
Accuracy Assessment of 3D-Printed Surgical Guides for Palatal Miniscrew Placement: A Retrospective Study

 , , ,
, , , 

Abstract
1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
Future Research Directions and Possible Applications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Stursa, L.; Wendl, B.; Jakse, N.; Pichelmayer, M.; Weiland, F.; Antipova, V.; Kirnbauer, B. Accuracy of Palatal Orthodontic Mini-Implants Placed Using Fully Digital Planned Insertion Guides: A Cadaver Study. J. Clin. Med. 2023, 12, 6782. [Google Scholar] [CrossRef] [PubMed]
- Santmartí-Oliver, M.; Jorba-García, A.; Moya-Martínez, T.; de-la-Rosa-Gay, C.; Camps-Font, O. Safety and Accuracy of Guided Interradicular Miniscrew Insertion: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 7697. [Google Scholar] [CrossRef] [PubMed]
- Schwärzler, A.; Ludwig, B.; Chitan, P.; Lettner, S.; Sagl, B.; Jonke, E. Transfer accuracy of 3D printed versus CAD/CAM milled surgical guides for temporary orthodontic implants: A preclinical micro CT study. J. Dent. 2024, 146, 105060. [Google Scholar] [CrossRef] [PubMed]
- Antoszewska-Smith, J.; Sarul, M.; Łyczek, J.; Konopka, T.; Kawala, B. Effectiveness of orthodontic miniscrew implants in anchorage reinforcement during en-masse retraction: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 440–455. [Google Scholar] [CrossRef]
- Di Leonardo, B.; Ludwig, B.; Lisson, J.A.; Contardo, L.; Mura, R.; Hourfar, J. Insertion torque values and success rates for paramedian insertion of orthodontic mini-implants: A retrospective study. J. Orofac. Orthop. 2018, 79, 109–115. [Google Scholar] [CrossRef]
- Faegheh, G.; Khosravifard, N.; Maleki, D.; Hosseini, S.K. Evaluation of Palatal Bone Thickness and Its Relationship with Palatal Vault Depth for Mini-Implant Insertion Using Cone Beam Computed Tomography Images. Turk. J. Orthod. 2022, 35, 120–126. [Google Scholar] [CrossRef]
- Nucera, R.; Costa, S.; Bellocchio, A.M.; Barbera, S.; Drago, S.; Silvestrini, A.; Migliorati, M. Evaluation of palatal bone depth, cortical bone, and mucosa thickness for optimal orthodontic miniscrew placement performed according to the third palatal ruga clinical reference. Eur. J. Orthod. 2022, 44, 530–536. [Google Scholar] [CrossRef]
- Negrisoli, S.; Angelieri, F.; Gonçalves, J.R.; da Silva, H.D.P.; Maltagliati, L.; Raphaelli Nahás-Scocate, A.C. Assessment of the bone thickness of the palate on cone-beam computed tomography for placement of miniscrew-assisted rapid palatal expansion appliances. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 849–857. [Google Scholar] [CrossRef]
