

Current Concepts about Calcaneal Fracture Management: A Review of Metanalysis and Systematic Reviews

 ,
,  ,
,  , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
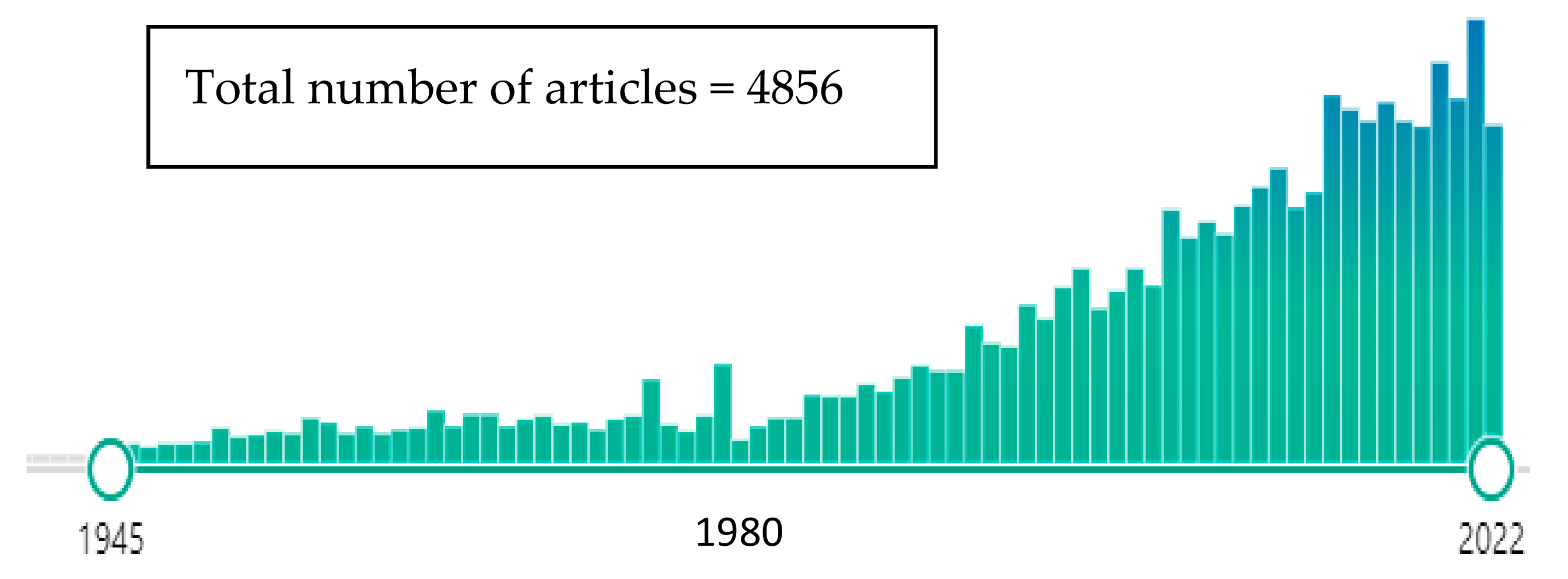
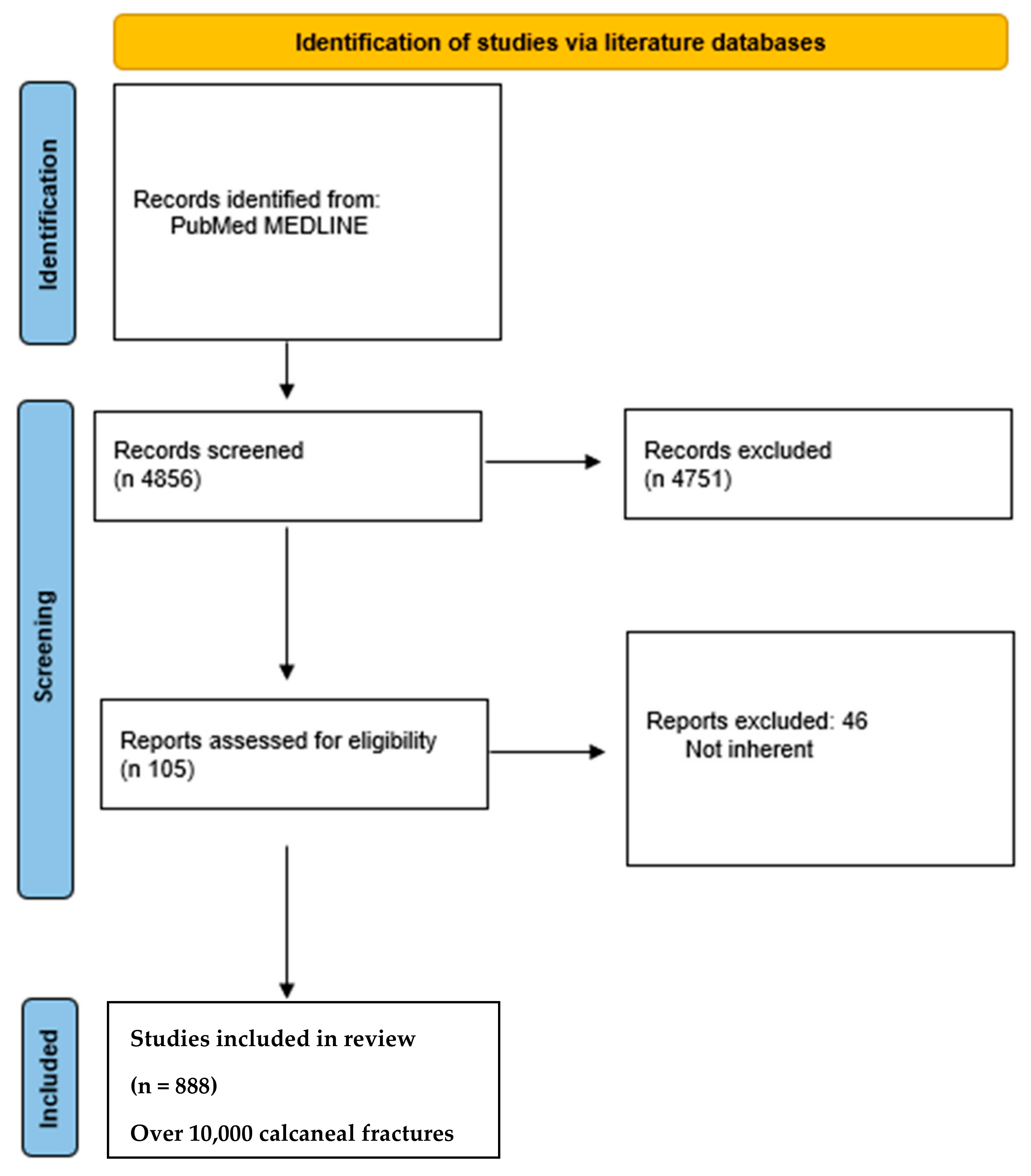
3.1. Articles Selection and Data Extraction
3.2. Surgical Approaches
3.3. Surgery vs. Conservative Treatment
3.4. Complications
3.5. Arthroscopy
3.6. ORIF vs. Arthrodesis
3.7. 3D Printing
3.8. Percutaneous Screws vs. ORIF
3.9. Fracture Dislocation and Timing
3.10. Various Treatments
3.11. Pedobarography
3.12. Circular External Fixator
3.13. Open Fractures
3.14. Bone Graft
3.15. Percutaneous Osteosynthesis vs. ORIF
3.16. Peroneal Tendon Instability
3.17. Weight-Bearing Timing
3.18. Cadaver Osteosynthesis
3.19. Percutaneous Osteosynthesis
3.20. Calcium Phosphate vs. Bone Graft
3.21. Primary Arthrodesis
4. Discussion
4.1. Surgery vs. Conservative Treatment
4.2. Complications
4.3. Surgical Approach
4.4. Arthroscopy
4.5. 3D Printing
4.6. ORIF vs. Arthrodesis
4.7. Cannulated Screws vs. ORIF
4.8. Resorbable Metal Osteosynthesis
4.9. Peroneal Tendons Instability
4.10. STA vs. MIS
4.11. Plates
4.12. ORIF vs. Percutaneous Treatment
4.13. Intra-Operative Computed Tomography (CT) Scan
4.14. Pedobarography
4.15. Circular External Fixation
4.16. Bone Grafts
4.17. Electromagnetic Fields
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, F.; Tian, H.; Li, S.; Liu, B.; Dong, T.; Zhu, Y.; Zhang, Y. Meta-analysis of two surgical approaches for calcaneal fractures: Sinus tarsi versus extensile lateral approach. ANZ J. Surg. 2017, 87, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Schepers, T. The sinus tarsi approach in displaced intra-articular calcaneal fractures: A systematic review. Int. Orthop. 2011, 35, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Yuan, B.; Guo, W.; Li, N.; Tian, H. Extensile lateral versus sinus tarsi approach for calcaneal fractures: A meta-analysis. Medicine 2021, 100, e26717. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Huang, L.; Liu, B.; Liu, Z.; Xu, X.; Liu, J.; Chu, T.; Pan, L. Efficacy of Sinus Tarsal Approach Compared with Conventional L-Shaped Lateral Approach in the Treatment of Calcaneal Fractures: A Meta-Analysis. Front. Surg. 2020, 7, 602053. [Google Scholar] [CrossRef]
- Lv, Y.; Zhou, Y.F.; Li, L.; Yu, Z.; Wang, Q.; Sun, Y.Y.; Zhou, D.S. Sinus tarsi approach versus the extended lateral approach for displaced intra-articular calcaneal fractures: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2021, 141, 1659–1667. [Google Scholar] [CrossRef]
- Seat, A.; Seat, C. Lateral Extensile Approach Versus Minimal Incision Approach for Open Reduction and Internal Fixation of Displaced Intra-articular Calcaneal Fractures: A Meta-analysis. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2020, 59, 356–366. [Google Scholar] [CrossRef]
- Ieropoli, G.; Villafane, J.H.; Zompi, S.C.; Morozzo, U.; D’Ambrosi, R.; Usuelli, F.G.; Berjano, P. Successful treatment of infected wound dehiscence after minimally invasive locking-plate osteosynthesis of tibial pilon and calcaneal fractures by plate preservation, surgical debridement and antibiotics. Foot 2017, 33, 44–47. [Google Scholar] [CrossRef]
