
Texture Analysis in [18F]-Fluciclovine PET/CT Aids to Detect Prostate Cancer Biochemical Relapse: Report of a Preliminary Experience

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
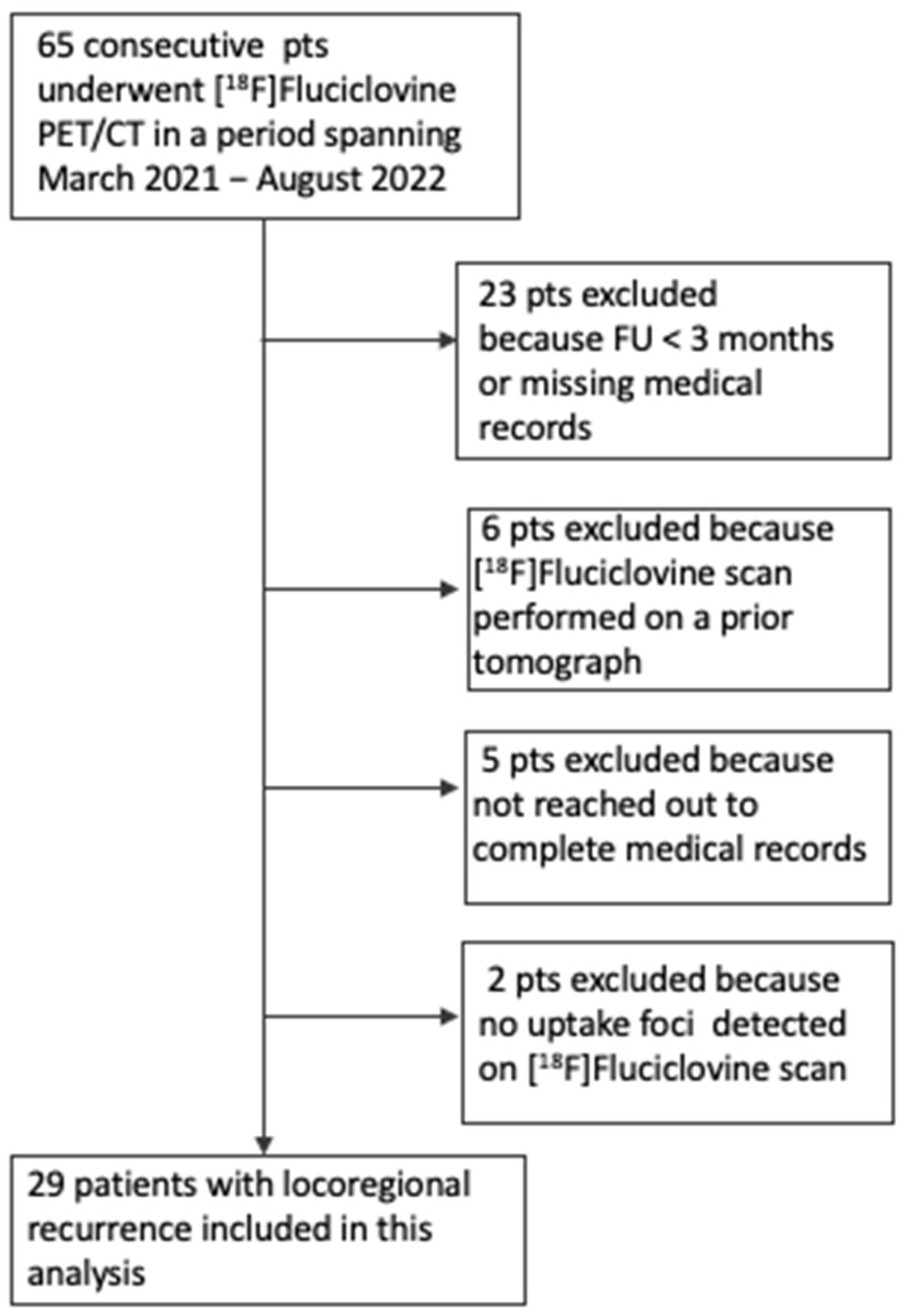
2.1. Population
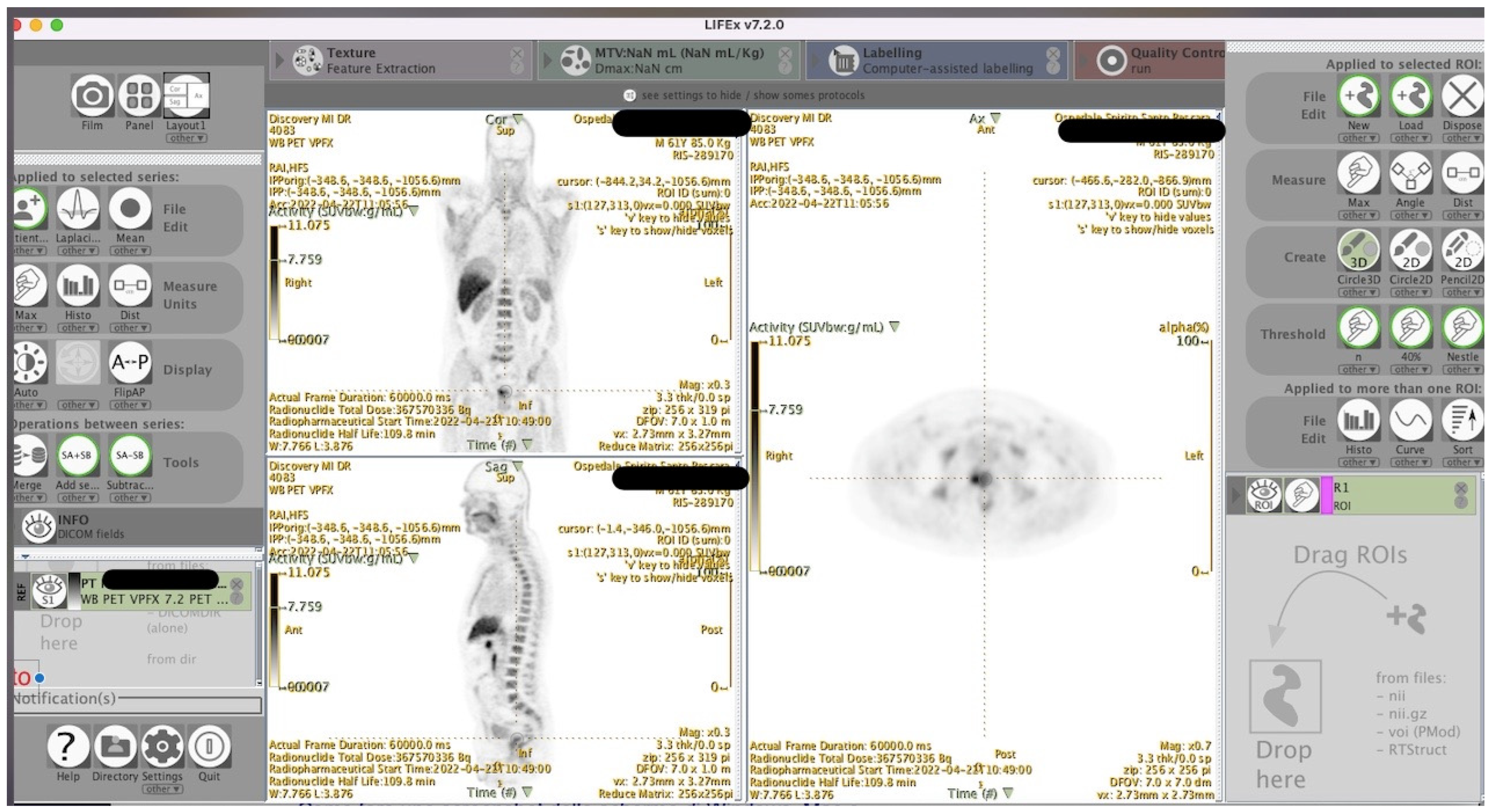
2.2. Image Acquisition
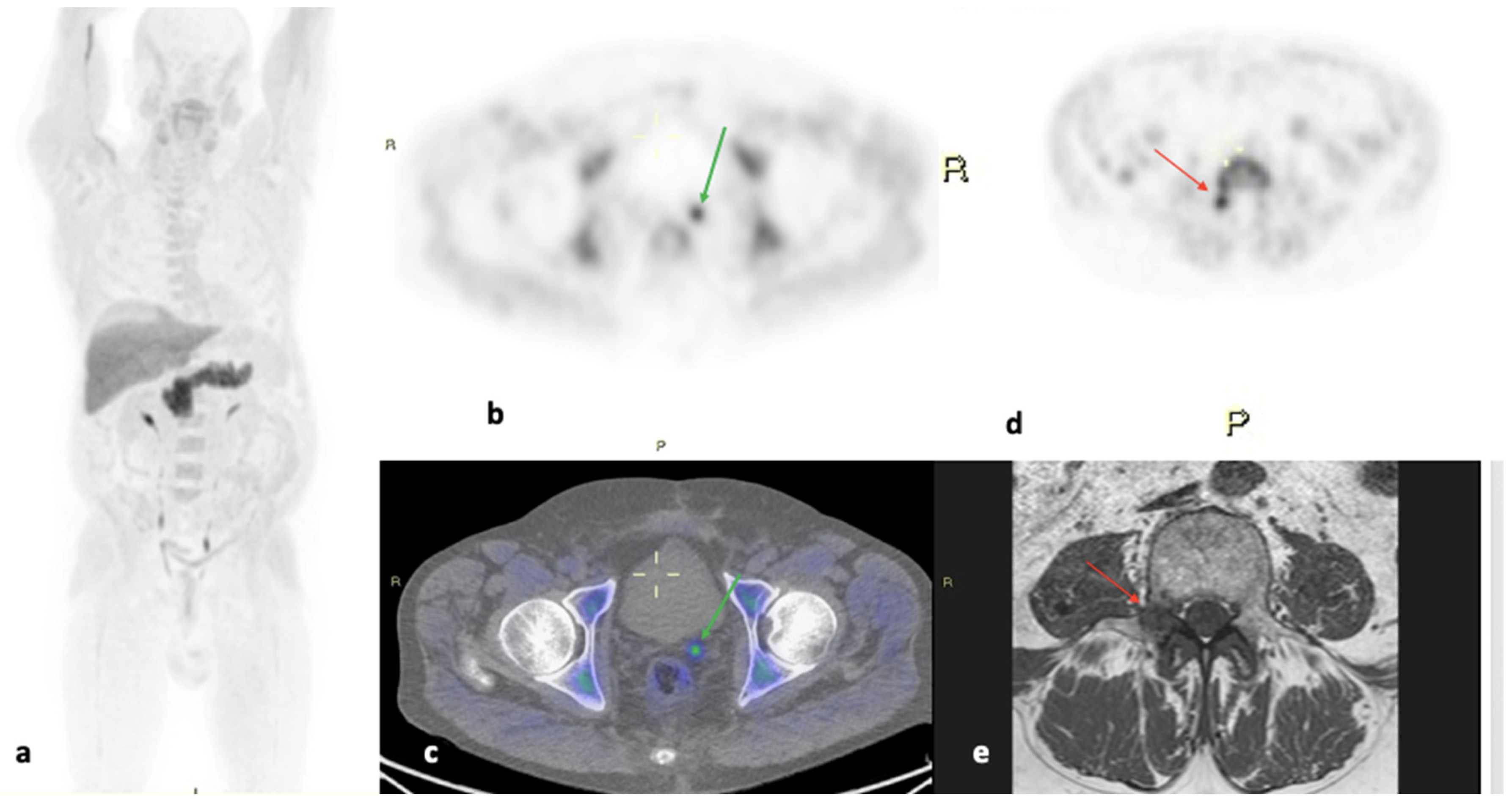
2.3. Image Interpretation
2.4. Extraction and Selection of Radiomic Features
2.5. Statistical Analysis
3. Results
- Model I: IntensityHistogramSkewness and INTENSITY.HISTOGRAM_MinimumHistogramGradientGreyLevel.SUVbw.IBSI.RHQZ.
