



Incidence of Carpal Tunnel Syndrome and Other Coexisting Brachial Plexus Neuropathies in Bullseye Shooters—A Pilot Retrospective Clinical and Neurophysiological Assessment

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
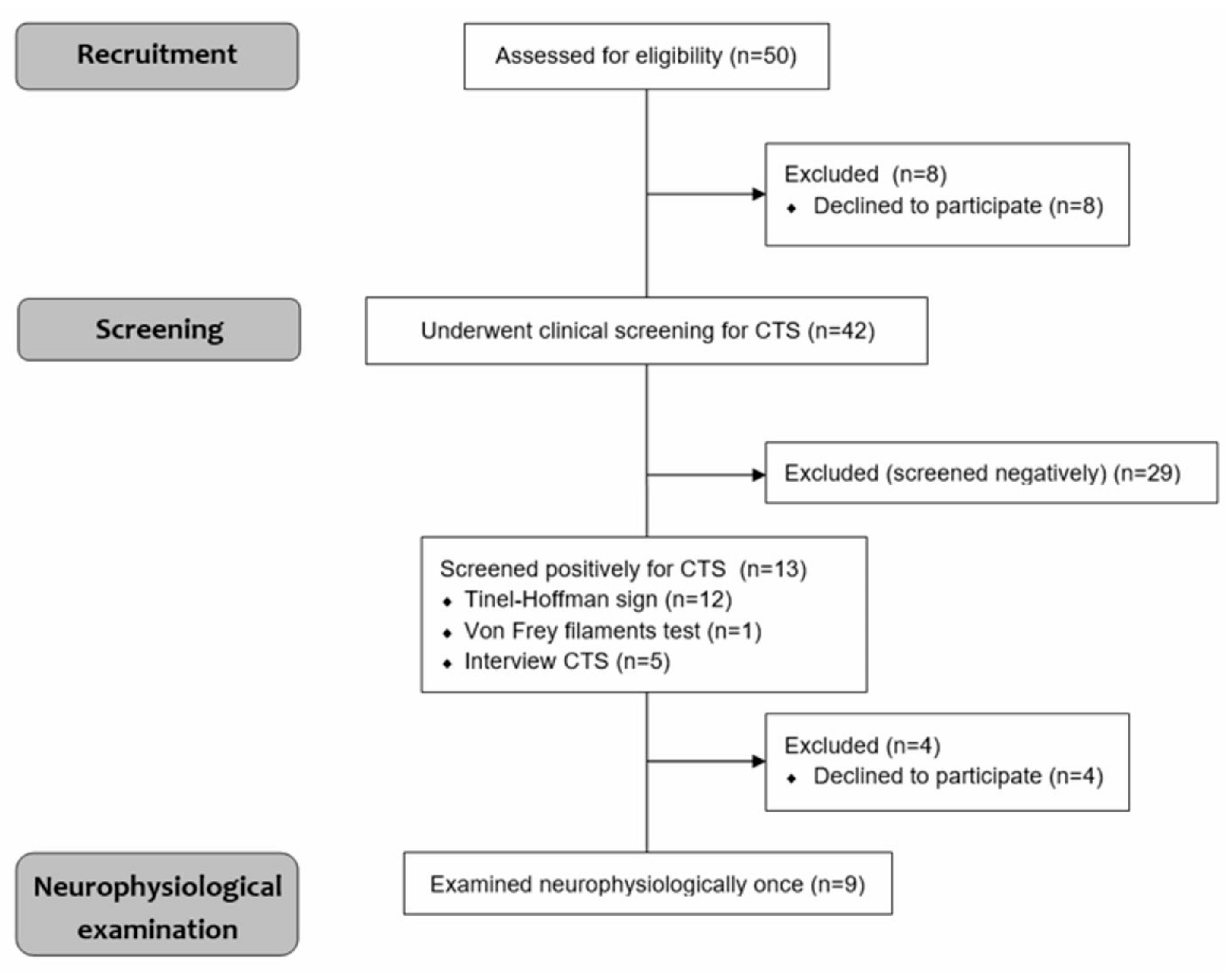
2.1. Participants and Study Design
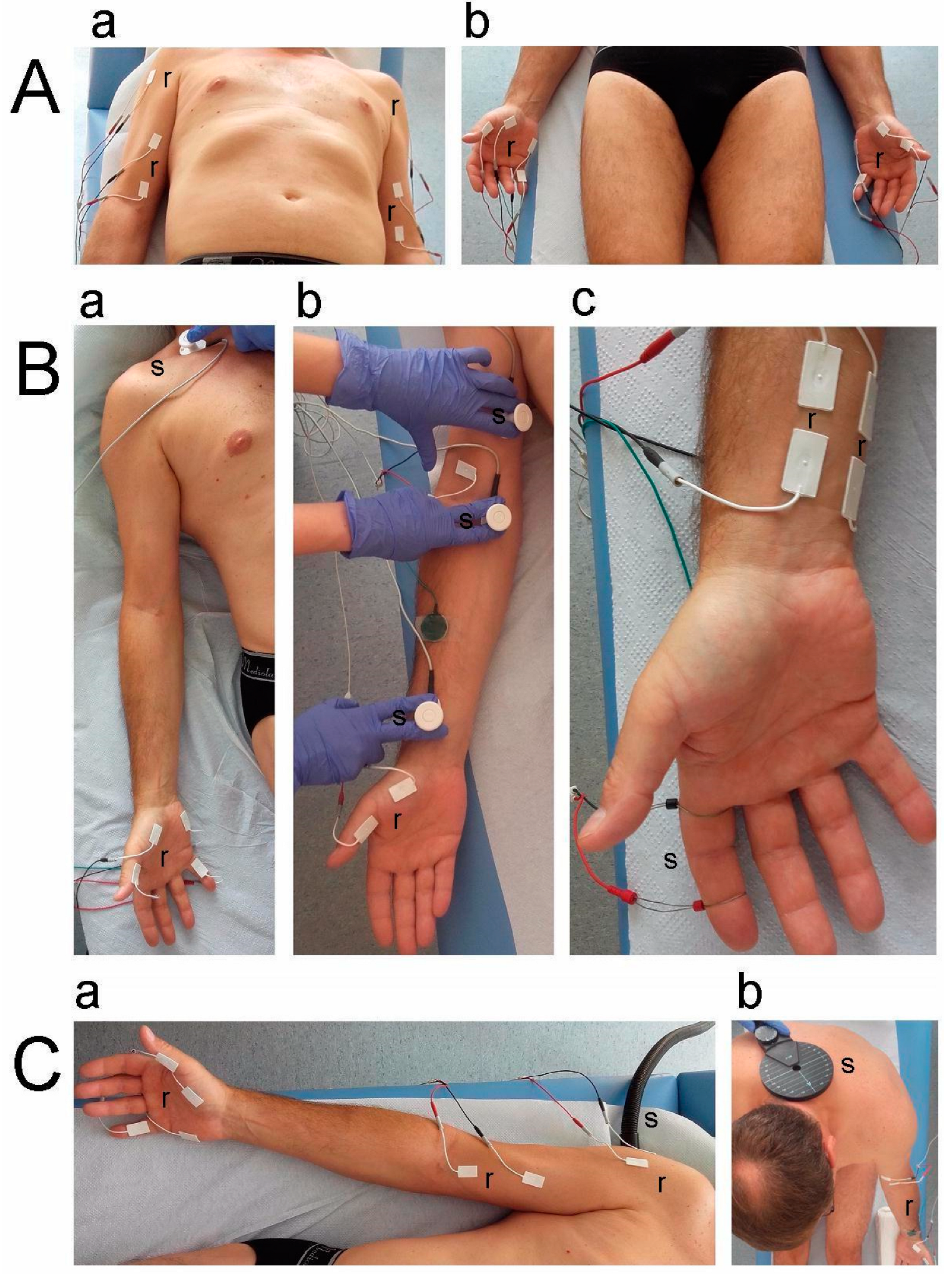
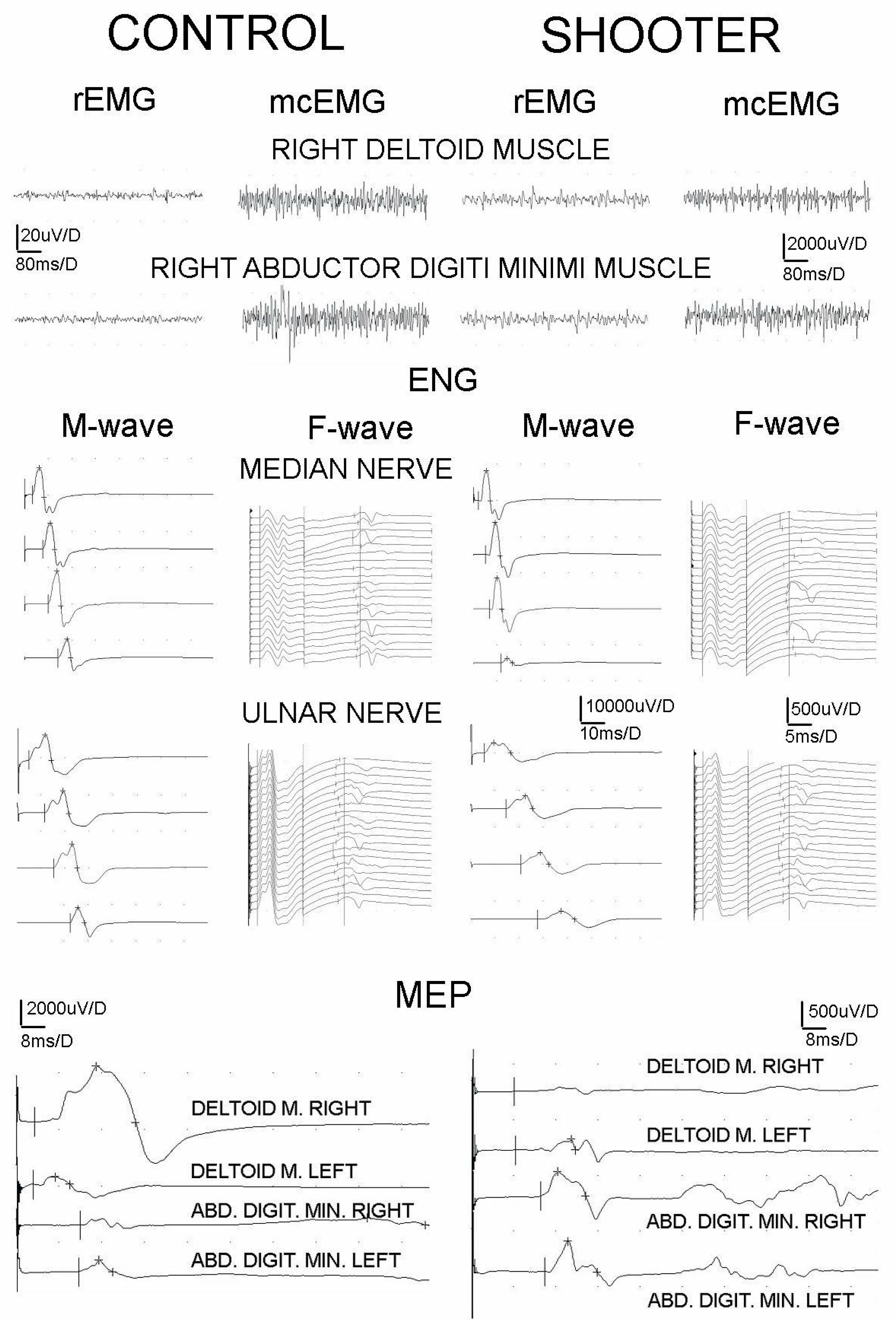
2.2. Neurophysiological Testing
2.3. Statistical Analysis
3. Results
4. Discussion
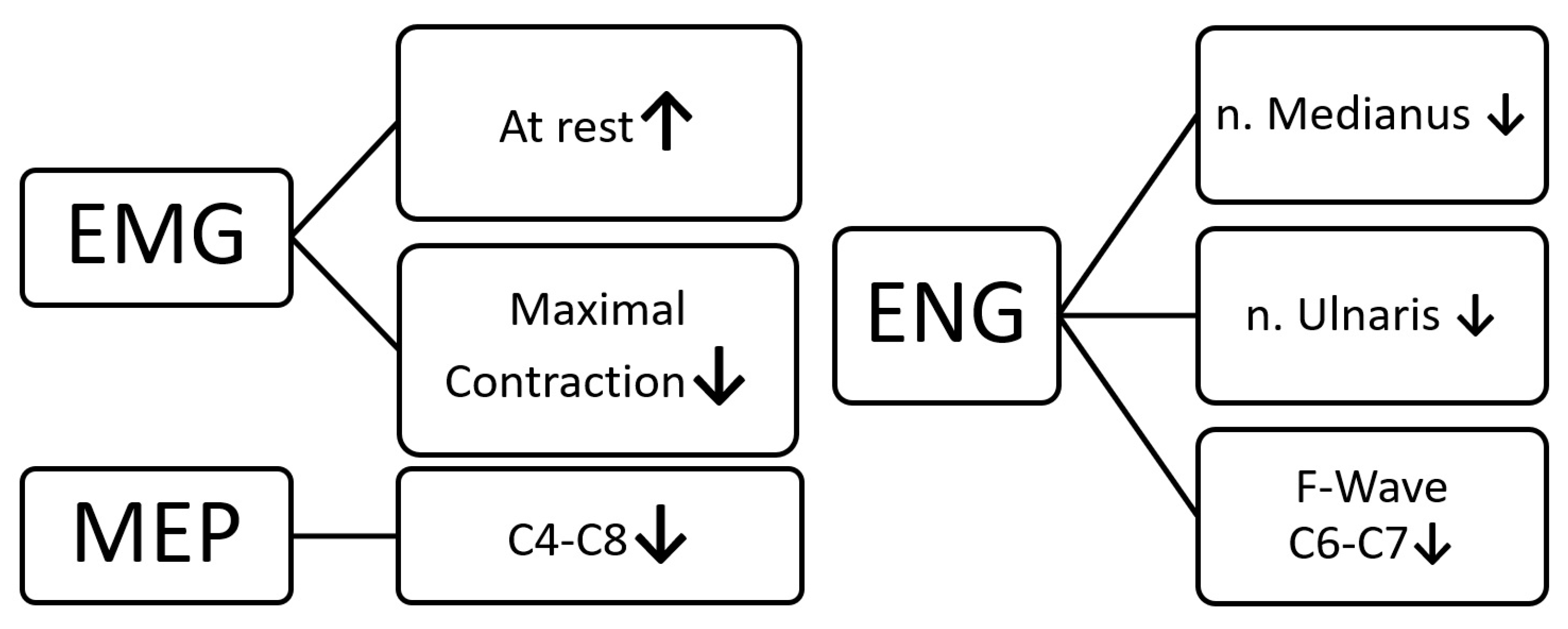
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adamczyk, G. Nerve Entrapment of Upper Extremities in Sports. In Sports Injuries; Doral, M.N., Karlsson, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Belviso, I.; Palermi, S.; Sacco, A.M.; Romano, V.; Corrado, B.; Zappia, M.; Sirico, F. Brachial Plexus Injuries in Sport Medicine: Clinical Evaluation, Diagnostic Approaches, Treatment Options, and Rehabilitative Interventions. J. Funct. Morphol. Kinesiol. 2020, 5, 22. [Google Scholar] [CrossRef]
- Sorbie, G.G.; Hunter, H.H.; Grace, F.M.; Gu, Y.; Baker, J.S.; Ugbolue, U.C. An electromyographic study of the effect of hand grip sizes on forearm muscle activity and golf performance. Res. Sports Med. 2016, 24, 207–218. [Google Scholar] [CrossRef]
- Ertan, H. Muscular activation patterns of the bow arm in recurve archery. J. Sci. Med. Sport 2009, 12, 357–360. [Google Scholar] [CrossRef]