- Indino, C.; Villafane, J.H.; D’Ambrosi, R.; Manzi, L.; Maccario, C.; Berjano, P.; Usuelli, F.G. Effectiveness of subtalar arthroereisis with endorthesis for pediatric flexible flat foot: A retrospective cross-sectional study with final follow up at skeletal maturity. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2020, 26, 98–104. [Google Scholar] [CrossRef]
- Fan, B.; Zhou, X.; Wei, Z.; Ren, Y.; Lin, W.; Hao, Y.; Shi, G.; Feng, S. Cannulated screw fixation and plate fixation for displaced intra-articular calcaneus fracture: A meta-analysis of randomized controlled trials. Int. J. Surg. 2016, 34, 64–72. [Google Scholar] [CrossRef]
- Zeng, Z.; Yuan, L.; Zheng, S.; Sun, Y.; Huang, F. Minimally invasive versus extensile lateral approach for sanders type II and III calcaneal fractures: A meta-analysis of randomized controlled trials. Int. J. Surg. 2018, 50, 146–153. [Google Scholar] [CrossRef]
- Selim, A.; Ponugoti, N.; Chandrashekar, S. Systematic Review of Operative vs Nonoperative Treatment of Displaced Intraarticular Calcaneal Fractures. Foot Ankle Orthop. 2022, 7, 24730114221101609. [Google Scholar] [CrossRef] [PubMed]
- Meena, S.; Hooda, A.; Sharma, P.; Mittal, S.; Sharma, J.; Chowdhury, B. Operative versus Non operative treatment of displaced intraarticular fracture of calcaneum: A meta-analysis of randomized controlled trials. Acta Orthop. Belg. 2017, 83, 161–169. [Google Scholar] [PubMed]
- Zhang, C.; Ye, Z.M.; Lin, P.; Miao, X.D. Lateral Fracture-Dislocation of the Calcaneus: Case Reports and a Systematic Review. Orthop. Surg. 2021, 13, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Barini, M.; Zagaria, D.; Licandro, D.; Pansini, S.; Airoldi, C.; Leigheb, M.; Carriero, A. Magnetic Resonance Accuracy in the Diagnosis of Anterior Talo-Fibular Ligament Acute Injury: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 1782. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 state-ment: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, H.; Zhou, J.; Yu, G. Treatment of displaced intraarticular calcaneal fractures with or without bone grafts: A systematic review of the literature. Indian J. Orthop. 2012, 46, 130–137. [Google Scholar] [CrossRef]
- Yao, H.; Liang, T.; Xu, Y.; Hou, G.; Lv, L.; Zhang, J. Sinus tarsi approach versus extensile lateral approach for displaced intra-articular calcaneal fracture: A meta-analysis of current evidence base. J. Orthop. Surg. Res. 2017, 12, 43. [Google Scholar] [CrossRef]
- Yu, T.; Xiong, Y.; Kang, A.; Zhou, H.; He, W.; Zhu, H.; Yang, Y. Comparison of sinus tarsi approach and extensile lateral approach for calcaneal fractures: A systematic review of overlapping meta-analyses. J. Orthop. Surg. 2020, 28, 2309499020915282. [Google Scholar] [CrossRef]
- Nosewicz, T.L.; Dingemans, S.A.; Backes, M.; Luitse, J.S.K.; Goslings, J.C.; Schepers, T. A systematic review and meta-analysis of the sinus tarsi and extended lateral approach in the operative treatment of displaced intra-articular calcaneal fractures. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2019, 25, 580–588. [Google Scholar] [CrossRef]
- Wu, M.H.; Sun, W.C.; Yan, F.F.; Hou, Z.Q.; Feng, F.; Cai, L. Minimally invasive sinus tarsal approach versus conventional L-shaped lateral approach in treating calcaneal fractures: A Meta-analysis. Zhongguo Gu Shang China J. Orthop. Traumatol. 2017, 30, 1118–1126. [Google Scholar]
