Palpreast—A New Wearable Device for Breast Self-Examination

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
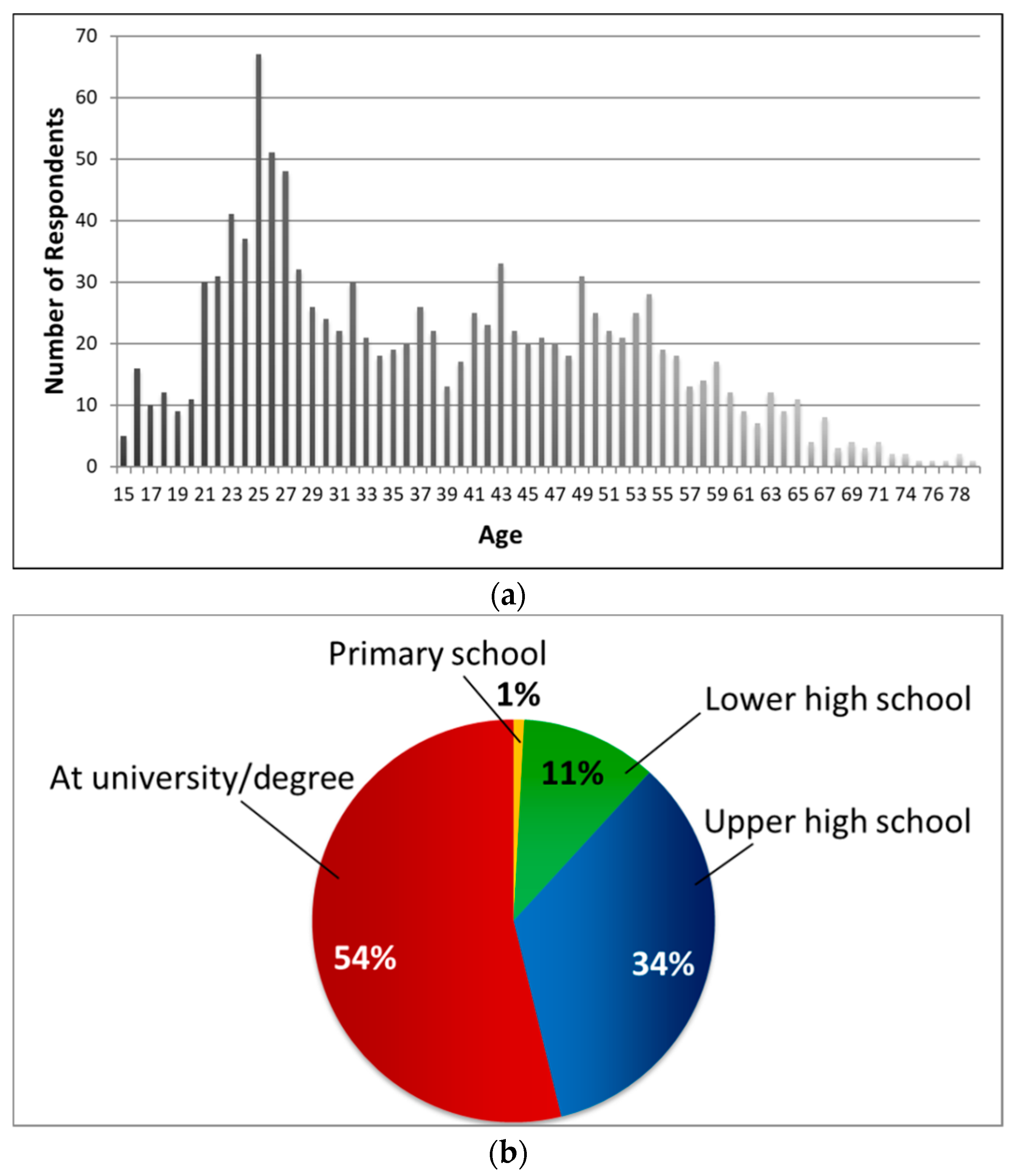
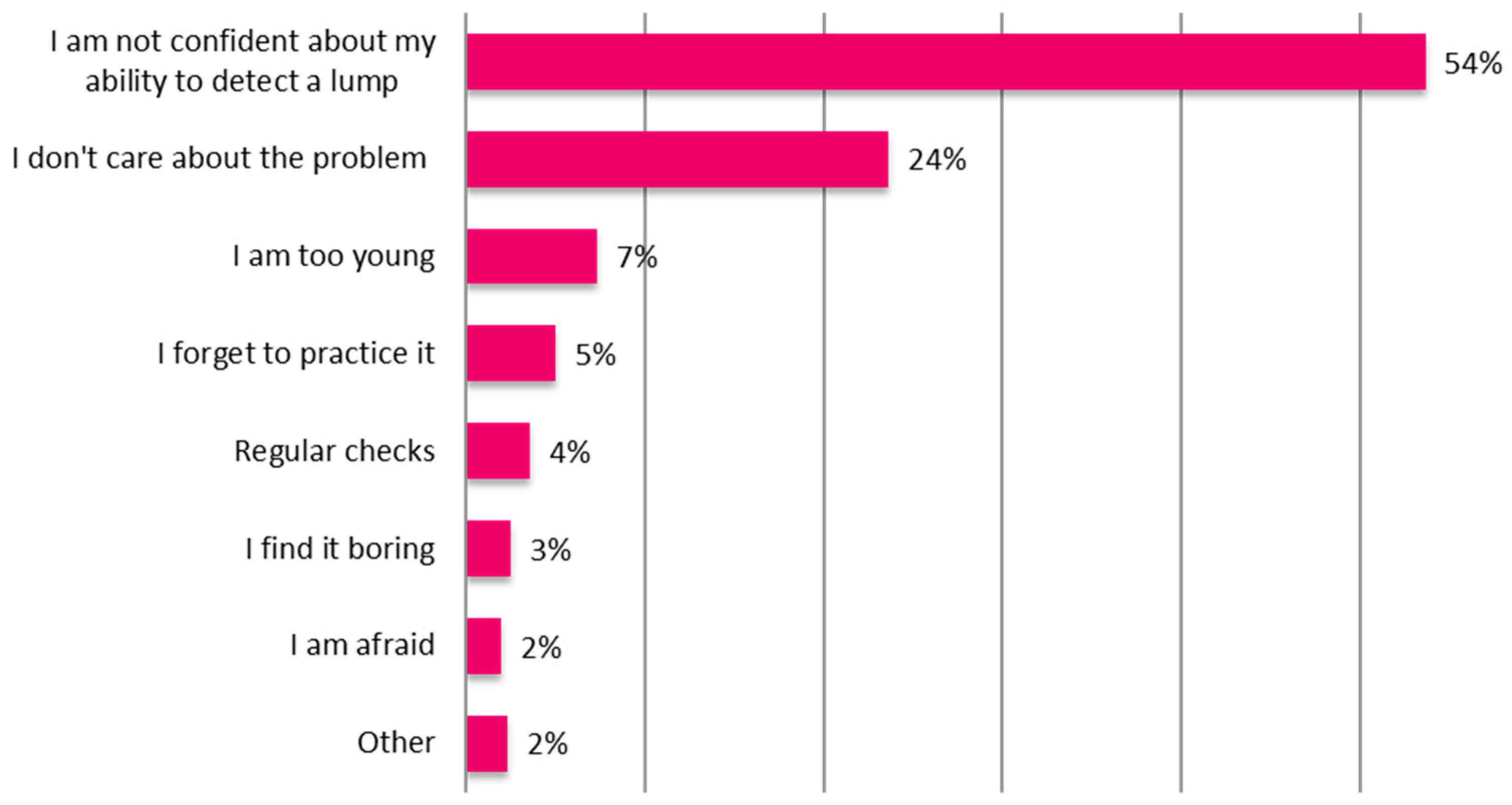
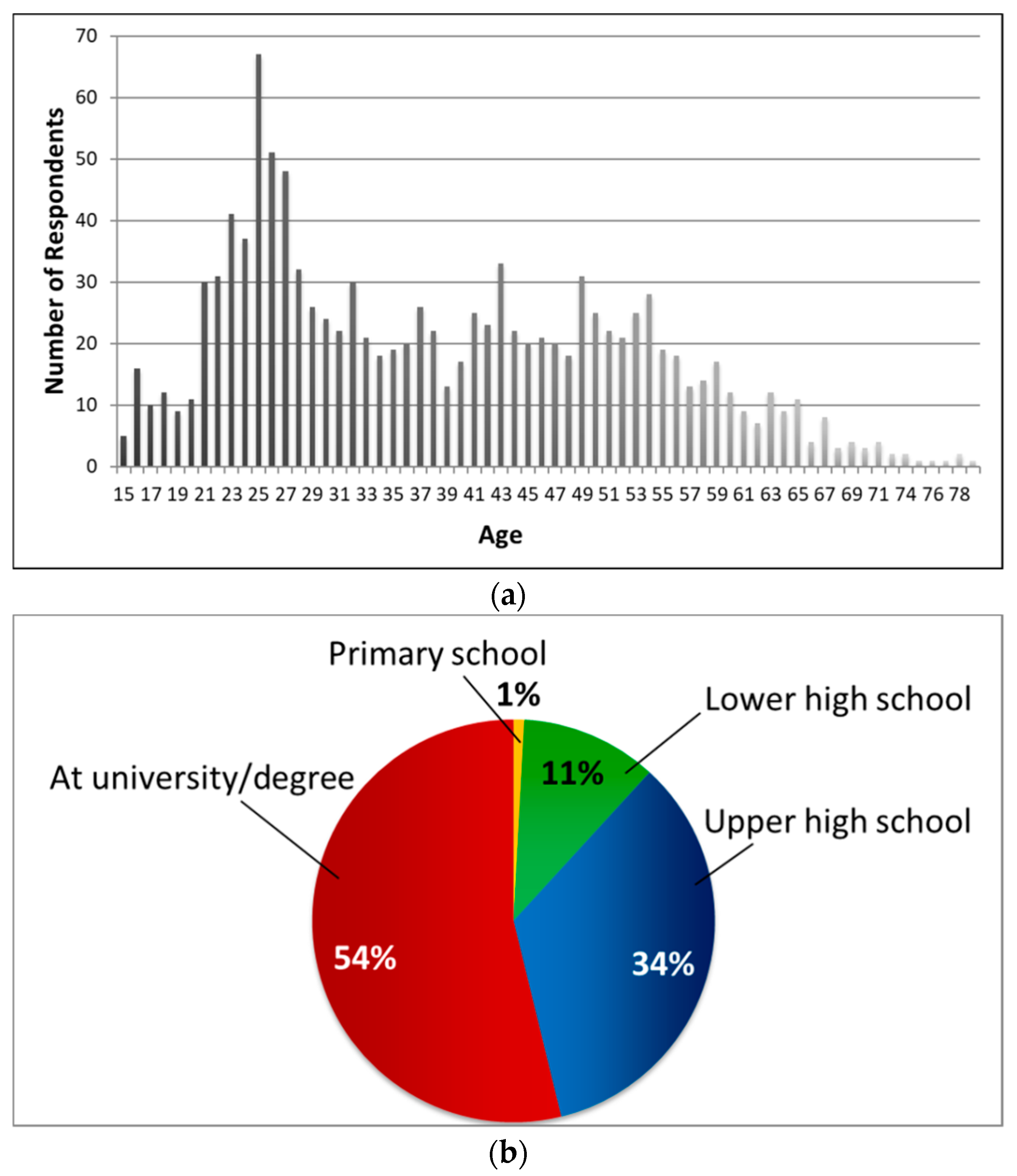
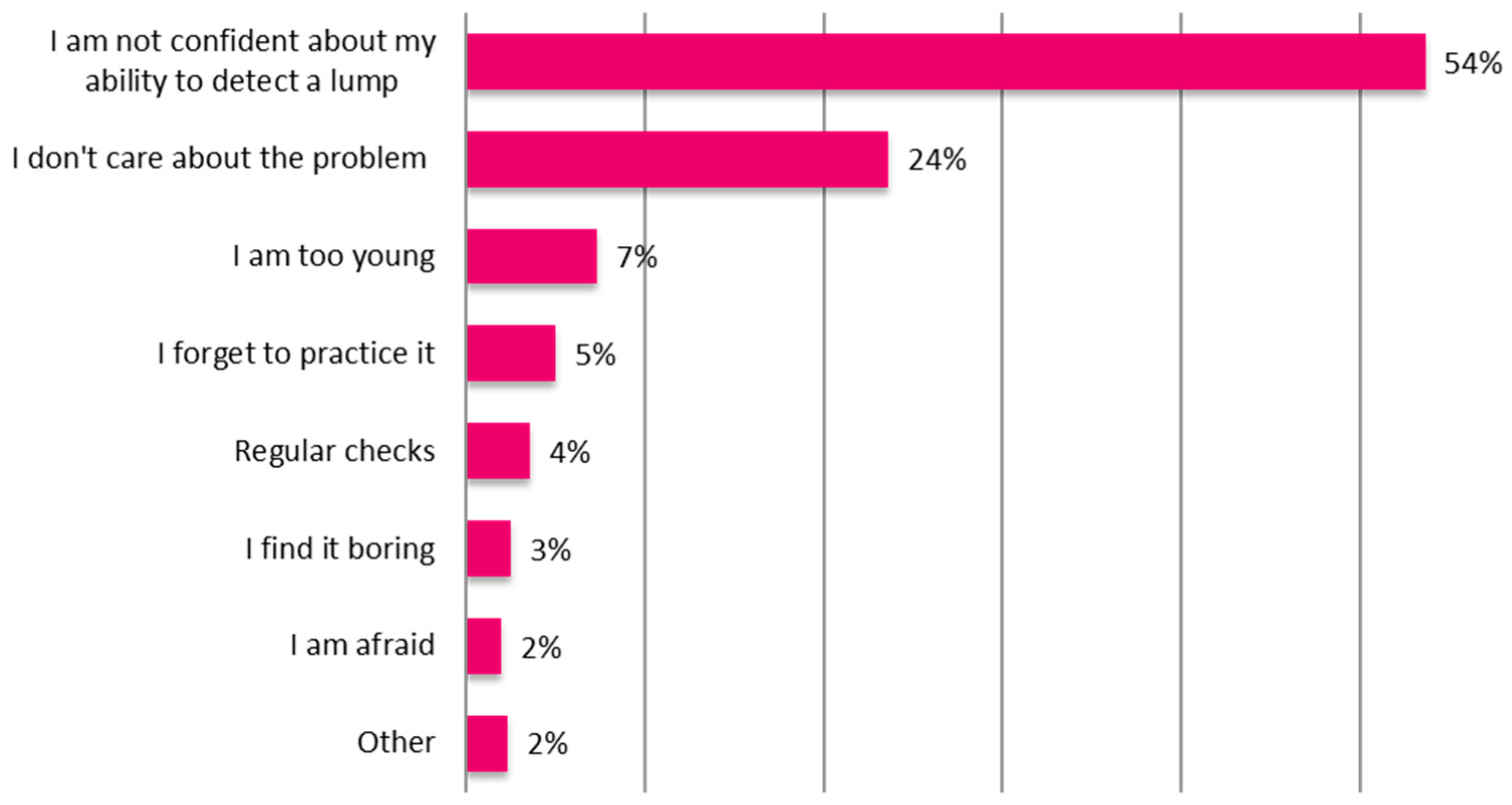
2. Survey
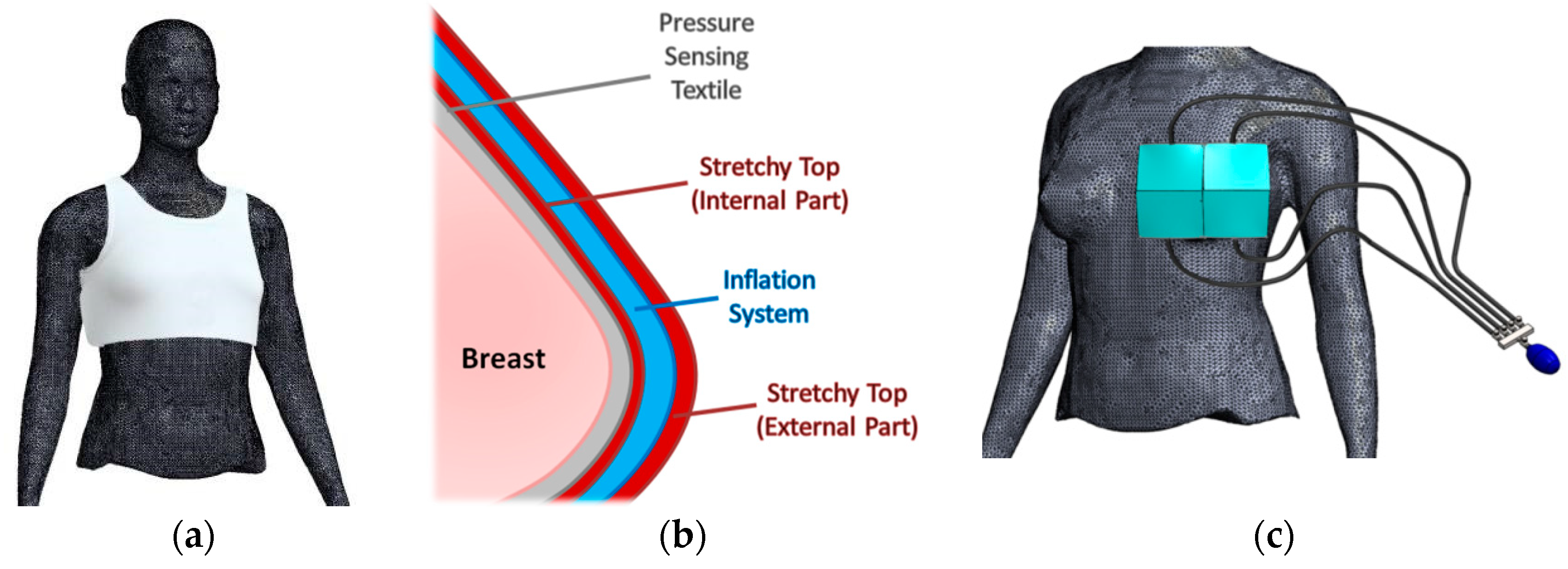
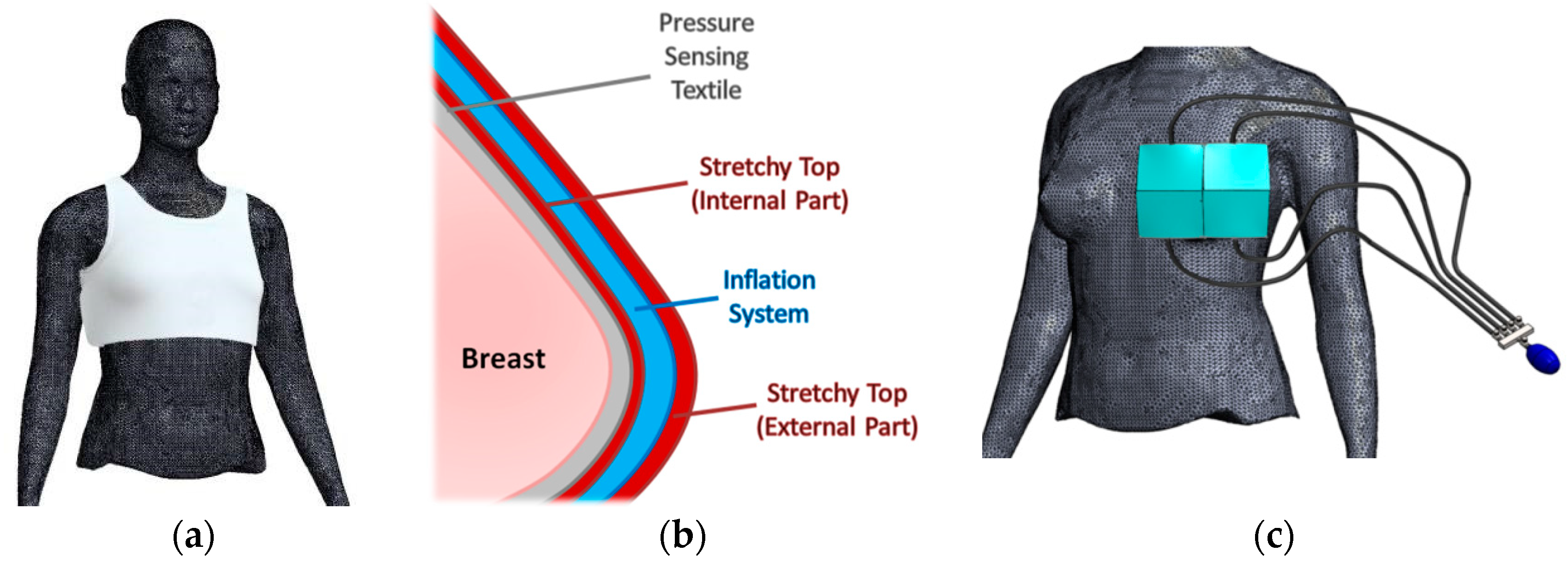
3. Device Concept
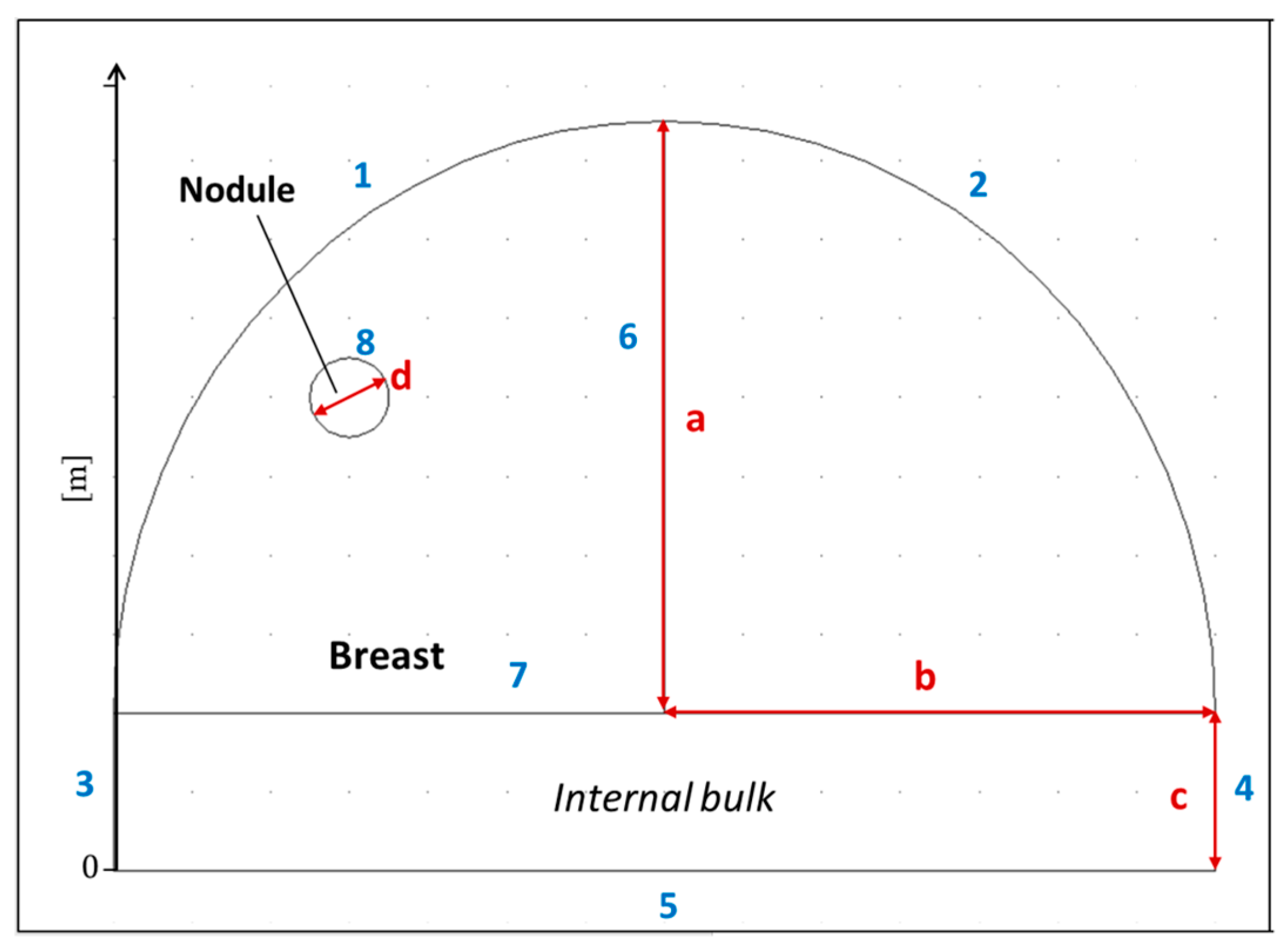
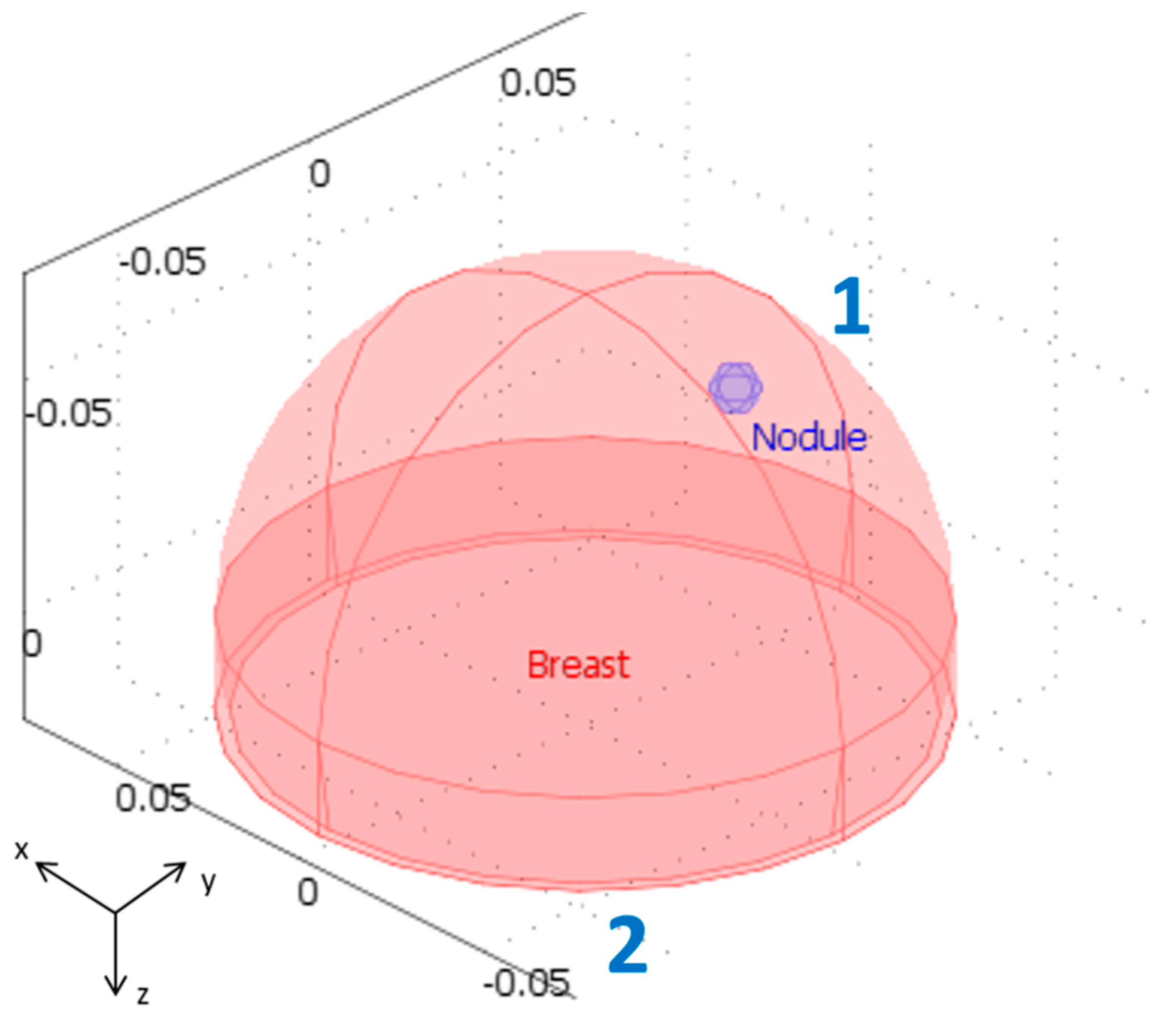
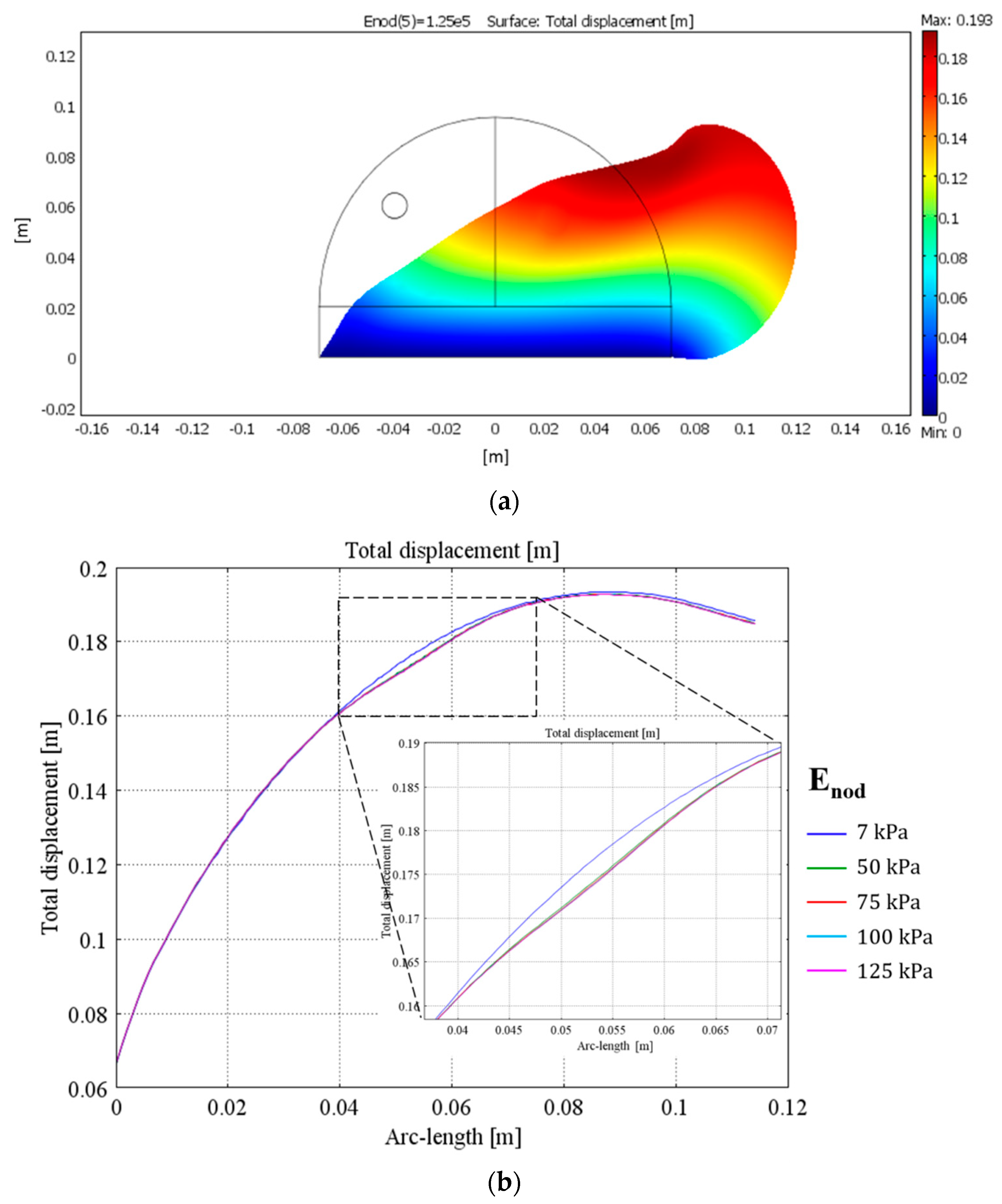
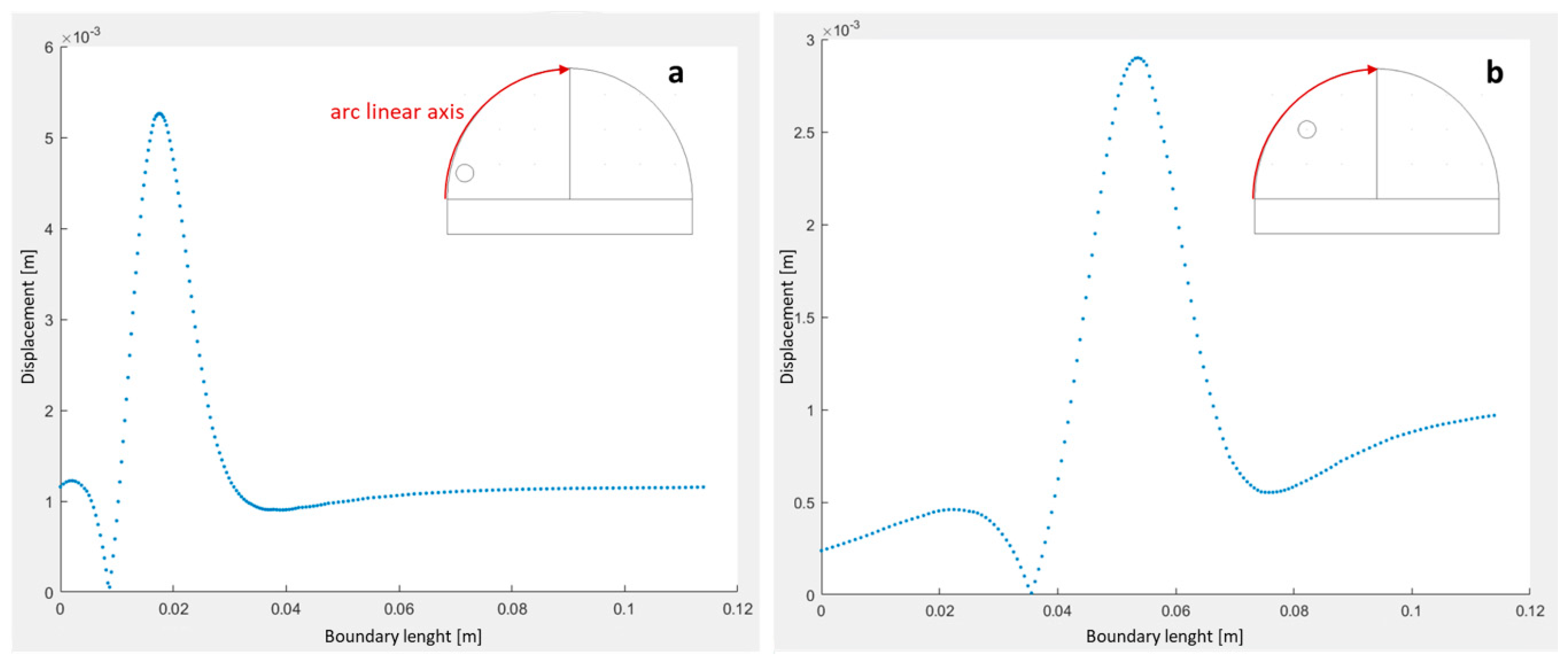
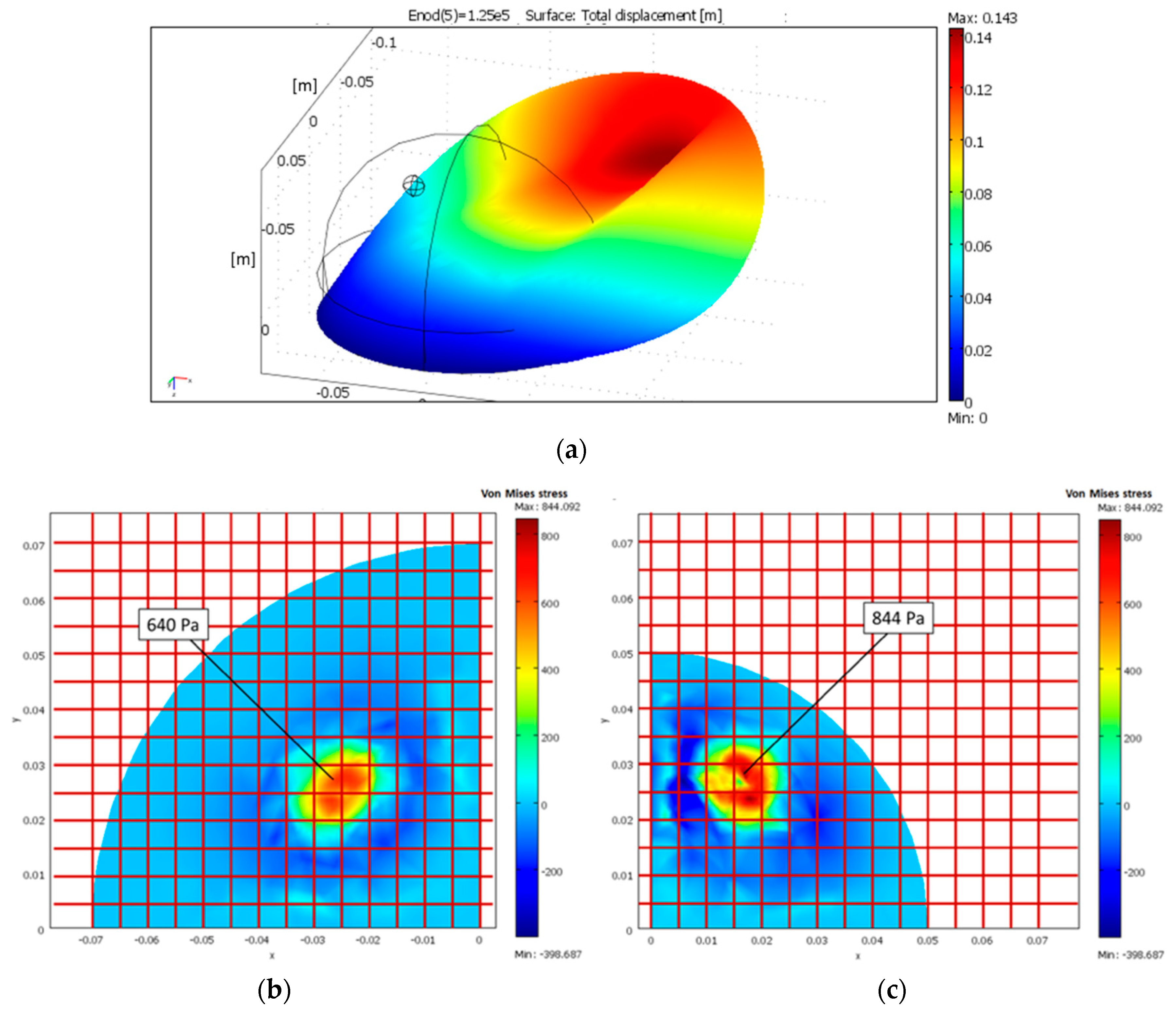
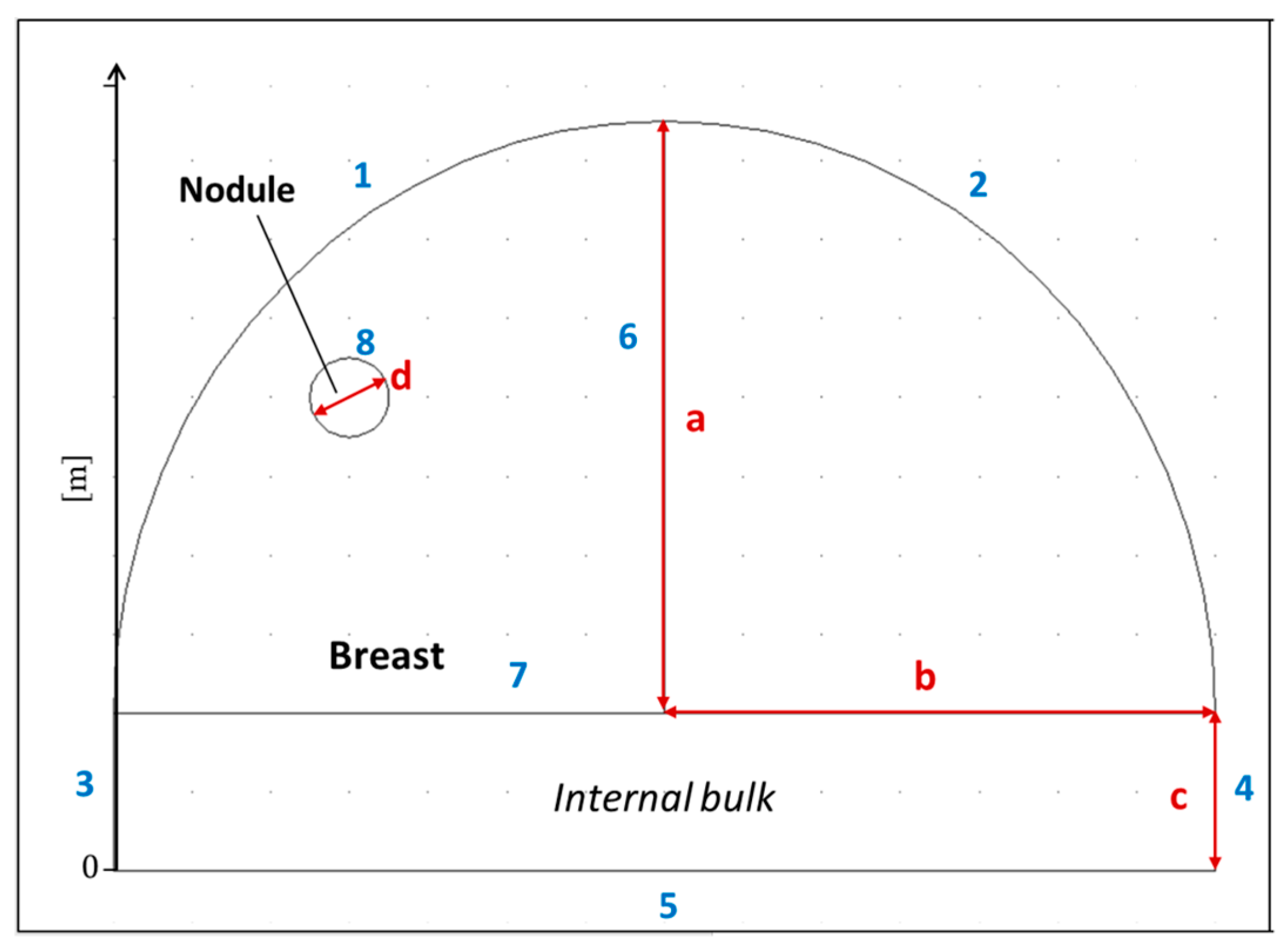
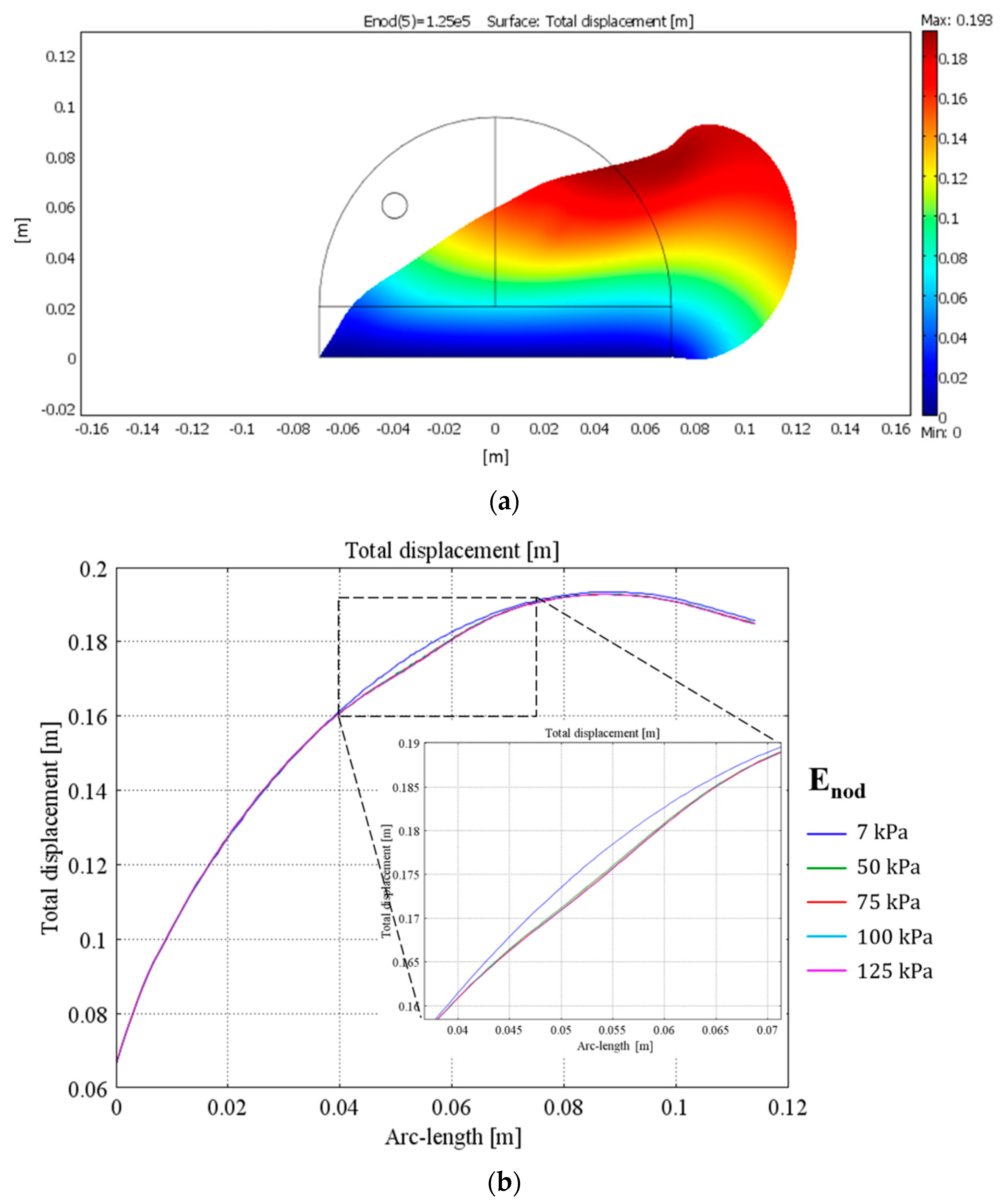
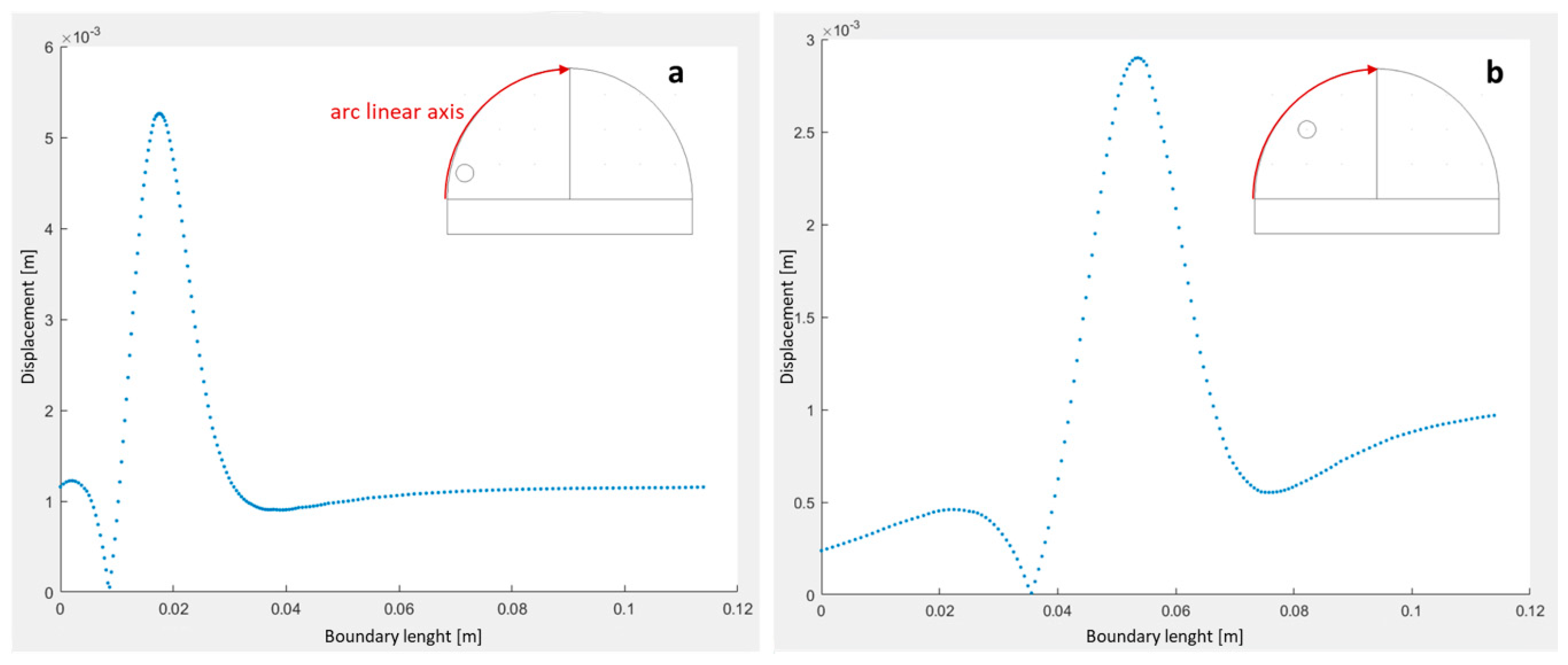
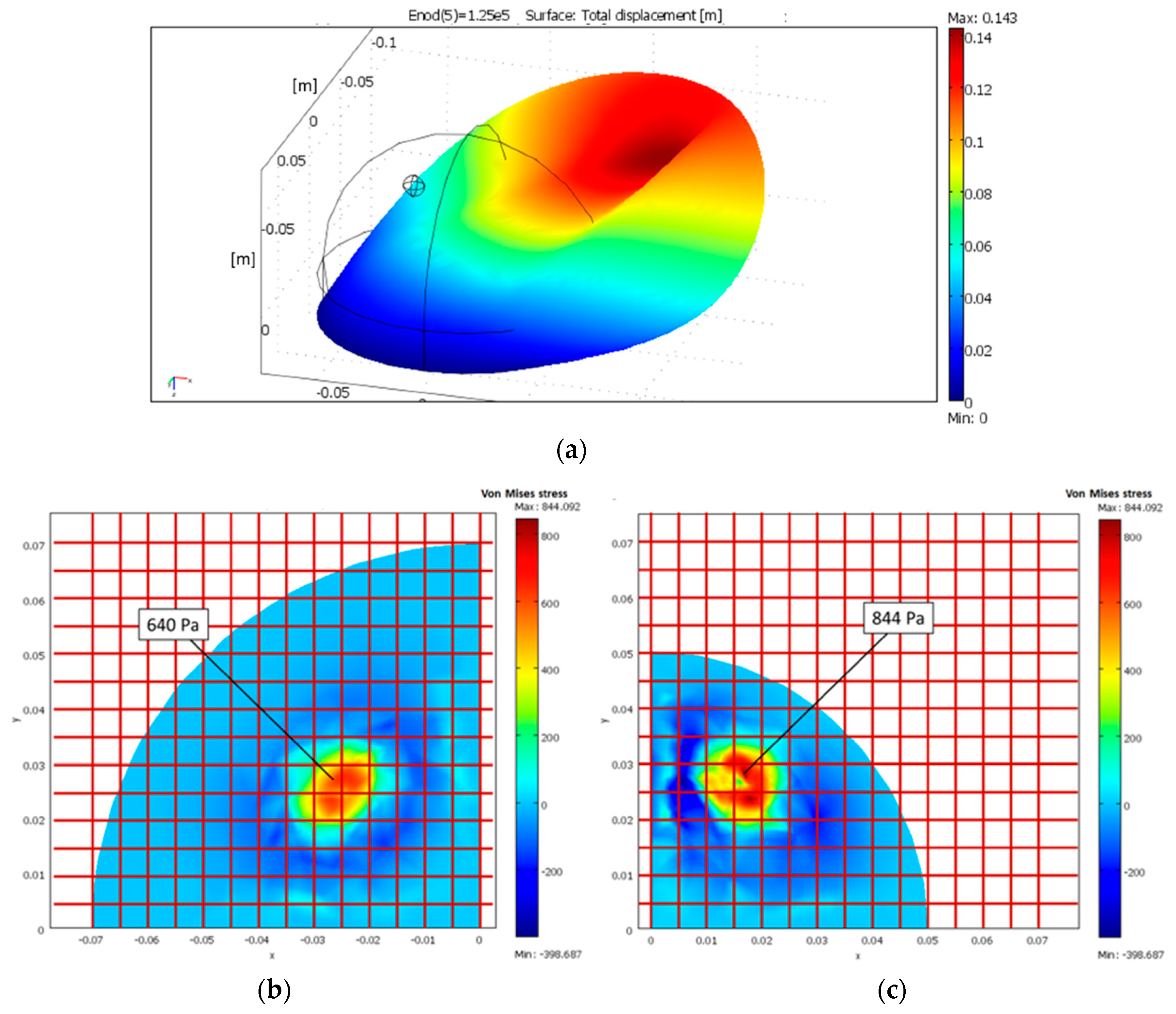
4. Finite Element Analysis
- The biological tissue and inclusions were homogeneous, linear elastic, and isotropic;
- The Poisson’s ratio of each material is 0.45, i.e., the breast could be considered as an almost incompressible material;
