
Assessing Table Tennis Technical Proficiency in Individuals with Disabilities: A Scoping Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Research Question
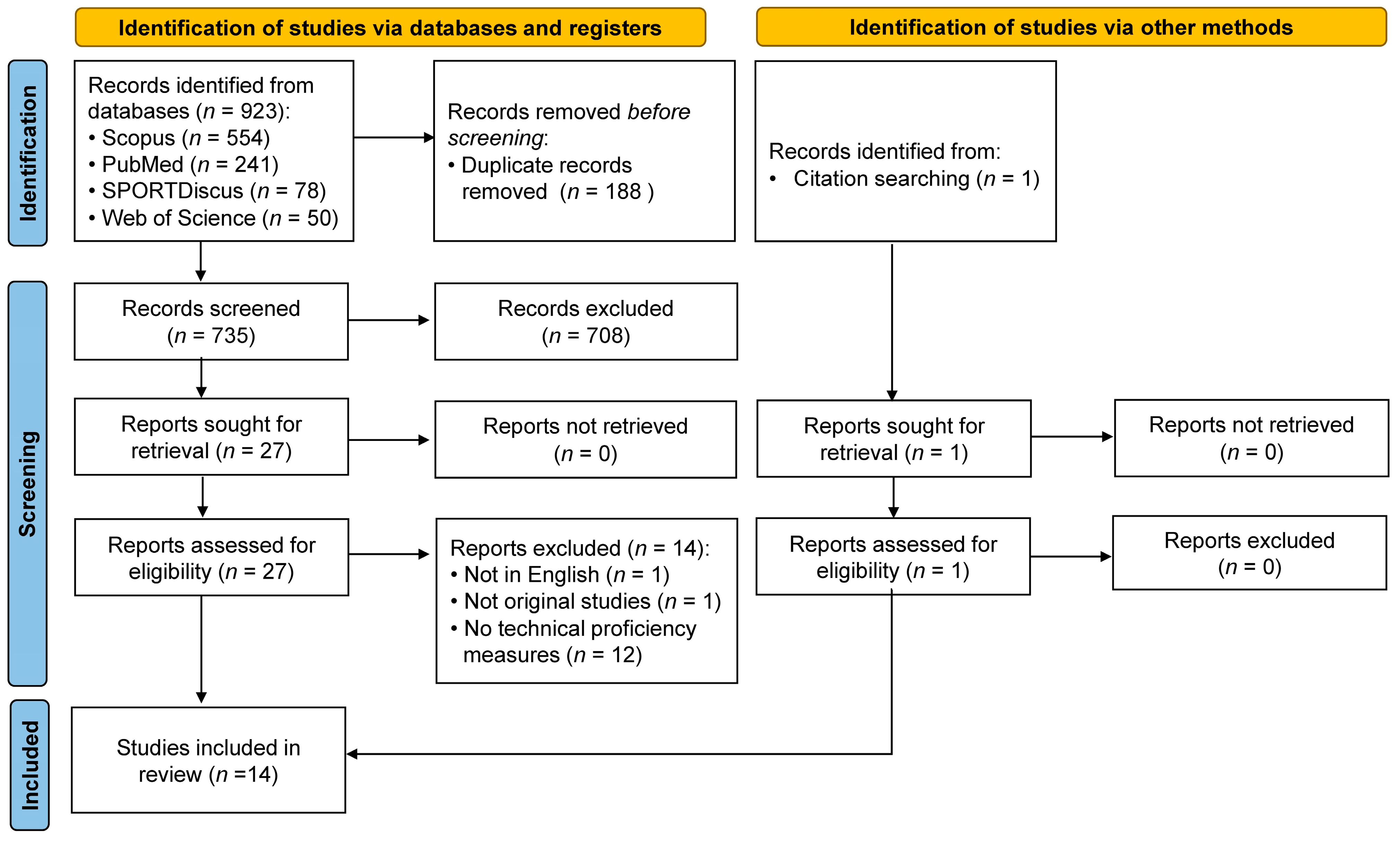
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Selection of Studies
2.5. Data Extraction
3. Results
3.1. Overview of Study Characteristics

{kind=link}
{kind=link}
| Articles | Country/Region | Participants | Protocols | Key Findings |
|---|---|---|---|---|
| Galas et al. [27] | Poland | 23 para-table tennis players (16 males, 7 females) in the senior Polish para-table tennis team (MAge 31.8 ± 12.22 years; MPlay 16.9 ± 10.5 years; MWeek 9.7 ± 4.7 h):
| Stroke accuracy was assessed at high ball speed (80 balls per minute) delivered by a robot:
| Reliability over 3 sessions: slight agreement for extreme side service (ICC = 0.25) and strong agreement for the other 5 tests (ICC = 0.52–0.66).No difference between types of disability; test results not correlated with world rankings. |
| Smits-Engelsman et al. [31] | South Africa | 50 (25 boys, 25 girls) Grade 1 to Grade 3 children (MAge 7.2 ± 1.0 years), including 16 developmental coordination disorders (DCDs) and 34 typically developing (TD). | “Cup Ping-Pong” game: This game was performed in small groups of 2–4 children supervised by two physiotherapists. Participants were instructed to throw a Ping-Pong (table tennis) ball against the wall at 1 m distance and catch it in a plastic beer cup in the other hand. A total of 10 trials were conducted and the number of times the ball was caught was counted. | Both children with DCD and TD performed better on trained and non-trained balls, and balance and agility tasks after 10 weeks of training via active video games. |
| Van Biesen et al. [16] | 16 countries from 3 different continents (Europe, Africa, and Asia) | 47 male elite table tennis players:
| Table tennis-specific test battery for service return accuracy:
| The elite table tennis players with ID did not reach the same level of technical proficiency in returning serves compared to players without ID. |
| Van Biesen et al. [19] | 15 countries from 5 different continents (Europe, Africa, Australia, Asia, and South America) | Elite table tennis players with (n = 71) and without ID (n = 17).Players with ID (90% competed in the INAS World Championships, MPlay 13 ± 5 years):
| The players were asked to play 12 series of 5 rallies against an able-bodied opponent. There were 6 service variations delivered in a standardised sequence:
| Inter-rater reliability (r = 0.75); intra-rater reliability (r = 0.90) among coaches.Lower proficiency scores in players with ID than those without ID.No significant correlation (r = 0.08, p > 0.05) between the total tactical proficiency and IQ scores in players with ID. |
| Wu et al. [21] | 5 continents including 23 countries | 87 (56 males, 31 females) international players with ID (MAge 2.69 ± 8.1 years, MPlay 11.8 ± 7.3 years, MWeek10.4 ± 6.9 h). | Service Accuracy—players were instructed to perform 6 types of service:
| Recommendation of cut-off scores to classify players:
|
| Articles | Country/Region | Participants | Protocols | Key Findings |
|---|---|---|---|---|
| Inbal et al. [30] | Israel | 20 Special Olympics table tennis players (sex: NR):