- Bai, L.; Hou, Y.L.; Lin, G.H.; Zhang, X.; Liu, G.Q.; Yu, B. Sinus tarsi approach (STA) versus extensile lateral approach (ELA) for treatment of closed displaced intra-articular calcaneal fractures (DIACF): A meta-analysis. Orthop. Traumatol. Surg. Res. OTSR 2018, 104, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Meena, S.; Gangary, S.K.; Sharma, P. Review Article: Operative versus nonoperative treatment for displaced intraarticular calcaneal fracture: A meta-analysis of randomised controlled trials. J. Orthop. Surg. 2016, 24, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Lin, Q.R.; Diao, X.C.; Wu, L.; Yu, B. Surgical versus nonsurgical treatment of displaced intra-articular calcaneal fracture: A meta-analysis of current evidence base. Int. Orthop. 2012, 36, 1615–1622. [Google Scholar] [CrossRef]
- Griffin, D.; Parsons, N.; Shaw, E.; Kulikov, Y.; Hutchinson, C.; Thorogood, M.; Lamb, S.E.; Investigators UKHFT. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: Randomised controlled trial. BMJ 2014, 349, g4483. [Google Scholar] [CrossRef]
- Luo, X.; Li, Q.; He, S.; He, S. Operative Versus Nonoperative Treatment for Displaced Intra-Articular Calcaneal Fractures: A Meta-Analysis of Randomized Controlled Trials. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2016, 55, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Lin, F.; Chen, E.; Xue, D.; Pan, Z. Operative Versus Nonoperative Treatment of Displaced Intra-Articular Calcaneal Fractures: A Meta-Analysis of Randomized Controlled Trials. J. Orthop. Trauma 2016, 30, e75–e81. [Google Scholar] [CrossRef] [PubMed]
- Bruce, J.; Sutherland, A. Surgical versus conservative interventions for displaced intra-articular calcaneal fractures. Cochrane Database Syst. Rev. 2013, 1, CD008628. [Google Scholar] [CrossRef] [PubMed]
- Randle, J.A.; Kreder, H.J.; Stephen, D.; Williams, J.; Jaglal, S.; Hu, R. Should calcaneal fractures be treated surgically? A meta-analysis. Clin. Orthop. Relat. Res. 2000, 377, 217–227. [Google Scholar] [CrossRef]
- Wei, N.; Yuwen, P.; Liu, W.; Zhu, Y.; Chang, W.; Feng, C.; Chen, W. Operative versus nonoperative treatment of displaced intra-articular calcaneal fractures: A meta-analysis of current evidence base. Medicine 2017, 96, e9027. [Google Scholar] [CrossRef]
- Liu, Y.; Li, Z.; Li, H.; Zhang, Y.; Wang, P. Protective Effect of Surgery Against Early Subtalar Arthrodesis in Displaced Intra-articular Calcaneal Fractures: A Meta-Analysis. Medicine 2015, 94, e1984-0. [Google Scholar] [CrossRef]
- Backes, M.; Spierings, K.E.; Dingemans, S.A.; Goslings, J.C.; Buckley, R.E.; Schepers, T. Evaluation and quantification of geographical differences in wound complication rates following the extended lateral approach in displaced intra-articular calcaneal fractures—A systematic review of the literature. Injury 2017, 48, 2329–2335. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Chen, E.; Xue, D.; Yin, H.; Pan, Z. Risk factors for wound complications of closed calcaneal fractures after surgery: A systematic review and meta-analysis. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Su, P.; Li, J. Complications in the Management of Displaced Intra-articular Calcaneal Fractures: A Systematic Review and Network Meta-Analysis of 2538 Patients. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2022, 61, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Halvachizadeh, S.; Klingebiel, F.K.L.; Pfeifer, R.; Gosteli, M.; Schuerle, S.; Cinelli, P.; Zelle, B.A.; Pape, H.C. The local soft tissue status and the prediction of local complications following fractures of the ankle region. Injury 2022, 53, 1789–1795. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.E.; Joo, P.; Oh, I.; Miller, C.; Kwon, J.Y. Arthroscopically Assisted Internal Fixation of Foot and Ankle Fractures: A Systematic Review. Foot Ankle Orthop. 2021, 6, 2473011420950214. [Google Scholar] [CrossRef] [PubMed]
