

Electrical Stimulation May Improve the Feeding and Nutritional Status of Children with Dysphagia



Abstract
1. Introduction
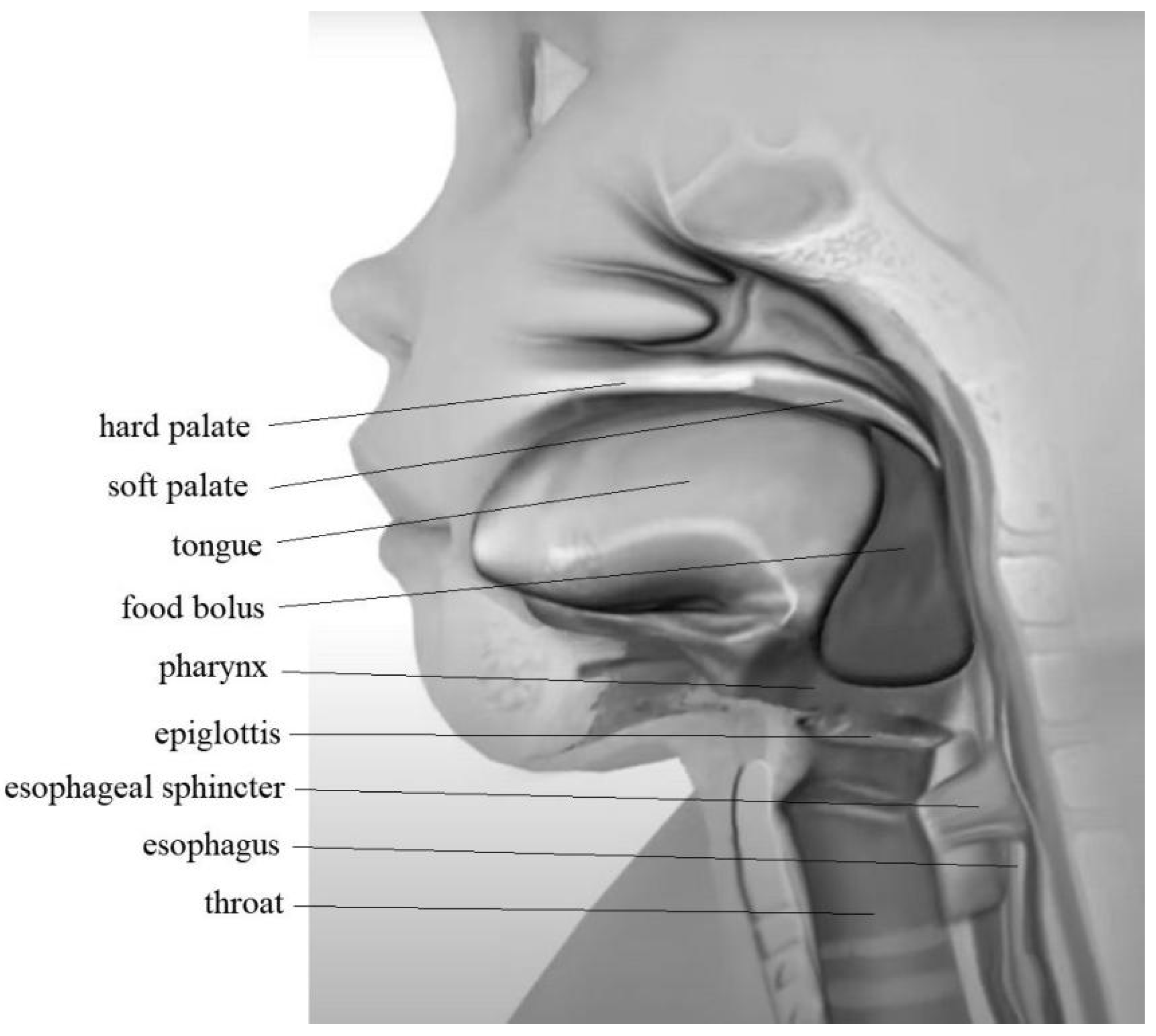
2. The Swallowing Process
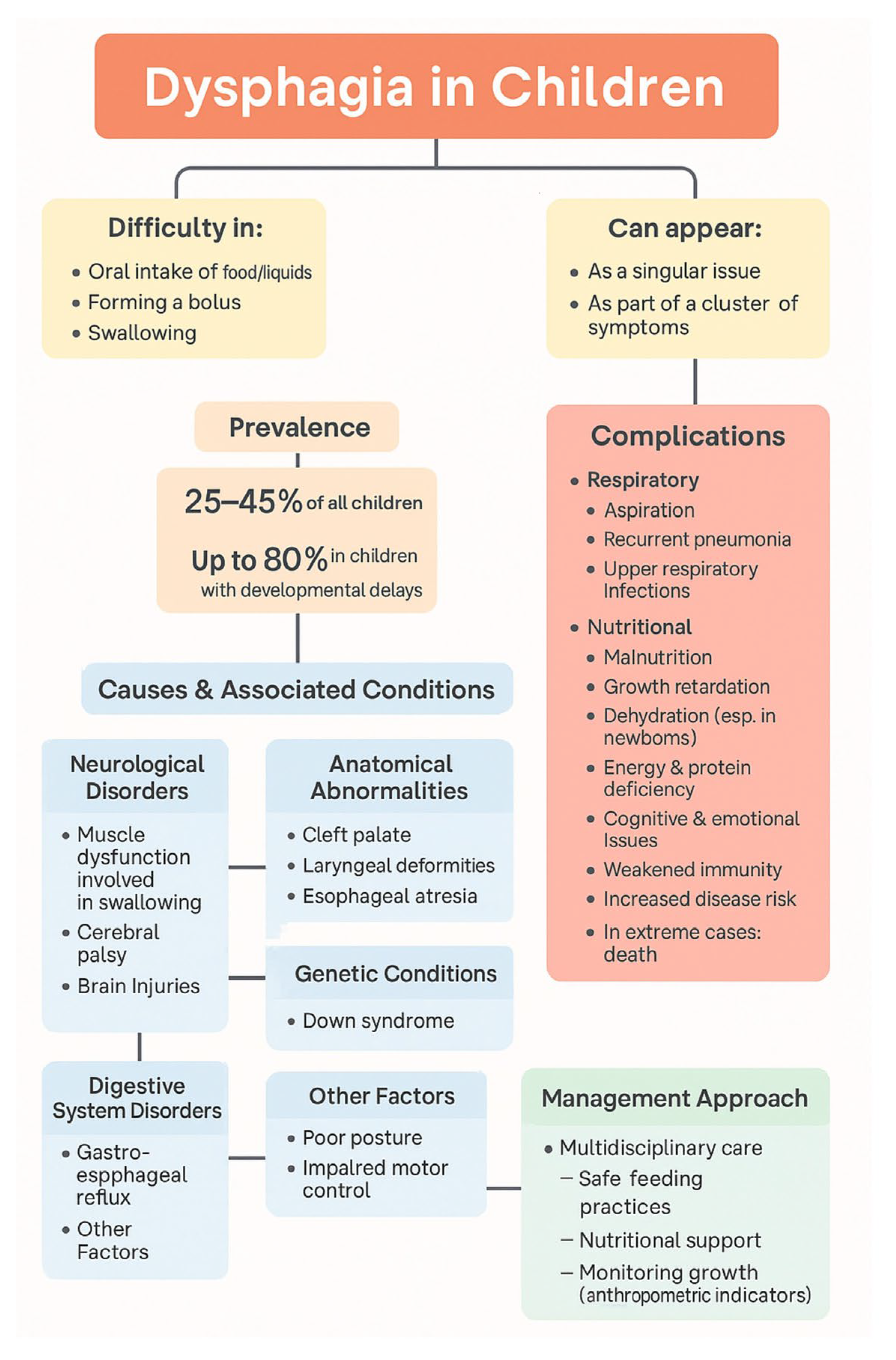
3. Symptoms of Dysphagia
4. Causes of Swallowing Disorder
5. Treatment of Dysphagia
6. Electrical Stimulation
7. NMES in Children with Dysphagia
8. Technical Parameters of NMES
9. Future Perspectives of NMES in Dysphagia Treatment
10. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| NMES | Neuromuscular Electric Stimulation |
| PFD | Pediatric Feeding Disorders |
| WHO | World Health Organization |
References
- Prasse, J.E.; Kikano, G.E. Clinical pediatrics an overview of pediatric dysphagia. Clin. Pediatr. 2009, 48, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Dodrill, P.; Gosa, M.M. Pediatric dysphagia: Physiology, assessment, and management. Ann. Nutr. Metab. 2015, 66, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Tuchman, D. Dysfunctional swallowing in the pediatric patient: Clinical considerations. Dysphagia 1998, 23, 203–208. [Google Scholar] [CrossRef]
- Matsuo, K.; Palmer, J.F. Anatomy and Physiology of Feeding and Swallowing—Normal and Abnormal. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 691–707. [Google Scholar] [CrossRef]
- Ertekin, C.; Aydogdu, I. Neurophysiology of swallowing. Clin. Neurophysiol. 2003, 114, 2226–2244. [Google Scholar] [CrossRef]
- Miller, S.; Jungheim, M.; Kühn, D.; Ptok, M. Electrical stimulation in treatment of pharyngolaryngeal dysfunctions. Folia Phoniatr. Logop. 2013, 65, 154–168. [Google Scholar] [CrossRef]
- Jaafar, N.H.; Othman, A.; Majid, N.A.; Harith, S.; Zabidi-Hussin, Z. Parent-report Instruments for assessing feeding difficulties in children with neurological impairments: A systematic review. Dev. Med. Child. Neurol. 2019, 61, 135–144. [Google Scholar] [CrossRef]
- Lawlor, C.M.; Choi, S. Diagnosis and Management of Pediatric Dysphagia: A Review. JAMA Pediatr. 2019, 173, 91–98. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Barikroo, A. Transcutaneous electrical stimulation and dysphagia rehabilitation: A narrative review. Rehabil. Res. Pract. 2020, 2020, 4865614. [Google Scholar] [CrossRef]
- Sullivan, P.B.; Lambert, B.; Rose, M.; Ford-Adams, M.; Johnson, A.; Griffiths, P. Prevalence and severity of feeding and nutritional problems in children with neurological impairment: Oxford Feeding Study. Dev. Med. Child. Neurol. 2000, 42, 674–680. [Google Scholar] [CrossRef]
- Manikam, R.; Perman, J.A. Pediatric feeding disorders. J. Clin. Gastroenterol. 2000, 30, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Motion, S.; Northstone, K.; Emond, A.; Stucke, S.; Golding, J. Early feeding problems in children with cerebral palsy: Weight and neurodevelopmental outcomes. Dev. Med. Child Neurol. 2002, 44, 40–43. [Google Scholar] [PubMed]
- Sdravou, K.; Fotoulaki, M.; Emmanouilidou-Fotoulaki, E.; Andreoulakis, E.; Makris, G.; Sotiriadou, F.; Printza, A. Feeding Problems in Typically Developing Young Children, a Population-Based Study. Children 2021, 8, 388. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N. The prevalence of pediatric voice and swallowing problems in the United States. Laryngoscope 2015, 125, 746–750. [Google Scholar] [CrossRef]
- Tutor, J.D.; Gosa, M.M. Dysphagia and aspiration in children. Pediatr. Pulmonol. 2012, 47, 321–337. [Google Scholar] [CrossRef]
- Bass, N.H.; Morrell, R.M. The neurology of swallowing. In Dysphagia, Diagnosis and Management; Groher, M.E., Ed.; Butterworth-Heinemann: Boston, MA, USA, 1992; pp. 1–29. [Google Scholar]
- Duffy, K.L. Dysphagia in Children. J. Pediatr. Health Care 2018, 32, 321–329. [Google Scholar] [CrossRef]