| Construction of 4 types of tests with motor actions linked to table tennis skills:
| Good internal consistency between items in each type of tests:
|
| Kong and Yam [22] | Singapore | International para-athlete (1 male, 51 years, Class 7, 20 years of playing experience).Able-bodied controls (9 male university students, MAge 23.5 ± 1.6 years, MPlay 13.4 ± 2.6 years).All trained at least 2 sessions per week in the past 3 months. | Balls were delivered by a table tennis robot. Participants performed 30 trials (3 sets of 10 consecutive drives) for forehand topspin drives and 30 trials (3 sets of 10 consecutive drives) for backhand topspin drives. They were instructed to return the ball diagonally to land on the lower half of the table within the marked 0.80 m × 0.76 m zone. Returns were deemed valid when the ball landed diagonally within the target zone. Shoulder abduction/adduction angles and joint range of motion were measured using inertial sensors. | Joint range of motion of the para-player was comparable to the control group in the forehand [para-player 38°, controls32 (15)°] and larger in the backhand [para-player 35°, controls 24 (16)°].Waveform analysis revealed differences (p < 0.05) in movement patterns. |
| Lim et al. [24] | Singapore | 6 wheelchair para-table tennis players (sex: NR) from the National Table Tennis Team:
| Sweep time (ST)—players were required to perform forehand and backhand stroke shots on balls placed in 6 different positions. The table tennis balls were propped up to 40 mm high and positioned on designated positions (maximum/intermediate/near reach for forehand and backhand). The players were required to hit the ball over the net and land it on the opposite table like a table tennis game. This task aims to replicate the full table area covered around the table by players in a rally during competition. The time taken to complete the task is the sweep time (ST). | Reference data of ST in para-athletes:
|
| Van Biesen et al. [17] | 15 countries from 5 different continents (Europe, Africa, Australia, Asia, and South America) | Elite table tennis players with (n = 71) and without ID (n = 17).Players with ID competed in the INAS-FID World Table Tennis Championships:
| To assess the technical proficiency, the player was asked to perform 10 different sets of 10 identical strokes. Players were instructed to return services delivered by a robot to the opposite side of the table using prescribed forehand and backhand strokes:
| Reliability (inter-rater: ranging from 0.76 to 1.0; intra-rater: ranging from 0.96 to 1.0).Significant differences in technical proficiency of all types of strokes (except block) among players with and without ID (the latter performed better), but no gender differences regardless of disabilities. |
