

Ensemble Learning-Based Coronary Artery Disease Detection Using Computer Tomography Images


Abstract
1. Introduction
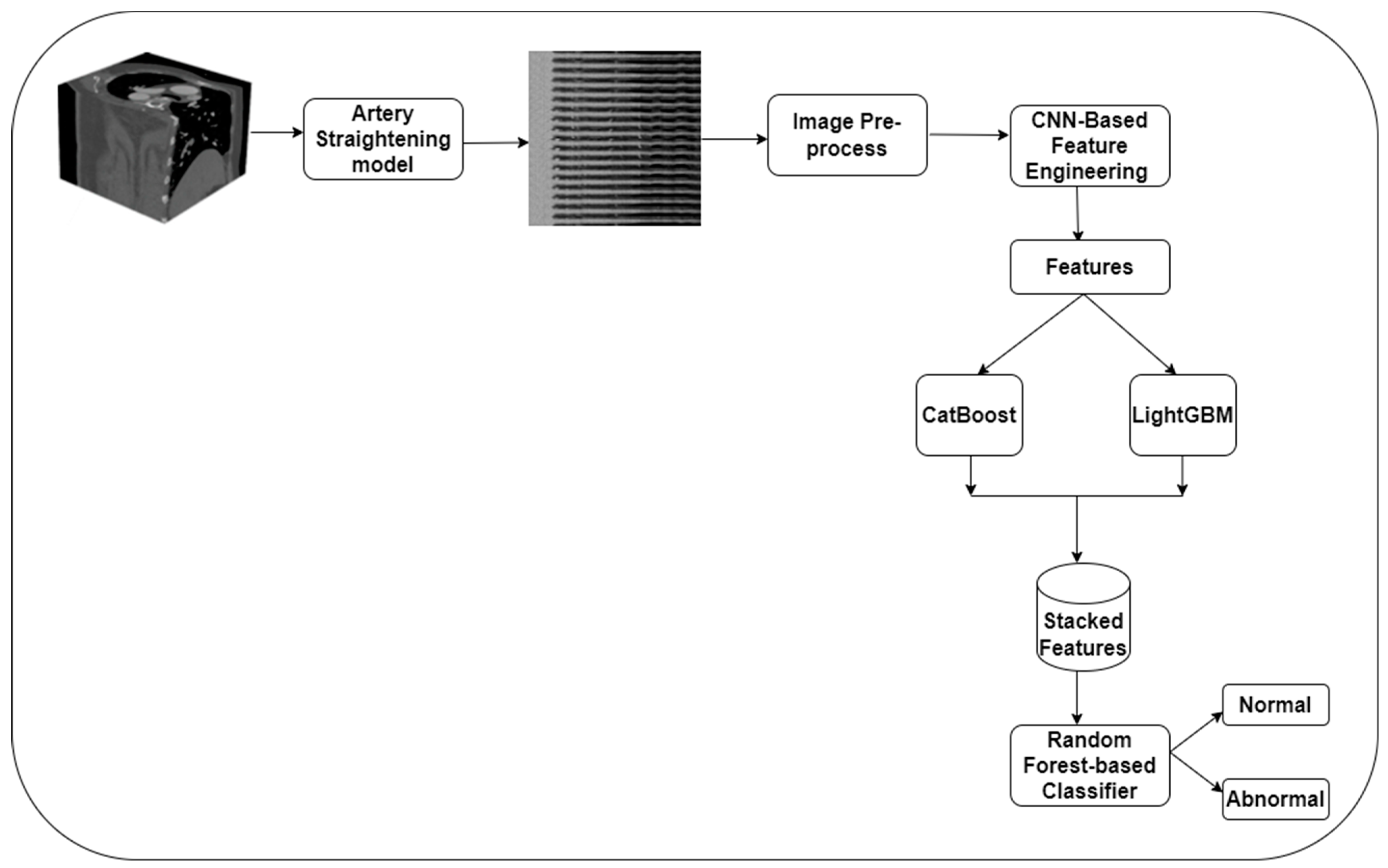
- A feature engineering model based on the MobileNet V3 model is proposed for extracting meaningful features from the CCTA images.