- Marouby, S.; Cellier, N.; Mares, O.; Kouyoumdjian, P.; Coulomb, R. Percutaneous arthroscopic calcaneal osteosynthesis for displaced intra-articular calcaneal fractures: Systematic review and surgical technique. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2020, 26, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.F.; Vale, C.; Gonzalez, T.; Gomes, T.M.; Oliva, X.M. Osteosynthesis or primary arthrodesis for displaced intra-articular calcaneus fractures Sanders type IV—A systematic review. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2022, 28, 281–287. [Google Scholar] [CrossRef]
- Shi, G.; Liu, W.; Shen, Y.; Cai, X. 3D printing-assisted extended lateral approach for displaced intra-articular calcaneal fractures: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 682. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, N.; Guo, W.; Wang, W.; Zhang, Q. Cannulated screw fixation versus plate fixation in treating displaced intra-articular calcaneus fractures: A systematic review and meta-analysis. Int. Orthop. 2021, 45, 2411–2421. [Google Scholar] [CrossRef]
- Gougoulias, N.; Khanna, A.; McBride, D.J.; Maffulli, N. Management of calcaneal fractures: Systematic review of randomized trials. Br. Med. Bull. 2009, 92, 153–167. [Google Scholar] [CrossRef]
- Bridgman, S.; Dunn, K.; McBride, D.; Richards, P. WITHDRAWN: Interventions for treating calcaneal fractures. Cochrane Database Syst. Rev. 2008, 4, CD001161. [Google Scholar] [CrossRef]
- Wallin, K.J.; Cozzetto, D.; Russell, L.; Hallare, D.A.; Lee, D.K. Evidence-based rationale for percutaneous fixation technique of displaced intra-articular calcaneal fractures: A systematic review of clinical outcomes. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2014, 53, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Veltman, E.S.; Doornberg, J.N.; Stufkens, S.A.; Luitse, J.S.; van den Bekerom, M.P. Long-term outcomes of 1730 calcaneal fractures: Systematic review of the literature. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2013, 52, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Pelliccioni, A.A.; Bittar, C.K.; Zabeu, J.L. Surgical treatment of intraarticular calcaneous fractures of sanders’ types II and III. Systematic review. Acta Ortop. Bras. 2012, 20, 39–42. [Google Scholar] [CrossRef]
- Shi, F.; Wu, S.; Cai, W.; Zhao, Y. Comparison of 5 Treatment Approaches for Displaced Intra-articular Calcaneal Fractures: A Systematic Review and Bayesian Network Meta-Analysis. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2020, 59, 1254–1264. [Google Scholar] [CrossRef]
- Sanders, F.R.K.; Peters, J.J.; Schallig, W.; Mittlmeier, T.; Schepers, T. What is the added value of pedobarography for assessing functional outcome of displaced intra-articular calcaneal fractures? A systematic review of existing literature. Clin. Biomech. 2020, 72, 8–15. [Google Scholar] [CrossRef]
