
Waferless Orthognathic Surgery with Customized Osteosynthesis and Surgical Guides: A Prospective Study

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
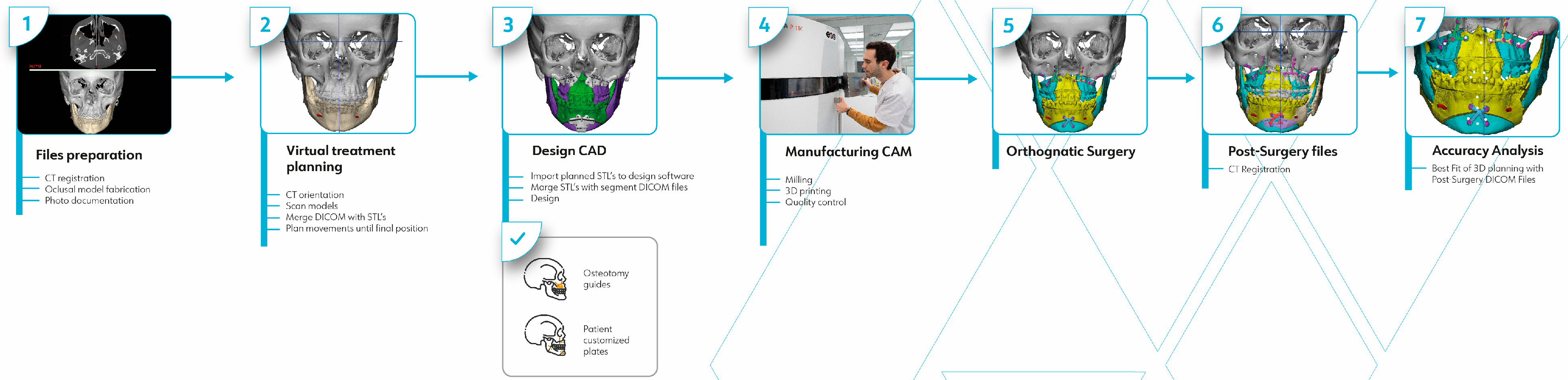
2.1. Patient Orthognathic Planning Protocol
2.2. Two-Dimensional Virtual Surgical Planning
2.3. Three-Dimensional Virtual Surgical Planning
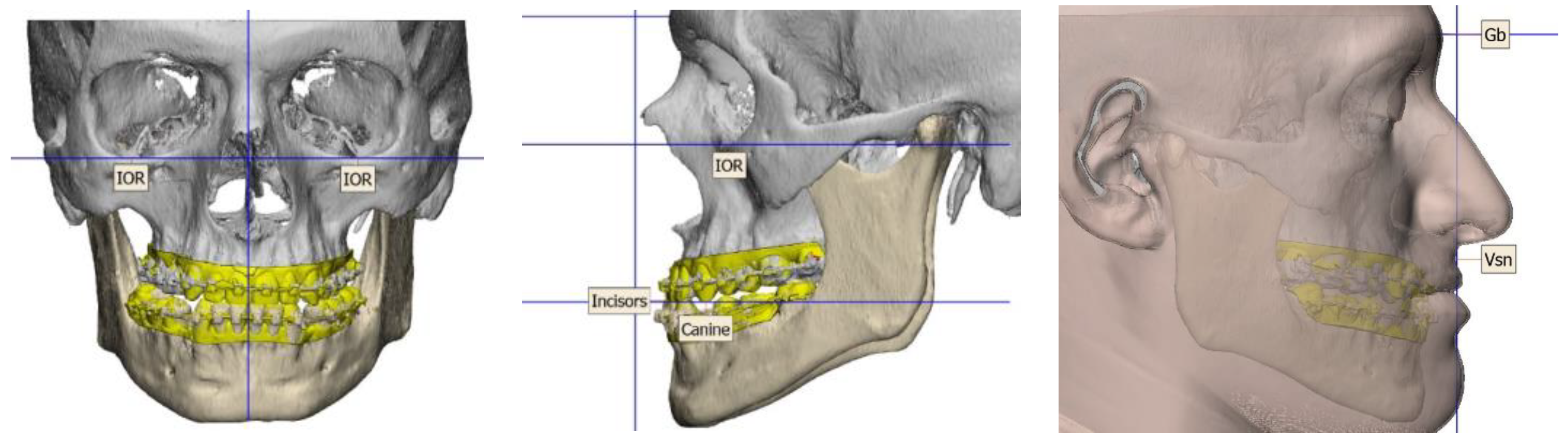
2.4. Data Sampling
- -
- Occlusal: tips of the mesiobuccal cuspids of the first molars, tips of the upper canines, upper incisor point, and lower incisor point.