- Andreoli, S.M.; Wilson, B.L.; Swanson, C. Neuromuscular electrical stimulation improves feeding and aspiration status in medically complex children undergoing feeding therapy. Int. J. Pediatr. Otorhinolaryngol. 2019, 127, 109646. [Google Scholar] [CrossRef]
- Propp, R.; Gil, P.J.; Marcus, S.; Ren, L.; Cohen, E.; Friedman, J.; Mahant, S. Neuromuscular electrical stimulation for children with dysphagia: Asystematic review. J. Pediatr. Dysphagia Ther. 2024, 12, 45–56. [Google Scholar] [CrossRef]
- Christiaanse, M.E.; Mabe, B.; Russell, G.; Long Simeone, T.; Fortunato, J.; Rubin, B. Neuromuscular electrical stimulation is no more effective than usual care for the treatment of primary dysphagia in children. Pediatr. Pulmonol. 2011, 46, 559–565. [Google Scholar] [CrossRef]
- Phalen, J.A. Managing feeding problems and feeding disorders. Pediatrics Rev. 2013, 34, 549–557. [Google Scholar] [CrossRef]
- Printza, A.; Sdravou, K.; Triaridis, S. Dysphagia Management in Children: Implementation and Perspectives of Flexible Endoscopic Evaluation of Swallowing (FEES). Children 2022, 9, 1857. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A. Evaluation and Treatment of Swallowing Disorders; Pro-Ed, Inc.: Austin, TX, USA, 1998. [Google Scholar]
- Kubitscheck de Oliveira Santos, J.; Côrtes Gama, A.C.; Alves Silvério, K.C.; Cordeiro Diniz Oliveira, N.F. The use of electrical stimulation in speech therapy clinical: An integrative literature review. Braz. J. Speech Ther. 2015, 20, 201–209. [Google Scholar]
- Alamer, A.; Melese, H.; Nigussie, F. Effectiveness of neuromuscular electrical stimulation on post-stroke dysphagia: A systematic review of randomized controlled trials. Clin. Interv. Aging 2020, 15, 1521–1531. [Google Scholar] [CrossRef]
- Diéguez-Pérez, I.; Leirós-Rodríguez, R. Effectiveness of different application parameters of neuromuscular electrical stimulation for the treatment of dysphagia after a stroke: A systematic review. J. Clin. Med. 2020, 9, 2618. [Google Scholar] [CrossRef]
- Chen, Y.W.; Chang, K.H.; Chen, H.C.; Liang, W.M.; Wang, Y.H.; Lin, Y.N. The effects of surface neuromuscular electrical stimulation on post-stroke dysphagia: A systematic review and metaanalysis. Clin. Rehabil. 2016, 30, 24–35. [Google Scholar] [CrossRef]
- Bhatt, A.D.; Goodwin, N.; Cash, E. Impact of transcutaneous neuromuscular electrical stimulation on dysphagia in patients with head and neck cancer treated with definitive chemoradiation. Head. Neck 2015, 37, 1051–1056. [Google Scholar] [CrossRef]
- Benfer, K.A.; Weir, K.A.; Boyd, R.N. Clinimetrics of measures of oropharyngeal dysphagia for preschool children with cerebral palsy and neurodevelopmental disabilities: A systematic review. Dev. Med. Child. Neurol. 2012, 54, 784–795. [Google Scholar] [CrossRef]
- Terré, R.; Mearin, F. A randomized controlled study of neuromuscular electrical stimulation in oropharyngeal dysphagia secondary to acquired brain injury. Eur. J. Neurol. 2015, 22, 687-e44. [Google Scholar] [CrossRef]
- Simonelli, M.; Ruoppolo, G.; Iosa, M.; Morone, G.; Fusco, A.; Grasso, M.G.; Gallo, A.; Paolucci, S. A stimulus for eating. The use of neuromuscular transcutaneous electrical stimulation in patients affected by severe dysphagia after subacute stroke: A pilot randomized controlled trial. NeuroRehabilitation 2019, 44, 103–110. [Google Scholar] [CrossRef]
- Kushner, D.S.; Peters, K.; Eroglu, S.T.; Perless-Carroll, M.; Johnson-Greene, D. Neuromuscular electrical stimulation efficacy in acute stroke feeding tube-dependent dysphagia during inpatient rehabilitation. Am. J. Phys. Med. Rehabil. 2013, 92, 486–495. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, B.H.; Park, Y.H. Analysis of Dysphagia Patterns Using a Modified Barium Swallowing Test Following Treatment of Head and Neck Cancer. Yonsei Med. J. 2015, 56, 1221–1226. [Google Scholar] [CrossRef]
