

Fully Digitalized Workflow of Flipper Fabrication: Different Three-Dimensional Printing Strategies and Characteristics


Abstract
1. Introduction
2. Case Description
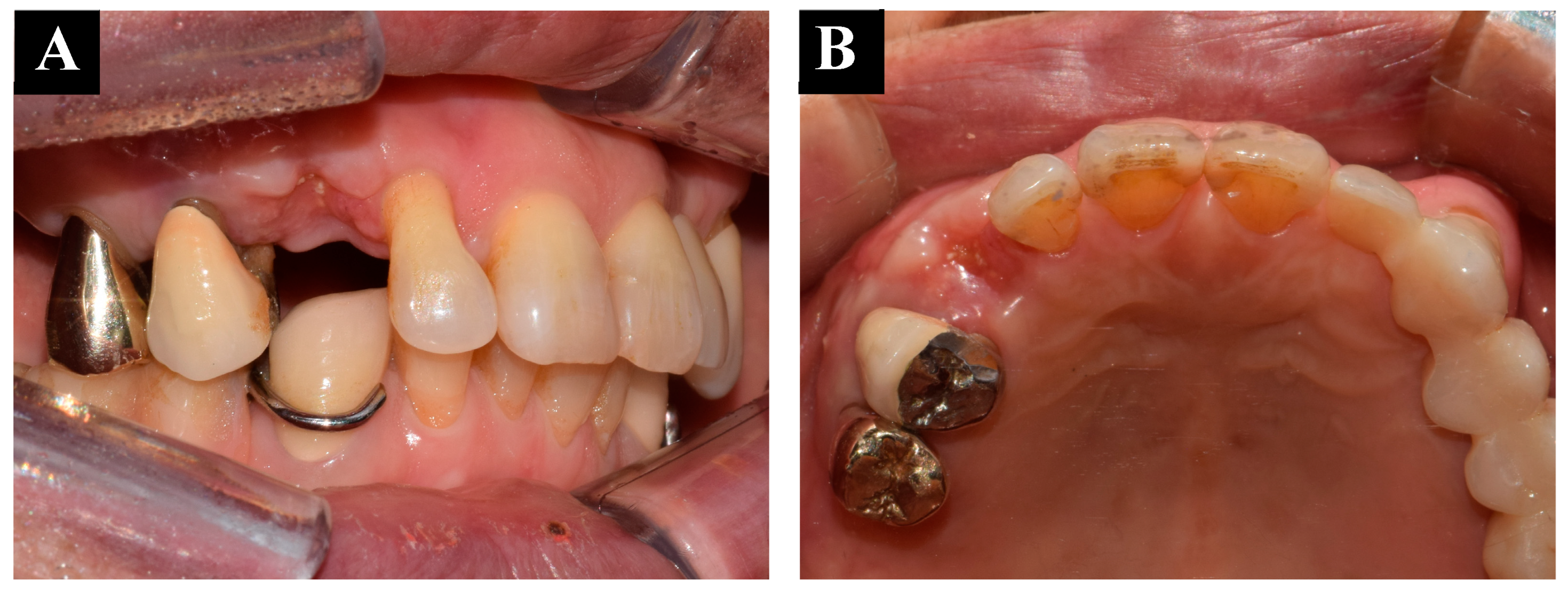
2.1. History and Clinical Examination
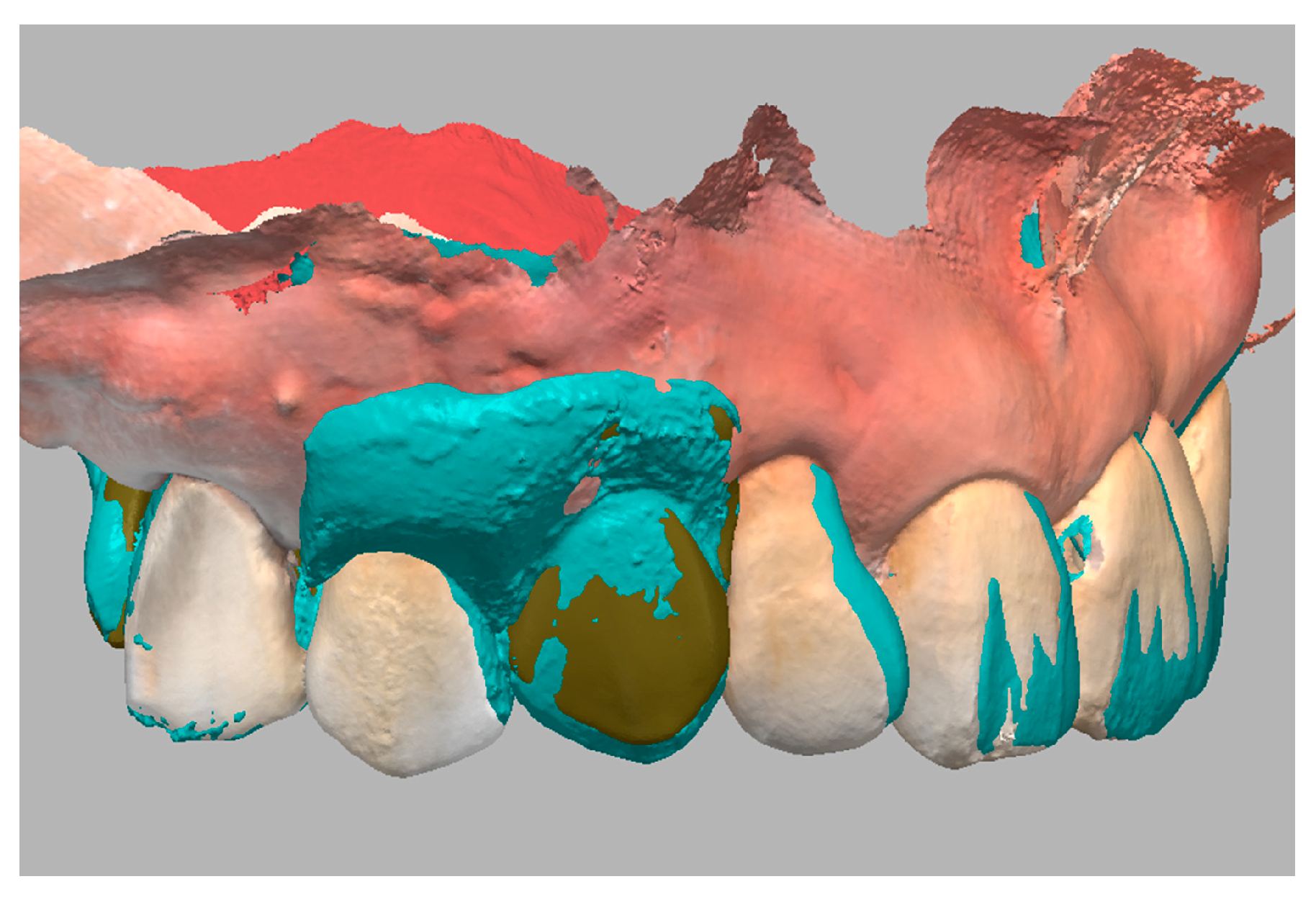
2.2. Treatment Planning
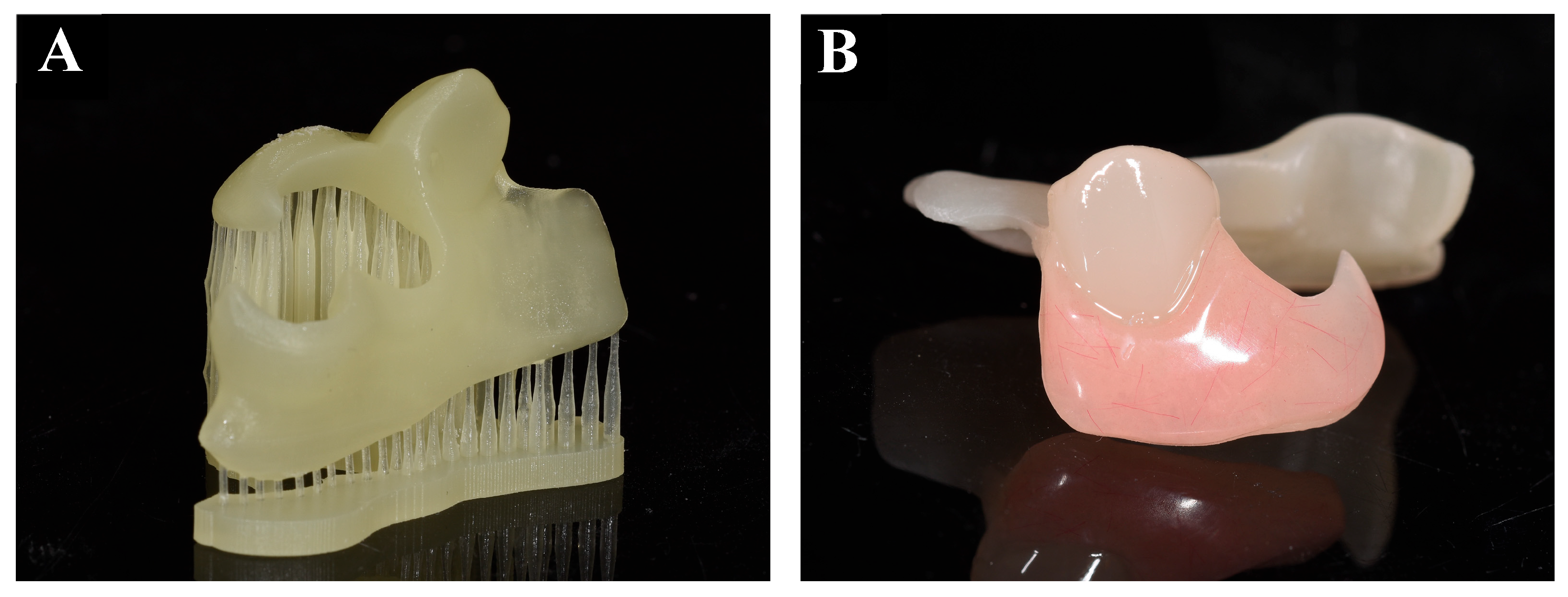
2.3. Fabrication of Flippers
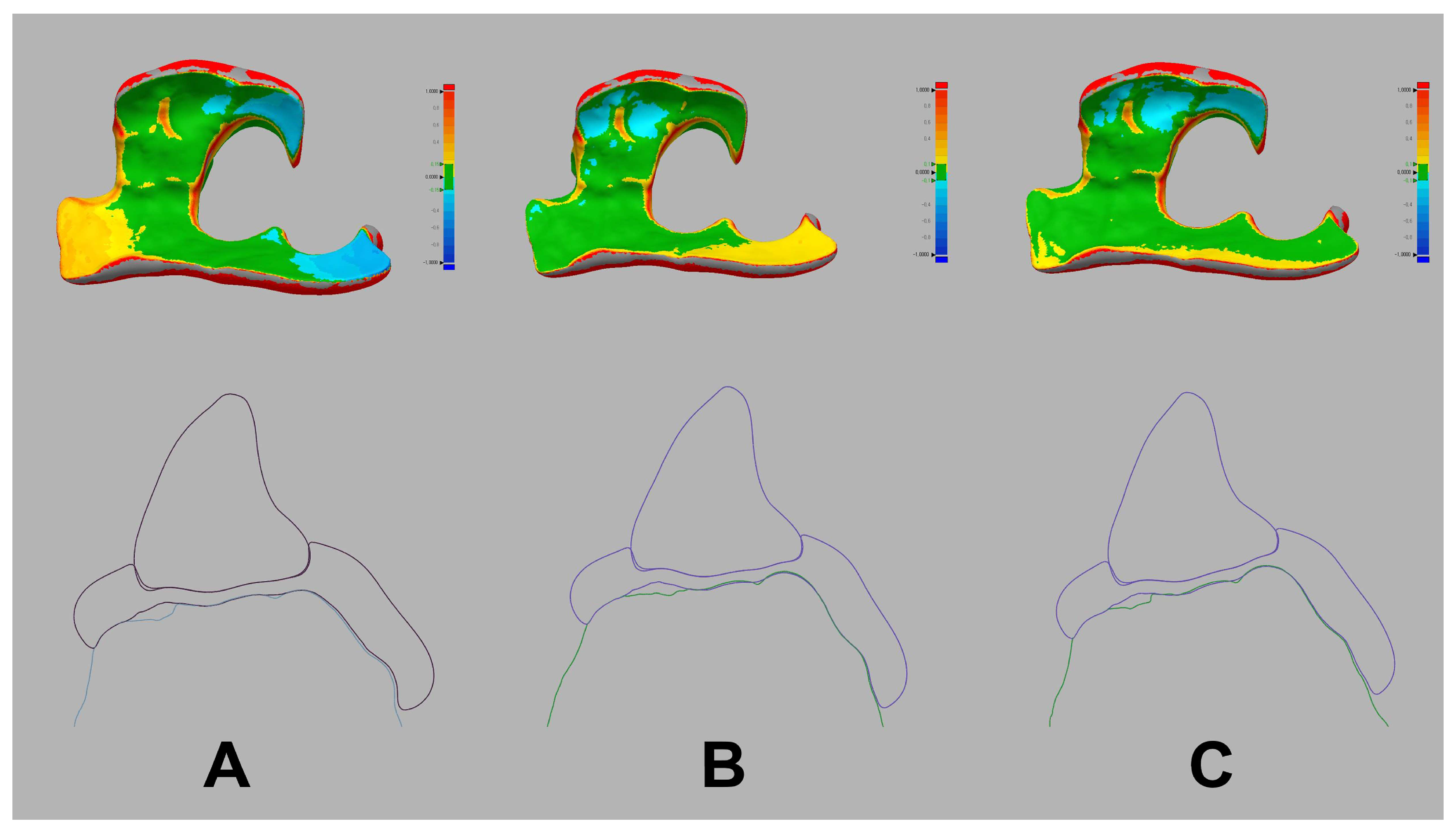
2.4. Fit Accuracy Analysis of the Flippers
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, K.; Aeran, H.; Kumar, N.; Gupta, N. Flexible thermoplastic denture base materials for aesthetical removable partial denture framework. J. Clin. Diagn. Res. 2013, 7, 2372–2373. [Google Scholar] [CrossRef]
- Pellizzer, E.P.; Mazaro, J.V.; Verri, F.R.; Antenucci, R.M.; Goiato, M.C. Removable partial denture in combination with a milled fixed partial prosthesis as interim restorations in long-term treatment. J. Prosthodont. 2010, 19, 77–80. [Google Scholar] [CrossRef]
- Zhang, H.; Lee, R.; Chung, K.H. A technique to fabricate a customized interim removable partial denture. J. Prosthet. Dent. 2009, 102, 187–190. [Google Scholar] [CrossRef]
- Polyzois, G.; Lagouvardos, P.; Kranjcic, J.; Vojvodic, D. Flexible Removable Partial Denture Prosthesis: A Survey of Dentists’ Attitudes and Knowledge in Greece and Croatia. Acta Stomatol. Croat. 2015, 49, 316–324. [Google Scholar] [CrossRef]