- -
- Skeletal: A point, B point, and pogonion point.
- -
- Titanium plates: anterior and posterior upper plates, inferior chin plate, and midpoint chin plate.
2.5. Statistical Analysis
3. Results
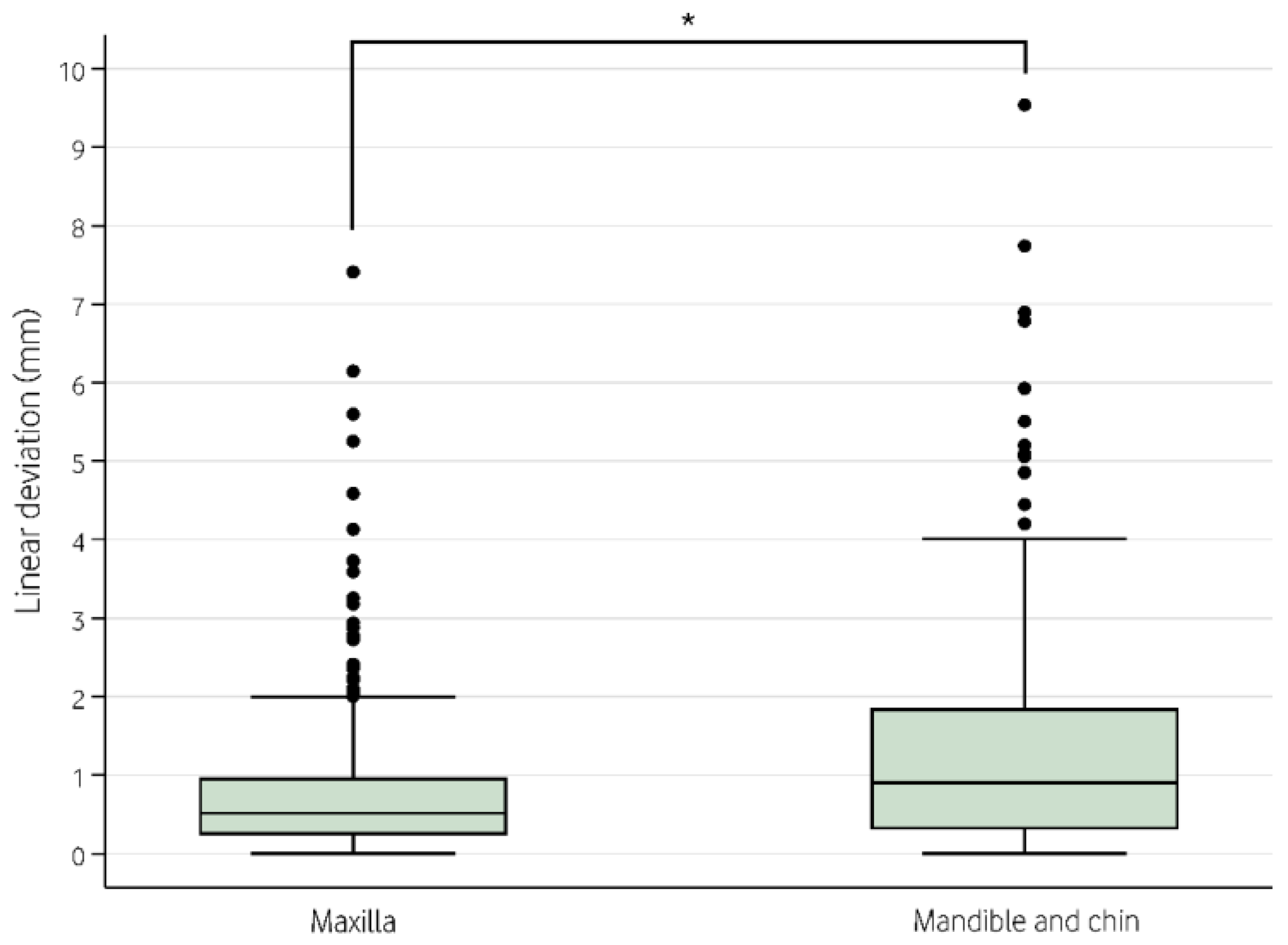
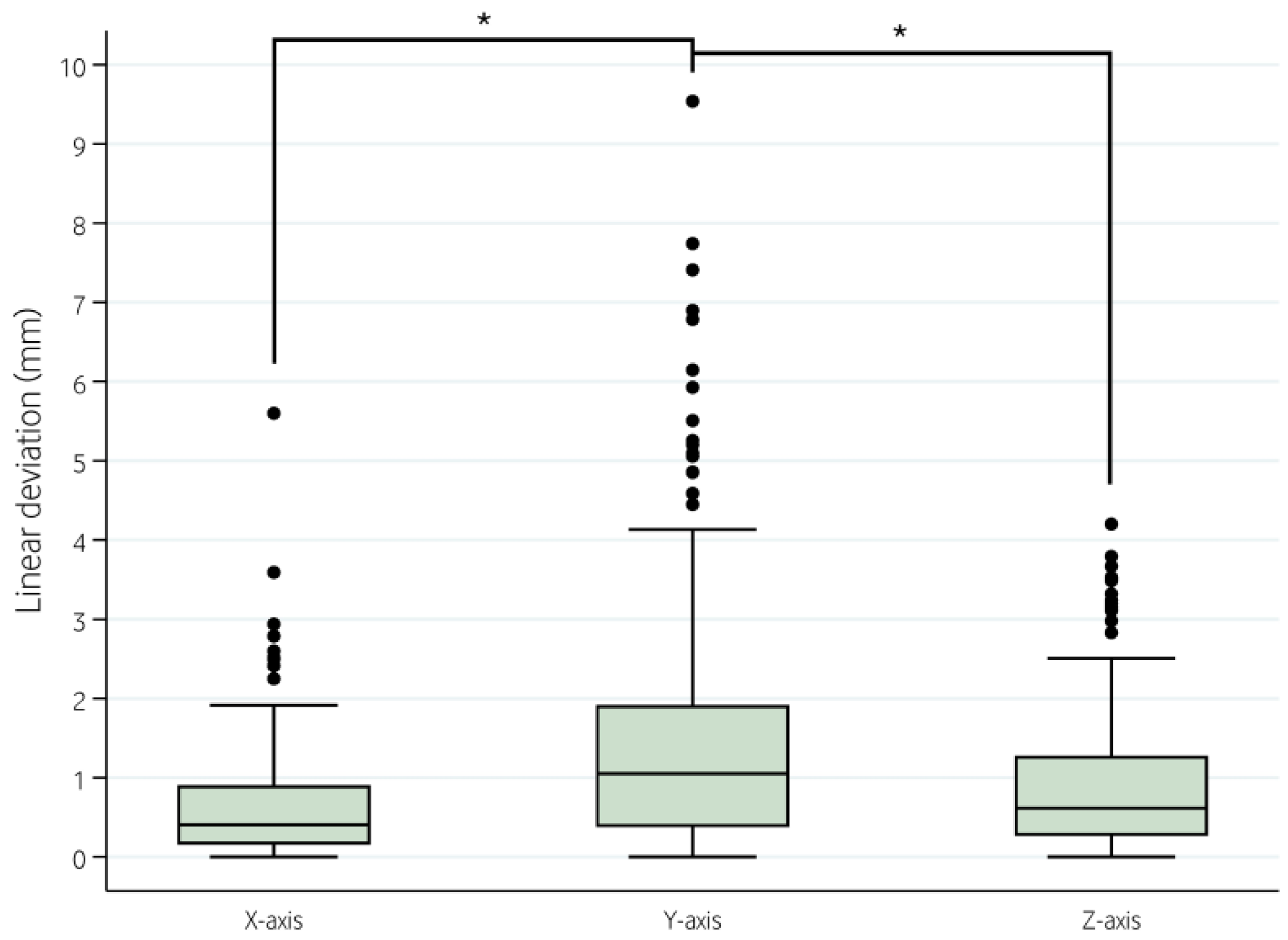
3.1. Absolute Values
3.2. Signed Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swennen, G.R.J.; Mollemans, W.; Schutyser, F. Three-dimensional treatment planning of orthognathic surgery in the era of virtual imaging. J. Oral Maxillofac. Surg. 2009, 67, 2080–2092. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Shang, H.; Liu, Y.; Zhao, J.; Zhao, Y. Computer-aided design and computer-aided manufacturing locating guides accompanied with prebent titanium plates in orthognathic surgery. J. Oral Maxillofac. Surg. 2012, 70, 2419–2426. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Kim, S.G. Redefining precision and efficiency in orthognathic surgery through virtual surgical planning and 3D printing: A narrative review. Maxillofac. Plast. Reconstr. Surg. 2023, 45, 42. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Luebbers, H.T.; Agbaje, J.O.; Schepers, S.; Vrielinck, L.; Lambrichts, I.; Politis, C. Accuracy of upper jaw positioning with intermediate splint fabrication after virtual planning in bimaxillary orthognathic surgery. J. Craniofac. Surg. 2013, 24, 1871–1876. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Baek, S.H. Comparison of the accuracy of the three-dimensional virtual method and the conventional manual method for model surgery and intermediate wafer fabrication. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.; Goonewardene, M.S.; Mian, A.; Allan, B.; Brock, D.; Trevenen, M. Accuracy of orthognathic surgery using 3D computer-assisted surgical simulation. Aust. Orthod. 2018, 34, 17–26. [Google Scholar] [CrossRef]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F.; Christensen, A.M.; Lasky, R.E.; Lemoine, J.J. Accuracy of the Computer-Aided Surgical Simulation (CASS) System in the Treatment of Patients With Complex Craniomaxillofacial Deformity: A Pilot Study. J. Oral Maxillofac. Surg. 2007, 65, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Metzger, M.C.; Hohlweg-Majert, B.; Schwarz, U.; Teschner, M.; Hammer, B.; Schmelzeisen, R. Manufacturing splints for orthognathic surgery using a three-dimensional printer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, e1–e7. [Google Scholar] [CrossRef]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F. Three-dimensional computer-aided surgical simulation for maxillofacial surgery. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2005, 13, 25–39. [Google Scholar] [CrossRef]
- Tucker, S.; Cevidanes, L.H.S.; Styner, M.; Kim, H.; Reyes, M.; Proffit, W. Comparison of actual surgical outcomes and 3-dimensional surgical simulations. J. Oral Maxillofac. Surg. 2010, 68, 2412–2421. [Google Scholar] [CrossRef]
- Sharifi, A.; Jones, R.; Ayoub, A.; Moos, K.; Walker, F.; Khambay, B. How accurate is model planning for orthognathic surgery? Int. J. Oral Maxillofac. Surg. 2008, 37, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Schouman, T.; Rouch, P.; Imholz, B.; Fasel, J.; Courvoisier, D.; Scolozzi, P. Accuracy evaluation of CAD/CAM generated splints in orthognathic surgery: A cadaveric study. Head Face Med. 2015, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Shen, S.; Jiang, W.; Li, J.; Jiang, T.; Xia, J.J. A new approach of splint-less orthognathic surgery using a personalized orthognathic surgical guide system: A preliminary study. Int. J. Oral Maxillofac. Surg. 2017, 46, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, S.; Bianchi, A.; Schiariti, G.; Badiali, G.; Marchetti, C. Computer-aided design and computer-aided manufacturing cutting guides and customized titanium plates are useful in upper maxilla waferless repositioning. J. Oral Maxillofac. Surg. 2015, 73, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Shakoori, P.; Yang, R.; Nah, H.D.; Scott, M.; Swanson, J.W.; Taylor, J.A. Computer-aided Surgical Planning and Osteosynthesis Plates for Bimaxillary Orthognathic Surgery: A Study of 14 Consecutive Patients. Plast Reconstr. Surg. Glob. Open 2022, 10, e4609. [Google Scholar] [CrossRef] [PubMed]
- Heufelder, M.; Wilde, F.; Pietzka, S.; Mascha, F.; Winter, K.; Schramm, A. Clinical accuracy of waferless maxillary positioning using customized surgical guides and patient specific osteosynthesis in bimaxillary orthognathic surgery. J. Craniomaxillofac. Surg. 2017, 45, 1578–1585. [Google Scholar] [CrossRef]
