A.; Allert, N.; Wirths, J.; Voges, J.; Timmermann, L.; Visser-Vandewalle, V. Deep brain stimulation of the posterior subthalamic area and the thalamus in patients with essential tremor: Study protocol for a randomized controlled pilot trial. Trials 2016, 17. [Google Scholar] [CrossRef] [PubMed]
- Hariz, M.I.; Shamsgovara, P.; Johansson, F.; Hariz, G.-M.; Fodstad, H. Tolerance and Tremor Rebound following Long-Term Chronic Thalamic Stimulation for Parkinsonian and Essential Tremor. Stereotact. Funct. Neurosurg. 2000, 72, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Ondo, W.; Jimenez-Shahed, J. Habituation and rebound to thalamic deep brain stimulation in long-term management of tremor associated with demyelinating neuropathy. Int. J. Neurosci. 2014, 124, 919–925. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pat-ID | Sex | Age (y) | DD (y); FU (m) | Syndrome | Plus-Sign | BL-TRS | OFF-TRS | ON-TRS | % (BL) | % (OFF) | Clinical Stimulation Settings Left Hemisphere | Clinical Stimulation Settings Right Hemisphere |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | f | 78 | 9; 11 | ET | - | 27 | - | 9 | 66.67 | - | C+, 0–100%, 60 µs, 130 Hz, 2.5 mA | C+, 8–100%, 60 µs, 130 Hz, 1 mA |
| 2 | m | 67 | 37; 54 | ET | - | 16 | 20 | 5 | 68.75 | 75 | C+, 2–50%, 4–50%, 60 µs, 223 Hz, 2.5 mA | C+, 10–50%, 12–50%, 60 µs, 223 Hz, 2.2 mA |
| 3 | m | 71 | 39; 10 | ET | - | 22 | 21 | 3 | 86.36 | 85.71 | C+, 5–34%, 6–33%, 7–33%; 60 µs; 174 Hz; 2 mA | C+, 10–24%, 11–23%, 12–23%, 13–10%, 14–10%, 15–10%; 60 µs; 130 Hz; 1.3 mA |
| 4 | m | 26 | 9; 18 | ET | - | 14 | 3 | 1 | 92.86 | 66.67 | C+, 3–100%, 60 µs, 174 Hz, 1.3 mA | C+, 11–100%, 60 µs, 174 Hz, 0.7 mA |
| 5 | m | 56 | 46; 26 | ET | - | 17 | 71 | 9 | 47.06 | 87.32 | C+, 3–100%, 60 µs, 130 Hz, 3 mA | C+, 11–100%, 60 µs, 174 Hz, 2 mA |
| 6 | m | 72 | 11; 6 | ET | - | 26 | 19 | 3 | 88.46 | 84.21 | C+, 1–100%, 60μs, 130 Hz, 1.1 mA | C+, 9–100%, 60μs, 130 Hz, 1 mA |
| 7 | m | 64 | 32; 6 | ET | - | - | 23 | 7 | - | 69.57 | C+, 0–100%, 60 µs, 130 Hz, 2.0 V | C+, 8–100%, 60 µs, 130 Hz, 1.8 V |
| 8 | m | 68 | 30; 61 | ET | - | - | 33 | 14 | - | 57.58 | C+, 0–50%, 1–50%, 90μs, 150 Hz, 2 V | C+, 10–100%, 90μs, 150 Hz, 2.2 V |
| 9 | m | 60 | 44; 3 | ET | - | - | 30 | 18 | - | 40.0 | C+, 1–100%, 60 µs, 130 Hz, 1.6 mA | C+, 9–100%, 60 µs, 130 Hz, 1.7 mA |
