1. Introduction
Annually, more than 40% of all employees in Europe suffer from work-related musculoskeletal disorders (WMSDs), such as low back, neck or shoulder pain, despite ongoing efforts to improve the working conditions [
1]. These WMSDs result from excessive physical workloads due to repetitive movements (61%), non-neutral posture (44%) and heavy material handlings (31%) [
1]. They are responsible for the absence of 3%–6% of the working time, causing an average cost of 2.5% of the gross domestic product across Europe [
2]. Of all these WMSDs, 52% are due to overloading during lifting tasks, of which 65% affect the back [
3]. It is assumed that by reducing excessive physical workloads, the amount of WMSDs can be reduced, as can the concomitant costs. For this, ergonomic guidelines, such as the ISO standards, can be used. The ISO standards, more specifically ISO standard 11228 Part 1, advises a reference mass for two handed lifting under ideal conditions. Ideal conditions are characterized by having a symmetric standing, one’s trunk in a neutral position, a horizontal distance to the object center of mass less than 25 cm, and a grip height of less than 25 cm above knuckle height, thereby allowing a firm grip. Lifting duration should not exceed 1 h per day, with a frequency less or equal than 0.2 lifts per minute. In addition, favorable environmental conditions are assumed, i.e., not too warm/cold and humid. Under ideal conditions, the reference loads are 25 and 15 kg for 95% of men and women, respectively. It is assumed that when the lift situation is in accordance with the above-mentioned guidelines, the lifting technique is more ergonomic and thus reduces the risk of developing WMSDs. The action mechanism potentially reduces the compressive and shear forces between the vertebras. This is important, as high compressive forces on the vertebral discs have been related to low back injury [
4].
Two standard lifting techniques, the stoop and the squat, are well-described in literature [
5,
6,
7,
8,
9,
10,
11]. In general, squatting is advised to lift heavy objects, as this technique is thought to result in lower disc compression and shear forces compared to the stoop. On the other hand, stoop lifting should be restricted to lifting light objects because stoop lifting causes higher disc compression and shear forces compared to the squat [
8]. The high disc compression observed during stoop lifting results from a high flexion moment around the L5S1 joint, causing high muscle forces delivered by the back extensor muscles (i.e., m. erector spinae) to overcome the external flexion moment. Indeed, it is known that the muscle forces of the extensor muscle are the main contributors to the compression of the vertebral joints [
6].
To estimate joint moments, shear and compression forces, different biomechanical models (like static models [
12], electromyography (EMG)-assisted models [
6,
13,
14,
15], finite element models [
9,
12], 2D dynamic linked segment models in combination with an EMG-assisted models [
14] and a full-body musculoskeletal OpenSim model [
16]) have been used. These studies found lower moments in the lower back with lower disc compression and shear forces during squat lifting compared to the stoop, and they thereby advised using the squat technique for lifting. However, most studies have only focused on the L5S1 joint in isolation and have neglected loading on the other joints within the human body, which are also likely to be affected by lifting techniques. Squatting results in lower lumbar extensor moments, but to our knowledge, the effect on the shoulder or other joints has not yet been investigated during these lifting techniques. This is highly relevant given the comparable prevalence of shoulder and low back injuries in industry [
1].
When muscle loading associated with different lifting techniques has been studied based on EMG, most studies [
8,
17,
18,
19,
20] have only focused on a limited number of muscles that span the fifth lumbar vertebrae joint (i.e., m. erector spinae illiocostalis). Despite the small number of muscles analyzed, these studies have confirmed the relationship between chronic low back pain and increased trunk muscle activity during squat lifting [
8,
17].
Nevertheless, muscle activations only present localized and therefore partial information on musculoskeletal loading. Other kinematic and kinetic measures are therefore being considered in ergonomic risk analysis. Joint moments that combine kinematic and kinetic movement and which represent the resultant joint action and joint power, thus providing an estimate of energy absorption or generation by the musculoskeletal system, may serve as alternative indicators of musculoskeletal function and loading. Though joint moments and power are often reported parameters in clinical gait research, they are less frequently used within an ergonomic research context [
21,
22].
The use of a full body musculoskeletal model, multiple EMG-based muscle analyses and the introduction of joint power tackles the single-joint-analyses-problem in this research field. Therefore, the aim of this study was to investigate the effect of squat and stoop lifting techniques on full body musculoskeletal loading, as assessed by joint power and moments calculated using a detailed full body musculoskeletal OpenSim model with a complex definition of the back and the shoulder. In addition, the effect of lifting technique on muscle activity of nine different muscles was studied. We hypothesized that squat lifting would shift the power and moment contribution to the extremities compared to stoop lifting, thereby redistributing the muscle activity away from the lumbar region to the limbs.
2. Materials and Methods
Ten healthy participants (7 men; age: 31.5 years (± 12.7), body mass index (BMI): 22.19 kg/m² (±3.98)) participated in this study. Participants were excluded when suffering from musculoskeletal disorders or were experiencing pain that could affect activities of daily living. All participants provided written informed consent prior to the start of the study, and all study procedures were approved by the local ethics committee (Universitair Ziekenhuis Leuven, S61611).
Participants executed two standard lifting techniques: Stoop and squat. The two lifting techniques were verbally explained, and a small demo was performed before the actual measurements. During stoop lifting, participants were instructed to fully extend their knees and incline their trunk to lift the box from the ground to the upright position; the squat was performed with fully flexed knees, a heel lift-off, and the trunk close to erect (
Figure 1) [
8].
Participants had to lift a standard weight of ten kilograms as well as a weight equal to 40% of the arm lifting strength test (ALST) [
23], performed before the start of the measurement.