- The breast was assumed to be placed on a non-deformable hard surface (identifiable with the rib cage), with a no-displacement constraint as boundary condition;
- The density of each material was set to 1000 kg/m3 (close to the density of water);
- Two different breast sizes were investigated—large breast (LB) and medium breast (MB);
- A pressure of 10 kPa was considered to simulate breast palpation.
5. Device Implementation
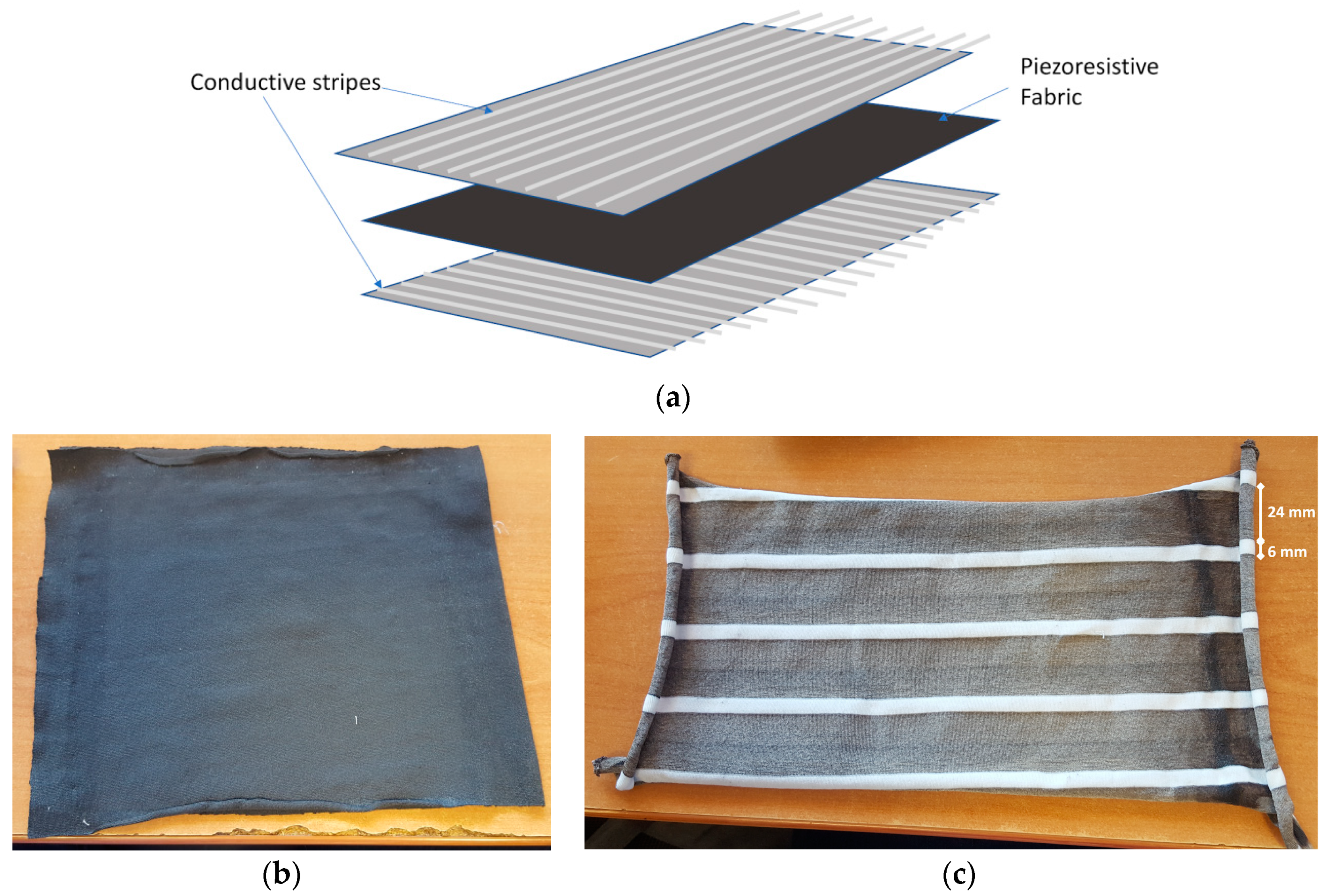
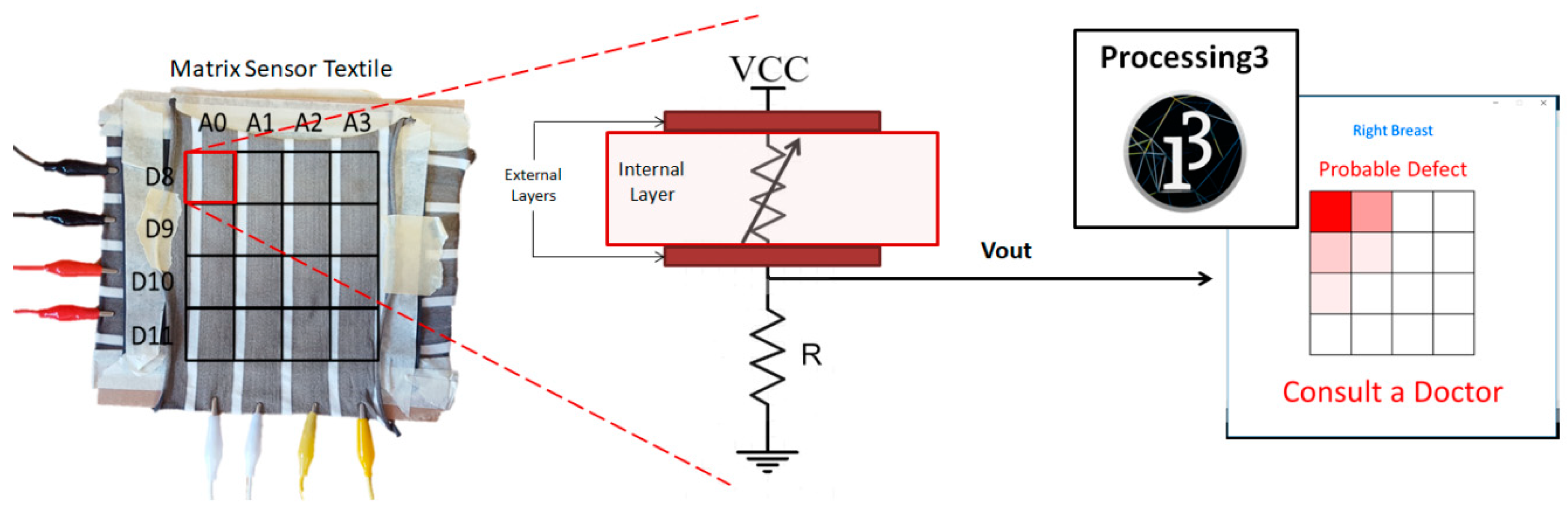
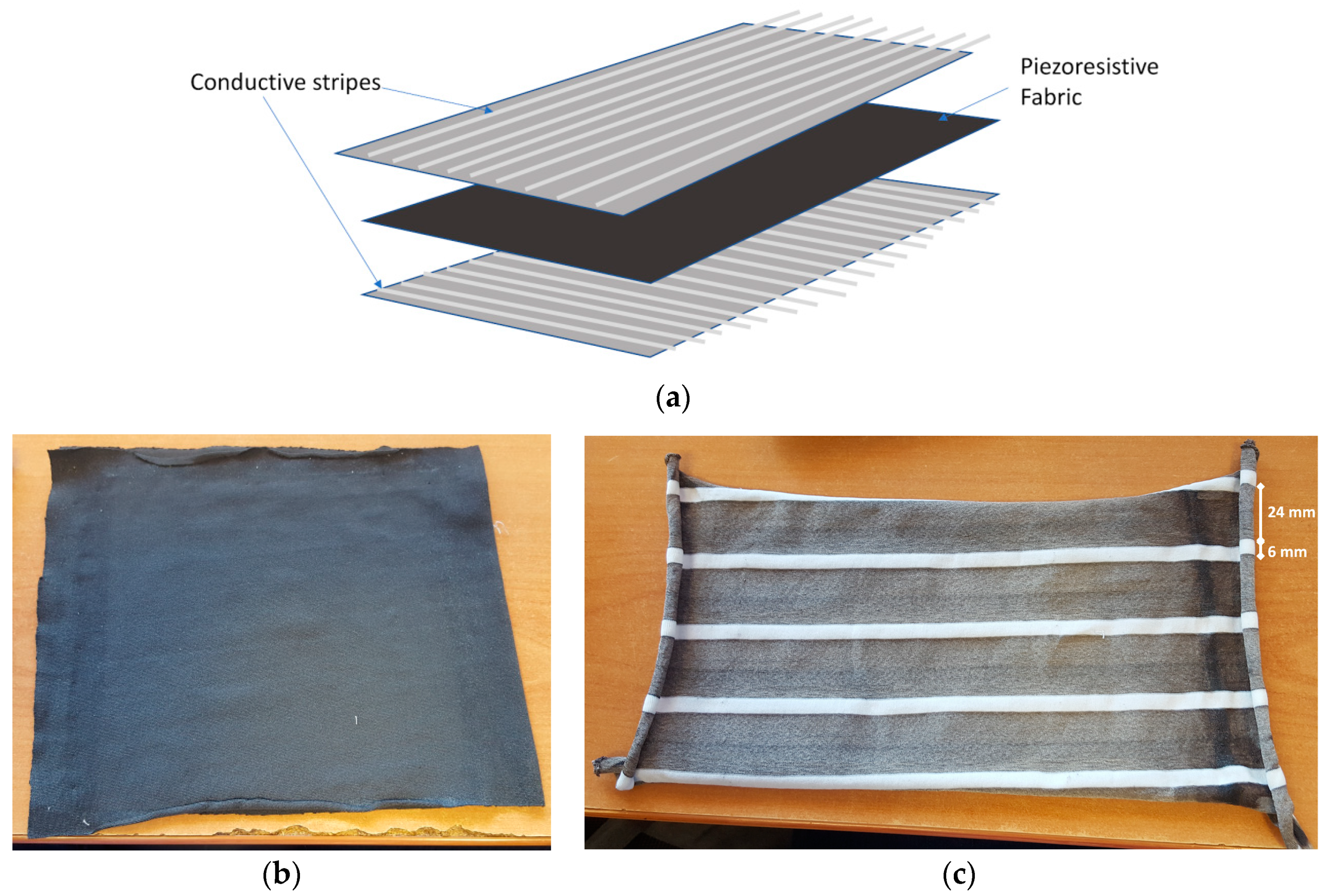
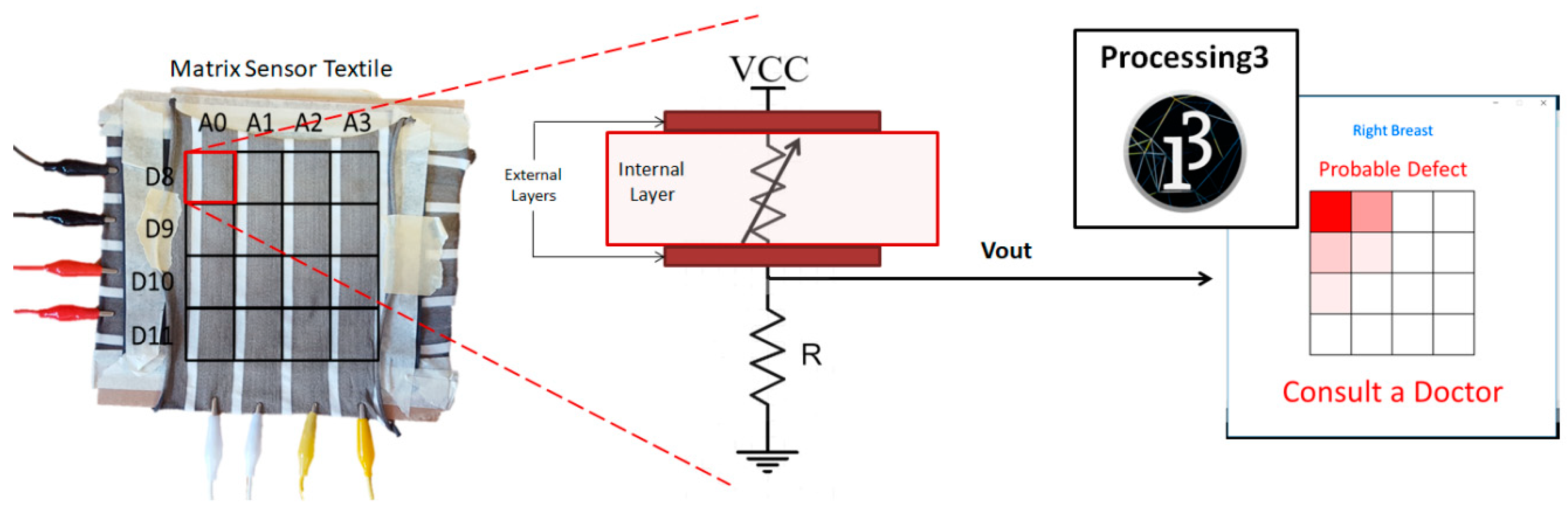
5.1. Textile Pressure Sensing Matrix
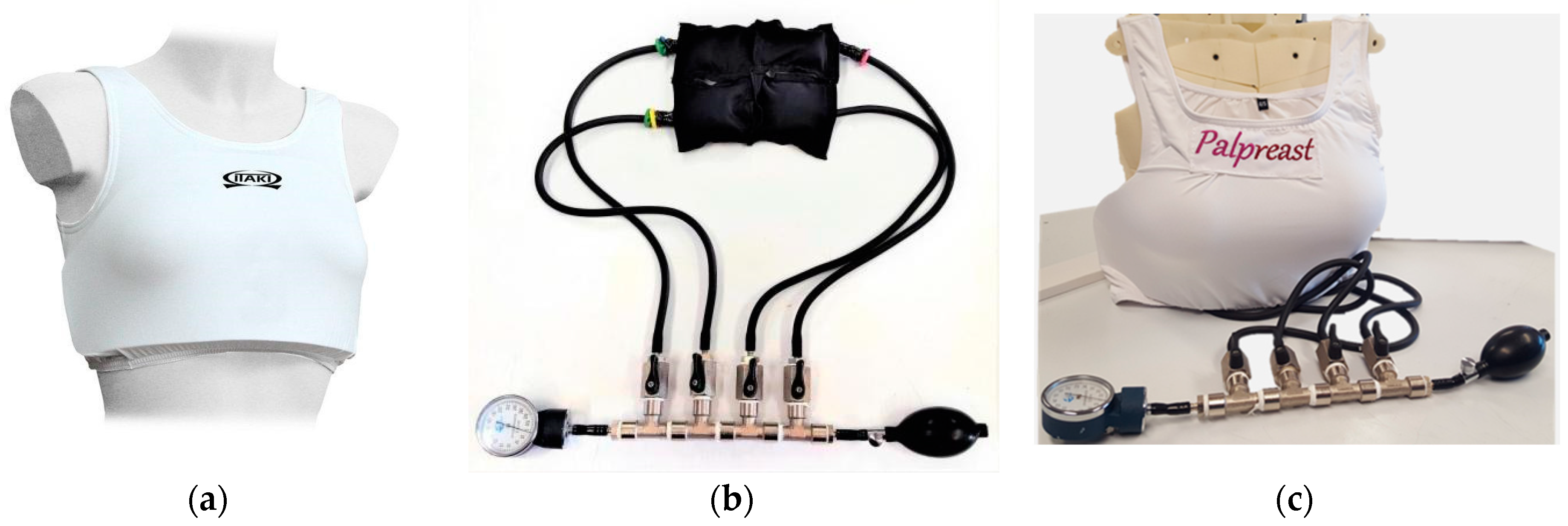
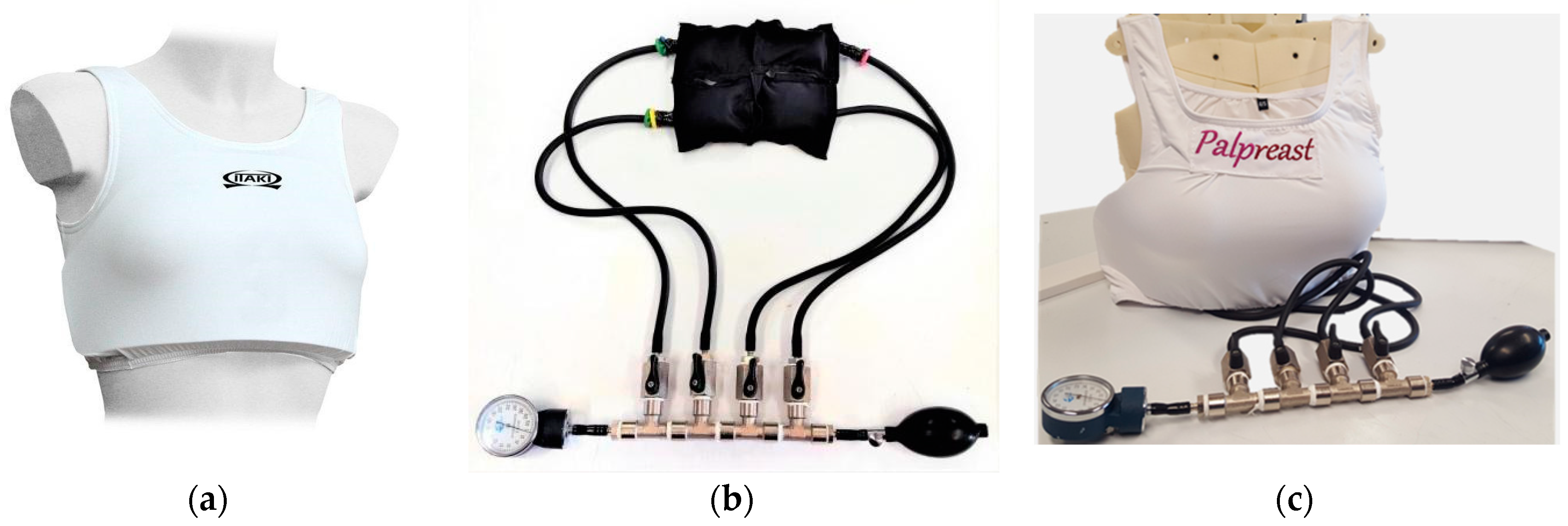
5.2. Actuation System
6. Device Characterization
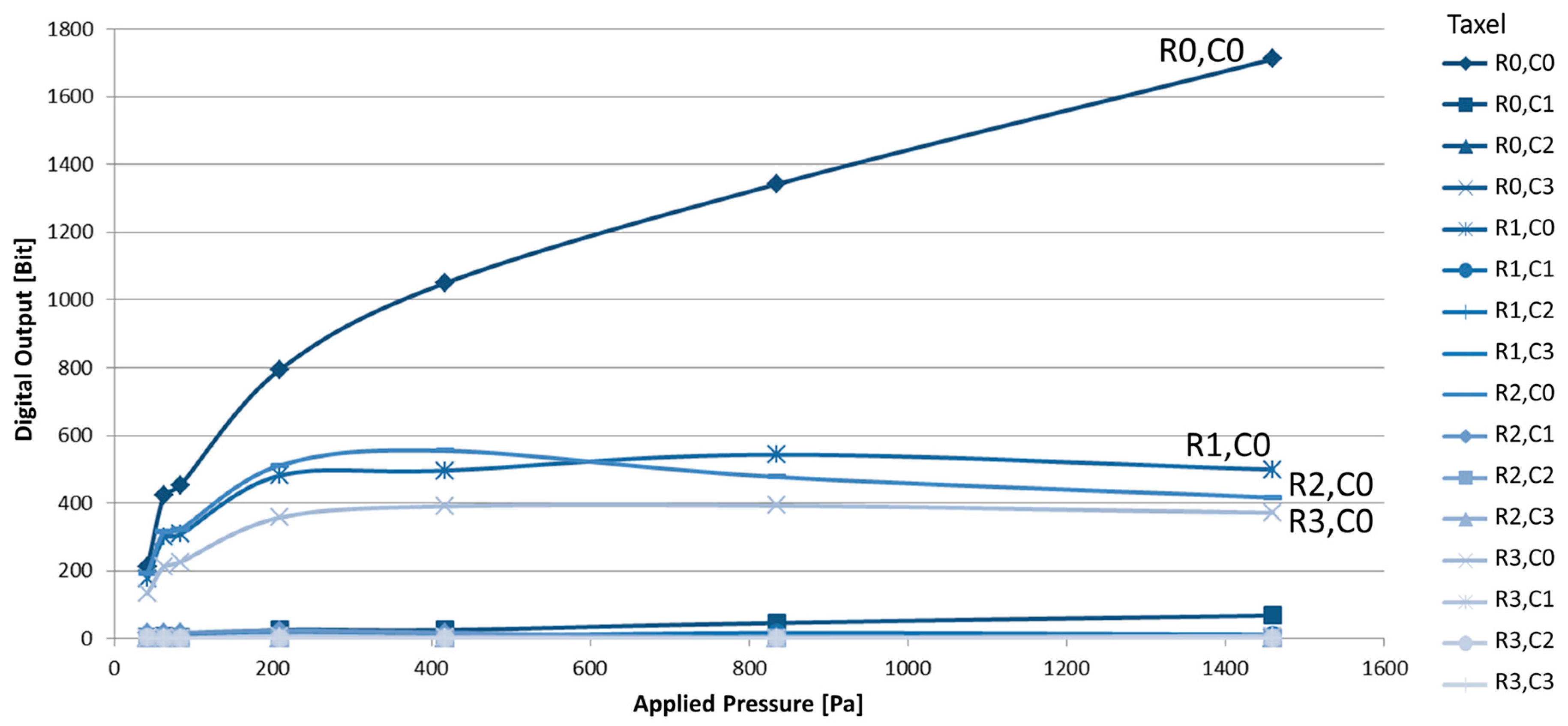
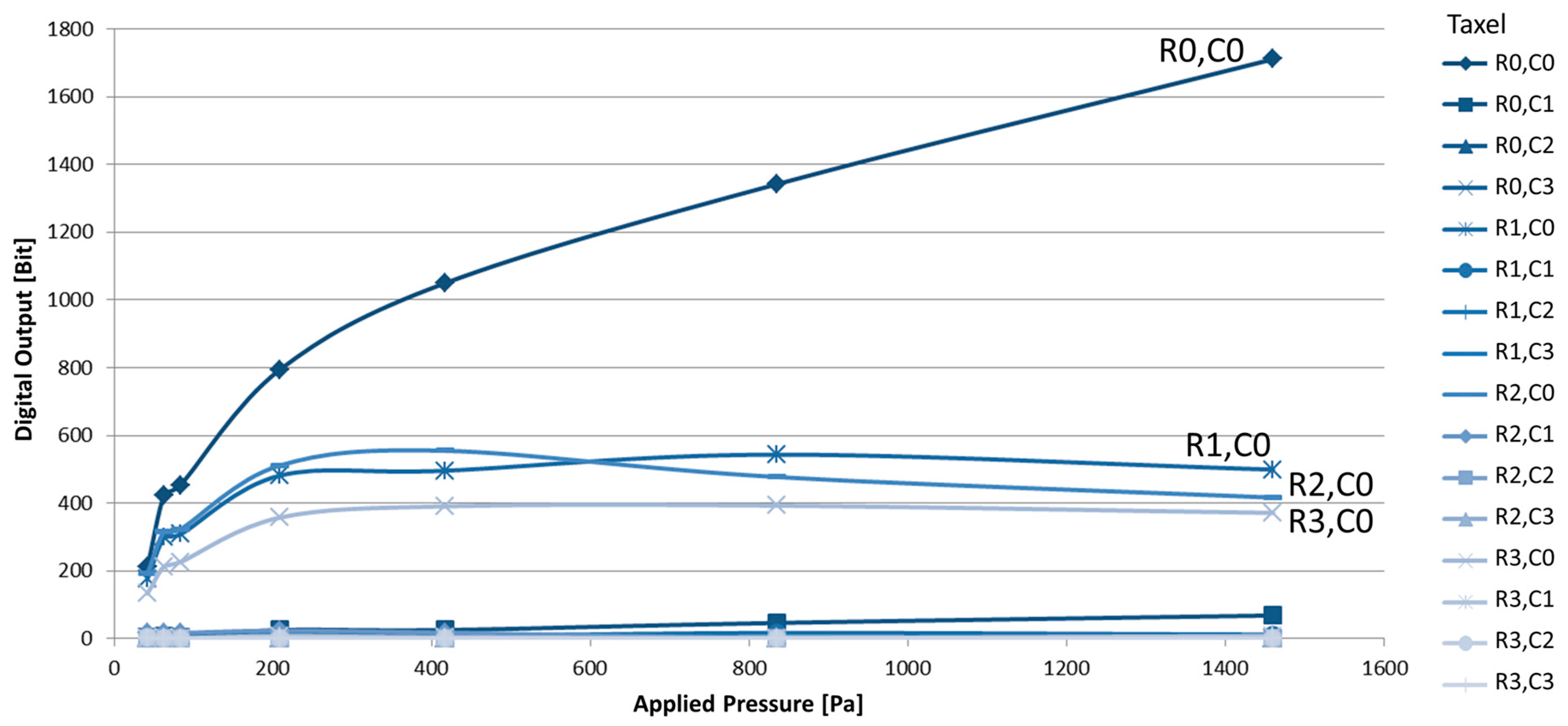
6.1. Sensing Matrix Calibration
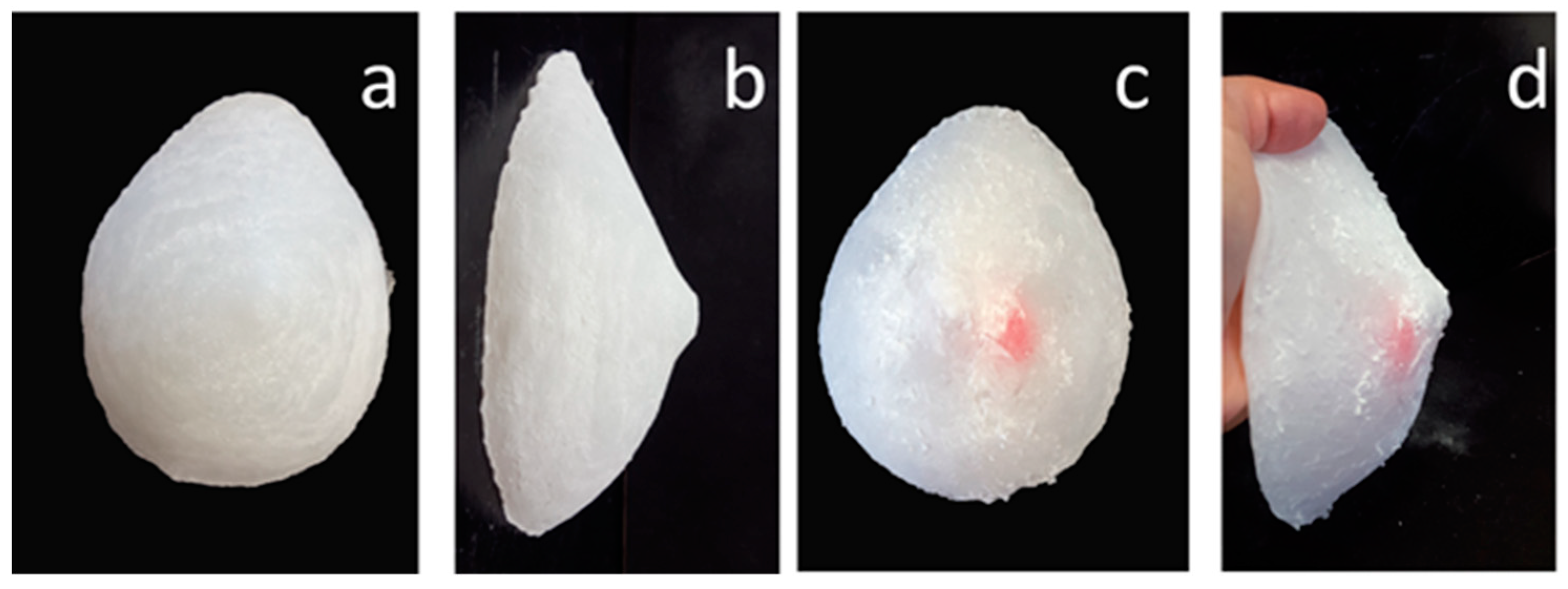
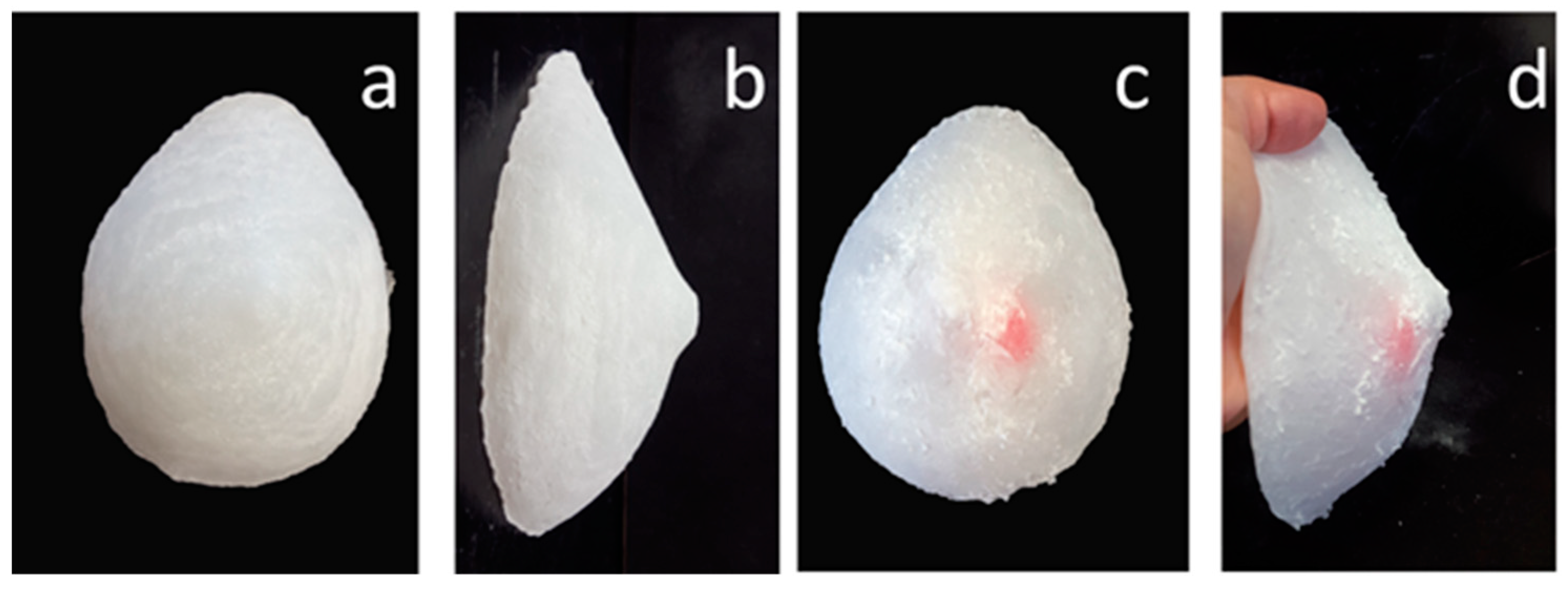
6.2. Phantom Fabrication
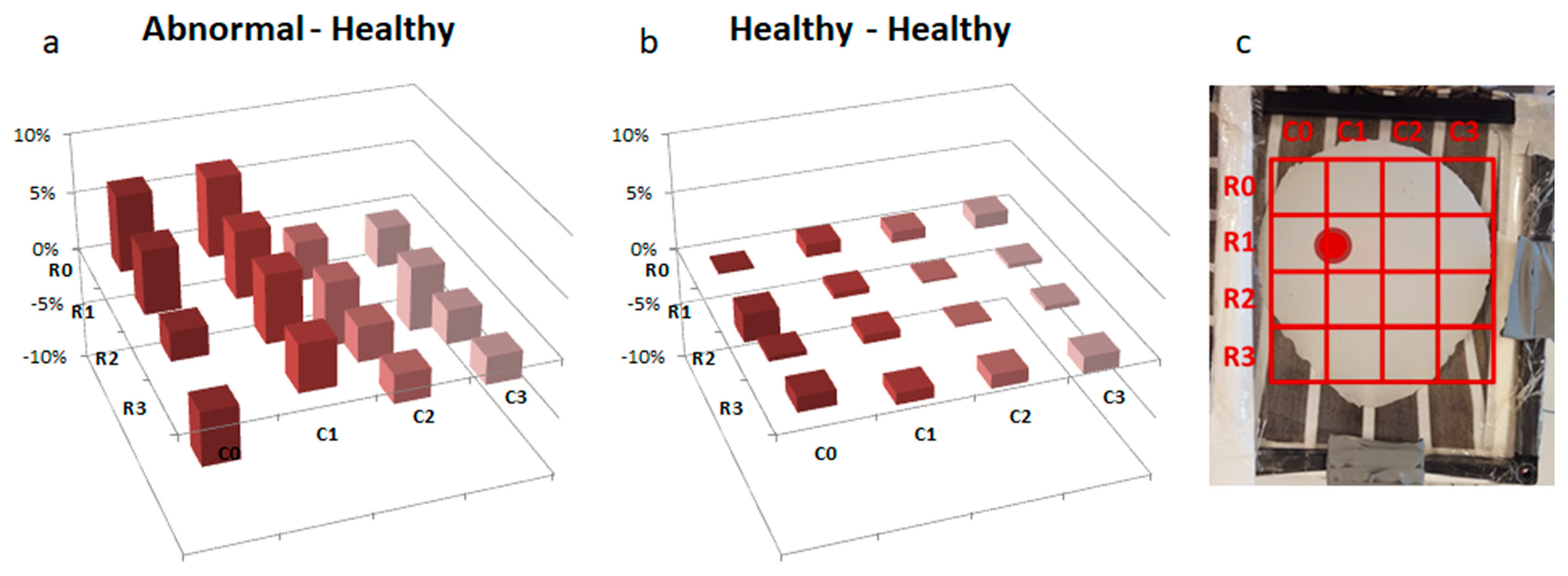
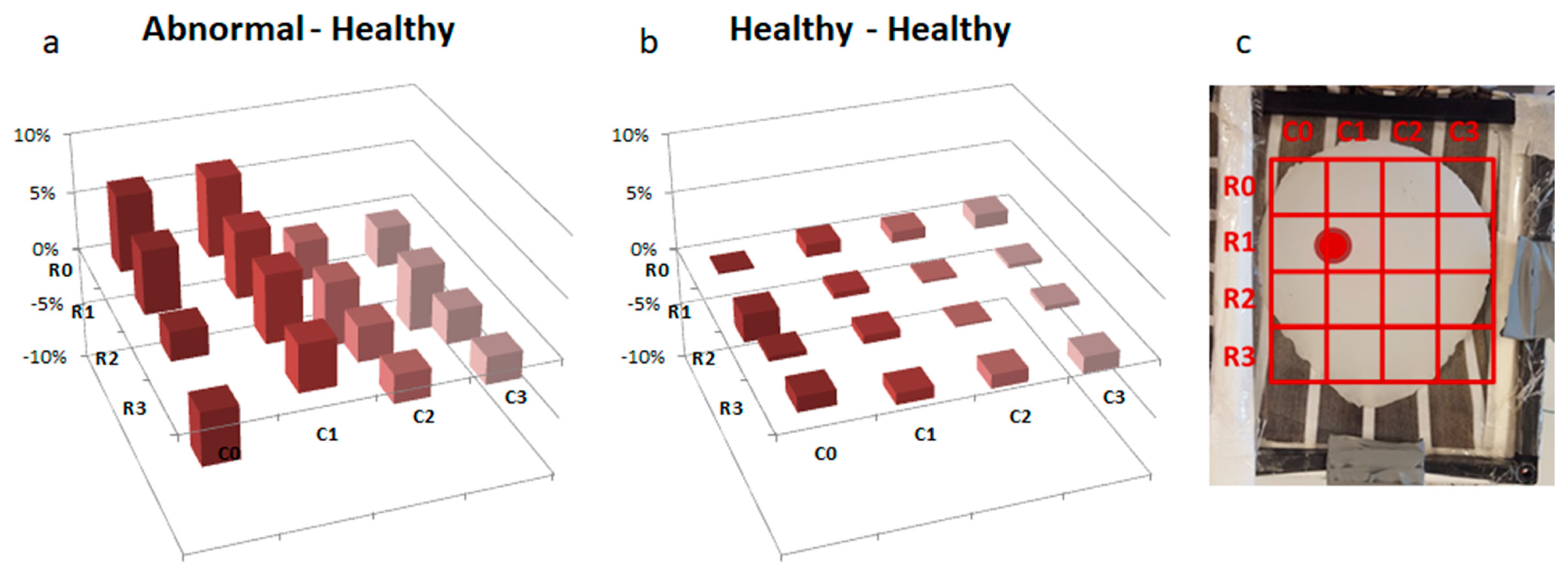
6.3. Nodule Identification Test Protocol
7. Characterization Results