- Model II: IntensityHistogramSkewness and GLSZM_SmallZoneEmphasis.IBSI.5QRC.
- Model III: IntensityHistogramSkewness and GLSZM_SmallZoneHighGreyLevelEmphasis.IBSI.HW1V.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Choi, H.; Paeng, J.C.; Cheon, G.J. Radiomics in oncological PET/CT: A methodological overview. Nucl. Med. Mol. Imaging 2019, 53, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.J.R.; Azad, G.; Owczarczyk, K.; Siddique, M.; Goh, V. Challenges and Promises of PET Radiomics. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- van Timmeren, J.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—“How-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef] [PubMed]
- Sanduleanu, S.; Woodruff, H.C.; De Jong, E.E.; Van Timmeren, J.E.; Jochems, A.; Dubois, L.; Lambin, P. Tracking tumor biology with radiomics: A systematic review utilizing a radiomics quality score. Radiother. Oncol. 2018, 127, 349–360. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Cavinato, L.; Pegoraro, M.; Ragni, A.; Sollini, M.; Erba, P.A.; Ieva, F. Imaging-based representation and stratification of intra-tumor heterogeneity via tree-edit distance. Sci. Rep. 2022, 12, 19607. [Google Scholar] [CrossRef]
- Chowdhury, R.; Ganeshan, B.; Irshad, S.; Lawler, K.; Eisenblatter, M.; Milewicz, H.; Rodrigues-Justo, M.; Miles, K.; Ellis, P.; Groves, A.; et al. The use of molecular imaging combined with genomic techniques to understand the heterogeneity in cancer metastasis. Br. J. Radiol. 2014, 87, 20140065. [Google Scholar] [CrossRef] [PubMed]
- Cookson, M.S.; Aus, G.; Burnett, A.L.; Canby-Hagino, E.D.; D’Amico, A.V.; Dmochowski, R.R.; Eton, D.T.; Forman, J.D.; Goldenberg, S.L.; Hernandez, J.; et al. Variation in the definition of biochemical recurrence in patients treated for localized prostate cancer: The American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel report and recommendations for a standard in the reporting of surgical outcomes. J. Urol. 2007, 177, 540–545. [Google Scholar]
- Roach, M., 3rd; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Artibani, W.; Porcaro, A.B.; De Marco, V.; Cerruto, M.A.; Siracusano, S. Management of Biochemical Recurrence after Primary Curative Treatment for Prostate Cancer: A Review. Urol. Int. 2018, 100, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Siegel, B.A.; Teoh, E.J.; Andriole, G.L.; LOCATE Study Group. Prostate cancer recurrence in patients with negative or equivocal conventional imaging: A role for 18F-fluciclovine-PET/CT in delineating sites of recurrence and identifying patients with oligometastatic disease. Urol. Oncol. 2021, 39, 365.e9–365.e16. [Google Scholar] [CrossRef] [PubMed]
- Gusman, M.; Aminsharifi, J.A.; Peacock, J.G.; Anderson, S.B.; Clemenshaw, M.N.; Banks, K.P. Review of 18F-Fluciclovine PET for Detection of Recurrent Prostate Cancer. Radiographics 2019, 39, 822–841. [Google Scholar] [CrossRef] [PubMed]
- Sun, A.; Liu, X.; Tang, G. Carbon-11 and fluorine-18 labeled amino acid tracers for positron emission tomography imaging of tumors. Front. Chem. 2018, 5, 124. [Google Scholar] [CrossRef]