Ten infrared cameras (100 Hz, VICON, Oxford Metrics, Oxford, UK) captured 3D-marker trajectories during the lifting tasks. Retroflective markers were placed on the participants according to the plug-in gait marker model [
24] extended with a spine marker model [
25], and the single markers on the upper and lower arms and legs were replaced by three marker clusters. Two ground-embedded force plates synchronously recorded the ground reaction forces (1000 Hz, AMTI, Watertown, MA, USA). In addition, the unilateral (right side) muscle activation of 9 muscles was recorded, (more specifically, m. rectus femoris, m. biceps femoris, m. trapezius descendens, m. deltoideus anterior, m. deltoideus medius, m. triceps brachii, m. biceps brachii, m. erector spinae illiocostalis, and m. erector spinae longissimus) using surface electromyography (1000 Hz, Cometa, Bareggio, Italy) according to the Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM)-guidelines.
Measured data were processed using a standard musculoskeletal modelling workflow implemented in OpenSim 3.3 [
26] to calculate joint angles and moments. Three validated musculoskeletal models were combined: A modified model of the fully articulated thoracolumbar spine and rib cage model [
27], a modified model of an upper extremity model [
28], and the gait2354 lower extremity model [
29]. To simplify the model, the joints between the five lumbar vertebrae were described as 3 degrees of freedom joints, and the thorax was defined as one rigid segment linked as a weld joint with L1. In addition, the kinematics of L4–L5 and L2–L3 were defined using a coupled coordinate function using the joint angle of L5–S1 and L3–L4 as an independent variable. The weight of the box was accounted for by adding half of the weight of the box to the mass of metacarpal III on the right and left hand.
Firstly, the generic model was scaled to the subjects’ anthropometry based on the weight and the marker positions measured during a calibration trial. Secondly, joint angles (
Appendix A) were calculated using inverse kinematics [
30]. Thirdly joint moments were calculated using the Inverse Dynamics Tool implemented in OpenSim and normalized to body weight to account for differences in body mass. Joint power was then calculated based on the angular velocity and the normalized joint moment. Lastly, the moment impulse was calculated as the area under the normalized moment curve to estimate the cumulative loading over the whole lifting or lowering phase. Raw EMG signals were band pass filtered (20–400 Hz) and full-wave rectified. Then, the rectified signal was filtered with a 6 Hz low pass filter and normalized to the maximal muscle activity obtained during maximal voluntary contractions (MVC) measured during isolated tests before the lifting tests. Next, muscle effort was determined as the area under the MVC-normalized curve.
Subsequently, peak joint moments, powers, and muscle activities were determined during the lowering and lifting part of each trial, and the three were averaged over three trials per participant. The lifting and lowering phase started when the velocity of the box exceeded 0.25 cm/s and ended when the velocity was below 0.25 cm/s.
A general linear mixed model was used to identify statistically significant differences between techniques, weights and handling phases, i.e., lowering and lifting (MATLAB 2018a, The MathWorks, Inc., Natick, MA, United States). In this statistical model, the parameters (i.e., peak moment, peak power, peak muscle activity, moment impulse and muscle effort) are the different response variables; the technique, weights and handling phase are the predictor variables; and the subject is the grouping variable. As the distance between the load and L5 while handling 10 kg was significantly higher during the squat than during the stoop (36.49 ± 4.87 and 31.60 ± 3.09 cm for the squat and the stoop, respectively), the distance between the load and L5 was used as a covariate. Differences were interpreted as significantly different when α < 0.05.
3. Results
The weight equal to 40% of the arm lifting strength test (ALST) was, on average, 12 ± 4 kg. The results of the 10 kg condition are shown in
Appendix B. In general, the differences between the two conditions, the 10 kg and 40% ALST tests, were rather small, and differences in the 10 kg condition are in line with the differences observed in the 40% ALST condition. The 40% ALST condition is described in this section because this weight is relative to the strength of the participant and therefore did not influence the results between the male and female participants [
31], as three women and seven men were included in this study.