- Muir, R.L.; Forrester, R.; Sharma, H. Fine Wire Circular Fixation for Displaced Intra-Articular Calcaneal Fractures: A Systematic Review. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2019, 58, 755–761. [Google Scholar] [CrossRef]
- Spierings, K.E.; Min, M.; Nooijen, L.E.; Swords, M.P.; Schepers, T. Managing the open calcaneal fracture: A systematic review. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2019, 25, 707–713. [Google Scholar] [CrossRef]
- Zheng, W.; Xie, L.; Xie, H.; Chen, C.; Chen, H.; Cai, L. With versus without bone grafts for operative treatment of displaced intra-articular calcaneal fractures: A meta-analysis. Int. J. Surg. 2018, 59, 36–47. [Google Scholar] [CrossRef]
- Wang, X.J.; Su, Y.X.; Li, L.; Zhang, Z.H.; Wei, X.C.; Wei, L. Percutaneous poking reduction and fixation versus open reduction and fixation in the treatment of displaced calcaneal fractures for Chinese patients: A systematic review and meta-analysis. Chin. J. Traumatol. Zhonghua Chuang Shang Za Zhi 2016, 19, 362–367. [Google Scholar] [CrossRef]
- Wu, J.; Zhou, F.; Yang, L.; Tan, J. Percutaneous Reduction and Fixation with Kirschner Wires versus Open Reduction Internal Fixation for the Management of Calcaneal Fractures: A Meta-Analysis. Sci. Rep. 2016, 6, 30480. [Google Scholar] [CrossRef] [PubMed]
- Majeed, H.; Barrie, J.; Munro, W.; McBride, D. Minimally invasive reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular calcaneal fractures: A systematic review of the literature. EFORT Open Rev. 2018, 3, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, K.; Mekhaimar, M.M.; Alhammoud, A. Prevalence of Peroneal Tendon Instability in Calcaneus Fractures: A Systematic Review and Meta-Analysis. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2018, 57, 572–578. [Google Scholar] [CrossRef] [PubMed]
- De Boer, A.S.; Van Lieshout, E.M.M.; Van Moolenbroek, G.; Den Hartog, D.; Verhofstad, M.H.J. The effect of time to post-operative weightbearing on functional and clinical outcomes in adults with a displaced intra-articular calcaneal fracture; A systematic review and pooled analysis. Injury 2018, 49, 743–752. [Google Scholar] [CrossRef]
- Dingemans, S.A.; Sintenie, F.W.; de Jong, V.M.; Luitse, J.S.K.; Schepers, T. Fixation Methods for Calcaneus Fractures: A Systematic Review of Biomechanical Studies Using Cadaver Specimens. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2018, 57, 116–122. [Google Scholar] [CrossRef]
- Van Hoeve, S.; Poeze, M. Outcome of Minimally Invasive Open and Percutaneous Techniques for Repair of Calcaneal Fractures: A Systematic Review. J. Foot Ankle Surg. Off. Publ. Am. Coll. Foot Ankle Surg. 2016, 55, 1256–1263. [Google Scholar] [CrossRef]
- Bajammal, S.S.; Zlowodzki, M.; Lelwica, A.; Tornetta, P., 3rd; Einhorn, T.A.; Buckley, R.; Leighton, R.; Russell, T.A.; Larsson, S.; Bhandari, M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J. Bone Jt. Surg. Am. Vol. 2008, 90, 1186–1196. [Google Scholar] [CrossRef]
- Schepers, T. The primary arthrodesis for severely comminuted intra-articular fractures of the calcaneus: A systematic review. Foot Ankle Surg. Off. J. Eur. Soc. Foot Ankle Surg. 2012, 18, 84–88. [Google Scholar] [CrossRef]
- Schepers, T. The subtalar distraction bone block arthrodesis following the late complications of calcaneal fractures: A systematic review. Foot 2013, 23, 39–44. [Google Scholar] [CrossRef]
- Leigheb, M. Wrist traumatology in the 2020s. Minerva Orthop. 2021, 72, 93–94. [Google Scholar] [CrossRef]
