
Examination of the Validity and Reliability of the Greek Version of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.2.1. Demographics
2.2.2. The Psychological Readiness of Injured Athlete to Return to Sport Questionnaire (PRIA-RS)
2.2.3. The Causes of Re-Injury Worry Questionnaire (CR-IWQ)
- “Re-injury worry due to rehabilitation” (Cronbach’s α = 0.95, score range 8–56): higher scores indicate increased concern about re-injury due to poor rehabilitation programs;
- “Re-injury worry due to opponent’s ability” (Cronbach’s α = 0.93, score range 4–28): a higher score implies greater concern about re-injury due to the opponent’s ability [30].
2.2.4. The Sport Confidence Questionnaire of Rehabilitated Athletes Returning to Competition (SCQ-RARC)
- “Confidence due to rehabilitation” (Cronbach’s α = 0.93, score range 8–56): a higher score means the athlete’s confidence has increased as a result of a successful rehabilitation program;
- “General confidence” (Cronbach’s α = 0.97, score range 6–42): a greater score indicates that the athlete feels more confident in their own capabilities [31].
2.2.5. The Attention Questionnaire of Rehabilitated Athletes Returning to Competition (AQ-RARC)
- “Functional attention” (Cronbach’s α = 0.97, score range 7–49): a higher score implies greater attention by the athlete;
- “Distraction attention” (Cronbach’s α = 0.94, score range 3–21): an athlete who scores higher is more easily distracted [32].
2.3. Procedure
Validation Procedure
2.4. Statistical Analysis
3. Results
3.1. Face and Content Validity
3.2. Internal Consistency and Test–Retest Reliability
3.3. Construct Validity
3.4. Concurrent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| 1 | 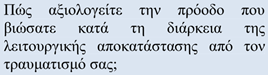 | ΠOΛΥ ΚAΚH □ | ΚAΚH □ | OΥΤΕ ΚAΛH OΥΤΕ ΚAΚH □ | ΚAΛH □ | ΠOΛΥ ΚAΛH □ |
| 2 | Πώς είναι η διάθεσή σας; | ΠOΛΥ ΚAΚH □ | ΚAΚH □ | OΥΤΕ ΚAΚH □ OΥΤΕ ΚAΛH | ΚAΛH □ | ΠOΛΥ ΚAΛH □ |
| 3 | Πώς είναι η φυσική σας κατάσταση ενόψει μίας πιθανής επιστροφής στην ομάδα; | ΠOΛΥ ΚAΚH □ | ΚAΚH □ | OΥΤΕ ΚAΚH □ OΥΤΕ ΚAΛH | ΚAΛH □ | ΠOΛΥ ΚAΛH □ |
| 4 | Πώς αξιολογείτε τη λειτουργικότητα της τραυματισμένης σας περιοχής; | ΠOΛΥ ΚAΚH □ | ΚAΚH □ | OΥΤΕ ΚAΚH □ OΥΤΕ ΚAΛH | ΚAΛH □ | ΠOΛΥ ΚAΛH □ |
| 5 | Aισθάνεστε κάποια ενόχληση ή κάποιο κώλυμα που σας αποτρέπει να προπονηθείτε σε κανονικό ρυθμό; | ΝAΙ □ | - | ΔΕΝ ΞΕΡΩ □ | - | OΧΙ □ |
| 6 | Aισθάνεστε νευρικά σχετικά με την επιστροφή στην κανονική προπόνηση με την ομάδα; | ΝAΙ □ | - | ΔΕΝ ΞΕΡΩ □ | - | OΧΙ □ |
| 7 | Πόσο ασφαλής αισθάνεστε όταν συμμετέχετε σε φυσικές δραστηριότητες ή όταν κινείτε την τραυματισμένη περιοχή; | ΕΛAΧΙΣΤA □ | ΛΙΓO □ | OΥΤΕ ΠOΛΥ OΥΤΕ ΛΙΓO □ | ΠOΛΥ □ | ΠAΡA ΠOΛΥ □ |
| 8 | Δώστε μία εκτιμώμενη πιθανότητα να βιώσετε σύντομα έναν ίδιο επανατραυματισμό. | 80–100% □ | 60–80% □ | 40–60% □ | 20–40% □ | 0–20% □ |
| 9 | Πόση πίεση αισθάνεστε από τον περίγυρό σας όσον αφορά την επιστροφή σας στην προπόνηση με την ομάδα; | ΥΠΕΡΒOΛΙΚH □ | ΥΨHΛH □ | ΚAΝOΝΙΚH □ | ΧAΜHΛH □ | ΜHΔΕΝΙΚH □ |
| 10 | Πώς θα αξιολογούσατε τη γενική σας κατάσταση ενόψει μίας πιθανής επιστροφής σας σε πλήρη προπόνηση; | ΠOΛΥ ΚAΚH □ | ΚAΚH □ | OΥΤΕ ΚAΛH OΥΤΕ ΚAΚH □ | ΚAΛH □ | ΠOΛΥ ΚAΛH □ |
References
- SFIA. 2022 Sports, Fitness, and Leisure Activities Topline Participation Report; Sports & Fitness Industry Association: Laurel, MD, USA, 2022. [Google Scholar]