| Van Biesen et al. [18] | NR | 24 elite players with mild ID: 13 males; 11 females (MAge 25 ± 6 years, MIQ 61 ± 9).Top 16 male and female players participated in the 2009 INAS World Championships. | The technical proficiency of the table tennis players was measured in two conditions: Simulation Testing vs. Game Play. In Simulation Testing, all players underwent a standardised test battery measuring the proficiency of 10 skills. In Game Play, players were videotaped during competition, wherein a minimum of three actual play sets per player were analysed. A set is a game wherein one of the players scores 11 points against the other player with a minimal difference of two points. Videos taken during Simulation Testing and Game Play were analysed by five table tennis experts. These experts rated the forehand and backhand stroke skills using a technical observation protocol (1—the criterion was clearly observable; 0—the criterion was not observable or was incompletely executed):
| Technical proficiency during standardised Simulation Testing is positively related to proficiency during Game Play in some measures (flick, topspin–forehand, and topspin–backhand) but not all. |
| Van Biesen et al. [19] | 15 countries from 5 different continents (Europe, Africa, Australia, Asia, and South America) | Elite table tennis players with (n = 71) and without ID (n = 17).Players with ID (90% competed in the INAS World Table Tennis Championships, MPlay 13 ± 5 years):
| Participants received 12 series of five rallies against an able-bodied opponent with instructions to “try to win each rally”. There were six service variations delivered in a standardised sequence: no spin to backhand, backspin to forehand, topspin to middle, left sidespin to backhand, backspin–sidespin combination to forehand, and topspin–sidespin combination to middle. Each time a player attempted a return and subsequent rally, an expert rated the tactical proficiency (TAP) scores (0 to 2 per item):
| Inter-rater reliability (r = 0.75); intra-rater reliability (r = 0.90) among coaches.Lower proficiency scores in players with ID than those without ID.No significant correlation (r = 0.08, p > 0.05) between the total TAP and IQ scores in players with ID. |
| Van Biesen et al. [20] | NR | 88 well-trained players with ID (MAge 27.5 ± 8.4 years; MIQ 59.9 ± 9.6):
| Test 1 Received different types of services and played rallies with an experienced player with instructions to “try to win each rally”. Tactical proficiency scores (0 to 2 per item) assessed by coaches:
| Selective cognitive factors are related to tactical proficiency in table tennis among athletes with ID. Simple reaction time is the best predictor for table tennis proficiency overall. |
| Wu et al. [21] | 5 continents including 23 countries | 87 (56 males, 31 females) international players with ID (MAge 2.69 ± 8.1 years, MPlay 11.8 ± 7.3 years, MWeek10.4 ± 6.9 h). | Participants were to play using certain types of table tennis skills a few times and to try to make a consistent rally. The player’s coach demonstrates a trial and classifiers clearly explain the testing skill to the player. The main types of skills included
| Recommendation of cut-off scores to classify players:
|
| Yam et al. [23] | Singapore | 19 male table tennis athletes:
| Players to return balls delivered from a robot. They performed a total of 30 trials (3 sets of 10 consecutive drives) for forehand topspin drives and 30 trials (3 sets of 10 consecutive drives) for backhand topspin drives. Only the trials with projected balls landing diagonally on the lower half of the table within the targeted zone (0.80 m × 0.76 m) were deemed valid. Inertial measurement unit (IMU) sensors were employed to measure upper limb joint angles during forehand topspin and backhand topspin drives:
| Clear differencesin upper limb kinematics between the able-bodied and wheelchair players, especially in the elbow and wrist. Among para-players, noticeable variations in techniques were also observed between different disability classes. |
| Articles | Country/Region | Participants | Protocols | Key Findings |
|---|---|---|---|---|
| Lim et al. [24] | Singapore | 6 wheelchair para-table tennis players (sex: NR) from the National Table Tennis Team:
| Sweep area (SA)—with shoulders parallel to the table edge, the most superior position of the acromion was then used to position the player, 30 cm away from the table. The players were instructed to draw a perimeter that represented their maximal reach on a piece of paper attached to the table. The perimeter was drawn with a marker attached to their hands. The total reachable area on the table by the player is defined as sweep area (SA).Tipping angle—the players were seated and required to perform a maximal reach to the right and left side along the frontal plane to the point where each player felt that they may fall over from the side. The respective tipping angle is defined as the angle between the player’s spine from the seated position to the maximal reach position on the frontal plane. This angle was measured using Kinovea software (version 0.8.15), from videos taken from a camera placed directly behind the players while executing the reach. | Reference data for assessing the movement and ability of para-athletes:
|
| Tang et al. [25] | Singapore | Two male wheelchair para-athletes (Class 1 athlete: lack of triceps and control of muscles beneath the chest level; Class 2 athlete: operate in a motorised wheelchair). |
| Improvement in SA when using the new grip (11.7%, Class 1 athlete) and new Velcro harness with bungee cord (94%, Class 2 athlete). |
| Zembová et al. [26] | Slovakia | 24 male table tennis players (playing > 10 years, competing > 6 years).Wheelchair para-players (n = 11, MAge 36.55 ± 10.31 years):
| Trunk rotation angular kinematics were measured on a torso dynamometer. Participants were then required to complete 5 repetitions of trunk rotations to each side, in the seated position with a barbell of 1 kg placed on their shoulders behind the neck. They were instructed to perform trunk rotations with maximal effort in the acceleration phase. They had to engage their core muscles to stiffen the torso and stabilise the spine. Biomechanical variables were analysed:
| No difference between dominant and non-dominant sides (p > 0.05) for both groups.All angular kinematics during trunk rotation were significantly lower (p < 0.05) in para-table tennis players than able-bodied athletes. |
3.2. Participant Characteristics
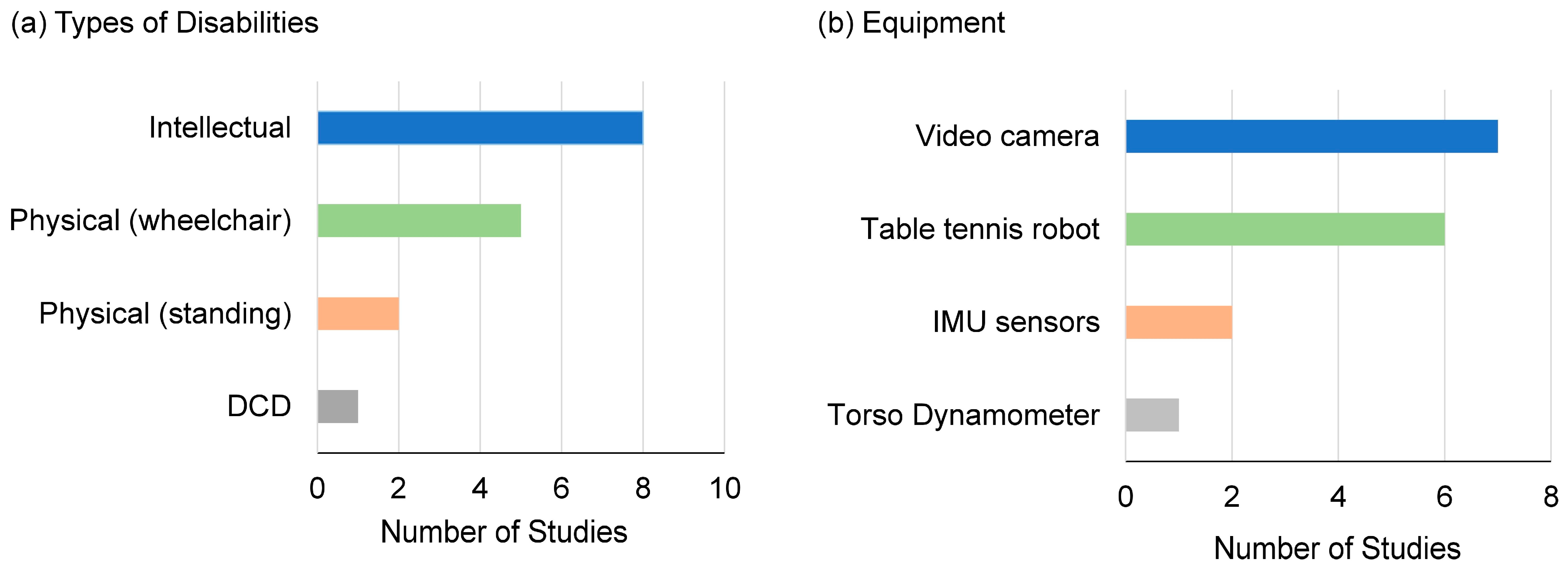
3.3. Types of Disabilities
3.4. Table Tennis-Specific Tests
4. Discussion
4.1. Table Tennis Technical Proficiency Tests
4.1.1. Accuracy
4.1.2. Skill and Control
4.1.3. Functional Reach and Trunk Rotation
4.2. Validity and Reliability
4.3. Practical Implications
4.4. Future Directions