- Leigheb, M.; Janicka, P.; Andorno, S.; Marcuzzi, A.; Magnani, C.; Grassi, F. Italian translation, cultural adaptation and validation of the “American Orthopaedic Foot and Ankle Society’s (AOFAS) ankle-hindfoot scale”. Acta Bio-Medica Atenei Parm. 2016, 87, 38–45. [Google Scholar]
- Leigheb, M.; Massa, M.; Bosetti, M.; Nico, P.; Tarallo, L.; Pogliacomi, F.; Grassi, F.A. Autologous Platelet Rich Plasma (PRP) in the treatment of elbow epicondylitis and plantar fasciitis: Medium to long term clinical outcome. Acta Bio-Medica Atenei Parm. 2020, 91, e2020029. [Google Scholar]
- Leigheb, M.; Rusconi, M.; De Consoli, A.; Fredo, M.; Rimondini, L.; Cochis, A.; Pogliacomi, F.; Grassi, F.A. Arthroscopically-assisted Reduction and Internal Fixation (ARIF) of tibial plateau fractures: Clinical and radiographic medium-term follow-up. Acta Bio-Medica Atenei Parm. 2020, 91, 152–159. [Google Scholar]
- Villafane, J.H.; Valdes, K.; Pedersini, P.; Berjano, P. Osteoarthritis: A call for research on central pain mechanism and personalized prevention strategies. Clin. Rheumatol. 2019, 38, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Caruso, I.; Leonardini, A.; Caizzi, G.; Vicenti, G.; Caporusso, M.; Guarini, F.; Bernardis, M.; Moretti, B.; Giorgino, F. Diabetic foot: Clinical ap-proach. Minerva Orthop. 2022, 73, 63–75. [Google Scholar] [CrossRef]
- Buda, R.; Bruni, D.; Pantalone, A. Current concepts in the treatment of ankle osteoarthritis. Minerva Orthop. 2021, 72, 539–540. [Google Scholar] [CrossRef]
- Wang, H.; Pei, H.; Chen, M.; Wang, H. Incidence and predictors of surgical site infection after ORIF in calcaneus fractures, a retrospective cohort study. J. Orthop. Surg. Res. 2018, 13, 293. [Google Scholar] [CrossRef]
- Cochis, A.; Bonetti, L.; Sorrentino, R.; Contessi Negrini, N.; Grassi, F.; Leigheb, M.; Rimondini, L.; Fare, S. 3D Printing of Thermo-Responsive Methylcellulose Hydrogels for Cell-Sheet Engineering. Materials 2018, 11, 579. [Google Scholar] [CrossRef]
- Parchi, P. 3D printing in orthopedic surgery. Minerva Orthop. 2021, 72, 347–348. [Google Scholar] [CrossRef]
- Aprato, A.; Giudice, C. 3D printing in pediatrics orthopedics. Minerva Orthop. 2022, 73, 551–553. [Google Scholar] [CrossRef]
- Bonatti, A.F.; Chiesa, I.; Micalizzi, S.; Vozzi, G.; De Maria, C. Bioprinting for bone tissue engineering. Minerva Orthop. 2021, 72, 376–394. [Google Scholar] [CrossRef]
- Leigheb, M.; Veneziano, M.; Tortia, R.; Bosetti, M.; Cochis, A.; Rimondini, L.; Grassi, F.A. Osteosynthesis devices in absorbable Magnesium alloy in comparison to standard ones: A Systematic Review on effectiveness and safety. Acta Bio-Medica Atenei Parm. 2021, 92, e2021025. [Google Scholar]
- Bosetti, M.; Borrone, A.; Leigheb, M.; Shastri, V.P.; Cannas, M. Injectable Graft Substitute Active on Bone Tissue Regeneration. Tissue Eng. Part A 2017, 23, 1413–1422. [Google Scholar] [CrossRef] [PubMed]
- Vicenti, G.; Ottaviani, G.; Bizzoca, D.; Carrozzo, M.; Simone, F.; Grosso, A.; Zavattini, G.; Elia, R.; MAuruccia, M.; SOlarino, G.; et al. The manage-ment of post-traumatic bone defects: A systematic review. Minerva Orthop. 2022, 73, 10–19. [Google Scholar] [CrossRef]
- Waldorff, E.I.; Markov, M.S. Magnetic and electromagnetic field in therapeutic application for bone stimulation. Minerva Orthop. 2022, 73, 73–74. [Google Scholar] [CrossRef]