- Åman, M.; Forssblad, M.; Henriksson-Larsén, K. Incidence and severity of reported acute sports injuries in 35 sports using insurance registry data. Scand. J. Med. Sci. Sports 2016, 26, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Hulteen, R.M.; Smith, J.J.; Morgan, P.J.; Barnett, L.M.; Hallal, P.C.; Colyvas, K.; Lubans, D.R. Global participation in sport and leisure-time physical activities: A systematic review and meta-analysis. Prev. Med. 2017, 95, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Bueno, A.M.; Pilgaard, M.; Hulme, A.; Forsberg, P.; Ramskov, D.; Damsted, C.; Nielsen, R.O. Injury prevalence across sports: A descriptive analysis on a representative sample of the Danish population. Inj. Epidemiol. 2018, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Smpokos, E.; Mourikis, C.; Theos, C.; Linardakis, M. Injury prevalence and risk factors in a Greek team’s professional football (soccer) players: A three consecutive seasons survey. Res Sports Med. 2019, 27, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injury incidence and distribution in elite football—A prospective study of the Danish and the Swedish top divisions. Scand. J. Med. Sci. Sports 2005, 15, 21–28. [Google Scholar] [CrossRef]
- Stubbe, J.H.; van Beijsterveldt, A.M.M.; van der Knaap, S.; Stege, J.; Verhagen, E.A.; Van Mechelen, W.; Backx, F.J. Injuries in professional male soccer players in the Netherlands: A prospective cohort study. J. Athl. Train. 2015, 50, 211–216. [Google Scholar] [CrossRef]
- Gómez-Piqueras, P.; Ardern, C.; Prieto-Ayuso, A.; Robles-Palazón, F.J.; Cejudo, A.; Baranda, P.S.; Olmedilla, A. Psychometric Analysis and Effectiveness of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire on Injured Soccer Players. Int. J. Environ. Res. Public Health 2020, 17, 1536. [Google Scholar] [CrossRef] [PubMed]
- Gkikopoulos, G.; Chronopoulou, C.; Christakou, A. Examining re-injury worry, confidence and attention after a sport musculoskeletal injury. J. Sports Med. Phys. Fit. 2020, 60, 428–434. [Google Scholar] [CrossRef]
- Wiese-Bjornstal, D.M.; Smith, A.M.; Shaffer, S.M.; Morrey, M.A. An integrated model of response to sport injury: Psychological and sociological dynamics. J. Appl. Sport Psychol. 1998, 10, 46–69. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. A systematic review of the psychological factors associated with returning to sport following injury. Br. J. Sports Med. 2013, 47, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Forsdyke, D.; Smith, A.; Jones, M.; Gledhill, A. Psychosocial factors associated with outcomes of sports injury rehabilitation in competitive athletes: A mixed studies systematic review. Br. J. Sports Med. 2016, 50, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Sonesson, S.; Kvist, J.; Ardern, C.; Österberg, A.; Silbernagel, K.G. Psychological factors are important to return to pre-injury sport activity after anterior cruciate ligament reconstruction: Expect and motivate to satisfy. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Fischerauer, S.F.; Talaei-Khoei, M.; Bexkens, R.; Ring, D.C.; Oh, L.S.; Vranceanu, A.M. What is the relationship of fear avoidance to physical function and pain intensity in injured athletes? Clin. Orthop. Relat. Res. 2018, 476, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Clement, D.; Arvinen-Barrow, M.; Fetty, T. Psychosocial responses during different phases of sport-injury rehabilitation: A qualitative study. J. Athl. Train. 2015, 50, 95–104. [Google Scholar] [CrossRef]