- Shyu, W.C.; Lin, J.C.; Chang, M.K.; Tsao, W.L. Compressive radial nerve palsy induced by military shooting training: Clinical and electrophysiological study. J. Neurol. Neurosurg. Psychiatr. 1993, 56, 890–893. [Google Scholar] [CrossRef] [PubMed]
- Zeman, V.; Pitr, K. Dysfunction of the motor system in sports shooters. Sports Med. Train. Rehabil. 2001, 10, 1–11. [Google Scholar] [CrossRef]
- Bryndal, A.; Wojtysiak, M.; Moskal, J.; Lipiec-Kowalska, J.; Borowczyk, M.; Tańska, M.; Grochulska, A.; Huber, J.; Majchrzycki, M. Motor Evoked Potentials after Supraspinal Stimulation in Pre- and Postoperative Evaluations of Patients with Cervical Radiculopathy. BioMed Res. Int. 2019, 2019, 4576493. [Google Scholar] [CrossRef] [PubMed]
- Huber, J.; Lisiński, P.; Polowczyk, A. Reinvestigation of the dysfunction in neck and shoulder girdle muscles as the reason of cervicogenic headache among office workers. Disabil. Rehabil. 2013, 35, 793–802. [Google Scholar] [CrossRef]
- Huber, J.; Leszczyńska, K.; Wincek, A.; Szymankiewicz-Szukała, A.; Fortuna, W.; Okurowski, S.; Tabakow, P. The Role of Peripheral Nerve Electrotherapy in Functional Recovery of Muscle Motor Units in Patients after Incomplete Spinal Cord Injury. Appl. Sci. 2021, 11, 9764. [Google Scholar] [CrossRef]
- Kaczmarek, A.M.; Huber, J.; Leszczyńska, K.; Wietrzak, P.; Kaczmarek, K. Relationships between the Clinical Test Results and Neurophysiological Findings in Patients with Thoracic Outlet Syndrome. Bioengineering 2022, 9, 598. [Google Scholar] [CrossRef]