- An EL-based CAD detection model is introduced using CatBoost, LightGBM, and RF classifiers to classify the CCTA images into normal and abnormal classes.
- Generalization of the CAD detection model using real-time datasets.
2. Materials and Methods
2.1. Image Acquisition
2.2. Image Preprocessing
2.3. Feature Engineering
2.4. CAD Identification
2.5. Performance Evaluation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, S.; Rim, B.; Jou, S.-S.; Gil, H.-W.; Jia, X.; Lee, A.; Hong, M. Deep-Learning-Based Coronary Artery Calcium Detection from CT Image. Sensors 2021, 21, 7059. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Fu, Y.; Lin, J.; Ji, Y.; Fang, Y.; Wu, J. Coronary Artery Disease Detection by Machine Learning with Coronary Bifurcation Features. Appl. Sci. 2020, 10, 7656. [Google Scholar] [CrossRef]
- Abdar, M.; Książek, W.; Acharya, U.R.; Tan, R.-S.; Makarenkov, V.; Pławiak, P. A new machine learning technique for an accurate diagnosis of coronary artery disease. Comput. Methods Programs Biomed. 2019, 179, 104992. [Google Scholar] [CrossRef] [PubMed]
- Denzinger, F.; Wels, M.; Breininger, K.; Taubmann, O.; Mühlberg, A.; Allmendinger, T.; Gülsün, M.A.; Schöbinger, M.; André, F.; Buss, S.J.; et al. How scan parameter choice affects deep learning-based coronary artery disease assessment from computed tomography. Sci. Rep. 2023, 13, 2563. [Google Scholar] [CrossRef] [PubMed]
- Zreik, M.; van Hamersvelt, R.W.; Khalili, N.; Wolterink, J.M.; Voskuil, M.; Viergever, M.A.; Leiner, T.; Isgum, I. Deep Learning Analysis of Coronary Arteries in Cardiac CT Angiography for Detection of Patients Requiring Invasive Coronary Angiography. IEEE Trans. Med. Imaging 2019, 39, 1545–1557. [Google Scholar] [CrossRef]
- Cheung, W.K.; Bell, R.; Nair, A.; Menezes, L.J.; Patel, R.; Wan, S.; Chou, K.; Chen, J.; Torii, R.; Davies, R.H.; et al. A Computationally Efficient Approach to Segmentation of the Aorta and Coronary Arteries Using Deep Learning. IEEE Access 2021, 9, 108873–108888. [Google Scholar] [CrossRef]
- Alizadehsani, R.; Abdar, M.; Roshanzamir, M.; Khosravi, A.; Kebria, P.M.; Khozeimeh, F.; Nahavandi, S.; Sarrafzadegan, N.; Acharya, U.R. Machine learning-based coronary artery disease diagnosis: A comprehensive review. Comput. Biol. Med. 2019, 111, 103346. [Google Scholar] [CrossRef]
- Yang, W.; Chen, C.; Yang, Y.; Chen, L.; Yang, C.; Gong, L.; Wang, J.; Shi, F.; Wu, D.; Yan, F. Diagnostic performance of deep learning-based vessel extraction and stenosis detection on coronary com-puted tomography angiography for coronary artery disease: A multi-reader multi-case study. Radiol. Medica 2023, 128, 307–315. [Google Scholar] [CrossRef]
- Al’aref, S.J.; Maliakal, G.; Singh, G.; van Rosendael, A.R.; Ma, X.; Xu, Z.; Alawamlh, O.A.H.; Lee, B.; Pandey, M.; Achenbach, S.; et al. Machine learning of clinical variables and coronary artery calcium scoring for the prediction of obstructive coronary artery disease on coronary computed tomography angiography: Analysis from the CONFIRM registry. Eur. Hear. J. 2020, 41, 359–367. [Google Scholar] [CrossRef]
- Ren, P.; He, Y.; Guo, N.; Luo, N.; Li, F.; Wang, Z.; Yang, Z. A deep learning-based automated algorithm for labeling coronary arteries in computed tomography angiography images. BMC Med. Inform. Decis. Mak. 2023, 23, 249. [Google Scholar] [CrossRef]
- Kaba, Ş.; Haci, H.; Isin, A.; Ilhan, A.; Conkbayir, C. The Application of Deep Learning for the Segmentation and Classification of Coronary Arteries. Diagnostics 2023, 13, 2274. [Google Scholar] [CrossRef] [PubMed]