- Podlog, L.; Wadey, R.; Stark, A.; Lochbaum, M.; Hannon, J.; Newton, M. An adolescent perspective on injury recovery and the return to sport. Psychol. Sport Exerc. 2013, 14, 437–446. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: An updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br. J. Sports Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef]
- Podlog, L.; Banham, S.M.; Wadey, R.; Hannon, J.S. Psychological readiness to return to competitive sport following injury: A qualitative study. Sport Psychol. 2015, 29, 1–14. [Google Scholar] [CrossRef]
- Nwachukwu, B.U.; Adjei, J.; Rauck, R.C.; Chahla, J.; Okoroha, K.R.; Verma, N.N.; Allen, A.A.; Williams, R.J. How much do psychological factors affect lack of return to play after anterior cruciate ligament reconstruction? A systematic review. Orthop. J. Sports Med. 2019, 7, 2325967119845313. [Google Scholar] [CrossRef]
- Piussi, R.; Berghdal, T.; Sundemo, D.; Grassi, A.; Zaffagnini, S.; Sansone, M.; Samuelsson, K.; Senorski, E.H. Self-Reported symptoms of depression and anxiety after ACL injury: A Systematic Review. Orthop. J. Sports Med. 2022, 10, 23259671211066493. [Google Scholar] [CrossRef]
- McPherson, A.L.; Feller, J.A.; Hewett, T.E.; Webster, K.E. Smaller change in psychological readiness to return to sport is associated with second anterior cruciate ligament injury among younger patients. Am. J. Sports Med. 2019, 47, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Christakou, A.; Stavrou, N.A.; Psychountaki, M.; Zervas, Y. Re-injury worry, confidence and attention as predictors of a sport re-injury during a competitive season. Res. Sports Med. 2020, 30, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Bizzini, M. Consensus statement on return to sport from the First World Congress in Sports Physical. Br. J. Sports Med. 2016, 50, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, H.P.; Pollock, N.; Chakraverty, R.; Ardern, C.L. Return to play in elite sport: A shared decision-making process. Br. J. Sports Med. 2017, 51, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Piqueras, P.; Sainz de Baranda, P.; Ortega, E.; Contreras, O.; Olmedilla, A. Design and validation of a questionnaire on the perception of the athlete regarding his return to training after injury. Rev. Psicol. Deporte 2014, 23, 479–487. [Google Scholar]
- Glazer, D. Development and preliminary validation of the injury-psychological readiness to return to sport (I-PRRS) scale. J. Athl. Train. 2009, 44, 185–189. [Google Scholar] [CrossRef]
- Walker, N.; Thatcher, J.; Lavallee, D. A preliminary development of the Re-Injury Anxiety Inventory (RIAI). Phys. Ther. Sport 2010, 11, 23–29. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A.; Lambros, C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Phys. Ther. Sport 2008, 9, 9–15. [Google Scholar] [CrossRef]
- Christakou, A.; Zervas, Y.; Stavrou, N.A.; Psychountaki, M. Development and validation of the Causes of Re-Injury Worry Questionnaire. Psychol. Health Med. 2011, 16, 94–114. [Google Scholar] [CrossRef]
- Christakou, A.; Stavrou, N.A.; Psychountaki, M.; Zervas, Y. Development and validation of sport confidence questionnaire of rehabilitated athletes returning to competition. Ann. Orthop. Musculoskelet. Dis. 2019, 2, 1021. [Google Scholar]