- Blasi, A.; Nucera, R.; Ronsivalle, V.; Candida, E.; Grippaudo, C. Asymmetry index for the photogrammetric assessment of facial asymmetry. Am. J. Orthod. Dentofac. Orthop. 2022, 162, 394–402. [Google Scholar] [CrossRef]
- Sánchez-Riofrío, D.; Viñas, M.J.; Ustrell-Torrent, J.M. CBCT and CAD-CAM technology to design a minimally invasive maxillary expander. BMC Oral. Health 2020, 20, 303. [Google Scholar] [CrossRef]
- Aiello, D.; Nucera, R.; Costa, S.; Figliuzzi, M.M.; Paduano, S. A Simplified Digital Approach to the Treatment of a Postpuberty Patient with a Class III Malocclusion and Bilateral Crossbite. Case Rep. Dent. 2021, 2021, 3883187. [Google Scholar] [CrossRef] [PubMed]
- Burak, K.; Hilmi, B.M. Evaluating palatal mucosal thickness in orthodontic miniscrew sites using cone-beam computed tomography. BMC Oral. Health 2024, 24, 1153. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hämmerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral. Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar]
- D’Haese, J.; Van De Velde, T.; Komiyama, A.; Hultin, M.; De Bruyn, H. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: A review of the literature. Clin. Implant. Dent. Relat. Res. 2012, 14, 321–335. [Google Scholar] [CrossRef]
- Poggio, P.M.; Incorvati, C.; Velo, S.; Carano, A. “Safe zones”: A guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod. 2006, 76, 191–197. [Google Scholar] [CrossRef]
- Kim, T.; Lee, S.; Kim, G.B.; Hong, D.; Kwon, J.; Park, J.W.; Kim, N. Accuracy of a simplified 3D-printed implant surgical guide. J. Prosthet. Dent. 2020, 124, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Baumgaertel, S. Quantitative investigation of palatal bone depth and cortical bone thickness for mini-implant placement in adults. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 104–108. [Google Scholar] [CrossRef]
- Hourfar, J.; Ludwig, B.; Bister, D.; Braun, A.; Kanavakis, G. The most distal palatal ruga for placement of orthodontic mini-implants. Eur. J. Orthod. 2015, 37, 373–378. [Google Scholar] [CrossRef]
- Nucera, R.; Ciancio, E.; Maino, G.; Barbera, S.; Imbesi, E.; Bellocchio, A.M. Evaluation of bone depth, cortical bone, and mucosa thickness of palatal posterior supra-alveolar insertion site for miniscrew placement. Prog. Orthod. 2022, 23, 18. [Google Scholar] [CrossRef]