- Nanni, C.; Zanoni, L.; Bach-Gansmo, T.; Minn, H.; Willoch, F.; Bogsrud, T.V.; Edward, E.P.; Savir-Baruch, B.; Teoh, E.; Ingram, F.; et al. [18F]Fluciclovine PET/CT: Joint EANM and SNMMI procedure guideline for prostate cancer imaging-version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Autorino, R.; Gui, B.; Panza, G.; Boldrini, L.; Cusumano, D.; Russo, L.; Nardangeli, A.; Persiani, S.; Campitelli, M.; Ferrandina, G.; et al. Radiomics-based prediction of two-year clinical outcome in locally advanced cervical cancer patients undergoing neoadjuvant chemoradiotherapy. Radiol. Med. 2022, 127, 498–506. [Google Scholar] [CrossRef]
- Limkin, E.J.; Sun, R.; Dercle, L.; Zacharaki, E.I.; Robert, C.; Reuzé, S.; Schernberg, A.; Paragios, N.; Deutsch, E.; Ferté, C. Promises and challenges for the implementation of computational medical imaging (radiomics) in oncology. Ann. Oncol. 2017, 28, 1191–1206. [Google Scholar] [CrossRef] [PubMed]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and Reproducibility of Radiomic Features: A Systematic Review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1143–1158. [Google Scholar] [CrossRef] [PubMed]
- Paller, C.J.; Olatoye, D.; Xie, S.; Zhou, X.; Denmeade, S.R.; Eisenberger, M.A.; Antonarakis, E.S.; Carducci, M.A.; Rosner, G.L. The effect of the frequency and duration of PSA measurement on PSA doubling time calculations in men with biochemically recurrent prostate cancer. Prostate Cancer Prostatic Dis. 2014, 17, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Brewster, S.F. PSA Velocity and Doubling Time in Diagnosis and Prognosis of Prostate Cancer. Br. J. Med. Surg. Urol. 2012, 5, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Kim, E.E.; Shokouhi, S.; Tokita, K.; Shin, H.W. Texture Analysis of F-18 Fluciclovine PET/CT to Predict Biochemically Recurrent Prostate Cancer: Initial Results. Tomography 2020, 6, 301–307. [Google Scholar] [CrossRef]
- Lee, J.J.; Yang, H.; Franc, B.L.; Iagaru, A.; Davidzon, G.A. Deep learning detection of prostate cancer recurrence with 18F-FACBC (fluciclovine, Axumin®) positron emission tomography. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2992–2997. [Google Scholar] [CrossRef] [PubMed]
- Alongi, P.; Stefano, A.; Comelli, A.; Laudicella, R.; Scalisi, S.; Arnone, G.; Barone, S.; Spada, M.; Purpura, P.; Bartolotta, T.V.; et al. Radiomics analysis of 18F-Choline PET/CT in the prediction of disease outcome in high-risk prostate cancer: An explorative study on machine learning feature classification in 94 patients. Eur. Radiol. 2021, 31, 4595–4605. [Google Scholar] [CrossRef] [PubMed]
- Malaspina, S.; Ettala, O.; Tolvanen, T.; Rajander, J.; Eskola, O.; Boström, P.J.; Kemppainen, J. Flare on [18F]PSMA-1007 PET/CT after short-term androgen deprivation therapy and its correlation to FDG uptake: Possible marker of tumor aggressiveness in treatment-naïve metastatic prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://uroweb.org/guidelines/prostate-cancer (accessed on 30 August 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Diagnosis (yo, Mean ± SD) | 66 ± 7 | ||
|---|---|---|---|
| Gleason Score | No. Patients | % | |
| nd | 1 | 3 | |
| 3 + 2 | 2 | 6 | |
| 3 + 3 | 6 | 19 | |