| 10 | m | 53 | 44; 3 | ET | - | - | 17 | 7 | - | 58.82 | C+, 2–34%, 3–33%, 4–33%, 60 µs, 130 Hz, 1.4 mA | C+, 10–34%,11–33%, 12–33%, 60 µs, 130 Hz, 0.7 mA |
| 11 | m | 48 | 34; 67 | ET | - | - | 8 | 3 | - | 62.5 | VIM 1: C+, 1–0.3 V, 60μs, 120 Hz VIM 2:2–1.1 V, 60μs, 120 Hz | C+, 9–50%, 10–50%, 60μs, 120 Hz, 1.3 V |
| 12 | m | 62 | 29; 67 | ET | - | - | 35 | 6 | - | 82.86 | VIM 1: C+, 0–3.1 V, 60μs, 120 Hz VIM 2: C+, 1–1.3 V, 60 μs, 120 Hz | VIM 1: C+, 9–2.1 V, 60 μs, 120 Hz VIM 2:10–2.8 V, 60 μs, 120 Hz |
| 13 | m | 54 | 45; 18 | ET | - | - | 30 | 13 | - | 56.67 | C+, 2–34%, 3–33%, 4–33%, 204 Hz, 50 µs, 1.3 mA | C+, 10–34%, 11–33%, 12–33%, 204 Hz, 50 µs, 1.7 mA |
| 14 | f | 72 | 61; 12 | ET-p | RT | 34 | - | 3 | 91.18 | - | C+, 0–100%, 60 µs, 130 Hz, 2.2 V | C+, 8–100%, 60 µs, 130 Hz, 2.4 V |
| 15 | m | 22 | 13; 11 | ET-p | Dystonia, MCI | 51 | - | 21 | 58.82 | - | C+, 3–30% 4–60% 5–10%, 60 µs 174 Hz, 5.7 mA | C+, 11–25% 12–75%, 60 µs 174 Hz, 4 mA |
| 16 | f | 61 | 15; 11 | ET-p | RT, MCI | 37 | - | 20 | 45.95 | - | C+, 2–100%, 60 us, 130 Hz, 3.9 mA | C+, 10–100%, 60 us, 130 Hz, 3.9 mA |
| 17 | m | 60 | 29; 10 | ET-p | Dystonia | 21 | 32 | 10 | 52.38 | 68.75 | C+, 1–30%, 2–35%, 3–35%, 60 µs, 130 Hz, 1.9 mA | C+, 13–33%, 14–33%, 15–34%, 60 µs, 130 Hz, 1.6 mA |
| 18 | m | 66 | 16; 9 | ET-p | RT | 33 | 58 | 28 | 15.15 | 51.72 | C+, 1–100%, 60 µs, 208 Hz, 4.2 mA | C+, 11–100%, 60 µs, 208 Hz, 2.5 mA |
| 19 | m | 66 | 49; 43 | ET-p | Dystonia | 46 | 48 | 14 | 69.57 | 70.83 | C+, 3–100%, 60 µs, 130 Hz, 3.8 mA | C+, 11-, 100%, 60 µs, 130 Hz, 2.9 mA |
| 20 | f | 61 | 60; 4 | ET-p | MCI | 17 | 26 | 11 | 35.29 | 57.69 | C+, 2–100%, 60 μs, 130 Hz, 6.5 mA | C+, 10–100%, 60 μs, 130 Hz, 4 mA |
| 21 | m | 70 | 29; 5 | ET-p | RT, MCI | 16 | 21 | 11 | 31.25 | 47.62 | C+; 1–100%, 60 μs, 130 Hz, 1 mA | C+, 9–100%, 60 μs, 130 Hz, 1 mA |
| 22 | f | 63 | 21; 3 | ET-p | MCI | 15 | 20 | 4 | 73.33 | 80.0 | C+, 1–100%, 60 µs, 130 Hz, 1.4 mA | C+, 9–100%, 60 µs, 130 Hz, 1.2 mA |
| 23 | f | 77 | 27; 8 | ET-p | RT, MCI | 34 | 42 | 7 | 79.41 | 83.33 | C+, 1–62%, 2–14%, 3–12%, 4–12%, 50 µs, 174 Hz, 1.8 mA | C+, 9–75%, 10–9%, 11–8%, 12–8%, 50 µs, 174 Hz, 1.7 mA |
| 24 | f | 68 | 31; 31 | ET-p | RT, Ataxia | 18 | 25 | 6 | 66.67 | 76.0 | 2–70%, 3–30%, 5 + 100%, 60 µs, 174 Hz, 2.0 mA | 10–70%, 11–30%, 13 + 100%, 60 µs, 174 Hz, 2.0 mA |