- Winkler, S.; Wood, R.; Boberick, K.G.; Perizzolo, D.; Knowles, T.; Heideman, G.; Graham, L. An interim denture technique and case reports. J. Oral Implantol. 2005, 31, 129–133. [Google Scholar] [CrossRef]
- Hill, E.E.; Rubel, B.; Smith, J.B. Flexible removable partial dentures: A basic overview. Gen. Dent. 2014, 62, 32–36. [Google Scholar]
- Mubaraki, M.Q.; Moaleem, M.M.A.; Alzahrani, A.H.; Shariff, M.; Alqahtani, S.M.; Porwal, A.; Al-Sanabani, F.A.; Bhandi, S.; Tribst, J.P.M.; Heboyan, A.; et al. Assessment of conventionally and digitally fabricated complete dentures: A comprehensive review. Materials 2022, 15, 3868. [Google Scholar] [CrossRef]
- Dusmukhamedov, S.; Lee, C.N.; Jeong, S.M.; Choi, B.H. Digital denture fabrication: A technical note. Appl. Sci. 2021, 11, 8093. [Google Scholar] [CrossRef]
- Lin, W.S.; Harris, B.T.; Pellerito, J.; Morton, D. Fabrication of an interim complete removable dental prosthesis with an in-office digital light processing three-dimensional printer: A proof-of-concept technique. J. Prosthet. Dent. 2018, 120, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Piao, X.; Park, J.M.; Kim, D.H.; Shim, J.S. Application of additive and subtractive manufacturing technology for a digitally fabricated removable partial denture after a partial maxillectomy: A clinical report. J. Prosthet. Dent. 2022, 127, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Jurado, C.A.; Tsujimoto, A.; Alhotan, A.; Villalobos-Tinoco, J.; AlShabib, A. Digitally Fabricated Immediate Complete Dentures: Case Reports of Milled and Printed Dentures. Int. J. Prosthodont. 