- Pannell, W.C.; Heckmann, N.; Alluri, R.K.; Sivasundaram, L.; Stevanovic, M.; Ghiassi, A. Predictors of Nerve Injury After Gunshot Wounds to the Upper Extremity. Hand 2017, 12, 501–506. [Google Scholar] [CrossRef]
- Feng, Y.; Schlösser, F.J.; Sumpio, B.E. The Semmes Weinstein monofilament examination as a screening tool for diabetic peripheral neuropathy. J. Vasc. Surg. 2009, 50, 675–682. [Google Scholar] [CrossRef]
- Lisiński, P.; Huber, J. Evolution of Muscles Dysfunction from Myofascial Pain Syndrome Through Cervical Disc-Root Conflict to Degenerative Spine Disease. Spine 2017, 42, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Haloua, M.H.; Sierevelt, I.; Theuvenet, W.J. Semmes-Weinstein mono-filaments: Influence of temperature, humidity and age. J. Hand Surg. 2011, 36, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Lifchez, S.D.; Means, K.R.; Dunn, R.E.; Williams, E.H.; Dellon, A.L. Intra- and inter-examiner variability in performing Tinel’s test. J. Hand Surg. 2010, 35, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Wincek, A.; Huber, J.; Leszczyńska, K.; Fortuna, W.; Okurowski, S.; Chmielak, K.; Tabakow, P. The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation rTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury. J. Clin. Med. 2021, 10, 2975. [Google Scholar] [CrossRef]
- Kaczmarek, K.; Huber, J.; Leszczyńska, K.; Daroszewski, P. Electroneurographic Evaluation of Neural Impulse Transmission in Patients after Ischemic Stroke Following Functional Electrical Stimulation of Antagonistic Muscles at Wrist and Ankle in Two-Month Follow-Up. Int. J. Environ. Res. Public. Health 2022, 19, 713. [Google Scholar] [CrossRef]