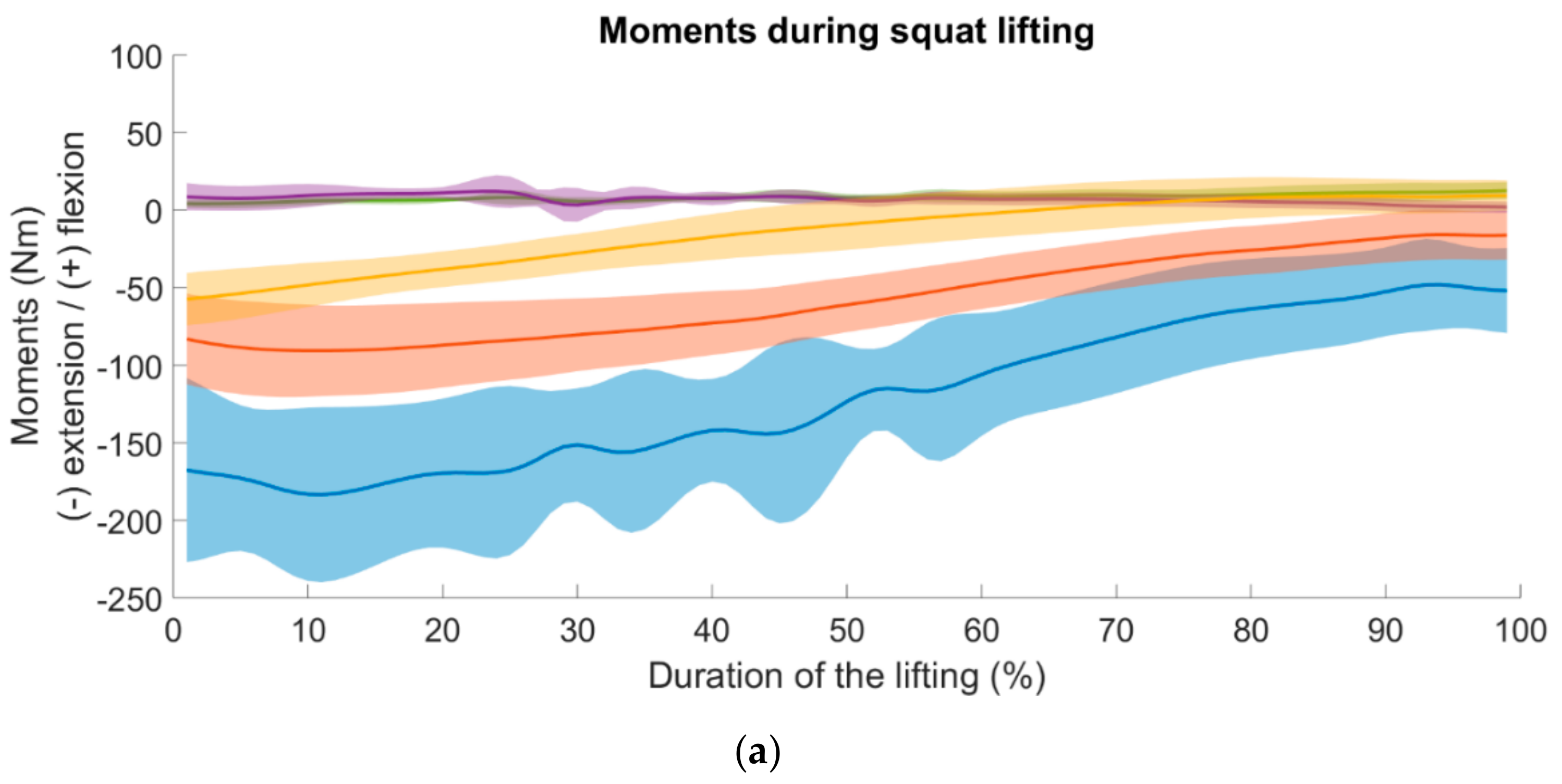
Joint moments during squat and stoop lifting are presented in
Figure 2, and joint power is presented in
Figure 3. For all lifting conditions and both techniques, the highest joint moments during lifting and lowering were observed in L5S1, followed by the hip and knee (
Figure 2). Joint power generation was highest at the hip for both techniques, with knee power generation being equal to hip power during squat lifting (
Figure 3). During squat lifting, power was mainly generated by the hip and knee extensors (
Figure 3a). On the other hand, during stoop lifting, knee flexors mainly absorbed power throughout the movement (
Figure 3b). Power generation and absorption when lifting were inverted during lowering to absorption and generation, respectively. When lowering while using the squat technique, power was mainly absorbed at the hip and knee, whereas when lowering while using the stoop technique, power was mainly absorbed at the hip.