- Rjiba, S.; Urruty, T.; Bourdon, P.; Fernandez-Maloigne, C.; Delepaule, R.; Christiaens, L.-P.; Guillevin, R. CenterlineNet: Automatic Coronary Artery Centerline Extraction for Computed Tomographic Angiographic Images Using Convolutional Neural Network Architectures. In Proceedings of the 2020 Tenth International Conference on Image Processing Theory, Tools and Applications (IPTA), Paris, France, 9–12 November 2020; pp. 1–6. [Google Scholar]
- Apostolopoulos, I.D.; Apostolopoulos, D.I.; Spyridonidis, T.I.; Papathanasiou, N.D.; Panayiotakis, G.S. Multi-input deep learning approach for Cardiovascular Disease diagnosis using Myocardial Perfusion Imaging and clinical data. Phys. Medica 2021, 84, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Algarni, M.; Al-Rezqi, A.; Saeed, F.; Alsaeedi, A.; Ghabban, F. Multi-constraints based deep learning model for automated segmentation and diagnosis of coronary artery disease in X-ray angiographic images. PeerJ Comput. Sci. 2022, 8, e993. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Xiong, G.; Zeng, H.; Zhou, Q.; Jiang, J.; Guo, X. Machine learning-aided risk strati-fication system for the prediction of coronary artery disease. Int. J. Cardiol. 2021, 326, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Zhang, J.; Xie, H.; Zhao, Y.; Zhang, S.; Gu, L. Automatic detection of coronary artery stenosis by convolutional neural network with temporal constraint. Comput. Biol. Med. 2020, 118, 103657. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Kweon, J.; Roh, J.-H.; Lee, J.-H.; Kang, H.; Park, L.-J.; Kim, D.J.; Yang, H.; Hur, J.; Kang, D.-Y.; et al. Deep learning segmentation of major vessels in X-ray coronary angiography. Sci. Rep. 2019, 9, 16897. [Google Scholar] [CrossRef] [PubMed]
- Magboo VP, C.; Magboo MS, A. Diagnosis of Coronary Artery Disease from Myocardial Perfusion Imaging Using Convolutional Neural Networks. Procedia Comput. Sci. 2023, 218, 810–817. [Google Scholar] [CrossRef]
- Acharya, U.R.; Meiburger, K.M.; Koh, J.E.W.; Vicnesh, J.; Ciaccio, E.J.; Lih, O.S.; Tan, S.K.; Aman, R.R.A.R.; Molinari, F.; Ng, K.H. Automated plaque classification using computed tomography angiography and Gabor transformations. Artif. Intell. Med. 2019, 100, 101724. [Google Scholar] [CrossRef]
- Masuda, T.; Nakaura, T.; Funama, Y.; Oda, S.; Okimoto, T.; Sato, T.; Noda, N.; Yoshiura, T.; Baba, Y.; Arao, S.; et al. Deep learning with convolutional neural network for estimation of the characterisation of coronary plaques: Validation using IB-IVUS. Radiography 2021, 28, 61–67. [Google Scholar] [CrossRef]
- Tatsugami, F.; Higaki, T.; Nakamura, Y.; Yu, Z.; Zhou, J.; Lu, Y.; Fujioka, C.; Kitagawa, T.; Kihara, Y.; Iida, M.; et al. Deep learning–based image restoration algorithm for coronary CT angiography. Eur. Radiol. 2019, 29, 5322–5329. [Google Scholar] [CrossRef]
- Peper, J.; Suchá, D.; Swaans, M.; Leiner, T. Functional cardiac CT–going beyond anatomical evaluation of coronary artery disease with Cine CT, CT-FFR, CT perfusion and machine learning. Br. J. Radiol. 2020, 93, 20200349. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Chiesa, M.; Baggiano, A.; Spadafora, P.; De Santis, R.; Guglielmo, M.; Scafuri, S.; Fusini, L.; Mushtaq, S.; Conte, E.; et al. Diagnostic performance of deep learning algorithm for analysis of computed tomography myocardial perfusion. Eur. J. Nucl. Med. 2022, 49, 3119–3128. [Google Scholar] [CrossRef]
- Wong, K.K.; Fortino, G.; Abbott, D. Deep learning-based cardiovascular image diagnosis: A promising challenge. Futur. Gener. Comput. Syst. 2020, 110, 802–811. [Google Scholar] [CrossRef]