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- U.S. Breast Cancer Statistics. Available online: https://www.breastcancer.org/symptoms/understand_bc/statistics (accessed on 14 July 2018).
- American Cancer Society. How Common Is Breast Cancer? Available online: https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html (accessed on 12 July 2018).
- Associazione Italiana di Oncologia Medica; Associazione Italiana dei Registri Tumori. I numeri del cancro in Italia; Il Pensiero Scientifico: Roma, Italy, 2017. [Google Scholar]
- Cardoso, F.; Loibl, S.; Pagani, O.; Graziottin, A.; Panizza, P.; Martincich, L.; Gentilini, O.; Peccatori, F.; Fourquet, A.; Delaloge, S.; et al. The European Society of Breast Cancer Specialists recommendations for the management of young women with breast cancer. Eur. J. Cancer 2012, 48, 3355–3377. [Google Scholar] [CrossRef] [PubMed]
- Samphao, S.; Wheeler, A.J.; Rafferty, E.; Michaelson, J.S.; Specht, M.C.; Gadd, M.A.; Hughes, K.S.; Smith, B.L. Diagnosis of breast cancer in women age 40 and younger: Delays in diagnosis result from underuse of genetic testing and breast imaging. Am. J. Surg. 2009, 198, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Nover, A.B.; Jagtap, S.; Anjum, W.; Yegingil, H.; Shih, W.Y.; Shih, W.H.; Brooks, A.D. Modern breast cancer detection: A technological review. J. Biomed. Imaging 2009, 26. [Google Scholar] [CrossRef] [PubMed]
- Carioli, G.; Malvezzi, M.; Rodriguez, T.; Bertuccio, P.; Negri, E.; La Vecchia, C. Trends and predictions to 2020 in breast cancer mortality in Europe. Breast 2017, 36, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Sure. Sure Touch. 2017. Available online: https://suretouch.us/ (accessed on 11 July 2018).
- Sarvazyan, A.; Egorov, V.; Sarvazyan, N. Tactile sensing and tactile imaging in detection of cancer. Biosens. Mol. Technol. Cancer Diagn. 2012, 337–352. [Google Scholar]
- Yousuf, M.A.; Asiyanbola, B.A. A review of force and resonance sensors used in the clinical study of tissue properties. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2013, 227, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Egorov, V.; Sarvazyan, A.P. Mechanical imaging of the breast. IEEE Trans. Med. Imaging 2008, 27, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Ramião, N.G.; Martins, P.S.; Rynkevic, R.; Fernandes, A.A.; Barroso, M.; Santos, D.C. Biomechanical properties of breast tissue, a state-of-the-art review. Biomech. Model. Mechanobiol. 2016, 15, 1307–1323. [Google Scholar] [CrossRef] [PubMed]
- Breast Self-Exam. Available online: https://www.breastcancer.org/symptoms/testing/types/self_exam (accessed on 7 July 2018).
- Elmore, J.G.; Armstrong, K.; Lehman, C.D.; Fletcher, S.W. Screening for breast cancer. JAMA 2005, 293, 1245–1256. [Google Scholar] [CrossRef] [PubMed]
- Higia Technologies. “Eva”. Available online: https://www.higia.tech/en/eva (accessed on 11 July 2018).
- Cyrcadia Health. iT bra. Available online: http://cyrcadiahealth.com/ (accessed on 11 July 2018).
- Intelligent Artificial Brassiere. CN Patent CN106913320A, 16 March 2017.
- E-Bra and Methods for Early Detection of Breast Tumor. U.S. Patent WO2013177370A1, 28 November 2013.