- Cakmak, T.E.; Sen, E.I.; Doruk, C.; Sen., C.; Sezikli, S.; Yaliman, A. The Effects of Neuromuscular Electrical Stimulation on Swallowing Functions in Post-stroke Dysphagia: A Randomized Controlled Trial. Dysphagia 2023, 38, 874–885. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, X.; Qiao, J.; Song, G.; Xu, Y.; Zhang, Y.; Xu, D.; Gao, W.; Li, Y.; Xu, C. Effects of transcutaneous neuromuscular electrical stimulation on swallowing disorders: A systematic review and meta-analysis. Am. J. Phys. Med. Rehabil. 2020, 99, 701–711. [Google Scholar] [CrossRef]
- Schwemmle, C.; Arens, C. Feeding, eating, and swallowing disorders in infants and children: An overview. Int. J. Pediatr. Otorhinolaryngol. 2018, 112, 151–158. [Google Scholar]
- Florie, M.G.M.H.; Pilz, W.; Dijkman, R.H.; Kremer, B.; Wiersma, A.; Winkens, B.; Baijens, L.W.J. The Effect of Cranial Nerve Stimulation on Swallowing: A Systematic Review. Dysphagia 2020, 36, 216–230. [Google Scholar] [CrossRef]
- Kilinc, D.D.; Mansiz, D. Myofunctional orofacial examination tests: A literature review. J. Orofacial Res. 2023, 12, 201–215. [Google Scholar] [CrossRef]
- Hennessy, M.; Goldenberg, D. Surgical anatomy and physiology of swallowing. Operative Tech. Otolaryngol. Head. Neck Surg. 2016, 27, 60–66. [Google Scholar] [CrossRef]
- Costa, M.M.B. Neural control of swallowing. Arq. Gastroenterol. 2018, 55, 61–75. [Google Scholar] [CrossRef]
- Feher, J. Mouth and Esophagus. In Quantitative Human Physiology, 2nd ed.; Feher, J., Ed.; Academic Press: Cambridge, MA, USA, 2017; pp. 771–784. [Google Scholar]
- Goday, P.S.; Huh, S.Y.; Silverman, A.; Lukens, C.T.; Dodrill, P.; Cohen, S.C.; Delaney, A.L.; Feuling, M.B.; Noel, R.J.; Gisel, E.; et al. Pediatric Feeding Disorder: Consensus Definition and Conceptual Framework. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 124–129. [Google Scholar] [CrossRef]
- Mari, A.; Sweis, R. Assessment and management of dysphagia and achalasia. Clin. Med. 2021, 21, 119–123. [Google Scholar] [CrossRef]
- Russo, G.; Strisciugli, C. Dysphagia: A practical approach. Glob. Pediatr. 2024, 7, 100136. [Google Scholar] [CrossRef]
- Weir, K.; McMahon, S.; Barry, L. Clinical signs and symptoms of oropharyngeal aspiration and dysphagia in children. Eur. Res. J. 2009, 33, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Yoon, I.J.; Shin, J.H.; Park, E.S. Effects of Neuromuscular Electrical Stimulation on the Swallowing Function in a Child—A Case Report. J. Korean Dysphagia Soc. 2018, 2, 110–116. [Google Scholar] [CrossRef]
- Winnicka, E. Therapy of dysphagia using electrostimulation: Experience in pediatric population. Gastroenterol. Klin. 2019, 15, 85–92. [Google Scholar]
- Hewetson, R.; Singh, S. The lived experience of mothers of children with chronic feeding and/or swallowing difficulties. Dysphagia 2009, 24, 322–332. [Google Scholar] [CrossRef]
- Arslan, S.S.; Soyer, T.; Demir, N.; Yalcın, S.; Karaduman, A.; Karnak, I.; Tanyel, F.C. Effect of swallowing rehabilitation protocol on swallowing function in patients with esophageal atresia and/or tracheoesophageal fistula. Eur. J. Pediatr. Surg. 2017, 27, 526–532. [Google Scholar] [CrossRef]
- Attrill, S.; White, S.; Murray, J.; Hammond, S.; Doeltgen, S. Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: A systematic review. BMC Health Serv. Res. 2018, 18, 594. [Google Scholar] [CrossRef]
- Dziewas, R.; Beck, A.M.; Clave, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.E.; Leischker, A.; Martino, R.; Pluschinski, P.; Roester, A.; et al. Recognizing the importance of dysphagia: Stumbling blocks and stepping stones in the twenty-first century. Dysphagia 2017, 32, 78–82. [Google Scholar] [CrossRef]
- Todorović, J.; Zelić, M.; Jerkić, L. Eating and Swallowing Disorders in Children with Cleft Lip and/or Palate. Acta Fac. Med. Naiss. 2022, 39, 5–13. [Google Scholar] [CrossRef]
- Dharmaraj, R.; Elmaoued, R.; Alkhouri, R.; Vohra, P.; Castillo, R.O. Evaluation and Management of Pediatric Feeding Disorder. Gastrointest. Disord. 2023, 5, 75–86. [Google Scholar] [CrossRef]