- Räty, H.P.; Kujala, U.M.; Videman, T.; Impivaara, O.; Crites Battié, M.; Sarna, S. Lifetime musculoskeletal symptoms and injuries among former elite male athletes. Int. J. Sports Med. 1997, 18, 625–632. [Google Scholar] [CrossRef]
- Ojanen, T.; Kyröläinen, H.; Igendia, M.; Häkkinen, K. Effect of Prolonged Military Field Training on Neuromuscular and Hormonal Responses and Shooting Performance in Warfighters. Mil. Med. 2018, 183, e705–e712. [Google Scholar] [CrossRef]
- Rubens, O.; Logina, I.; Kravale, I.; Eglite, M.; Donaghy, M. Peripheral neuropathy in chronic occupational inorganic lead exposure: A clinical and electrophysiological study. J. Neurol. Neurosurg. Psychiatr. 2001, 71, 200–204. [Google Scholar] [CrossRef]
- Sakellariou, V.I.; Badilas, N.K.; Mazis, G.A.; Stavropoulos, N.A.; Kotoulas, H.K.; Kyriakopoulos, S.; Tagkalegkas, I.; Sofianos, I.P. Brachial Plexus Injuries in Adults: Evaluation and Diagnostic Approach. ISRN Orthop. 2014, 2014, 726103. [Google Scholar] [CrossRef]
- Wiertel-Krawczuk, A.; Huber, J. Standard neurophysiological studies and motor evoked potentials in evaluation of traumatic brachial plexus injuries—A brief review of the literature. Neurol. Neurochir. Pol. 2018, 52, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Wiertel-Krawczuk, A.; Huber, J.; Szymankiewicz-Szukała, A.; Wincek, A. Neurophysiological Evaluation of Neural Transmission in Brachial Plexus Motor Fibers with the Use of Magnetic versus Electrical Stimuli. Sensors 2023, 23, 4175. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control (N = 9) | Shooters (N = 9) | p |
|---|---|---|---|
| Age (years) | 41.6 ± 13.0 | 43.4 ± 14.1 | 0.08 |
| Weight (kg) | 76.2 ± 11.8 | 82.4 ± 16.1 | 0.06 |
| Height (cm) | 172.8 ± 6.5 | 174.7 ± 10.1 | 0.08 |
| BMI | 25.4 ± 2.9 | 27.0 ± 4.8 | 0.08 |
| Shooting hand/dominant hand | Right = 9 | Right = 8 Left = 1 | 0.05 |
| Practice (years) | NA | 7.1 ± 36.0 | NA |
| Frequency of training (x/month) | NA | 4.8 ± 3.4 | NA |
| Pain VAS (0–10) | 0 | 1 | 0.06 |
| vfF filaments, 2nd fingertip (C6–C7) | 1 | 2 | 0.02 |
| vfF filaments, 5th fingertip (C8–T1) | 1 | 2 | 0.02 |
| vfF filaments, area over biceps (C5) | 1 | 2 | 0.05 |
| Site of Recording | Parameter | Control | Shooters | p | ||||
|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | |||
| sEMG | DEL | rEMG (µV) | 13.3 ± 4.3 | 15.0 ± 3.5 | 18.9 ± 5.4 | 18.3 ± 4.3 | 0.05 | 0.06 |
| mcEMG (µV) | 1522.2 ± 198.6 | 1567.0 ± 163.6 | 1211.1 ± 132.6 | 1522.0 ± 443.8 | 0.03 | 0.13 | ||
| FE | 2.3 ± 0.5 | 2.3 ± 0.5 | 2.7 ± 0.4 | 2.3 ± 0.5 | 0.06 | 0.12 | ||
| BB | rEMG (µV) | 13.8 ± 3.3 | 16.1 ± 3.3 | 22.2 ± 6.6 | 18.3 ± 6.6 | 0.02 | 0.07 | |
| mcEMG (µV) | 1522.2 ± 454.0 | 1577.7 ± 484.1 | 1422.2 ± 840.8 | 1344.4 ± 769.9 | 0.09 | 0.1 | ||
| FE | 2.7 ± 0.4 | 2.7 ± 0.4 | 2.3 ± 0.5 | 2.2 ± 0.4 | 0.05 | 0.04 | ||