- De Maria, C.; Di Pietro, L.; Lantada, A.D.; Madete, J.; Makobore, P.N.; Mridha, M.; Ravizza, A.; Torop, J.; Ahluwalia, A. Safe innovation: On medical device legislation in Europe and Africa. Health Policy Technol. 2018, 7, 156–165. [Google Scholar] [CrossRef]
- Arti, A.; De Maria, C.; Lantada, A.D.; Di Pietro, L.; Alice, R.; Mannan, M.; Madete, J.; Makobore, P.N.; Aabloo, A.; Kitsing, R.; et al. Towards Open Source Medical Devices-Current Situation, Inspiring Advances and Challenges. Biodevices 2018, 1, 141–149. [Google Scholar] [CrossRef]
- Skovoroda, A.R.; Klishko, A.N.; Gusakyan, D.A.; Mayevskii, Y.I.; Yermilova, V.D.; Oran-skaya, G.A.; Sarvazyan, A.P. Quantitative analysis of the mechanical characteristics of pathologically changed soft biological tissues. Biophysics 1995, 40, 1359–1364. [Google Scholar]
- Krouskop, T.A.; Wheeler, T.M.; Kallel, F.; Garra, B.S.; Hall, T. Elastic moduli of breast and prostate tissues under compression. Ultrason. Imaging 1998, 20, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Lukowicz, P. Textile pressure force mapping. In Smart Textiles; Springer: Cham, Swizerland, 2017; pp. 31–47. [Google Scholar] [CrossRef]