- Maino, B.G.; Paoletto, E.; Lombardo, L., 3rd; Siciliani, G. A Three-Dimensional Digital Insertion Guide for Palatal Miniscrew Placement. J. Clin. Orthod. 2016, 50, 12–22. [Google Scholar]
- Su, L.; Song, H.; Huang, X. Accuracy of two orthodontic mini-implant templates in the infrazygomatic crest zone: A prospective cohort study. BMC Oral. Health 2022, 22, 252. [Google Scholar] [CrossRef] [PubMed]
- Pozzan, L.; Migliorati, M.; Dinelli, L.; Riatti, R.; Torelli, L.; Di Lenarda, R.; Contardo, L. Accuracy of the digital workflow for guided insertion of orthodontic palatal TADs: A step-by-step 3D analysis. Prog. Orthod. 2022, 23, 27. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, B.; Vasudavan, S.; Drescher, D. CAD-CAM-fabricated mini-implant insertion guides for the delivery of a distalization appliance in a single appointment. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.C.; Huang, J.N.; Zhao, S.F.; Xu, X.J.; Xie, Z.J. Radiographic and surgical template for placement of orthodontic microimplants in interradicular areas: A technical note. Int. J. Oral. Maxillofac. Implant. 2006, 21, 629–634. [Google Scholar]
- Yuan, L.; Zhao, R.; Liu, J.; Tang, R.; Bai, S.; Liu, X. The success rate of infrazygomatic mini-implants placed with and without surgical guides: A historical control study. BMC Oral. Health 2025, 25, 124. [Google Scholar] [CrossRef]
- Cantarella, D.; Savio, G.; Grigolato, L.; Zanata, P.; Berveglieri, C.; Lo Giudice, A.; Isola, G.; Del Fabbro, M.; Moon, W. A New Methodology for the Digital Planning of Micro-Implant-Supported Maxillary Skeletal Expansion. Med. Devices 2020, 13, 93–106. [Google Scholar] [CrossRef]
- Bae, M.J.; Kim, J.Y.; Park, J.T.; Cha, J.Y.; Kim, H.J.; Yu, H.S.; Hwang, C.J. Accuracy of miniscrew surgical guides assessed from cone-beam computed tomography and digital models. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 893–901. [Google Scholar] [CrossRef]
- Qiu, L.; Haruyama, N.; Suzuki, S.; Yamada, D.; Obayashi, N.; Kurabayashi, T.; Moriyama, K. Accuracy of orthodontic miniscrew implantation guided by stereolithographic surgical stent based on cone-beam CT-derived 3D images. Angle Orthod. 2012, 82, 284–293. [Google Scholar] [CrossRef]
- Melo, A.C.; Andrighetto, A.R.; Hirt, S.D.; Bongiolo, A.L.; Silva, S.U.; Silva, M.A. Risk factors associated with the failure of miniscrews—A ten-year cross sectional study. Braz. Oral. Res. 2016, 30, e124. [Google Scholar] [CrossRef]