- Serrano-Antón, B.; Otero-Cacho, A.; López-Otero, D.; Díaz-Fernández, B.; Bastos-Fernández, M.; Pérez-Muñuzuri, V.; Muñuzuri, A.P. Muñuzuri. Coronary artery segmentation based on transfer learning and UNet architecture on computed tomography coronary angiography images. IEEE Access 2023, 11, 75484–75496. [Google Scholar] [CrossRef]
- Zhang, J.; Zhu, H.; Chen, Y.; Yang, C.; Cheng, H.; Li, Y.; Wang, F. En-semble machine learning approach for screening of coronary heart disease based on echocardiography and risk factors. BMC Med. Inform. Decis. Mak. 2021, 21, 187. [Google Scholar] [CrossRef]
- Kolukisa, B.; Bakir-Gungor, B. Ensemble feature selection and classification methods for machine learning-based coronary artery disease diagnosis. Comput. Stand. Interfaces 2023, 84, 103706. [Google Scholar] [CrossRef]
- Alothman, A.F.; Sait, A.R.W.; Alhussain, T.A. Detecting Coronary Artery Disease from Computed Tomography Images Using a Deep Learning Technique. Diagnostics 2022, 12, 2073. [Google Scholar] [CrossRef]
- Wahab Sait, A.R.; Dutta, A.K. Developing a Deep-Learning-Based Coronary Artery Disease Detec-tion Technique Using Computer Tomography Images. Diagnostics 2023, 13, 1312. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Liu, J.; Sun, Z.; Cui, Y.; He, Y.; Yang, Z. Deep learning analysis in coronary computed tomographic angiography imaging for the assessment of patients with coronary artery stenosis. Comput. Methods Programs Biomed. 2020, 196, 105651. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Chen, M.; Wang, X.; Wang, X.; Hao, G.; Hao, G.; Cheng, X.; Cheng, X.; Ma, C.; Ma, C.; et al. Diagnostic performance of deep learning-based vascular extraction and stenosis detection technique for coronary artery disease. Br. J. Radiol. 2020, 93, 20191028. [Google Scholar] [CrossRef] [PubMed]
- Papandrianos, N.; Papageorgiou, E. Automatic Diagnosis of Coronary Artery Disease in SPECT Myocardial Perfusion Imaging Employing Deep Learning. Appl. Sci. 2021, 11, 6362. [Google Scholar] [CrossRef]
- Pan, L.-S.; Li, C.-W.; Su, S.-F.; Tay, S.-Y.; Tran, Q.-V.; Chan, W.P. Coronary artery segmentation under class imbalance using a U-Net based architecture on computed tomography angiography images. Sci. Rep. 2021, 11, 14493. [Google Scholar] [CrossRef] [PubMed]
- Zeleznik, R.; Foldyna, B.; Eslami, P.; Weiss, J.; Alexander, I.; Taron, J.; Parmar, C.; Alvi, R.M.; Banerji, D.; Uno, M.; et al. Deep convolutional neural networks to predict cardiovascular risk from computed tomography. Nat. Commun. 2021, 12, 715. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Xiao, J.; Wang, X.; Li, Z.; Guo, N.; Hu, Y.; Li, X.; Wang, X. Clinical Evaluation of the Automatic Coronary Artery Disease Reporting and Data System (CAD-RADS) in Coronary Computed Tomography Angiography Using Convolutional Neural Networks. Acad. Radiol. 2023, 30, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Lee, D.Y.; Cha, W.C.; Chung, M.J.; Lee, K.-S.; Cho, B.H.; Choi, J.H. Automatic stenosis recognition from coronary angiography using convolutional neural networks. Comput. Methods Programs Biomed. 2021, 198, 105819. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, X.; Liu, C.; Zeng, Q.; Zheng, Y.; Chu, X.; Yao, L.; Wang, J.; Jiao, Y.; Karmakar, C. A fusion framework based on multi-domain features and deep learning features of phonocardiogram for coronary artery disease detection. Comput. Biol. Med. 2020, 120, 103733. [Google Scholar] [CrossRef] [PubMed]
- Random Forest Classifier. Available online: https://gist.github.com/pb111/88545fa33780928694388779af23bf58 (accessed on 5 March 2023).