| 25 | f | 70 | 56; 38 | ET-p | RT | - | 64 | 39 | - | 39.06 | C+, 1–100%, 60 us, 185 Hz, 2.8 mA | C+, 9–100%, 60 us, 185 Hz, 2.8 mA |
| 26 | m | 52 | 41; 98 | ET-p | MCI | - | 51 | 13 | - | 74.51 | C+, 1–100%, 60 µs, 200 Hz, 2.0 V | C+, 9–100%m, 60 µs, 200 Hz, 3.3 V |
| 27 | m | 77 | 16; 13 | ET-p | RT | - | 41 | 18 | - | 56.1 | C+, 1–100%, 60 µs, 200 Hz, 2.0 V | C+, 9–100%m, 60 µs, 200 Hz, 3.3 V |
| 28 | f | 75 | 10; 28 | ET-p | RT | - | 41 | 2 | - | 95.12 | C+, 2–100%, 60 µs, 125 Hz, 3.2 mA | VIM 1: C+, 8–50% 9–50%, 60 µs, 125 Hz, 3.6 mA Vim 2: C+, 9–100%, 60 µs, 125 Hz, 3.2 mA |
| 29 | m | 64 | 5; 15 | ET-p | Ataxia | - | 53 | 36 | - | 32.08 | 5 + 34%. 6 + 33%, 7 + 33%, 1–90%, 2–5%, 4–5% 40 µs, 204 Hz, 5 mA | 13 + 34%, 14 + 33%, 15 + 33%, 9–80%, 11–10%, 40 µs, 204 Hz, 4.7 mA |
| 30 | f | 65 | 24; 12 | ET-p | Ataxia | - | 33 | 5 | - | 84.85 | C+, 2–21%, 3–5%, 4–29%, 5–17%,6–5%,7–23%, 60 µs, 149 Hz, 2.3 mA | C+, 10–17%, 11–26%, 12–27%, 13–10%, 14–10%, 15–10%, 60 µs, 149 Hz, 2.3 mA |
| 31 | m | 58 | 11; 12 | ET-p | MCI | - | 47 | 22 | - | 53.19 | C+, 0–100%, 60 µs, 130 Hz, 3.3 V | C+, 8–100%, 60 µs, 130 Hz, 3.3 V |
| 32 | m | 69 | 6; 111 | ET-p | RT | - | 64 | 36 | - | 43.75 | C+, 0–100%, 60 µs, 180 Hz, 3.5 V | C+, 8–100%, 60 µs, 180 Hz, 3.1 V |
| 33 | f | 57 | 43; 32 | ET-p | Dystonia | - | 58 | 0 | - | 100.0 | VIM 1:C+; 2–100%, 2.4 V 90μs, 120 Hz VIM 2:3–100%, 90μs, 120 Hz, 1.8 V | C+, 10–100%, 60μs, 120 Hz, 2.8 V |
| 34 | m | 79 | 3; 37 | ET-p | MCI | - | 58 | 13 | - | 48.0 | C+, 1–100%, 80 µs, 149 Hz, 2.7 mA | C+, 9–100%, 60 µs, 149 Hz, 2.1 mA |
| 35 | m | 63 | 13; 17 | ET-p | Dystonia, ataxia | - | 54 | 7 | - | 87.04 | C+ 10%, 1–100%, 2 + 30%, 3 + 30%, 4 + 30%, 50 µs, 179 Hz, 2.8 mA | C+ 20%, 12–60%, 15–40%, 10 + 19%, 11 + 19%, 13 + 21%, 14 + 21%, G + 20%, 50 µs, 179 Hz, 3.5 mA |
| 36 | m | 63 | 44; 9 | ET-p | RT, dystonia | - | 52 | 28 | - | 46.15 | 1–100%, 2 + 34%, 3 + 33%, 4 + 33%, 60 µs, 179 Hz, 3.1 mA | 9–100%, 10 + 34%, 11 + 33%, 12 + 33%, 70 µs, 179 Hz, 3.4 mA |
| 37 | m | 75 | 66; 7 | ET-p | RT, MCI | - | 28 | 8 | - | 71.43 | C+, 2–34%, 3–33%, 4–33%, 60 µs, 130 Hz, 2.1 mA | C+, 2–34%, 3–33%, 4–33%, 60 µs, 130 Hz, 2.1 mA |
| 38 | m | 67 | 18; 8 | ET-p | Ataxia | - | 22 | 18 | - | 18.18 | - | - |
| 39 | f | 66 | 9; 14 | ET-p | Dystonia, MCI | - | 16 | 4 | - | 75.0 | VIM 1: C+, 8–100%, 90 µs, 125 Hz, 1.3 V VIM 2: C+, 9–100%, 90 µs, 125 Hz, 2.1 V | VIM 1: C+, 1–100%, 90 µs, 125 Hz, 2.1 V; VIM 2: C+, 0–100%, 90 µs, 125 Hz, 1.3 V |