- Lanzoni, G.; Sembenini, C.; Gastaldo, S.; Leonardi, L.; Bentivoglio, V.P.; Faggian, G.; Bosa, L.; Gaio, P.; Cananzi, M. Esophageal Dysphagia in Children: State of the Art and Proposal for a Symptom-Based Diagnostic Approach. Front. Pediatr. 2022, 10, 885308. [Google Scholar] [CrossRef] [PubMed]
- Zaher, E.A.; Patel, P.; Atia, G.; Sigdel, S. Distal Esophageal Spasm: An Updated Review. Cureus 2023, 15, e41504. [Google Scholar] [CrossRef] [PubMed]
- Sirinawasatien, A.; Sakulthongthawin, P. Manometrically jackhammer esophagus with fluoroscopically/endoscopically distal esophageal spasm: A case report. BMC Gastroenterol. 2021, 21, 222. [Google Scholar] [CrossRef]
- Garcia, D.J.; Nashwan, A.J.; Al-Ansari, A.N. Congenital and Iatrogenic Esophageal Diverticula in Infants and Children: A Case Series of Four Patients. Cureus 2024, 16, e68806. [Google Scholar] [CrossRef]
- Young, E.; Philpott, H. Pathophysiology of Dysphagia in Eosinophilic Esophagitis: Causes, Consequences, and Management. Dig. Dis. Sci. 2022, 67, 1101–1115. [Google Scholar] [CrossRef]
- Peng, D.; Tan, Y.; Li, C.; Lv, L.; Zhu, H.; Liang, C.; Li, R.; Liu, D. Peroral Endoscopic Myotomy for Pediatric Achalasia: A Retrospective Analysis of 21 Cases With a Minimum Follow-Up of 5 Years. Front. Pediatr. 2022, 10, 845103. [Google Scholar] [CrossRef]
- Ortiz Pérez, P.; Valero-Arredondo, I.; Torcuato-Rubio, E.; Herrador-López, M.; Martín-Masot, R.; Navas-López, V.M. Nutritional Issues in Children with Dysphagia. Nutrients 2024, 16, 1590. [Google Scholar] [CrossRef]
- Ballesteros-Pomar, M.D.; Cherubini, A.; Keller, H.; Lam, P.; Rolland, Y.; Simmons, S.F. Texture-Modified Diet for Improving the Management of Oropharyngeal Dysphagia in Nursing Home Residents: An Expert Review. J. Nutr. Health Age 2020, 24, 576–581. [Google Scholar] [CrossRef]
- Lazarus, C.L. History of the use and impact of compensatory strategies in management of swallowing disorders. Dysphagia 2017, 32, 3–10. [Google Scholar] [CrossRef]
- Dipasquale, V.; Cucinotta, U.; Alibrandi, A.; Laganà, F.; Ramistella, V.; Romano, C. Early Tube Feeding Improves Nutritional Outcomes in Children with Neurological Disabilities: A Retrospective Cohort Study. Nutrients 2023, 15, 2875. [Google Scholar] [CrossRef]
- Miller, S.; Peters, K.; Ptok, M. Review of the effectiveness of neuromuscular electrical stimulation in the treatment of dysphagia—An update. J. Clin. Rehabil. 2022, 36, 455–466. [Google Scholar]
- Frost, J.; Robinson, H.F.; Hibberd, J. A comparison of neuromuscular electrical stimulation and traditional therapy, versus traditional therapy in patients with longstanding dysphagia. Curr. Oppin. Otolaryngol. Head Neck Surg. 2018, 26, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.H.; Jang, J.; Jang, E.G.; Park, Y.; Lee, S.Y.; Kim, B.R.; Park, D.; Park, S.; Hwang, H.; Kim, N.H.; et al. Clinical effectiveness of the sequential 4-channel NMES compared with that of the conventional 2-channel NMES for the treatment of dysphagia in a prospective double-blind randomized controlled study. J. Neuroeng. Rehabil. 2021, 18, 90. [Google Scholar] [CrossRef] [PubMed]
- Pechkham, P. Principles of electrical stimulation, Top. Spinal Cord. Inj. Rehabil. 1999, 5, 1–5. [Google Scholar] [CrossRef]
- Ryu, J.S.; Kang, J.Y.; Park, J.Y.; Nam, S.Y.; Choi, S.H.; Roh, J.L.; Kim, S.Y.; Choi, K.H. The effect of electrical stimulation therapy on dysphagia following treatment for head and neck cancer. Oral. Oncol. 2009, 45, 665–668. [Google Scholar] [CrossRef]
- Bengisu, S.; Demir, N.; Krespi, Y. Effectiveness of Conventional Dysphagia Therapy (CDT), Neuromuscular Electrical Stimulation (NMES), and Transcranial Direct Current Stimulation (tDCS) in Acute Post-Stroke Dysphagia: A Comparative Evaluation. Dysphagia 2024, 39, 77–91. [Google Scholar] [CrossRef]