| 3 + 4 | 12 | 39 | |
| 3 + 5 | 1 | 3 | |
| 4 + 3 | 5 | 16 | |
| 4 + 4 | 2 | 6 | |
| 4 + 5 | 1 | 3 | |
| 5 + 3 | 1 | 3 | |
| PSA at diagnosis (mean ± SD) 14.25 ± 14.9 ng/mL | |||
| <4 ng/mL | 2 | 6 | |
| 4 ÷ 10 ng/mL | 15 | 48 | |
| >10 ng/mL | 13 | 42 | |
| PSA at fluciclovine PET/CT | |||
| <1 ng/mL | 12 | 39 | |
| 1 ÷ 2 ng/mL | 9 | 29 | |
| >2 ng/mL | 9 | 29 | |
| Time to relapse (years) | |||
| <1 year | 4 | 13 | |
| 1 ÷ 3 years | 7 | 23 | |
| 3 ÷ 5 years | 2 | 6 | |
| 5 ÷ 10 years | 8 | 26 | |
| >10 years | 10 | 32 | |
| Radiomic Features | Mean | SD |
|---|---|---|
| MORCOMP1 | 0.045 | 0.017 |
| IH_KURTOSIS | 1.52 | 1.90 |
| IH_IntensityHistogramSkewness. SUVbw | 0.82 | 0.69 |
| GLCMDIVa | 2.67 | 3.04 |
| NGTDMCom | 118.35 | 156.29 |
| NGTDMStr | 3.40 | 3.61 |
| GLSZMSlZE | 0.35 | 0.13 |
| GLSLGLZE | 0.04 | 0.04 |
| GLSSZHLE | 44.34 | 45.74 |
| GLSLHGLE | 95,043.98 | 133,545.82 |
| GLSGLNU | 3.71 | 2.99 |
| GLSZSNU | 10.49 | 13.80 |
| GLSNZSNU | 0.18 | 0.07 |
| GLSZMZP | 0.10 | 0.18 |
| Sensitivity | Specificity | Threshold | J_Index | AUC | Low_AUC | High_AUC | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Training | Validation | Training | Validation | Training | Validation | Training | Validation | Training | Validation | Training | Validation | Training | Validation | |
| Model I | 100 | 60 | 50 | 100 | 0.36 | 0.62 | 0.5 | 0.6 | 80.21 | 70 | 0.6 | 0.29 | 1 | 1 |
| Model II | 66.67 | 80 | 87,5 | 10 | 0.69 | 0.79 | 0.54 | 0.8 | 82.29 | 95 | 0.63 | 0.81 | 1 | 1 |
| Model III | 91.67 | 80 | 75 | 100 | 0.36 | 0.95 | 0.67 | 0.8 | 81.25 | 90 | 0.6 | 0.68 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Travascio, L.; De Novellis, S.; Turano, P.; Di Nicola, A.D.; Di Egidio, V.; Calabria, F.; Frontino, L.; Frantellizzi, V.; De Vincentis, G.; Cimini, A.; et al. Texture Analysis in [18F]-Fluciclovine PET/CT Aids to Detect Prostate Cancer Biochemical Relapse: Report of a Preliminary Experience. Appl. Sci. 2024, 14, 3469. https://doi.org/10.3390/app14083469
Travascio L, De Novellis S, Turano P, Di Nicola AD, Di Egidio V, Calabria F, Frontino L, Frantellizzi V, De Vincentis G, Cimini A, et al. Texture Analysis in [18F]-Fluciclovine PET/CT Aids to Detect Prostate Cancer Biochemical Relapse: Report of a Preliminary Experience. Applied Sciences. 2024; 14(8):3469. https://doi.org/10.3390/app14083469
Chicago/Turabian StyleTravascio, Laura, Sara De Novellis, Piera Turano, Angelo Domenico Di Nicola, Vincenzo Di Egidio, Ferdinando Calabria, Luca Frontino, Viviana Frantellizzi, Giuseppe De Vincentis, Andrea Cimini, and et al. 2024. "Texture Analysis in [18F]-Fluciclovine PET/CT Aids to Detect Prostate Cancer Biochemical Relapse: Report of a Preliminary Experience" Applied Sciences 14, no. 8: 3469. https://doi.org/10.3390/app14083469
APA StyleTravascio, L., De Novellis, S., Turano, P., Di Nicola, A. D., Di Egidio, V., Calabria, F., Frontino, L., Frantellizzi, V., De Vincentis, G., Cimini, A., & Ricci, M. (2024). Texture Analysis in [18F]-Fluciclovine PET/CT Aids to Detect Prostate Cancer Biochemical Relapse: Report of a Preliminary Experience. Applied Sciences, 14(8), 3469. https://doi.org/10.3390/app14083469