- Wong, A.; Goonewardene, M.S.; Allan, B.P.; Mian, A.S.; Rea, A. Accuracy of maxillary repositioning surgery using CAD/CAM customized surgical guides and fixation plates. Int. J. Oral Maxillofac. Surg. 2021, 50, 494–500. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, 1628–1655. [Google Scholar] [CrossRef]
- Arnett, G.W.; Jelic, J.S.; Kim, J.; Cummings, D.R.; Beress, A.; Worley, C.M. Soft tissue cephalometric analysis: Diagnosis and treatment planning of dentofacial deformity. Am. J. Orthod. Dentofacial. Orthop. 1999, 116, 239–253. [Google Scholar] [CrossRef]
- Williams, A.; Walker, K.; Hughes, D.; Goodson, A.M.C.; Mustafa, S.F. Accuracy and cost effectiveness of a waferless osteotomy approach, using patient specific guides and plates in orthognathic surgery: A systematic review. Br. J. Oral Maxillofac. Surg. 2022, 60, 537–546. [Google Scholar] [CrossRef]
- Suojanen, J.; Leikola, J.; Stoor, P. The use of patient-specific implants in orthognathic surgery: A series of 32 maxillary osteotomy patients. J. Craniomaxillofac. Surg. 2016, 44, 1913–1916. [Google Scholar] [CrossRef]
- Zinser, M.J.; Sailer, H.F.; Ritter, L.; Braumann, B.; Maegele, M.; Zöller, J.E. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and “classic” intermaxillary splints to surgical transfer of virtual orthognathic planning. J. Oral Maxillofac. Surg. 2013, 71, 2151. [Google Scholar] [CrossRef]
- Karanxha, L.; Rossi, D.; Hamanaka, R.; Giannì, A.B.; Baj, A.; Moon, W. Accuracy of splint vs splintless technique for virtually planned orthognathic surgery: A voxel-based three-dimensional analysis. J. Craniomaxillofac. Surg. 2021, 49, 1–8. [Google Scholar] [CrossRef]
- Sánchez-Jáuregui, E.; Baranda-Manterola, E.; Ranz-Colio, Á.; Bueno de Vicente, Á.; Acero-Sanz, J. Custom made cutting guides and osteosynthesis plates versus CAD/CAM occlusal splints in positioning and fixation of the maxilla in orthognathic surgery: A prospective randomized study. J. Craniomaxillofac. Surg. 2022, 50, 609–614. [Google Scholar] [CrossRef]