- Guimarães, B.T.L.; Lepri, J.R. Możliwości zastosowania elektrostymulacji w motoryce twarzowo-ustnej. J. Orofac. Ther. 2024, 18, 45–53. [Google Scholar]
- Clark, H.; Lazarus, C.; Arvedson, J.; Schooling, T.; Frymark, T. Evidence-based systematic review: Effects of neuromuscular electrical stimulation on swallowing and neural activation. Am. J. Speech Lang. Pathol. 2009, 18, 361–375. [Google Scholar] [CrossRef]
- Eimoto, K.; Nagai, K.; Nakao, Y.; Uchiyama, Y.; Domen, K. Swallowing Rehabilitation With Neuromuscular Electrical Stimulation for Sarcopenic Dysphagia:A Case Report. Cureus 2024, 16, e59256. [Google Scholar]
- Elluru, R. Contemporary Trends in the Diagnosis and Management of Pediatric Dysphagia. Curr. Treat. Opt. Pediatr. 2024, 10, 295–300. [Google Scholar] [CrossRef]
- Carnaby-Mann, G.D.; Crary, M.A. Examining the evidence on neuromuscular electrical stimulation for swallowing. Arch. Otolaryngol. Head. Neck Surg. 2007, 133, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.L.; Liu, T.Y.; Huang, Y.C.; Leong, C.P. Functional outcome in acute stroke patients with oropharyngeal dysphagia after swallowing therapy. J. Stroke Cerebrovasc. Dis. 2014, 23, 2547–2553. [Google Scholar] [CrossRef]
- Permsirivanich, W.; Tipchatyotin, S.; Wongchai, M. Comparing the effect of rehabilitation swallowing therapy vs. neuromuscular electrical stimulation therapy among stroke patients with persistent pharyngeal dysphagia: A randomized controlled study. J. Med. Ass Thail. 2009, 92, 265. [Google Scholar]
- Blumenfeld, L.; Hahn, Y.; Lepage, A.; Leonard, R. Transcutaneous electrical stimulation versus traditional dysphagia therapy: A nonconcurrent cohort study. Otolaryngol. Head Neck Surg. 2006, 135, 754–757. [Google Scholar] [CrossRef]
- Pownall, S.; Enderby, P.; Sproson, L. Electrical stimulation for the treatment of dysphagia. In Electroceuts; Springer: Cham, Switzerland, 2017; pp. 137–156. [Google Scholar]
- Lv, J.; Zhu, M.; Zhang, Y. Effects of different intensity neuromuscular electrical stimulation on dysphagia in children with cerebral palsy. Chin. J. Rehabil. Med. 2019, 34, 159–164. [Google Scholar]
- El-Sheikh, A.; El-Tohamy, A.; Abd El-Aziz, B. Neuromuscular electrical stimulation therapy on controlling dysphagia in spastic cerebral palsy: A randomized controlled clinical trial. Polish J. Physiother. 2020, 20, 194–198. [Google Scholar]
- Ma, S.R.; Choi, J.B. Effect of electrical stimulation on aspiration in children with cerebral palsy and dysphagia. J. Phys. Ther. Sci. 2019, 31, 93–94. [Google Scholar] [CrossRef]
- Gao, S.; Gao, D.; Su, N.; Ge, K.J.; Liu, Y.M. Effect of acupuncture at proximal and distal acupoints combined with neuromuscular electrical stimulation on children with cerebral palsy salivation. Chin. Acupunct. Moxibustion 2018, 38, 825–830. [Google Scholar]
- Rice, K.L. Neuromuscular electrical stimulation in the early intervention population: A series of five case studies. Int. J. Allied Heal. Sci. Pract. 2012, 10, 9. [Google Scholar] [CrossRef]
- Propp, K.; Jiang, H.; Thoyre, S. Neuromuscular electrical stimulation for children with dysphagia: A systematic review. Phys. Occup. Ther. Pediatr. 2022, 42, 123–140. [Google Scholar] [CrossRef]
- Marcus, S.; Friedman, J.N.; Lacombe-Duncan, A.; Mahant, S. Neuromuscular electrical stimulation to treat dysphagia in infants and young children with neurological impairment. Clin. Pediatr. 2019, 58, 150–156. [Google Scholar]
- Andreoli, M.T.; Langmore, S.E.; Sohn, H. Electrical stimulation therapy for severe dysphagia in medically complex children: A case series. Int. J. Pediatr. Otorhinolaryngol. 2019, 124, 117–122. [Google Scholar]
- Winnicka, K.; Kowalska, K.; Szczepańska, J.; Mańczak, M. Improvement of swallowing function due to neuromuscular electrical stimulation in children with primary dysphagia. Polish J. Pediatr. 2024, 99, 54–61. [Google Scholar] [CrossRef]