- Mazzotti, A.; Langone, L.; Artioli, E.; Zielli, S.O.; Arceri, A.; Setti, S.; Leigheb, M.; Samaila, E.M.; Faldini, C. Applications and Future Perspective of Pulsed Electromagnetic Fields in Foot and Ankle Sport-Related Injuries. Appl. Sci. 2023, 13, 5807. [Google Scholar] [CrossRef]
- Schepers, T.; Heetveld, M.J.; Mulder, P.G.; Patka, P. Clinical outcome scoring of intra-articular calcaneal fractures. J. Foot Ankle Surg. 2008, 47, 213–218. [Google Scholar] [CrossRef][Green Version]




{kind=link}
{kind=link}
{kind=link}
| TOPIC | N Metanalyses and/or Systematic Reviews | N Articles Compared | Results |
|---|---|---|---|
| STA vs. ELA [1,2,3,4,5,6,10,16,17,18,19,20,21] | 13 | 8 8 7 8 X 12 15 5 27 9 8 7 8 | STA > ELA 9 STA = ELA 4 |
| Conservative treatment vs. surgical treatment [11,12,22,23,24,25,26,27,28,29,30] | 11 | 8 10 18 8 7 4 7 7 13 8 18 4 | Conservative treatment < surgical treatment 11 Conservative treatment = surgical treatment 1 |
| Complications and soft tissues [31,32,33,34] | 4 | 123 10 26 34 | ELA experienced the most frequent complications PA better results The state of the overlying tissues is the + important predictor No difference between POWI and POWC in the countries |
| ARIF vs. AREF [35,36] | 2 | 32 8 | ARIF = others treatments ARIF > into diagnosyis |
| ORIF vs arthrodesis [36,37] | 2 | 14 9 | ORIF > arthrodesis in Sanders type II/III ORIF = arthrodesis in Sanders type IV |
| 3D-printed-assisted [38] | 1 | 9 | “Excellent and good outcome, shorter operation time, less intraoperative blood loss, fewer intraoperative fluoroscopies, fewer complications”. |
| Cannulated screws vs. ORIF [9,39] | 2 | 5 7 | Same functional results Screw > ORIF for complications, quality of reduction, surgical timing |
| Dislocated fractures [13] | 1 | 4 | “Timely surgical intervention is essential for satisfactory clinic outcomes”. |
| Outcomes between treatments [13,40,41,42,43,44,45] | 6 | 4 7 25 3 2 17 | “Platelet-rich fibrin (PRF) (87.0%), MILA (52.9%), STA (46.6%), ELA (40.4%), nonoperative (23.1%). In terms of excellent and good satisfaction ratings, the treatments were ranked as follows: STA (96.2%), ELA (66.8%), PRF (34.9%), and nonoperative (2%). In terms of incision complications, the treatments were ranked as follows: PRF (84.1%), MILA (80.0%), STA (35.8%), and ELA (0.1%)”. “Results showed no difference in residual pain, but favoured surgical management on ability to return to the same work and to wear the same shoes as before the fracture”. “Displaced calcaneal fractures are treated surgically from 1 level I evidence study, 1 level II, and multiple studies with less than level II evidence, with open reduction and internal fixation as the method of choice. If the fracture is less complex, percutaneous treatment can be a good alternative according to current level 3 and 4 retrospective data”. “The results from the current data appear to be promising; however, the lack of statistical power and inconsistent documentation have made it difficult to determine any superiority. The complication rates were much lower than those with open procedures, regardless of the technique. The percutaneous fixation technique appears to be a favorable option for displaced intra-articular calcaneal fractures. Percutaneous fixation using Kirschner wires presented the best results, however, evidence is insufficient to assert superiority of this treatment in comparison with other surgical techniques. Sanders II/III” |