- Kraeima, J.; Schepers, R.H.; Spijkervet, F.K.L.; Maal, T.J.J.; Baan, F.; Witjes, M.J.H. Splintless surgery using patient-specific osteosynthesis in Le Fort I osteotomies: A randomized controlled multi-centre trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, C.; Bianchi, A.; Bassi, M.; Gori, R.; Lamberti, C.; Sarti, A. Mathematical modeling and numerical simulation in maxillofacial virtual surgery. J. Craniofac. Surg. 2007, 18, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Ong, T.K.; Banks, R.J.; Hildreth, A.J. Surgical accuracy in Le Fort I maxillary osteotomies. Br. J. Oral Maxillofac. Surg. 2001, 39, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, C.E.; Paranhos, L.R.; da Silva, R.P.; Herval, M.; Blumenberg, C.; Zanetta-Barbosa, D. Accuracy of orthognathic surgery with customized titanium plates—Systematic review. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Brucoli, M.; Baena, R.R.Y.; Boffano, P.; Benech, A. Psychological profiles in patients undergoing orthognathic surgery or rhinoplasty: A preoperative and preliminary comparison. Oral Maxillofac. Surg. 2019, 23, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Brucoli, M.; Zeppegno, P.; Benech, R.; Boffano, P.; Benech, A. Psychodynamic Features Associated With Orthognathic Surgery: A Comparison Between Conventional Orthognathic Treatment and “Surgery-First” Approach. J. Oral Maxillofac. Surg. 2019, 77, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Dutta, A.; Dutta, K.; Mukherjee, K. Biomechanical influence of plate configurations on mandible subcondylar fracture fixation: A finite element study. Med. Biol. Eng. Comput. 2023, 61, 2581–2591. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Gandini, P.; Alcozer, R.; Vallittu, P.K.; Scribante, A. Failure load and stress analysis of orthodontic miniscrews with different transmucosal collar diameter. J. Mech. Behav. Biomed. Mater. 2018, 87, 132–137. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Gender | Age (years) | TOD | TOS | Complications |
|---|---|---|---|---|---|
| 1 | Female | 21.13 | Asymmetry | BS + G | None |
| 2 | Female | 32.12 | Asymmetry | BS + G | None |
| 3 | Female | 46.16 | Class III | MS | None |
| 4 | Female | 22.66 | Class II subdivision 1 | BS | None |