- Christiaanse, M.E.; Mabe, B.; Russell, G. Evaluation of the use of neuromuscular electrical stimulation in children with dysphagia. Pediatr. Pulmonol. 2011, 46, 1031–1035. [Google Scholar] [CrossRef]
- Ma, L.; Choi, M. Neuromuscular electrical stimulation for children with dysphagia: A case study. Korean J. Pediatr. 2019, 62, 377–381. [Google Scholar]
- Song, W.J.; Park, J.H.; Lee, J.H.; Kim, M.Y. The effect of neuromuscular electrical stimulation on swallowing function in children with cerebral palsy: A randomized controlled trial. Hong Kong J. Occup. Therap 2015, 25, 30–35. [Google Scholar] [CrossRef]
- Freed, M.L.; Freed, L.; Chatburn, R.L.; Christian, M. Electrical stimulation for swallowing disorders caused by stroke. Dysphagia 2001, 16, 171–177. [Google Scholar]
- Ekberg, O.; Hamdy, S.; Woisard, V.; Wuttge-Hannig, A.; Ortega, P. Social and psychological burden of dysphagia: Its impact on diagnosis and treatment. Dysphagia 2002, 17, 139–146. [Google Scholar] [CrossRef]
- Ludlow, C.L.; Humbert, I.; Saxon, K.; Poletto, C.; Sonies, B.; Crujido, L. Effects of surface electrical stimulation during swallowing in chronic pharyngeal dysphagia. Dysphagia 2007, 22, 1–10. [Google Scholar] [CrossRef]
- Blumenfeld, L.; Hahn, Y.; Lepage, A.; Leonard, R. Transcutaneous neuromuscular electrical stimulation for dysphagia: A review of the literature. Otolaryngol. Head Neck Surg. 2006, 135, 754–757. [Google Scholar] [CrossRef]
- Guo, X.; Mu, H.; Sun, Y.; Wang, J.; Wei, J. Analysis of the Improvement Effect of Combined Application of Oral Rehabilitation Training and Neuromuscular Electrical Stimulation on Pediatric Swallowing Disorders. Int. J. Neurosci. 2024, 1–7, Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Zdanowicz, K.; Rycyk, A.; Lebensztejn, D.M.; Daniluk, U. Dysphagia Among Children—A Single-Center Experience. J. Clin. Med. 2025, 14, 2906. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.L.; Parker, K. Neuromuscular Electrical Stimulation—A Practical Guide; Los Amigos Research and Education Institute: Downey, CA, USA, 2006. [Google Scholar]
- Petrofsky, J.S. Electrical stimulation: Neurophysiological basis and application. Crit. Rev. Biomed. Eng. 2001, 29, 59–124. [Google Scholar]
- Chow, T.; Boutet, A.; Loh, A.; Germann, J.; Elias, G.J.B.; Hutchison, W.D.; Lozano, A.M. Kilohertz-frequency stimulation of the nervous system: A review of underlying mechanisms. Brain Funct. 2021, 14, 513–530. [Google Scholar]
- Doucet, B.M.; Lam, A.; Griffin, L. Neuromuscular electrical stimulation for skeletal muscle function. Yale J. Biol. Med. 2012, 85, 201–215. [Google Scholar]
- Robinson, A.J.; Snyder-Mackler, L. Clinical Electrophysiology: Electrotherapy and Electrophysiologic Testing, 3rd ed.; Lippincott Williams & Wilkins: Baltimore, PA, USA, 2008. [Google Scholar]
- Maffiuletti, N.A. Physiological and methodological considerations for the use of neuromuscular electrical stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–234. [Google Scholar] [CrossRef]
- Sillen, M.J.H.; Franssen, F.M.E.; Gosker, H.R.; Wouters, E.F.M.; Spruit, M.A. Metabolic and Structural Changes in Lower-Limb Skeletal Muscle Following Neuromuscular Electrical Stimulation: A Systematic Review. PLoS ONE 2013, 9, e69391. [Google Scholar] [CrossRef]
- Lake, D.A. Neuromuscular electrical stimulation. An overview and its application in the treatment of sports injuries. Sports Med. 1992, 13, 320–336. [Google Scholar] [CrossRef]
- Ward, A.R. Electrical stimulation using kilohertz-frequency alternating current. Phys. Ther. Rev. 2009, 89, 181–190. [Google Scholar] [CrossRef]