- Christakou, A.; Zervas, Y.; Psychountaki, M.; Stavrou, N.A. Development and validation of the Attention Questionnaire of Rehabilitated Athletes Returning to Competition. Psychol. Health Med. 2012, 17, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Hatcher, L.; Stepanski, E.J. A Step-by-Step Approach to Using the SAS System for Univariate and Multivariate Statistics; SAS Institute: Cary, NC, USA, 1994. [Google Scholar]
- Calvert, M.; Brundage, M.; Jacobsen, P.B.; Schünemann, H.J.; Efficace, F. The CONSORT Patient-Reported Outcome (PRO) extension: Implications for clinical trials and practice. Health Qual. Life Outcomes 2013, 11, 184. [Google Scholar] [CrossRef] [PubMed]
- Parlakidis, K.; Krokos, D.; Sagredaki, M.-L.; Kontopoulos, L.A.; Christakou, A. Examining the Relationship between Psychological and Functional Status after a Sports Musculoskeletal Injury. Appl. Sci. 2024, 14, 8258. [Google Scholar] [CrossRef]
- Christakou, A.; Gkiokas, G.; Valsamis, N.; Paraskevopoulos, E.; Papandreou, M. Examining the Relationship and the Gender Differences between Re-Injury Worry, Confidence, and Attention after a Sport Musculoskeletal Injury. J. Clin. Med. 2024, 13, 4428. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation andcultural adaptation process for patient-reported outcomes (PRO)measures: Report of the ISPOR task force for translation and cultural adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Osborne, J.; Costello, A.; Kellow, J. Best practices in exploratory factor analysis. In Best Practices in Quantitative Methods; Osborne, J., Ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2008; pp. 86–99. [Google Scholar]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar]
- Tabachnick, B.G.; Fidell, I.S. Using Multivariate Statistics; Harper Collins Publishers: New York, NY, USA, 1996. [Google Scholar]
- Worthington, R.W.; Whittaker, T.A. Scale development research: A content analysis and recommendations for best practices. Couns. Psychol. 2006, 34, 806–838. [Google Scholar] [CrossRef]
- Babbie, E. (Ed.) Conceptualization and measurements. In Practice of Social Research; Wadsworth Publishing Company: Belmont, CA, USA, 1992; pp. 113–135. [Google Scholar]
- Kline, P. (Ed.) Validity of psychosocial tests. In The Handbook of Psychological Testing; Routledge: London, UK, 1995; pp. 15–28. [Google Scholar]
- Johnston, L.H.; Carroll, D. The context of emotional responses to athletic injury: A qualitative analysis. J. Sport Rehabil. 1998, 7, 206–220. [Google Scholar] [CrossRef]
- Kahn, J.H. Factor analysis in counselling psychology research, training, and practice: Principles, advances, and applications. Couns. Psychol. 2006, 34, 684–718. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Marx, R.G.; Menezes, A.; Horovitz, L.; Jones, E.C.; Warren, R.F. A comparison of two time intervals for test-retest reliability of health status instruments. J. Clin. Epidemiol. 2003, 56, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Danner, D.; Aichholzer, J.; Rammstedt, B. Acquiescence in personality questionnaires: Relevance, domain specificity, and stability. J. Res. Pers. 2015, 57, 119–130. [Google Scholar] [CrossRef]
- Ferrando, P.J.; Morales-Vives, F.; Lorenzo-Seva, U. Assessing and controlling acquiescent responding when acquiescence and content are related: A comprehensive factor-analytic approach. Struct. Equ. Model. 2016, 23, 713–725. [Google Scholar] [CrossRef]