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Krahn, G.L. WHO World report on disability: A review. Disabil. Health J. 2011, 4, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.R.; Carroll, D.D.; Workman, L.M.; Carlson, S.A.; Brown, D.W. Physical activity and health-related quality of life: US adults with and without limitations. Qual. Life Res. 2014, 23, 2673–2680. [Google Scholar] [CrossRef]
- Rinaldi, R.G.; Manin, L.; Moineau, S.; Havard, N. Table tennis ball impacting racket polymeric coatings: Experiments and modeling of key performance metrics. Appl. Sci. 2019, 9, 158. [Google Scholar] [CrossRef]
- Malagoli, L.I.; Bartolomei, S.; Di Michele, R.; Gu, Y.; Baker, J.S.; Fantozzi, S.; Cortesi, M. Kinematic analysis of the racket position during the table tennis top spin forehand stroke. Appl. Sci. 2021, 11, 5178. [Google Scholar] [CrossRef]
- Schneider, R.; Lewerentz, L.; Lüskow, K.; Marschall, M.; Kemnitz, S. Statistical analysis of table-tennis ball trajectories. Appl. Sci. 2018, 8, 2595. [Google Scholar] [CrossRef]
- Pradas, F.; de la Torre, A.; Carrasco, L.; Muñoz, D.; Courel-Ibáñez, J.; González-Jurado, J.A. Anthropometric profiles in table tennis players: Analysis of sex, age, and ranking. Appl. Sci. 2021, 11, 876. [Google Scholar] [CrossRef]
- Li, X. Biomechanical analysis of different footwork foot movements in table tennis. Comp. Intell. Neurosci. 2022, 10, 9684535. [Google Scholar] [CrossRef]
- He, Y.; Fekete, G.; Sun, D.; Baker, J.S.; Shao, S.; Gu, Y. Lower limb biomechanics during the topspin forehand in table tennis: A systemic review. Bioengineering 2022, 9, 336. [Google Scholar] [CrossRef]
- Lam, W.K.; Fan, K.X.; Zheng, Y.; Lee, W.C.C. Joint and plantar loading in table tennis topspin forehand with different footwork. Eur. J. Sport Sci. 2019, 19, 471–479. [Google Scholar] [CrossRef]
- Mao, C.; Liu, T.; Li, X.; Lu, Z.; Li, Z.; Xing, K.; Chen, L.; Sun, Y. A Comparative Biomechanical Analysis of Topspin Forehand against Topspin and Backspin in Table Tennis. Appl. Sci. 2023, 13, 8119. [Google Scholar] [CrossRef]
- Xing, K.; Hang, L.; Lu, Z.; Mao, C.; Kang, D.; Yang, C.; Sun, Y. Biomechanical comparison between down-the-line and cross-court topspin backhand in competitive table tennis. Int. J. Environ. Res. Public Health 2022, 19, 5146. [Google Scholar] [CrossRef]
- Haas, F.; Baumgartner, T.; Klein-Soetebier, T.; Seifriz, F.; Klatt, S. Heatmap analysis to differentiate diverse player types in table tennis—A training and tactical strategy development potential. Appl. Sci. 2023, 13, 1139. [Google Scholar] [CrossRef]
- Wu, C.H.; Wu, T.C.; Lin, W.B. Exploration of applying pose estimation techniques in table tennis. Appl. Sci. 2023, 13, 1896. [Google Scholar] [CrossRef]
- Faber, I.R.; Nijhuis-Van Der Sanden, M.W.; Elferink-Gemser, M.T.; Oosterveld, F.G. The Dutch motor skills assessment as tool for talent development in table tennis: A reproducibility and validity study. J. Sports Sci. 2015, 33, 1149–1158. [Google Scholar] [CrossRef]
- Faber, I.R.; Koopmann, T.; Schipper-van Veldhoven, N.; Twisk, J.; Pion, J. Can perceptuo-motor skills outcomes predict future competition participation/drop-out and competition performance in youth table tennis players? A 9-year follow-up study. PLoS ONE 2023, 10, e0281731. [Google Scholar] [CrossRef]