- CatBoost. Available online: https://github.com/catboost/catboost (accessed on 6 March 2023).
- LightGBM. Available online: https://github.com/microsoft/LightGBM (accessed on 7 March 2023).
- Zeng, A.; Wu, C.; Lin, G.; Xie, W.; Hong, J.; Huang, M.; Zhuang, J.; Bi, S.; Pan, D.; Ullah, N.; et al. ImageCAS: A Large-Scale Dataset and Benchmark for Coronary Artery Segmentation based on Computed Tomography Angiography Images. arXiv 2022, arXiv:2211.01607. [Google Scholar] [CrossRef]
- Demirer, M.; Gupta, V.; Bigelow, M.; Erdal, B.; Prevedello, L.; White, R. Image dataset for a CNN algorithm development to detect coronary atherosclerosis in coronary CT angiography. Mendeley Data 2019. [Google Scholar] [CrossRef]
- Candemir, S.; White, R.D.; Demirer, M.; Gupta, V.; Bigelow, M.T.; Prevedello, L.M.; Erdal, B.S. Automated coronary artery atherosclerosis detection and weakly supervised localization on coronary CT angiography with a deep 3-dimensional convo-lutional neural network. Comput. Med. Imaging Graph. 2020, 83, 101721. [Google Scholar] [CrossRef]
- Graham, S.; Epstein, D.; Rajpoot, N. Dense Steerable Filter CNNs for Exploiting Rotational Symmetry in Histology Images. IEEE Trans. Med. Imaging 2020, 39, 4124–4136. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.J.; Chang, W.; Ye, J.C.; Kang, E.; Oh, D.Y.; Lee, Y.J.; Park, J.H.; Kim, Y.H. Low-Dose Abdominal CT Using a Deep Learning-Based Denoising Algorithm: A Comparison with CT Reconstructed with Filtered Back Projection or Iterative Reconstruction Algorithm. Korean J. Radiol. 2020, 21, 356–364. [Google Scholar] [CrossRef]
- Disanto, A.; Pepe, A.; Petrelli, L.; Gsaxner, C.; Li, J.; Jin, Y.; Brunetti, A.; Buongiorno, D.; Egger, J.; Bevilacqua, V. Enhancement of aortic dissections in CT angiography: Are common filters robust enough? In Medical Imaging 2022: Biomedical Applications in Molecular, Structural, and Functional Imaging; SPIE: Bellingham, WA, USA, 2022; Volume 12036, pp. 617–623. [Google Scholar]
- Yunus, M.M.; Sabarudin, A.; Karim, M.K.A.; Nohuddin, P.N.E.; Zainal, I.A.; Shamsul, M.S.M.; Yusof, A.K.M. Reproducibility and Repeatability of Coronary Computed Tomography Angiography (CCTA) Image Segmentation in Detecting Atherosclerosis: A Radiomics Study. Diagnostics 2022, 12, 2007. [Google Scholar] [CrossRef] [PubMed]
- Baskaran, L.; Maliakal, G.; Al’Aref, S.J.; Singh, G.; Xu, Z.; Michalak, K.; Min, J.K. Identification and quantification of cardiovascular structures from CCTA: An end-to-end, rapid, pixel-wise, deep-learning method. Cardiovasc. Imaging 2020, 13, 1163–1171. [Google Scholar]