| 5 | Female | 30.65 | Asymmetry | BS + G | None |
| 6 | Female | 38.34 | Asymmetry | BS + G | None |
| 7 | Male | 37.67 | Class II subdivision 2 | B + G | None |
| 8 | Male | 37.13 | Class III | BS + G | None |
| 9 | Male | 39.76 | Class I retrusive | B + G | None |
| 10 | Female | 21.31 | Class II subdivision 1 | BS | None |
| 11 | Male | 28.19 | Asymmetry | BS | None |
| 12 | Female | 24.84 | Class II subdivision 1 | BS + G | None |
| 13 | Female | 29.69 | Class II subdivision 1 | BS + G | None |
| 14 | Female | 38.33 | Class II subdivision 1 | B | Revision surgery |
| 15 | Female | 24.33 | Class II subdivision 2 | BS | None |
| 16 | Male | 40.82 | Asymmetry | BS | None |
| 17 | Male | 29.08 | Class III | MS | None |
| 18 | Female | 31.44 | Asymmetry | BS + G | None |
| 19 | Female | 22.47 | Asymmetry | BS + G | None |
| 20 | Male | 29.90 | Asymmetry | B + G | Revision surgery |
| 21 | Male | 34.39 | Class II subdivision 1 | BS + G | Revision surgery |
| Absolute | Signed | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| X | Y | Z | X | Y | Z | ||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Maxilla | First right molar | 0.63 | 0.55 | 1.14 | 1.25 | 0.77 | 0.61 | −0.13 | 0.83 | 0.69 | 1.56 | 0.11 | 0.99 |
| First left molar | 0.63 | 0.65 | 0.73 | 0.49 | 0.66 | 0.52 | 0.22 | 0.89 | 0.19 | 0.87 | −0.05 | 0.85 | |
| Right canine | 1.34 | 1.35 | 1.22 | 1.37 | 0.47 | 0.35 | −0.07 | 1.92 | −0.49 | 1.78 | 0.11 | 0.58 | |
| Left canine | 0.66 | 0.48 | 1.22 | 1.73 | 0.59 | 0.37 | 0.28 | 0.78 | −0.34 | 2.11 | −0.03 | 0.71 | |
| Right central incisor (upper) | 0.60 | 0.46 | 0.92 | 0.88 | 0.60 | 0.46 | −0.09 | 0.76 | 0.00 | 1.29 | −0.20 | 0.74 | |
| Left central incisor (upper) | 0.50 | 0.41 | 1.04 | 0.95 | 0.70 | 0.42 | 0.08 | 0.65 | −0.04 | 1.43 | −0.22 | 0.80 | |
| A | 0.58 | 0.76 | 0.94 | 0.84 | 0.58 | 0.74 | 0.12 | 0.95 | 0.91 | 0.87 | −0.51 | 0.79 | |
| Anterior right miniplate | 0.40 | 0.36 | 0.66 | 0.47 | 0.56 | 0.49 | −0.21 | 0.51 | 0.18 | 0.80 | 0.31 | 0.68 | |
| Anterior left miniplate | 0.47 | 0.39 | 0.86 | 0.58 | 0.68 | 0.51 | −0.19 | 0.58 | −0.29 | 1.01 | −0.17 | 0.85 | |
| Posterior right miniplate | 0.42 | 0.22 | 0.78 | 0.66 | 0.64 | 0.44 | 0.05 | 0.48 | −0.54 | 0.87 | −0.02 | 0.78 | |