- Van Biesen, D.; Verellen, J.; Meyer, C.; Mactavish, J.; Van de Vliet, P.; Vanlandewijck, Y. The ability of elite table tennis players with intellectual disabilities to adapt their service/return. Adapt. Phys. Act. Q. 2010, 27, 242–257. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, D.; Mactavish, J.; Pattyn, N.; Vanlandewijck, Y.C. Technical proficiency among table tennis players with and without intellectual disabilities. Hum. Mov. Sci. 2012, 31, 1517–1528. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, D.; Mactavish, J.; Vanlandewijck, Y.C. Comparing technical proficiency of elite table tennis players with intellectual disability: Simulation testing versus game play. Percept. Mot. Skills 2014, 118, 608–621. [Google Scholar] [CrossRef]
- Van Biesen, D.; Mactavish, J.; Vanlandewijck, Y.C. Tactical proficiency among table tennis players with and without intellectual disabilities. Eur. J. Sport Sci. 2014, 14, 403–409. [Google Scholar] [CrossRef]
- Van Biesen, D.; Mactavish, J.; Kerremans, J.; Vanlandewijck, Y.C. Cognitive predictors of performance in well-trained table tennis players with intellectual disability. Adapt. Phys. Act. Q. 2016, 33, 324–337. [Google Scholar] [CrossRef]
- Wu, S.K.; Li, Y.C.; Chang, Y.C.; Wu, K.C. Analysis of the table tennis specific test in classification for players with an intellectual disability. Glob. J. Intellect. Dev. Disabil. 2021, 9, 555764. [Google Scholar] [CrossRef]
- Kong, P.W.; Yam, J.W. Shoulder biomechanics of para-table tennis: A case study of a standing class para-athlete with severe leg impairment. BMC Sports Sci. Med. Rehabil. 2022, 14, 143. [Google Scholar] [CrossRef] [PubMed]
- Yam, J.W.; Pan, J.W.; Kong, P.W. Measuring upper limb kinematics of forehand and backhand topspin drives with IMU sensors in wheelchair and able-bodied table tennis players. Sensors 2021, 21, 8303. [Google Scholar] [CrossRef]
- Lim, D.; Yap, W.B.; Tan, Z.; Li, H.; Teng, P. A case study of para table tennis athlete’s functional ability. In Proceedings of the 3rd International Congress on Sport Sciences Research and Technology Support, Lisbon, Portugal, 15–17 November 2015; Volume 1, pp. 167–173. [Google Scholar]
- Tang, S.Q.; Li, K.H.H.; Lim, S.L.D. Design enhancement of overall Paralympics wheelchair for para table tennis competition. Proceedings of the Institution of Mechanical Engineers, Part P. J. Sports Eng. Technol. 2019, 233, 342–350. [Google Scholar] [CrossRef]
- Zemková, E.; Muyor, J.M.; Jeleň, M. Association of trunk rotational velocity with spine mobility and curvatures in para table tennis players. Int. J. Sports Med. 2018, 39, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Galas, S.; Andrzejewski, M.; Pluta, B. Reliability of accuracy and precision tests for elite para table tennis players. Adapt. Phys. Act. Q. 2023, 41, 268–286. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.W.C.; Lee, W.C.C.; Lam, W.K. Biomechanics of table tennis: A systematic scoping review of playing levels and maneuvers. Appl. Sci. 2020, 10, 5203. [Google Scholar] [CrossRef]
- Saaiq, M.; Ashraf, B. Modifying “Pico” question into “Picos” model for more robust and reproducible presentation of the methodology employed in a scientific study. World J. Plast. Surg. 2017, 6, 390. [Google Scholar] [PubMed]