| APB | rEMG (µV) | 13.9 ± 3.3 | 16.1 ± 3.3 | 18.9 ± 6.0 | 17.2 ± 7.5 | 0.02 | 0.1 | |
| mcEMG (µV) | 1588.9 ± 459.4 | 1611.1 ± 428.4 | 1600.0 ± 107.2 | 1677.8 ± 902.4 | 0.1 | 0.12 | ||
| FE | 2.8 ± 0.3 | 2.9 ± 0.3 | 2.6 ± 0.5 | 2.5 ± 0.5 | 0.12 | 0.11 | ||
| ADM | rEMG (µV) | 14.9 ± 2.5 | 15.0 ± 3.5 | 18.3 ± 5.6 | 17.7 ± 6.6 | 0.04 | 0.06 | |
| mcEMG (µV) | 1922.2 ± 120.4 | 2355.5 ± 111.7 | 1511.1 ± 459.4 | 1688.8 ± 348.0 | 0.02 | 0.03 | ||
| FE | 2.8 ± 0.3 | 2.7 ± 0.4 | 2.7 ± 0.4 | 2.5 ± 0.5 | 0.07 | 0.07 | ||
| ENG—median nerve | M-wave Wrist | Amplitude (µV) | 11,111.1 ± 2204.7 | 11,111.2 ± 2227.6 | 8833.3 ± 3142.4 | 9888.9 ± 2027.6 | 0.02 | 0.03 |
| Latency (ms) | 3.0 ± 0.3 | 3.1 ± 0.2 | 3.6 ± 1.2 | 3.5 ± 0.9 | 0.02 | 0.05 | ||
| M-wave | Amplitude (µV) | 977.7 ± 1487.3 | 972.8 ± 1394.4 | 7833.3 ± 3500.0 | 8333.3 ± 2397.9 | 0.02 | 0.05 | |
| FOC | Latency (ms) | 6.4 ± 0.6 | 6.5 ± 0.5 | 7.1 ± 0.8 | 7.2 ± 0.6 | 0.06 | 0.07 | |
| M-wave | Amplitude (µV) | 11,222.0 ± 1986.1 | 11,111.0 ± 1900.3 | 9444.4 ± 4245.9 | 11,278.0 ± 2796.3 | 0.02 | 0.06 | |
| Arm | Latency (ms) | 8.3 ± 0.4 | 8.4 ± 0.4 | 8.5 ± 1.0 | 9.0 ± 0.8 | 0.06 | 0.07 | |
| M-wave | Amplitude (µV) | 11,122.0 ± 1986.1 | 11,000.0 ± 2000.0 | 10,111.1 ± 669.8 | 12,811.1 ± 3206.0 | 0.07 | 0.06 | |
| Erb | Latency (ms) | 10.7 ± 1.7 | 10.5 ± 1.0 | 13.5 ± 0.7 | 13.4 ± 0.9 | 0.02 | 0.03 | |
| SCV—wrist | Amplitude (µV) | 16.2 ± 6.8 | 14.7 ± 7.7 | 14.0 ± 10.0 | 11.5 ± 5.3 | 0.05 | 0.03 | |