- Bax, L.; Staes, F.; Verhagen, A. Does Neuromuscular Electrical Stimulation Strengthen the Quadriceps Femoris? Sports Med. 2005, 35, 191–212. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Gondin, J.; Place, N.; Stevens-Lapsley, J.; Vivodtzev, I.; Minetto, M.A. Clinical Use of Neuromuscular Electrical Stimulation for Neuromuscular Rehabilitation: What Are We Overlooking? Arch. Phys. Med. Rehabil. 2018, 99, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Ward, A.R.; Shkuratova, N. Russian electrical stimulation: The early experiments. Phys. Ther. 2002, 82, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Oh, D.H.; Chang, M.Y. Effects of sensory stimulation using interferential current on swallowing function in children with cerebral palsy: A pilot study. Ann. Rehabil. Med. 2017, 41, 828–835. [Google Scholar]
- Furuta, T.; Takemura, M.; Tsujita, J.; Oku, Y. Interferential electric stimulation applied to the neck increases swallowing frequency. Dysphagia 2012, 27, 94–100. [Google Scholar] [CrossRef]
- Assoratgoon, I.; Shiraishi, N.; Tagaino, R.; Ogawa, T.; Sasaki, K. Sensory neuromuscular electrical stimulation for dysphagia rehabilitation: A literature review. J. Oral Rehabil. 2022, 50, 157–164. [Google Scholar] [CrossRef]
- Ebdah, S. Neuromuscular Electrical Stimulation for Dysphagia Treatment: Adoption, Perceived Barriers, and Clinical Practices. Am. J. Speech Lang. Pathol. 2024, 33, 2839–2854. [Google Scholar] [CrossRef]
- Shune, S.; Moon, J.B. Neuromuscular Electrical Stimulation in Dysphagia Management: Clinician Use and Perceived Barriers. Contemp. Issues Commun. Sci. Disord. 2012, 39, 55–68. [Google Scholar] [CrossRef]
- Chang, M.C.; Park, J.S.; Lee, B.J.; Park, D. Effectiveness of pharmacologic treatment for dysphagia in Parkinson’s disease: A narrative review. Neurol. Sci. 2020, 42, 513–519. [Google Scholar] [CrossRef]
- Morgan, T.A.; Dodrill, P.; Ward, E.C. Interventions for oropharyngeal dysphagia in children with neurological impairment. Cochrane Database Syst. Rev. 2012, 10, CD009456. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| NMES | Traditional Therapy | Criterion |
|---|---|---|
| Electrical stimulation of the muscles responsible for swallowing | Muscle activation through manual massage or the patient’s intentional exercises | Mechanism of Action |
| Passive (electrodes are attached, allowing the patient to focus on other activities) | Passive–active (exercises controlled by the patient or passive manual therapy without the possibility to engage in other tasks) | Type of Activity |
| Requires specialized equipment | It can be performed without any devices | Equipment |
| High—requires precise electrode placement | Lower—relatively easy to learn and implement by parents | Application Complexity |
| May require several sessions to get used to the stimulation | Variable and less predictable adaptation time | Patient Adaptation Time |
| Muscle stimulation can be quantified using device parameters | Difficult to objectively measure the strength of muscle contractions during exercises | Possibility of Objective Evaluation |
| Authors/Year | Study Type | Participants | Population | Treatment Outcomes | Adverse Events |
|---|---|---|---|---|---|
| Propp et al., 2022 [85] | Systematic review | 393 | Children with oropharyngeal dysphagia, including neurological disorders | Improved swallowing function; SMD from 0.18 to 1.49 | Rare; no serious events |
| Marcus et al., 2019 [86] | Prospective pilot | 10 | Infants and young children with severe dysphagia and neurological impairment | 100% improvement in swallowing; 5 achieved oral feeding | Mild skin irritation |
| Andreoli et al., 2019 [87] | Case series | 186 | Children with severe dysphagia | Improvement in feeding and reduced aspiration | Not reported |
| Winnicka et al., 2024 [88] | Observational | 20 | Children with primary dysphagia | Improved swallowing; reduced enteral feeding | No serious events |
| Christiaanse et al., 2011 [89] | Retrospective | 186 | Children with primary and acquired dysphagia | No improvement in primary; improvement in acquired dysphagia | Not reported |