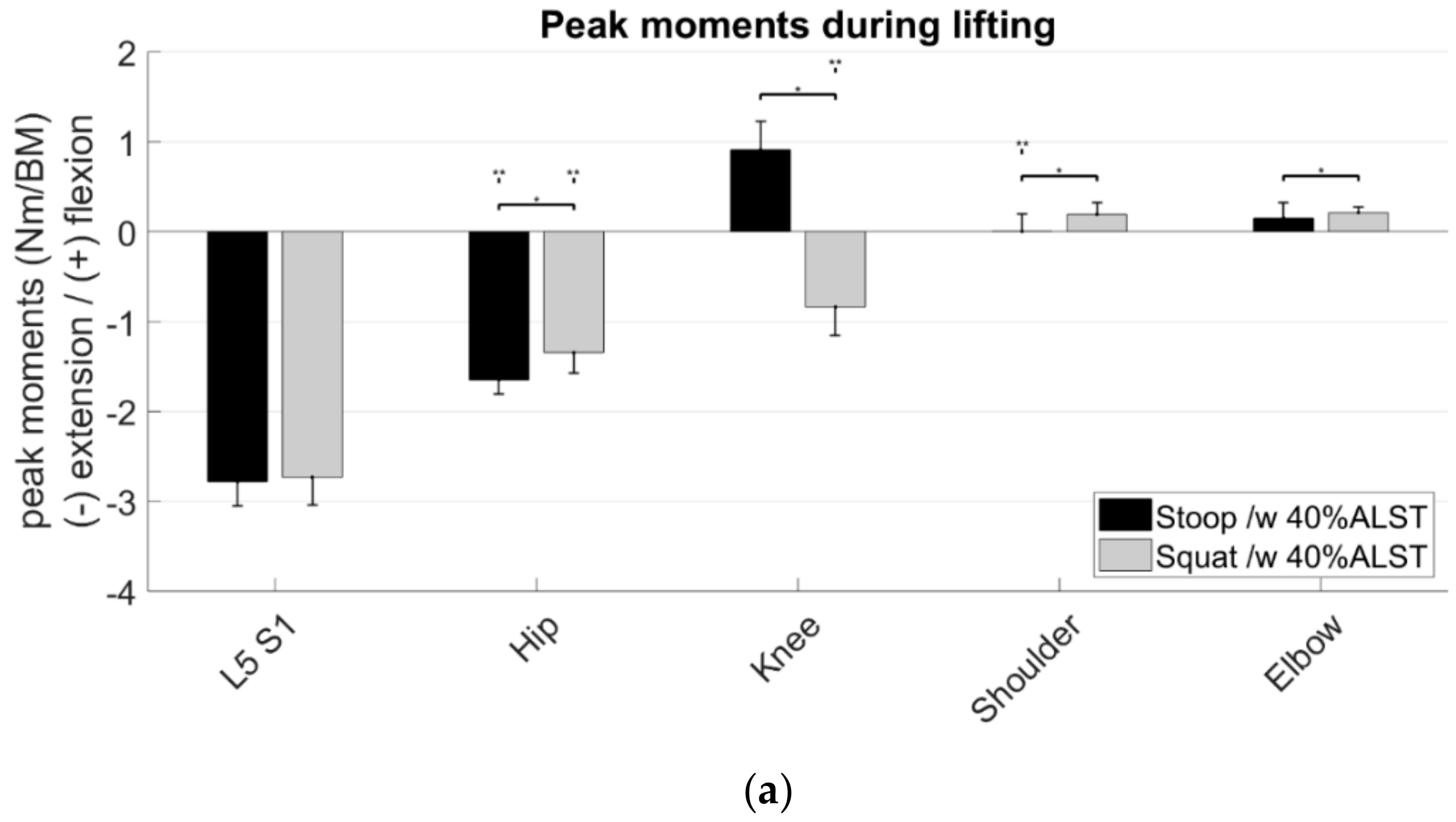
3.1. Peak Moments
Between lifting techniques, no significant differences in L5S1 peak moments were found, hip extension moments were significantly lower during squat lifting than during stoop lifting, and extension moments were significantly higher for the shoulder and the elbow flexion moment (
Figure 4a,b). During squat lifting, a peak knee extension moment was observed in contrast to a knee flexion moment during stoop lifting (
Figure 4a).
Peak hip extension moments were significantly higher during lifting than during lowering, whereas the opposite was observed for the shoulder flexion moments during stoop lifting. During squat lifting, peak knee extension moments were higher during lifting than during lowering.
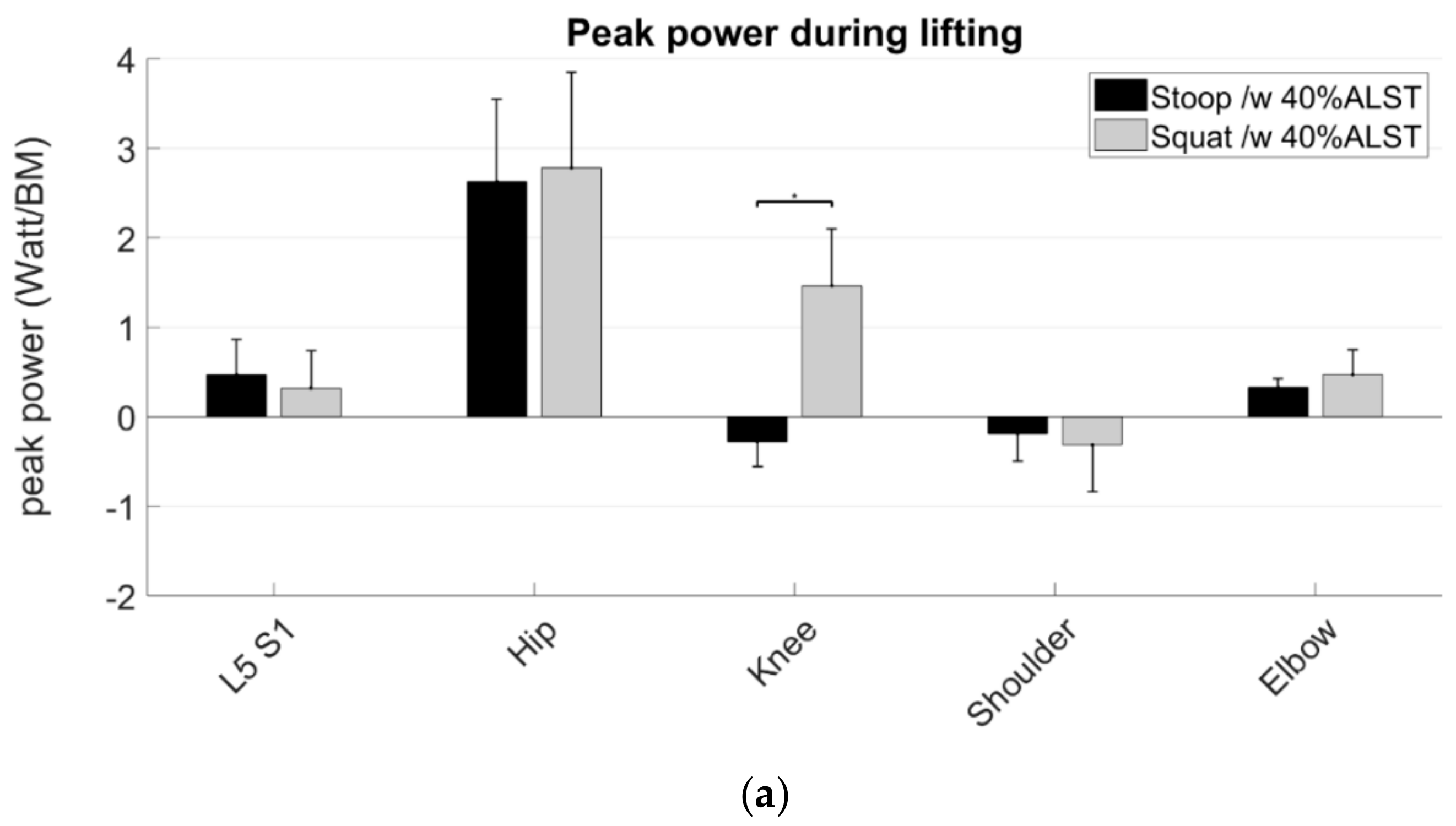
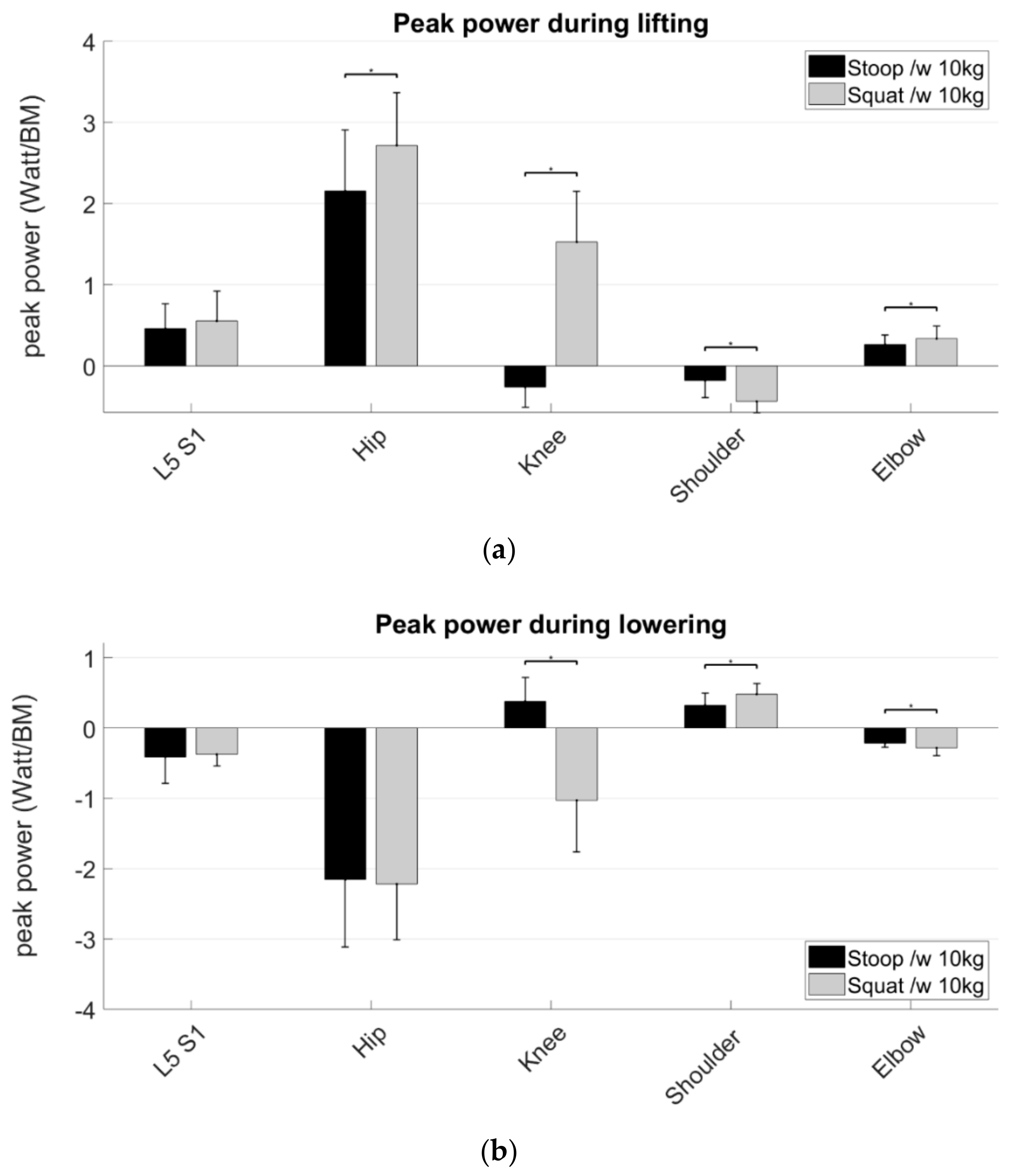
3.2. Peak Power
Between lifting techniques, no significant differences in power generation nor absorption in L5S1 were found (
Figure 5a). Hip and elbow peak power generation and absorption were significantly higher during the squat than during stoop lifting. Power generation and absorption in the knee were opposed during the squat compared to the stoop but were significantly higher during the squat than during the stoop.
Power generation and absorption during lifting were inverted during lowering. However, this did not affect the differences between lifting techniques.
The 40% ALST-condition resulted in significantly higher peak power generation and absorption in the hip and the elbow during stoop lifting and significantly higher peak power generation in the shoulder during the lowering phase of the stoop lift technique. In general, the results for peak moments and power were similar while handling a box of 10 kg. These results are shown in
Appendix B (
Figure A4 and
Figure A5).