| 40 | f | 77 | 47; 11 | ET-p | Dystonia | - | 16 | 7 | - | 56.25 | C+, 2–100%, 60 µs, 130 Hz, 3.6 mA | C+, 10–29%, 11–43%, 12–28%, 60 µs, 130 Hz, 1.9 mA |
| 41 | f | 80 | 20; 34 | ET-p | Dystonia, ataxia | - | 56 | 33 | - | 41.07 | C+, 5–32%, 6–29%, 7–29% 8–10% 40 µs 170 Hz 3.3 mA | C+, 13–45%, 14–40%, 15–15% 40 µs 170 Hz 4.1 mA |
| 42 | f | 70 | 7; 4 | ET-p | RT | - | 44 | 15 | - | 65.91 | C+, 1–100%, 60 µs, 130 Hz, 1.2 mA | C+, 9–100%, 60 µs, 130 Hz, 1.2 mA |
| 43 | m | 72 | 14; 25 | ET-p | RT | - | 64 | 25 | - | 60.94 | VIM1: C+, 2–100%, 60 us, 125 Hz, 2.9 VVIM 2: C+, 1–100%, 60 us, 125 Hz, 1.8 V | C+, 8-, 100%, 60 us, 125 Hz 3.0 |
| 44 | m | 55 | 10; 26 | ET-p | MCI | - | 39 | 0 | - | 51.28 | VIM 1: C+, 1–100%, 125 µs, 60 Hz, 0.5 V; VIM 2: C+, 2–100%, 125 µs, 60 Hz, 3.5 V | VIM1: C+, 9–100%, 125 µs, 60 Hz, 0.5 V VIM 2: C+, 10–100%, 125 µs, 60 Hz, 3.8 V |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steffen, J.K.; Jergas, H.; Petry-Schmelzer, J.N.; Dembek, T.A.; Thies, T.; Jost, S.T.; Dafsari, H.S.; Kessler, J.; Wirths, J.; Fink, G.R.; et al. Thalamic Deep Brain Stimulation in Essential Tremor Plus Is as Effective as in Essential Tremor. Brain Sci. 2020, 10, 970. https://doi.org/10.3390/brainsci10120970
Steffen JK, Jergas H, Petry-Schmelzer JN, Dembek TA, Thies T, Jost ST, Dafsari HS, Kessler J, Wirths J, Fink GR, et al. Thalamic Deep Brain Stimulation in Essential Tremor Plus Is as Effective as in Essential Tremor. Brain Sciences. 2020; 10(12):970. https://doi.org/10.3390/brainsci10120970
Chicago/Turabian StyleSteffen, Julia K., Hannah Jergas, Jan N. Petry-Schmelzer, Till A. Dembek, Tabea Thies, Stefanie T. Jost, Haidar S. Dafsari, Josef Kessler, Jochen Wirths, Gereon R. Fink, and et al. 2020. "Thalamic Deep Brain Stimulation in Essential Tremor Plus Is as Effective as in Essential Tremor" Brain Sciences 10, no. 12: 970. https://doi.org/10.3390/brainsci10120970
APA StyleSteffen, J. K., Jergas, H., Petry-Schmelzer, J. N., Dembek, T. A., Thies, T., Jost, S. T., Dafsari, H. S., Kessler, J., Wirths, J., Fink, G. R., Visser-Vandewalle, V., & Barbe, M. T. (2020). Thalamic Deep Brain Stimulation in Essential Tremor Plus Is as Effective as in Essential Tremor. Brain Sciences, 10(12), 970. https://doi.org/10.3390/brainsci10120970