| Ma and Choi, 2019 [90] | Interventional | 5 | Children with cerebral palsy | Reduced aspiration after 4 weeks | Not reported |
| Song et al., 2015 [91] | RCT | 20 | Children with cerebral palsy | Better swallowing outcomes than control group | Not reported |
| Advantages | Disadvantages |
|---|---|
| Increased muscle strength and activity | Lack of conclusive clinical evidence |
| Applicability in patients with severe dysphagia | Risk of incorrect application |
| Neuroplasticity | Cost and limited accessibility |
| Integration with other methods | Discomfort or lack of patient cooperation |
| Parameter | Range/Example | Clinical Significance | Source |
|---|---|---|---|
| Frequency (Hz) | 20–50 Hz | Higher frequencies produce stronger contractions but lead to faster muscle fatigue | Maffiuletti, 2010; Sillen et al., 2013 [103,104] |
| Pulse width (µs) | 200–400 µs | Wider pulses activate more motor units, increasing effectiveness | Lake, 1992; Ward, 2009 [105,106] |
| Contraction/rest time | 5–10 s/10–30 s | Rest periods reduce muscle fatigue and improve patient tolerance | Bax et al., 2005 [107] |
| Intensity (mA) | Individually adjusted | It should be sufficient to elicit a functional contraction without excessive discomfort | Maffiuletti, 2018 [108] |
| Waveform type | Symmetrical/asymmetrical | Symmetrical impulses are generally more comfortable, especially for superficial muscles | Ward and Shkuratova, 2002 [109] |
| Therapy duration | 15–30 min per session | Therapeutic effects are observed with regular sessions of 15–30 min | Sillen et al., 2013 [104] |
| Therapy frequency | 3–5 times per week | More frequent sessions enhance the cumulative effect of muscle training | Maffiuletti, 2018 [108] |
| Parameter | Device | ||
|---|---|---|---|
| VitalStim Plus | Ecostim | Vitalstim | |
| Type of therapy | NMES, sEMG biofeedback (swallowing) | TENS, EMS, massage | NMES (swallowing, facial muscles) |
| Pulse frequency | Adjustable; tailored to therapy needs | 2–100 Hz | 30–80 Hz (typical) |
| Pulse width | Adjustable; tailored to therapy needs | 100–300 µs | 200–300 µs (typical) |
| Number of channels | 4 (allows simultaneous therapy of different muscle groups) | 2 | 2 |
| Biofeedback (sEMG) | Yes (visual and auditory) | No | No |
| User interface | Touchscreen, color display, connectable to a computer or tablet | Backlit, LCD display | Simple, analog |
| Therapy programs | Predefined programs and the ability to create custom ones | 22 programs; 6 with customizable parameters | Standard protocols |
| Clinical application | Advanced dysphagia therapy with biofeedback | Pain relief, muscle training, massage | Dysphagia therapy, facial muscle rehabilitation |
| Additional features | Bluetooth, micro SD port, educational videos, anatomical library, therapy games | Belt clip, safety lock, battery-powered | — |
| Price | High | Low | Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budkowska, M.; Kolanowski, W. Electrical Stimulation May Improve the Feeding and Nutritional Status of Children with Dysphagia. Appl. Sci. 2025, 15, 5727. https://doi.org/10.3390/app15105727
Budkowska M, Kolanowski W. Electrical Stimulation May Improve the Feeding and Nutritional Status of Children with Dysphagia. Applied Sciences. 2025; 15(10):5727. https://doi.org/10.3390/app15105727
Chicago/Turabian StyleBudkowska, Monika, and Wojciech Kolanowski. 2025. "Electrical Stimulation May Improve the Feeding and Nutritional Status of Children with Dysphagia" Applied Sciences 15, no. 10: 5727. https://doi.org/10.3390/app15105727
APA StyleBudkowska, M., & Kolanowski, W. (2025). Electrical Stimulation May Improve the Feeding and Nutritional Status of Children with Dysphagia. Applied Sciences, 15(10), 5727. https://doi.org/10.3390/app15105727