- Mazzei, D.; De Maria, C.; Vozzi, G. Touch sensor for social robots and interactive objects affective interaction. Sens. Actuators A Phys. 2016, 251, 92–99. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nodule Position (Center) | LB [m] | MB [m] |
|---|---|---|
| x | −0.045 | −0.03 |
| y | 0.055 | 0.04 |
| Variable | [m] | [m] |
| a | 0.07 | 0.05 |
| b | 0.14 | 0.1 |
| c | 0.02 | 0.015 |
| d | 0.01 | 0.01 |
| Mesh Elements Degree of Freedom (DoF) | 914 | 790 |
| 3758 | 3270 | |
| Boundary Number | Boundary Condition | |
| 1 | Load Fx = −10000*nx_pn [Pa] Fy = −10000*ny_pn [Pa] | |
| 5 | Constraint Rx = 0, Ry = 0 | |
| 2,3,4,6,7,8 | No Constraint | |
| Nodule Position (Center) | LB [m] | MB [m] |
|---|---|---|
| x | −0.02 | 0.01 |
| y | 0.02 | 0.02 |
| z | −0.05 | −0.03 |
| Mesh Elements Degree of Freedom (DoF) | 9320 | 8635 |
| 41,328 | 38,355 | |
| Boundary Number | Boundary Condition | |
| 1 | Load Fx = −10000*nx_pn [Pa] Fy = −10000*ny_pn [Pa] Fz = −10000*ny_pn [Pa] | |