| Pedobarography for outcomes [46] | 1 | 9 | “As a prediction tool, it should be more standardised. may be useful in developing customized aids such as insoles, aiming for a more individualized improvement”. |
| Circular external fixator [47] | 1 | 11 | “Pin site infections were common (22.6%), serious complications, including deep infection (0.8%), wound infection (1.6%), and complex regional pain syndrome (0.8%), were exceedingly rare”. |
| Open fractures [48] | 1 | 18 | The degree of exposure affects the result, especially on the wound healing time |
| Bone plug [15,49] | 2 | 32 9 | “Bone grafts achieved better AOFAS scores than the non-bone graft group. The two groups had similar results in Böhler angle, Gissane angle, calcaneal width, and calcaneal height. No increased risk of postoperative complications was identified”. |
| Percutaneous osteosynthesis vs. ORIF [50,51,52] | 3 | 15 18 9 | No differences in functional scores ORIF < in wound complications |
| Peroneal tendons instability [53] | 1 | 9 | “Prevalence of peroneal tendon instability is associated with intraarticular calcaneal fractures and increases with the severity of the fracture”. |
| Timing of load-bearing [54] | 1 | 72 | “The adverse sequelae which are assumed to be associated with starting partial weightbearing already within six weeks after internal fixation of calcaneal fractures, is not supported by literature data”. |
| Osteosintesys on cadaver [55] | 1 | 14 | “None of the studies found a significant difference in favor of any of the fixation methods”. |
| Percutaneal osteosintesys [56] | 1 | 46 | “Best outcomes for the minimal invasive open surgical treatment of calcaneal fractures” |
| Cementation with calcium phosphate [57] | 1 | 14 | “Lower prevalence of pain at the fracture site”; loss of fracture reduction |
| Arthrodesis in Sanders type IV [58,59] | 2 | 7 22 | “Good results considering the severe nature of the injury”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leigheb, M.; Codori, F.; Samaila, E.M.; Mazzotti, A.; Villafañe, J.H.; Bosetti, M.; Ceccarini, P.; Cochis, A.; Daou, F.; Ronga, M.; et al. Current Concepts about Calcaneal Fracture Management: A Review of Metanalysis and Systematic Reviews. Appl. Sci. 2023, 13, 12311. https://doi.org/10.3390/app132212311
Leigheb M, Codori F, Samaila EM, Mazzotti A, Villafañe JH, Bosetti M, Ceccarini P, Cochis A, Daou F, Ronga M, et al. Current Concepts about Calcaneal Fracture Management: A Review of Metanalysis and Systematic Reviews. Applied Sciences. 2023; 13(22):12311. https://doi.org/10.3390/app132212311
Chicago/Turabian StyleLeigheb, Massimiliano, Francesco Codori, Elena Manuela Samaila, Antonio Mazzotti, Jorge Hugo Villafañe, Michela Bosetti, Paolo Ceccarini, Andrea Cochis, Farah Daou, Mario Ronga, and et al. 2023. "Current Concepts about Calcaneal Fracture Management: A Review of Metanalysis and Systematic Reviews" Applied Sciences 13, no. 22: 12311. https://doi.org/10.3390/app132212311
APA StyleLeigheb, M., Codori, F., Samaila, E. M., Mazzotti, A., Villafañe, J. H., Bosetti, M., Ceccarini, P., Cochis, A., Daou, F., Ronga, M., Grassi, F. A., & Rimondini, L. (2023). Current Concepts about Calcaneal Fracture Management: A Review of Metanalysis and Systematic Reviews. Applied Sciences, 13(22), 12311. https://doi.org/10.3390/app132212311