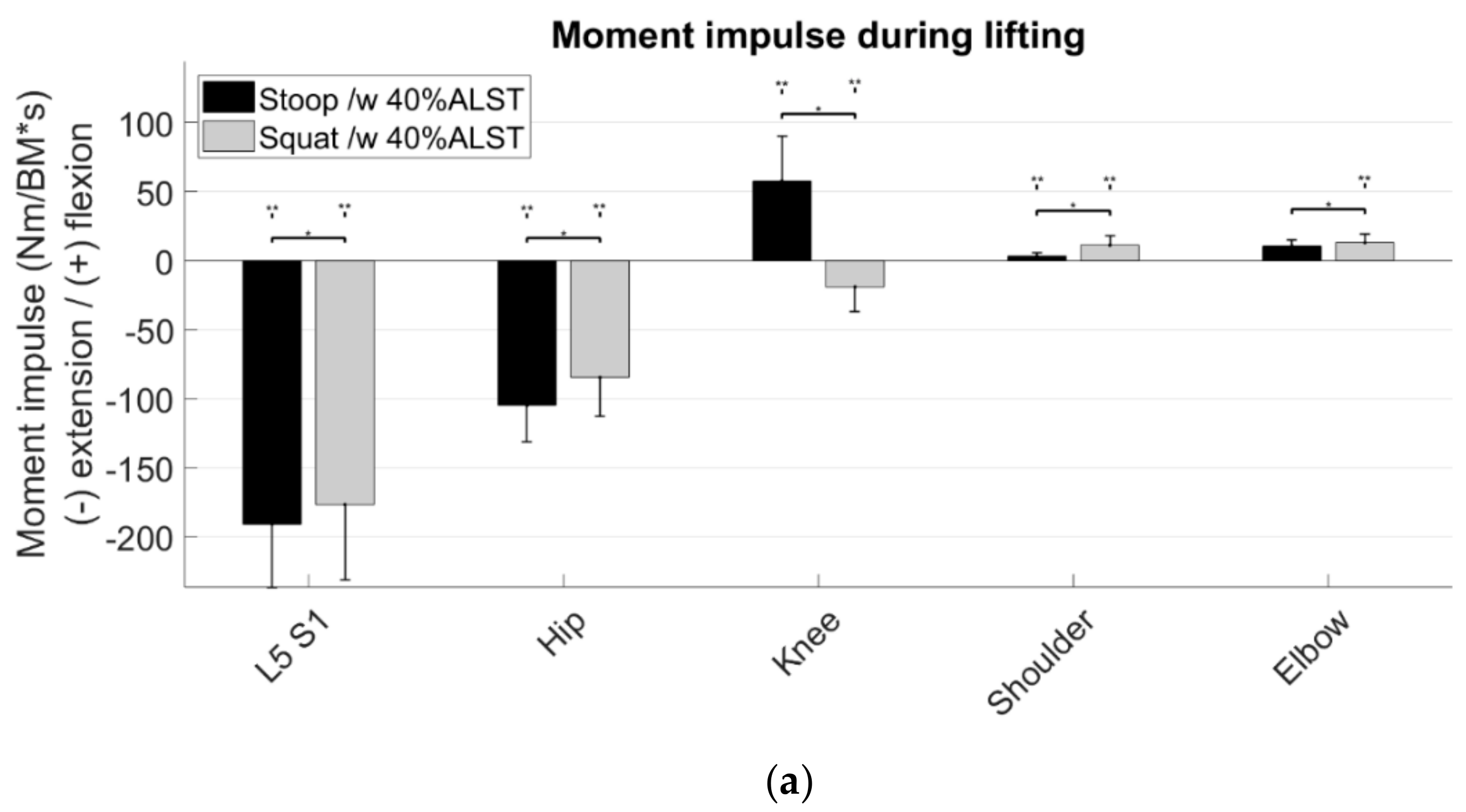
3.3. Moment Impulse
Between lifting techniques, significantly lower moment impulses were observed in L5S1, hip and knee, but significantly higher moment impulses were observed in the shoulder and elbow during the squat than during the stoop (
Figure 6). In general, moment impulses were significantly lower in all joints, except the elbow during the lifting stoop compared to lowering. The 40% ALST-condition resulted in a significantly lower moment impulse in the knee when lifting while using the stoop technique compared to the 10 kg-condition (
Appendix B Figure A3).
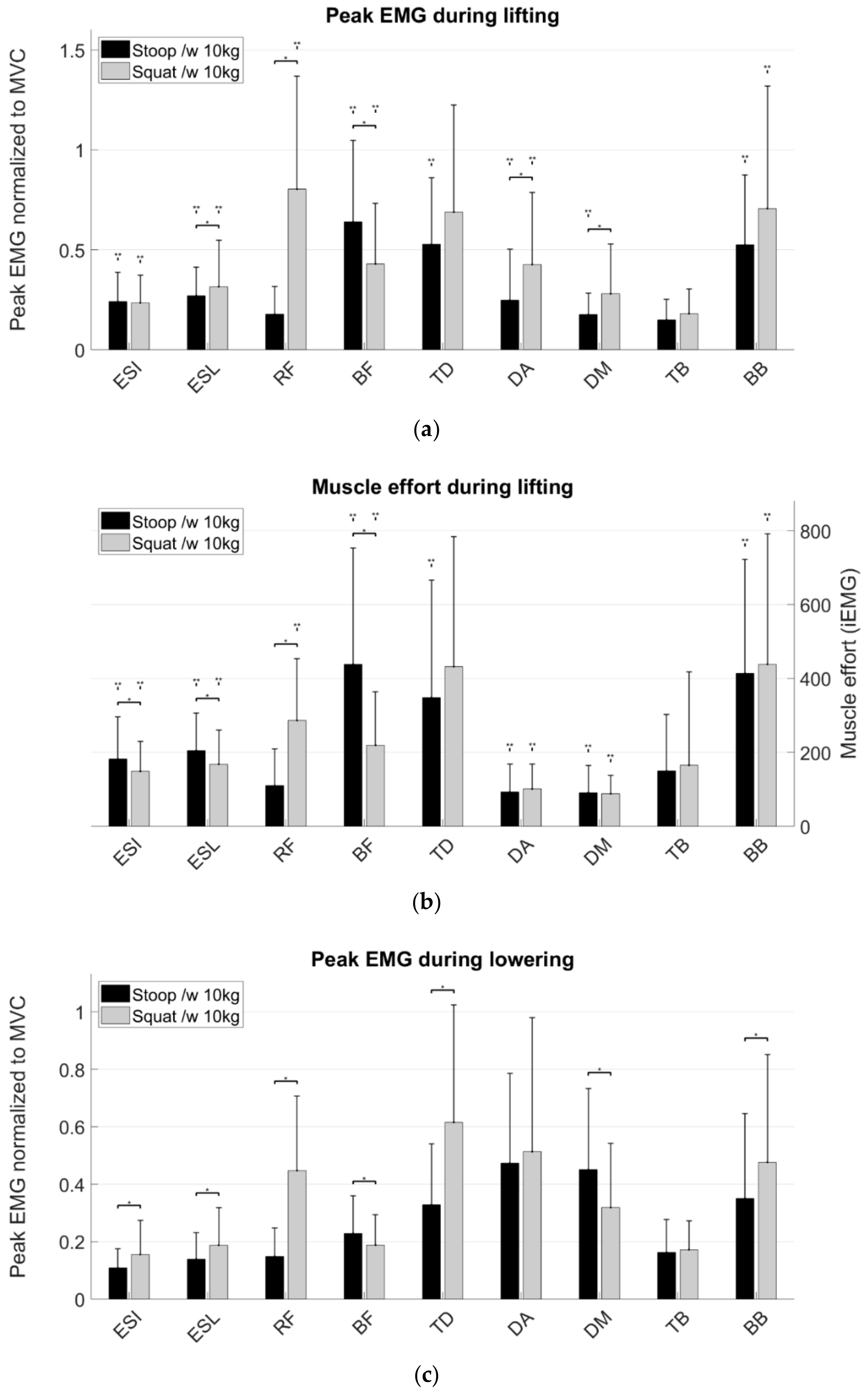
3.4. Peak Muscle Activity
Between lifting techniques, significantly higher muscle activity for the back extensors (i.e., erector spinae longissimus and iliocostalis), leg extensor (i.e., m. rectus femoris), and shoulder muscles (i.e., m. trapezius descendens, m. deltoideus anterior and medius) was observed during the squat than during the stoop. Significantly lower muscle activity of the leg flexor (i.e., m. biceps femoris) was observed during the squat than during the stoop (
Figure 7).
Muscle activity was significantly higher for the back extensors, arm flexor, leg extensor and flexor muscle but significantly lower for the shoulder muscles during lifting than during lowering. The handling phase had no effect on the m. triceps brachii activity.
The 40% ALST-condition resulted in lower muscle activity for the back muscles when lifting while using the squat technique and lower muscle activity of the shoulder muscles when lifting while using the stoop technique compared to the 10 kg condition (
Figure 7a—
Appendix B Figure A2a). The 40% ALST-condition had significantly lower muscle activity for the arm muscles and the m. deltoideus medius during lowering using the squat technique (
Figure 7c—
Appendix B Figure A2c).
3.5. Muscle Effort
Between techniques, the muscle effort of m. rectus femoris and shoulder muscles was significantly higher during the squat than during the stoop (
Figure 7c,d). Muscle effort of the back muscles and m. biceps femoris was significantly lower during the squat than during the stoop in the lifting phase. Muscle effort was significantly higher for almost all muscles except m. deltoideus anterior and medius during lifting than during lowering.
4. Discussion