| 2 | Constraint Rx = 0, Ry = 0, Rz = 0 | |
| Other elements | No Constraint | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arcarisi, L.; Di Pietro, L.; Carbonaro, N.; Tognetti, A.; Ahluwalia, A.; De Maria, C. Palpreast—A New Wearable Device for Breast Self-Examination. Appl. Sci. 2019, 9, 381. https://doi.org/10.3390/app9030381
Arcarisi L, Di Pietro L, Carbonaro N, Tognetti A, Ahluwalia A, De Maria C. Palpreast—A New Wearable Device for Breast Self-Examination. Applied Sciences. 2019; 9(3):381. https://doi.org/10.3390/app9030381
Chicago/Turabian StyleArcarisi, Lucia, Licia Di Pietro, Nicola Carbonaro, Alessandro Tognetti, Arti Ahluwalia, and Carmelo De Maria. 2019. "Palpreast—A New Wearable Device for Breast Self-Examination" Applied Sciences 9, no. 3: 381. https://doi.org/10.3390/app9030381
APA StyleArcarisi, L., Di Pietro, L., Carbonaro, N., Tognetti, A., Ahluwalia, A., & De Maria, C. (2019). Palpreast—A New Wearable Device for Breast Self-Examination. Applied Sciences, 9(3), 381. https://doi.org/10.3390/app9030381