2020, 33, 232–241. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Karasan, D.; Legaz, J.; Boitelle, P.; Mojon, P.; Fehmer, V.; Sailer, I. Accuracy of Additively Manufactured and Milled Interim 3-Unit Fixed Dental Prostheses. J. Prosthodont. 2022, 31, 58–69. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2016, 32, 54–64. [Google Scholar] [CrossRef]
- Li, R.; Chen, H.; Wang, Y.; Sun, Y. Suitability of the triple-scan method with a dental laboratory scanner to assess the 3D adaptation of zirconia crowns. J. Prosthet. Dent. 2021, 125, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.Y.; Lee, W.K.; Kwon, T.G.; Lee, D.H. Reliability of digital measurement methods on the marginal fit of fixed prostheses: A systematic review and meta-analysis of in vitro studies. J. Prosthet. Dent. 2020, 124, 350.e1–350.e11. [Google Scholar] [CrossRef]
- Dib Zakkour, S.; Dib Zakkour, J.; Guadilla, Y.; Montero, J.; Dib, A. Comparative Evaluation of the Digital Workflow and Conventional Method in Manufacturing Complete Removal Prostheses. Materials 2023, 16, 6955. [Google Scholar] [CrossRef] [PubMed]
- Bernauer, S.A.; Zitzmann, N.U.; Joda, T. The Complete Digital Workflow in Fixed Prosthodontics Updated: A Systematic Review. Healthcare 2023, 11, 679. [Google Scholar] [CrossRef]