This study compared whole body loading during two frequently used lifting techniques—squat and stoop lifting—based on joint moments, joint power and muscle activity. In general, squat lifting is the advised method to lift heavy objects because it reduces low back loading. However, it is likely that lifting technique affects joints other than L5S1 and could therefore contribute in the development of WMSDs. Indeed, the present results indicate that lifting technique has no significant effect on the peak moments and power generation in L5S1, but it does significantly increases musculoskeletal demand on the other joints. Furthermore, for the tested weights, the differences between lifting strategies were more pronounced than the effect of the weight lifted.
In line with our hypothesis, squat lifting was found to shift musculoskeletal loading merely to the extremities, potentially to safeguard the lower back. However, joint moments and powers in the back were found not to be significantly different between lifting techniques, therefore imposing similar musculoskeletal loading on the back during squat and stoop lifting. Squat lifting was found to be mainly executed by additional active work of the knee extensors compared to stoop lifting. This was further confirmed by the increased muscle activity of the rectus femoris muscle. Furthermore, squat lifting increased musculoskeletal loading in the shoulder and elbow. This could potentially explain the similar prevalence of WMSDs in the shoulder to low back pain in persons exposed to frequent lifting [
1].
Previously, squat lifting was advised to be used over stoop lifting to lift heavy objects because lower moments and compressive forces at the back were reported [
6,
8,
9,
20,
32]. This is in contrast to the findings of the present study, as similar joint moments were found in the L5S1 joint even when taking the distance between L5 and the object into account. Given the fact that muscle force is the dominant contributor to compressive forces on L5S1 and high muscle force results from high moments around L5S1 [
6], we could not conclude that the squat imposes lower compressive forces on L5S1 than the stoop [
6]. Based on the assumption that high flexion moments in L5S1 result in high compressive forces, we could assume (as we did not calculate compression and shear forces in this study) that compressive forces are similar between both techniques because both techniques resulted in similar moments around L5S1. Future research should focus on validating biomechanical models in order to calculate compression and shear forces at L5S1. Moreover, based on the L5S1 moment and power, we could not favor squat lifting over stoop lifting in contrast to current literature [
6,
9]. On the other hand, van Dieen et al. 1999 [
32] concluded that there is no evidence of advising squat over stoop lifting in their comprehensive review of 27 studies, which is in line with our results.