- Cui, H. Supervised Filter Learning for Coronary Artery Vesselness Enhancement Diffusion in Coronary CT Angiography Images. Int. J. Comput. Intell. Syst. 2020, 13, 488–495. [Google Scholar] [CrossRef]
- Sukanya, A.; Rajeswari, R. A modified Frangi’s vesselness measure based on gradient and grayscale values for coronary artery detection. J. Intell. Fuzzy Syst. 2019, 37, 2327–2336. [Google Scholar] [CrossRef]
- Muñoz-Gil, G.; Volpe, G.; Garcia-March, M.A.; Aghion, E.; Argun, A.; Hong, C.B.; Bland, T.; Bo, S.; Conejero, J.A.; Firbas, N.; et al. Objective comparison of methods to decode anomalous diffusion. Nat. Commun. 2021, 12, 6253. [Google Scholar] [CrossRef]
- Thapa, S.; Park, S.; Kim, Y.; Jeon, J.-H.; Metzler, R.; A Lomholt, M. Bayesian inference of scaled versus fractional Brownian motion. J. Phys. A Math. Theor. 2022, 55, 194003. [Google Scholar] [CrossRef]
- Muñoz-Gil, G.; Garcia-March, M.A.; Manzo, C.; Martín-Guerrero, J.D.; Lewenstein, M. Single tra-jectory characterization via machine learning. New J. Phys. 2020, 22, 013010. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Normal | Abnormal | Total Number of Images |
|---|---|---|---|
| 1 | 503 | 497 | 1000 |
| 2 | 1182 | 1182 | 2364 |
| Classes/ Metrics | Acc | Pre | Rec | F1 | Kap |
|---|---|---|---|---|---|
| Dataset 1 | |||||
| Normal | 99.8 | 98.9 | 99.1 | 99.0 | 95.6 |
| Abnormal | 99.7 | 99.1 | 98.8 | 98.9 | 95.8 |
| Average | 99.7 | 99.0 | 98.9 | 98.9 | 95.7 |
| Dataset 2 | |||||
| Normal | 99.6 | 98.8 | 98.7 | 98.7 | 95.7 |
| Abnormal | 99.7 | 98.9 | 98.6 | 98.7 | 95.8 |
| Average | 99.6 | 98.8 | 98.6 | 98.7 | 95.7 |
| Classes/Metrics | Acc | Pre | Rec | F1 | Kap |
|---|---|---|---|---|---|
| Alothman et al. [28] | 98.6 | 98.2 | 98.1 | 98.1 | 95.1 |
| Wahab Sait et al. [29] | 99.5 | 98.9 | 98.9 | 98.9 | 96.2 |
| Huang et al. [35] | 98.3 | 97.2 | 97.0 | 97.1 | 94.1 |
| Li et al. [37] | 97.4 | 97.5 | 97.8 | 97.6 | 93.4 |
| Moon et al. [36] | 98.5 | 97.9 | 97.6 | 97.7 | 94.7 |
| EfficientNet B7 | 97.8 | 96.9 | 97.2 | 97.0 | 91.5 |
| MobileNet V3 | 98.1 | 97.4 | 97.6 | 97.5 | 92.1 |
| Proposed Model | 99.7 | 99.0 | 98.9 | 98.9 | 95.7 |
| Classes/Metrics | Acc | Pre | Rec | F1 | Kap |
|---|---|---|---|---|---|
| Alothman et al. [28] | 98.6 | 98.2 | 97.8 | 97.9 | 94.2 |
| Wahab Sait et al. [29] | 99.4 | 98.5 | 98.6 | 98.7 | 95.0 |
| Huang et al. [35] | 97.5 | 97.1 | 97.5 | 97.2 | 93.2 |
| Li et al. [37] | 98.4 | 97.5 | 97.9 | 97.8 | 92.8 |
| Moon et al. [36] | 98.5 | 97.6 | 98.2 | 97.9 | 93.8 |