- Virard, F.; Venet, L.; Richert, R.; Pfeffer, D.; Viguié, G.; Bienfait, A.; Farges, J.C.; Ducret, M. Manufacturing of an immediate removable partial denture with an intraoral scanner and CAD-CAM technology: A case report. BMC Oral Health 2018, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, G.; Edwards, S.P.; Mayers, C.A.; Meneghetti, P.C.; Liu, F. Digital Immediate Complete Denture for a Patient with Rhabdomyosarcoma: A Clinical Report. J. Prosthodont. 2021, 30, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; An, Y.X.; Shi, Y.L.; Liu, L.P.; Zhao, Y.Q.; Wu, F.; Wei, H.B. A digital workflow to predict facial aesthetics in patients with maxillofacial trauma with implant retained prostheses. J. Prosthodont. Res. 2023, 67, 481–486. [Google Scholar] [CrossRef]
- Li, Y.; Yu, Y.; Feng, Y.; Liu, W. Predictable digital restorative workflow for minimally invasive esthetic rehabilitation utilizing a virtual patient model with global diagnosis principle. J. Esthet. Restor. Dent. 2022, 34, 769–775. [Google Scholar] [CrossRef]
- Choi, J.J.E.; Uy, C.E.; Plaksina, P.; Ramani, R.S.; Ganjigatti, R.; Waddell, J.N. Bond Strength of Denture Teeth to Heat-Cured, CAD/CAM and 3D Printed Denture Acrylics. J. Prosthodont. 2020, 29, 415–421. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Tera Harz TC-80DP | Tera Harz Flexible Denture—TFDH | Tera Harz II BR-23 |