- Inbal, B.; Grous, E.; Grous, V. How to increase the performance in Special Olimpics table tennis players. J. Phys. Act. 2016, 5, 28–45. [Google Scholar]
- Smits-Engelsman, B.C.; Bonney, E.; Jelsma, D. Task-specificity and transfer of skills in school-aged children with and without developmental coordination disorder. Res. Dev. Disabil. 2023, 133, 104399. [Google Scholar] [CrossRef]
- Katsikadelis, M.; Pilianidis, T.; Mantzouranis, N. Test-retest reliability of the table tennis specific battery test in competitive level young players. Eur. Psychomot. J. 2014, 6, 3–13. [Google Scholar]
- Furlanetto, T.S.; Sedrez, J.A.; Candotti, C.T.; Loss, J.F. Photogrammetry as a tool for the postural evaluation of the spine: A systematic review. World J. Orthop. 2016, 7, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, S.; Imai, S.; Inaoka, H.; Masuda, T.; Ishida, A.; Okawa, A.; Shinomiya, K. The lower lumbar spine moment and the axial rotational motion of a body during one-handed and double-handed backhand stroke in tennis. Int. J. Sports Med. 2005, 26, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Khong, S.W.J.; Kong, P.W. A simple and objective method for analyzing a gymnastic skill. Eur. J. Phys. Educ. Sport 2016, 12, 46–57. [Google Scholar] [CrossRef]
- Goh, G.L.; Goh, G.D.; Pan, J.W.; Teng, P.S.P.; Kong, P.W. Automated Service Height Fault Detection Using Computer Vision and Machine Learning for Badminton Matches. Sensors 2023, 23, 9759. [Google Scholar] [CrossRef] [PubMed]
- Uhlrich, S.D.; Falisse, A.; Kidziński, Ł.; Muccini, J.; Ko, M.; Chaudhari, A.S.; Hicks, J.L.; Delp, S.L. OpenCap: Human movement dynamics from smartphone videos. PLoS Comput. Biol. 2023, 19, e1011462. [Google Scholar] [CrossRef]
- Lafayette, T.B.d.G.; Kunst, V.H.d.L.; Melo, P.V.d.S.; Guedes, P.D.O.; Teixeira, J.M.X.N.; Vasconcelos, C.R.D.; Teichrieb, V.; da Gama, A.E.F. Validation of angle estimation based on body tracking data from RGB-D and RGB cameras for biomechanical assessment. Sensors 2023, 23, 3. [Google Scholar] [CrossRef]
| Criteria | Description | |
|---|---|---|
| P | Population | Individuals with physical or intellectual disabilities; no restriction on age or sex. |
| I | Intervention | Table tennis. |
| C | Comparison | Not applicable. |
| O | Outcome | Technical proficiency of table tennis tasks. |
| S | Study Design | Any original studies. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kong, P.W.; Ma, C.M.S. Assessing Table Tennis Technical Proficiency in Individuals with Disabilities: A Scoping Review. Appl. Sci. 2024, 14, 4815. https://doi.org/10.3390/app14114815
Kong PW, Ma CMS. Assessing Table Tennis Technical Proficiency in Individuals with Disabilities: A Scoping Review. Applied Sciences. 2024; 14(11):4815. https://doi.org/10.3390/app14114815
Chicago/Turabian StyleKong, Pui Wah, and Cecilia Man Sze Ma. 2024. "Assessing Table Tennis Technical Proficiency in Individuals with Disabilities: A Scoping Review" Applied Sciences 14, no. 11: 4815. https://doi.org/10.3390/app14114815
APA StyleKong, P. W., & Ma, C. M. S. (2024). Assessing Table Tennis Technical Proficiency in Individuals with Disabilities: A Scoping Review. Applied Sciences, 14(11), 4815. https://doi.org/10.3390/app14114815