| EfficientNet B7 | 96.8 | 97.2 | 97.6 | 97.4 | 91.8 |
| MobileNet V3 | 97.2 | 96.9 | 97.3 | 97.4 | 92.2 |
| Proposed Model | 99.6 | 98.8 | 98.6 | 98.7 | 95.7 |
| Classes/Metrics | Dataset 1 | Dataset 2 | ||||
|---|---|---|---|---|---|---|
| Loss | SD | CI | Loss | SD | CI | |
| Alothman et al. [28] | 2.7 | 0.0021 | [96.62–96.71] | 2.3 | 0.0017 | [98.55–98.61] |
| Wahab Sait et al. [29] | 1.9 | 0.0019 | [97.41–97.49] | 1.8 | 0.0019 | [98.64–98.72] |
| Huang et al. [35] | 2.4 | 0.0026 | [96.57–97.23] | 1.6 | 0.0019 | [97.81–98.42] |
| Li et al. [37] | 2.7 | 0.0027 | [95.81–96.34] | 2.5 | 0.0023 | [98.52–98.69] |
| Moon et al. [36] | 3.2 | 0.0029 | [95.82–98.91] | 2.4 | 0.0016 | [97.32–97.42] |
| EfficientNet B7 | 1.9 | 0.0035 | [96.13–97.15] | 1.7 | 0.0018 | [97.56–98.21] |
| MobileNet V3 | 2.2 | 0.0029 | [97.21–96.23] | 2.5 | 0.0021 | [98.12–98.26] |
| Proposed Model | 1.2 | 0.0013 | [98.41–98.72] | 1.2 | 0.0011 | [98.57–98.89] |
| Classes/Metrics | Dataset 1 | Dataset 2 | ||||
|---|---|---|---|---|---|---|
| Parameters (in Millions (M)) | FLOPs (in Giga (G)) | Learning Rate | Parameters (in Millions (M)) | FLOPs (in Giga (G)) | Learning Rate | |
| Alothman et al. [28] | 5.2 | 15.9 | 1 × | 4.3 | 16.2 | 1 × |
| Wahab Sait et al. [29] | 3.6 | 17.5 | 1 × | 3.6 | 15.8 | 1 × |
| Huang et al. [35] | 6.9 | 23.5 | 1 × | 8.1 | 24.6 | 1 × |
| Li et al. [37] | 7.1 | 24.9 | 1 × | 9.6 | 24.8 | 1 × |
| Moon et al. [36] | 7.4 | 23.7 | 1 × | 7.4 | 23.9 | 1 × |
| EfficientNet B7 | 4.8 | 15.8 | 1 × | 5.9 | 17.8 | 1 × |
| MobileNet V3 | 5.1 | 12.6 | 1 × | 4.8 | 13.4 | 1 × |
| Proposed Model | 3.8 | 12.1 | 1 × | 4.1 | 12.5 | 1 × |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sait, A.R.W.; Awad, A.M.A.B. Ensemble Learning-Based Coronary Artery Disease Detection Using Computer Tomography Images. Appl. Sci. 2024, 14, 1238. https://doi.org/10.3390/app14031238
Sait ARW, Awad AMAB. Ensemble Learning-Based Coronary Artery Disease Detection Using Computer Tomography Images. Applied Sciences. 2024; 14(3):1238. https://doi.org/10.3390/app14031238
Chicago/Turabian StyleSait, Abdul Rahaman Wahab, and Ali Mohammad Alorsan Bani Awad. 2024. "Ensemble Learning-Based Coronary Artery Disease Detection Using Computer Tomography Images" Applied Sciences 14, no. 3: 1238. https://doi.org/10.3390/app14031238
APA StyleSait, A. R. W., & Awad, A. M. A. B. (2024). Ensemble Learning-Based Coronary Artery Disease Detection Using Computer Tomography Images. Applied Sciences, 14(3), 1238. https://doi.org/10.3390/app14031238