|---|---|---|---|
| Density (g/cm3) | 1.076 ± 0.02 | 0.998 ± 0.02 | 1.015 ± 0.02 |
| Viscosity (cps) | 2000 ± 300 | 200 ± 50 | 1300 ± 300 |
| Shore hardness (D) | 90–110 | 80–100 | 85–105 |
| Flexural strength (Mpa) | 160–180 | 110–130 | 100–130 |
| Flexural modulus (Mpa) | 4500–5500 | 2800–3000 | 2500–2700 |
| Composition (weight %) | 2-Hydroxyethyl methacrylate 30-70 1,4-Butanediol polymer with α-hydro-ω-hydroxypoly(oxy-1,4-butanediyl) and 1,1′methylenebis[4-isocyanatobenzene] 20-60 α,α`-[(1-Methylethylidene)di-4,1-phenylene]bis[ω-[(2-methyl-1-oxo-2-propenyl)oxy]poly(oxy-1,2-ethanediyl) 1-20 Phenylbis(2,4,6-trimethylbenzoyl)phosphine oxide 0-10, 2,6-di-tert-butyl-p-cresol 0-1 Titanium dioxide 0-1 C.I. pigment yellow 180 0-1 Pyrrolo[3,4-c]pyrrole-1,4-dione, 3,6-bis(4-chlorophenyl)-2,5-dihydro-(C.I. pigment red 254) 0-1 | 1,3-Butadiene homopolymer 45-55 2-Propenoic acid, (5-ethyl-1,3-dioxan-5-yl)methyl ester 15-20 exo-1,7,7-Trimethylbicyclo[2.2.1]hept-2-ylacrylate 10-20 7,7,9(or 7,9,9)-Trimethyl-4,13-dioxo 3,14-dioxa-5,12-diazahexadecane-1,16-diyl 2-methyl-2-propenoate 5-15 Phenylbis(2,4,6-trimethyl benzoyl)phosphine oxide 0-10 Titanium dioxide 0-1 Pyrrolo[3,4-c]pyrrole-1,4-dione, 3,6-bis(4-chlorophenyl)-2,5-dihydro- (C.I. pigment red 254) 0-1 Zirconium dioxide 0-1 C.I. pigment yellow 180 0-1 C.I. solvent black 027 0-1 | 1,3-Butadiene homopolymer 50.19 