| Posterior left miniplate | 0.46 | 0.35 | 0.79 | 0.60 | 0.71 | 0.52 | 0.09 | 0.58 | −0.36 | 0.94 | 0.40 | 0.80 | |
| Mandible | Right central incisor (lower) | 0.88 | 0.70 | 1.32 | 1.03 | 1.17 | 0.96 | −0.13 | 1.14 | 0.05 | 1.70 | −0.42 | 1.48 |
| Left central incisor (lower) | 0.75 | 0.80 | 1.28 | 1.12 | 1.15 | 0.92 | −0.01 | 1.11 | −0.04 | 1.72 | −0.43 | 1.44 | |
| Pogonion | 0.97 | 0.81 | 2.13 | 2.66 | 1.21 | 1.01 | −0.11 | 1.27 | 0.88 | 3.33 | −0.95 | 1.27 | |
| B | 0.38 | 0.63 | 1.82 | 1.68 | 1.16 | 1.28 | −0.27 | 0.69 | 0.35 | 2.49 | −0.63 | 1.62 | |
| Midpoint chin miniplate | 1.08 | 1.04 | 1.68 | 1.85 | 1.73 | 0.93 | −0.52 | 1.43 | 0.73 | 2.43 | −1.13 | 1.65 | |
| Right inferior chin miniplate | 1.24 | 1.02 | 1.92 | 2.17 | 1.45 | 1.24 | −0.76 | 1.44 | 0.83 | 2.82 | −0.92 | 1.70 | |
| Left inferior chin miniplate | 1.22 | 0.96 | 1.94 | 1.76 | 1.67 | 1.03 | −0.25 | 1.57 | 0.30 | 2.66 | −1.02 | 1.72 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espino-Segura-Illa, M.; Camps-Font, O.; Ferrer-Fuertes, A.; Cuesta-González, F.; Zubillaga-Rodríguez, I.; Sieira-Gil, R. Waferless Orthognathic Surgery with Customized Osteosynthesis and Surgical Guides: A Prospective Study. Appl. Sci. 2024, 14, 1893. https://doi.org/10.3390/app14051893
Espino-Segura-Illa M, Camps-Font O, Ferrer-Fuertes A, Cuesta-González F, Zubillaga-Rodríguez I, Sieira-Gil R. Waferless Orthognathic Surgery with Customized Osteosynthesis and Surgical Guides: A Prospective Study. Applied Sciences. 2024; 14(5):1893. https://doi.org/10.3390/app14051893
Chicago/Turabian StyleEspino-Segura-Illa, Marc, Octavi Camps-Font, Ada Ferrer-Fuertes, Fran Cuesta-González, Ignacio Zubillaga-Rodríguez, and Ramón Sieira-Gil. 2024. "Waferless Orthognathic Surgery with Customized Osteosynthesis and Surgical Guides: A Prospective Study" Applied Sciences 14, no. 5: 1893. https://doi.org/10.3390/app14051893
APA StyleEspino-Segura-Illa, M., Camps-Font, O., Ferrer-Fuertes, A., Cuesta-González, F., Zubillaga-Rodríguez, I., & Sieira-Gil, R. (2024). Waferless Orthognathic Surgery with Customized Osteosynthesis and Surgical Guides: A Prospective Study. Applied Sciences, 14(5), 1893. https://doi.org/10.3390/app14051893