| Variables | Min/Max | M | SD |
|---|---|---|---|
| Age | 18/35 | 24.68 | 3.94 |
| Competitive experience (years) | 2/20 | 8.63 | 4.09 |
| Duration of injury (days) | 14/60 | 20.7 | 8.23 |
| Duration of absence from sport (days) | 15/60 | 20.9 | 8.18 |
| Duration of physiotherapy treatment (days) | 7/60 | 18.58 | 8.81 |
| Physiotherapy treatment sessions (per week) | 2/5 | 2.73 | 0.79 |
| Frequency | Percentage | ||
| Sex | Man | 113 | 100 |
| Sport | Football | 113 | 100 |
| Competing level | Amateur | 113 | 100 |
| Area of injury (Muscles/Tendons/ligaments) | Ankle | 36 | 31.9 |
| Knee | 15 | 13.3 | |
| Thigh | 58 | 51.3 | |
| Hip | 4 | 3.5 | |
| Medical treatment | Yes | 41 | 36.3 |
| No | 72 | 63.7 | |
| Injury deterioration | Yes | 8 | 7.1 |
| No | 105 | 92.9 |
| ICC | 95% Confidence Interval | SEM | (SEM/Grand Mean) × 100% | Cronbach’s α | ||
|---|---|---|---|---|---|---|
| Lower bound | Upper bound | |||||
| PRIA-RS | 0.991 | 0.978 | 0.996 | 3.15 | 8.18% | 0.82 |
| 1st factor a | 0.994 | 0.973 | 0.998 | 2.44 | 9.20% | 0.81 |
| 2nd factor b | 0.973 | 0.962 | 0.978 | 1.64 | 15.07% | 0.76 |
| Factor Loadings | |||
|---|---|---|---|
| PRIA-RS | 1st a | 2nd b | Communalities |
| Item 1 | 0.644 | 0.423 | |
| Item 2 | 0.743 | 0.649 | |
| Item 4 | 0.550 | 0.313 | |
| Item 5 | 0.880 | 0.832 | |
| Item 7 | 0.930 | 0.880 | |
| Item 9 | 0.578 | 0.334 | |
| Item 10 | 0.783 | 0.617 | |
| Item 3 | 0.713 | 0.508 | |
| Item 6 | 0.652 | 0.469 | |
| Item 8 | 0.568 | 0.425 | |
| Eigenvalues | 4.413 | 1.939 | |
| % explained variance | 44.13 | 19.39 | |
| % cumulative variance | 63.52 | ||
| SCQ-RARC | CR-IWQ | AQ-RARC | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SCQ-RARC d | CO-R e | G-CO f | CR-IWQ g | CR-IW Rehab h | CR-IW Opponent’s Ability i | AQ-RARC j | F-At k | At-D l | |
| PRIA-RS a | 0.366 ** | 0.401 ** | 0.271 ** | −0.128 | −0.111 ** | −0.127 | 0.321 | 0.369 ** | 0.186 * |
| 1st factor b | 0.335 * | 0.307 ** | 0.245 ** | −0.079 | −0.08 | −0.056 | 0.312 | 0.346 ** | 0.167 |
| 2nd factor c | 0.261 * | 0.276 ** | 0.231 * | −0.197 * | −0.129 | −0.249 ** | 0.235 | 0.262 ** | 0.107 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krokos, D.; Kandanoleon, A.; Paraskevopoulos, E.; Tsekoura, M.; Kapreli, E.; Christakou, A. Examination of the Validity and Reliability of the Greek Version of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire. Appl. Sci. 2024, 14, 11655. https://doi.org/10.3390/app142411655
Krokos D, Kandanoleon A, Paraskevopoulos E, Tsekoura M, Kapreli E, Christakou A. Examination of the Validity and Reliability of the Greek Version of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire. Applied Sciences. 2024; 14(24):11655. https://doi.org/10.3390/app142411655
Chicago/Turabian StyleKrokos, Dimitrios, Andreas Kandanoleon, Eleftherios Paraskevopoulos, Maria Tsekoura, Eleni Kapreli, and Anna Christakou. 2024. "Examination of the Validity and Reliability of the Greek Version of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire" Applied Sciences 14, no. 24: 11655. https://doi.org/10.3390/app142411655
APA StyleKrokos, D., Kandanoleon, A., Paraskevopoulos, E., Tsekoura, M., Kapreli, E., & Christakou, A. (2024). Examination of the Validity and Reliability of the Greek Version of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire. Applied Sciences, 14(24), 11655. https://doi.org/10.3390/app142411655