2-Propenoic acid, (5-ethyl-1,3-dioxan-5-yl)methyl ester 19.63 exo-1,7,7-Trimethylbicyclo[2.2.1]hept-2-ylacrylate 16.31 7,7,9(or 7,9,9)-Trimethyl-4,13-dioxo 3,14-dioxa-5,12-diazahexadecane-1,16-diyl 2-methyl-2-propenoate 12.55 Phenylbis(2,4,6-trimethylbenzoyl)phosphine oxide 1.32 Titanium dioxide 0-5 Zirconium dioxide 0-5 C.I. pigment yellow 180 0-5 Pyrrolo[3,4-c]pyrrole-1,4-dione, 3,6-bis(4-chlorophenyl)-2,5-dihydro- (C.I. pigment red 254) 0-5 C.I. solvent black 027 0-5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, S.; Lee, D.-H. Fully Digitalized Workflow of Flipper Fabrication: Different Three-Dimensional Printing Strategies and Characteristics. Appl. Sci. 2024, 14, 2838. https://doi.org/10.3390/app14072838
Rana S, Lee D-H. Fully Digitalized Workflow of Flipper Fabrication: Different Three-Dimensional Printing Strategies and Characteristics. Applied Sciences. 2024; 14(7):2838. https://doi.org/10.3390/app14072838
Chicago/Turabian StyleRana, Shilpa, and Du-Hyeong Lee. 2024. "Fully Digitalized Workflow of Flipper Fabrication: Different Three-Dimensional Printing Strategies and Characteristics" Applied Sciences 14, no. 7: 2838. https://doi.org/10.3390/app14072838
APA StyleRana, S., & Lee, D.-H. (2024). Fully Digitalized Workflow of Flipper Fabrication: Different Three-Dimensional Printing Strategies and Characteristics. Applied Sciences, 14(7), 2838. https://doi.org/10.3390/app14072838