- Crismani, A.G.; Bertl, M.H.; Celar, A.G.; Bantleon, H.P.; Burstone, C.J. Miniscrews in orthodontic treatment: Review and analysis of published clinical trials. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 108–113. [Google Scholar] [CrossRef]
- Maino, B.G.; Paoletto, E.; Cremonini, F.; Liou, E.; Lombardo, L. Tandem Skeletal Expander and MAPA Protocol for Palatal Expansion in Adults. J. Clin. Orthod. 2020, 54, 690–704. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Statistics | ||||
|---|---|---|---|---|
| Outcomes | Mean | Sd | Min | Max |
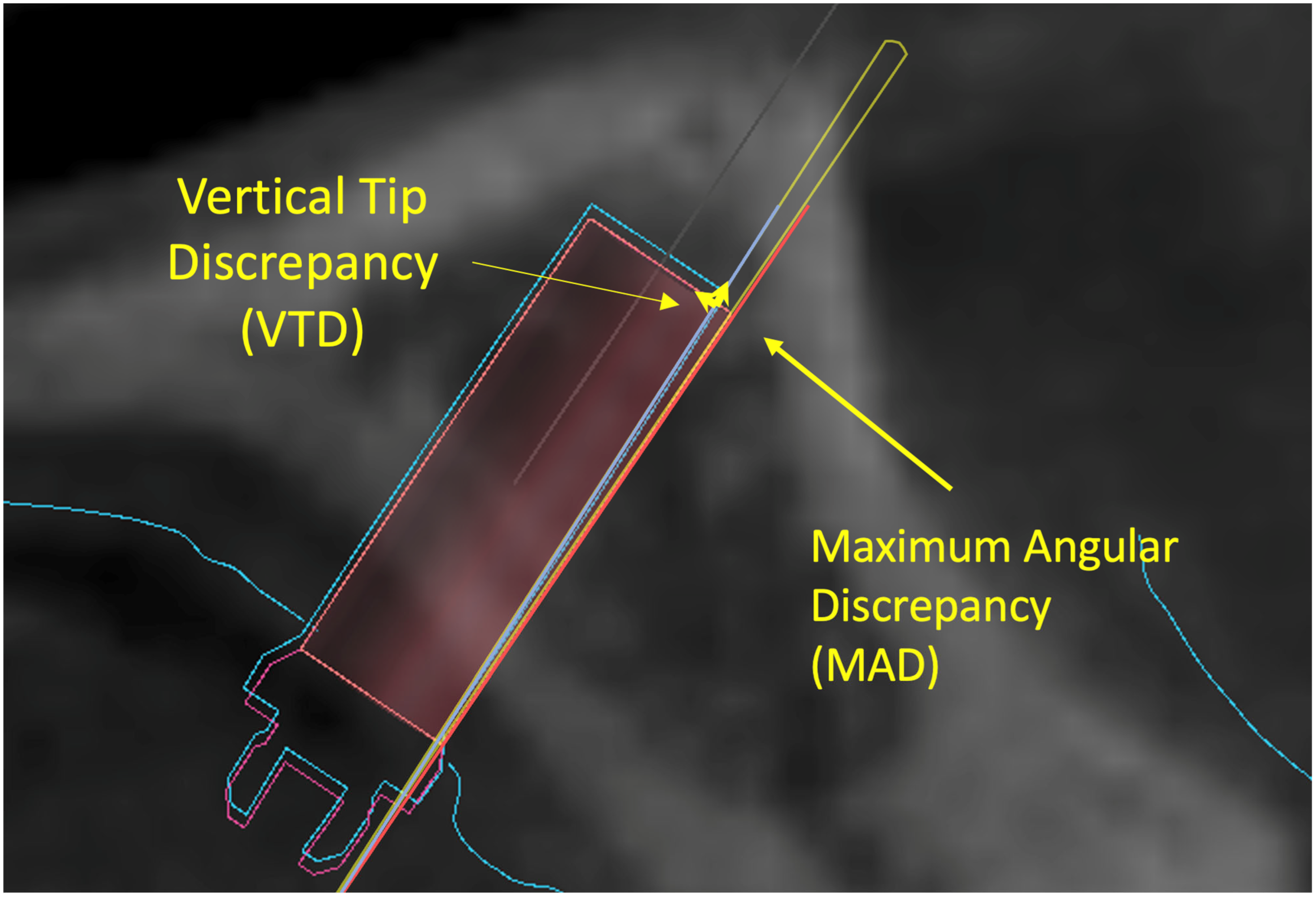
| Hor Head Dmax (mm) | 0.3 | 0.16 | 0.05 | 0.54 |
| Hor Tip Dmax (mm) | 0.66 | 0.21 | 0.38 | 1.04 |
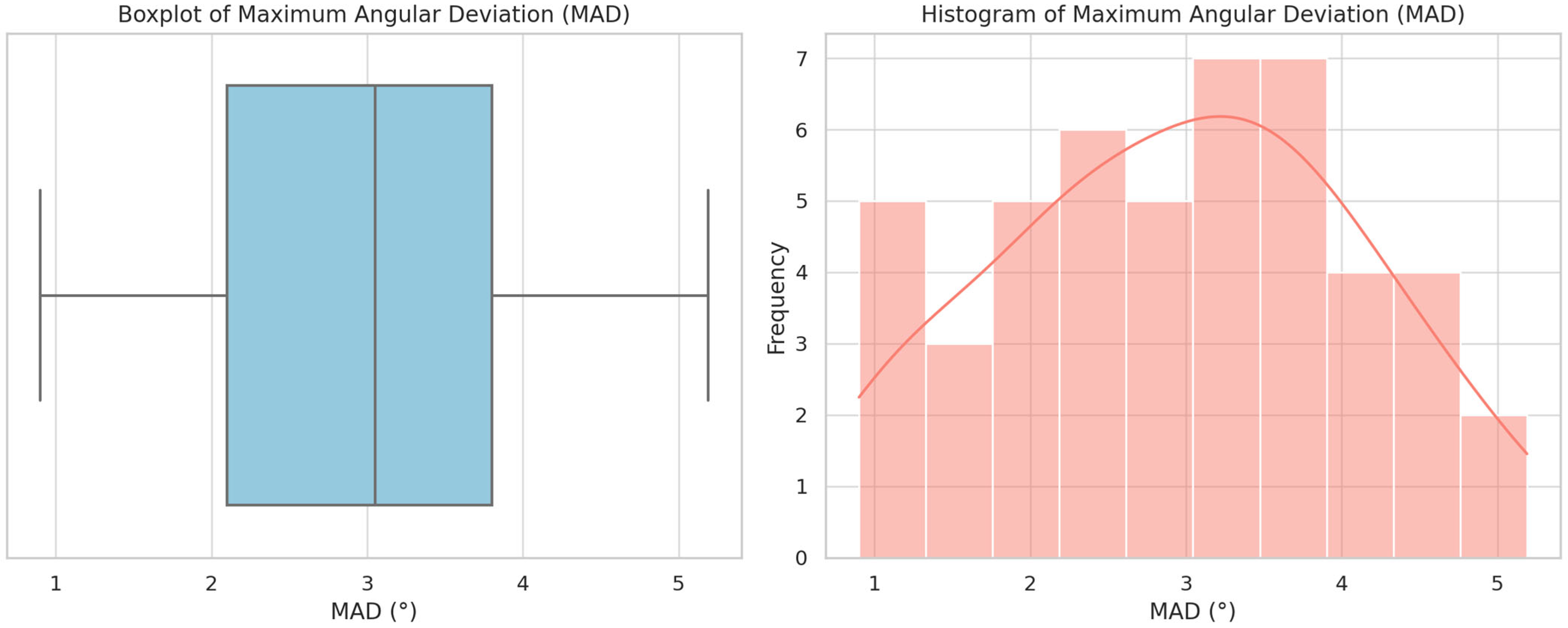
| MAD (°) | 2.95 | 1.13 | 0.9 | 5.19 |
| Vert HD (mm) | 0.35 | 0.21 | 0.06 | 0.66 |
| Vert TD (mm) | 0.67 | 0.67 | 0.07 | 2.16 |
| T-Paired Test | p-Value |
| hor head dx vs. hor tip dx | p < 0.05 |
| hor head sx vs. hor tip sx | p < 0.05 |
| hor head dx vs. hor head sx | NS |
| hor tip dx vs. hor tip sx | NS |
| VHD vs. VTD | p < 0.05 |
| HTDmax vs. HHDmax | NS |
| Spearman test | R-value |
| HTDmax and MAD | NS |
| HHDmax and MAD | NS |
| VTD and MAD | NS |
| VHD and MAD | R < 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellocchio, A.M.; Ciancio, E.; Barbera, S.; Aiello, D.; Portelli, M.; Militi, A.; Nucera, R. Accuracy Assessment of 3D-Printed Surgical Guides for Palatal Miniscrew Placement: A Retrospective Study. Appl. Sci. 2025, 15, 7836. https://doi.org/10.3390/app15147836
Bellocchio AM, Ciancio E, Barbera S, Aiello D, Portelli M, Militi A, Nucera R. Accuracy Assessment of 3D-Printed Surgical Guides for Palatal Miniscrew Placement: A Retrospective Study. Applied Sciences. 2025; 15(14):7836. https://doi.org/10.3390/app15147836
Chicago/Turabian StyleBellocchio, Angela Mirea, Elia Ciancio, Serena Barbera, Domenico Aiello, Marco Portelli, Angela Militi, and Riccardo Nucera. 2025. "Accuracy Assessment of 3D-Printed Surgical Guides for Palatal Miniscrew Placement: A Retrospective Study" Applied Sciences 15, no. 14: 7836. https://doi.org/10.3390/app15147836
APA StyleBellocchio, A. M., Ciancio, E., Barbera, S., Aiello, D., Portelli, M., Militi, A., & Nucera, R. (2025). Accuracy Assessment of 3D-Printed Surgical Guides for Palatal Miniscrew Placement: A Retrospective Study. Applied Sciences, 15(14), 7836. https://doi.org/10.3390/app15147836