Task characteristics, i.e., initial lifting height and dimensions object lift, influence back loading [
33], which makes comparisons with literature delicate. Even small adjustments to the squatting technique such as rotating the knees outwards already reduces back loading [
14], which was not controlled in this study. However, the handled weights during this experiment were fairly light, and the box was rather small (width: 21 cm; height: 14 cm; length: 36 cm) compared to other studies [
6,
9]. Potentially, the effect of the lifting technique will be more pronounced when heavier weights are handled. On the other hand, Kingma et al. 2004 concluded that squat lifting a box of 10.5 kg results in higher net moments and higher compression forces in L5S1 compared to the stoop. Our results, with similar moments in L5S1 during the squat and the stoop, can be explained by the higher upper body acceleration during the squat, as suggested by Kingma et al. 2004. This statement is supported by the fact that higher hip and knee joint powers are combined with lower hip and knee moments during the squat compared to the stoop.
However, when accounting for the execution time, i.e., based on the moment impulse on L5S1, squat lifting may still be preferred over stoop lifting. In addition to the slightly longer duration of the stoop lifting task, the longer persistence of the L5S1 extension moment during the stoop than during squat lifting may contribute to this finding (
Figure 2). As a result, the cumulative loading during the whole movement is lower during squat lifting. Considering that low back pain is a result of cumulative damage in the lower back [
4,
11,
31,
34,
35,
36], the squat should be recommend when lifting frequently to prevent back injury. This finding is also supported by the lower muscle effort in the back muscles during the squat. On the other hand, cumulative loading is higher in the shoulder and elbow during the squat compared to the stoop based on the higher moment impulse in shoulder and elbow. In addition, the higher muscle effort of the m. biceps brachii and trapezius descendens, especially during the lowering phase, support this statement, allowing us to conclude that there is an increased injury risk for the shoulder and elbow during repetitive squat lifting.
The handling phase had only a minor effect on musculoskeletal loading in terms of the peak moments, powers and moment impulses, but it had a major effect on muscle activity. In general, muscle activity was higher during lifting than during lowering. This is in line with previous work that has investigated extensor muscle activations during the stoop [
9]. The peak EMG of the back extensor muscles were lower during the lowering phase compared to the lifting phase (
Figure 7a,c) as back extensor muscles activation peaks twice during the stoop: One small peak during the lowering phase and a larger one during the lifting phase [
9]. Our results can be explained by the fact that the muscles have to overcome the moment generated by gravity during the lifting phase, whereas the muscles can cooperate with gravity to perform the required movement during lowering. This can be seen in the higher extensor muscles activity with the squat compared to the stoop while lowering the box, where the moment exerted by gravity can be used advantageous, resulting in higher muscle activation during squat lowering than during stoop lowering.
Interestingly, the findings based on the maximal loading (i.e., peak moment and power) differ from those that account for the movement duration (i.e., moment impulse and muscle effort). The most striking example is that the maximal loading in L5S1 did not differ between techniques, whereas moment impulse in L5S1 and muscle effort of the back muscles did differ between lifting techniques. This suggests that future risk assessment tools should also account for the duration of the lifting task instead of only focusing on the peak moments, as is currently typically done in practice. This is in line with a recently formulated fatigue-failure theorem [
37] that relates the pathomechanics of WMSDs to both repetition and force magnitude. Combined with our results, this suggests that ergonomic analysis should use a more holistic approach when analyzing the risk for WMSDs in work situations rather than focusing on the musculoskeletal loading of the target region. Moreover, our results indicate that multiple techniques (i.e., moment estimation and electromyography) should be combined when assessing ergonomic risk and evaluating the effectiveness of ergonomic interventions. This is, in particular, illustrated by the difference in elbow moment between the two different lifting techniques, whereas there was no difference in peak EMG or muscle effort for the m. biceps brachii and triceps brachii.
Though our results indicate that squat lifting imposes similar peak musculoskeletal loading compared to stoop lifting, our results should be interpreted in the context of some limitations. First, although the musculoskeletal model used in the present study has a detailed description of the shoulder and lumbar back region, the thorax is defined as one rigid segment. Furthermore, not all degrees of freedom in the shoulder were modelled (i.e., pro- and retraction of the shoulder griddle). Secondly, healthy volunteers whose lifting dynamics are likely to be different compared to experienced blue-collar workers were studied. It was previously found that experienced blue-collar workers have adopted a more efficient method for lifting over the years [
13]. However, we assume that the effect of experience on performance during isolated, well-standardized lifting tasks is minimal. Thirdly, the tasks performed in the lab might be difficult to generalize to real-world situations. According the National Institute for Occupational Safety and Health (NIOSH) [
38] equations, the task in the lab could be classified as heavy; however, the set-up in the lab mostly conformed the guidelines reported in ISO 11228 part 1, whereas in the industry, ideal circumstances are not likely to be present the whole time and the weight of the object to lift often exceeds the weight that was used in the present study. Future research should focus on differentiating more between weights and investigate the effect of weight on lifting techniques and musculoskeletal loading.
In summary, peak moments in L5S1, a well-recognized risk factor for developing WMSDs, is not different between the two techniques while lifting a box of approximately 10 kg, although the moment impulse is higher in L5S1, hip and knee during the stoop. In contrast to these findings, ergonomic guidelines suggest using squat lifting as much as possible during materials handling, and for that reason, a reevaluation of the ergonomic guidelines is needed. Therefore, we suggest to adopt a more holistic framework that combines different measurement modalities as used in the present study when analyzing working tasks and to evaluate the effect of an intervention on the WMSDs risk.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



