| Latency (ms) | 2.9 ± 0.1 | 2.9 ± 0.2 | 3.2 ± 0.6 | 3.3 ± 0.4 | 0.06 | 0.07 | ||
| F-wave (x/20) | 17.8 ± 1.8 | 17.3 ± 2.0 | 15.6 ± 3.4 | 16.1 ± 3.4 | 0.05 | 0.13 | ||
| M-F latency (ms) | 22.7 ± 2.0 | 23.9 ± 2.7 | 23.8 ± 2.7 | 24.6 ± 1.9 | 0.07 | 0.06 | ||
| ENG—ulnar nerve | M-wave Wrist | Amplitude (µV) | 10,556.0 ± 1130.4 | 10,888.9 ± 1763.8 | 9777.8 ± 322.1 | 10,111.1 ± 2204.8 | 0.05 | 0.06 |
| Latency (ms) | 3.1 ± 0.3 | 3.1 ± 0.1 | 2.7 ± 0.5 | 2.7 ± 0.2 | 0.06 | 0.07 | ||
| M-wave | Amplitude (µV) | 9000 ± 866.3 | 9666.7 ± 866.0 | 7477.8 ± 3362.2 | 8666.7 ± 1145.6 | 0.05 | 0.06 | |
| Sulcus uln. | Latency (ms) | 6.4 ± 0.4 | 6.5 ± 0.4 | 6.7 ± 0.5 | 6.5 ± 0.6 | 0.1 | 0.1 | |
| M-wave | Amplitude (µV) | 9888.9 ± 21453.0 | 9777.8 ± 1201.9 | 9666.7 ± 3741.7 | 9000.0 ± 1500.0 | 0.1 | 0.05 | |
| Arm | Latency (ms) | 8.2 ± 0.5 | 8.3 ± 0.3 | 8.8 ± 0.9 | 8.9 ± 0.9 | 0.1 | 0.1 | |
| M-wave | Amplitude (µV) | 10,556.0 ± 1130.4 | 10,889.0 ± 1763.8 | 4844.4 ± 3644.4 | 3644.4 ± 3178.1 | 0.03 | 0.02 | |
| Erb | Latency (ms) | 10.5 ± 1.6 | 10.4 ± 1.2 | 13.1 ± 1.2 | 12.9 ± 0.7 | 0.03 | 0.02 | |
| SCV—wrist | Amplitude (µV) | 16.7 ± 4.3 | 16.1 ± 6.4 | 10.9 ± 4.6 | 10.8 ± 4.3 | 0.02 | 0.02 | |
| Latency (ms) | 2.9 ± 0.2 | 2.9 ± 0.1 | 2.7 ± 0.3 | 3.0 ± 0.5 | 0.07 | 0.06 | ||
| F-wave (x/20) | 18.1 ± 1.5 | 18.1 ± 1.5 | 17.3 ± 2.6 | 16.7 ± 2.4 | 0.06 | 0.07 | ||
| M-F latency (ms) | 25.3 ± 0.7 | 25.5 ± 0.8 | 23.9 ± 2.2 | 25.0 ± 2.1 | 0.06 | 0.07 | ||
| MEP | DEL | Amplitude (µV) | 1188.9 ± 169.1 | 1177.8 ± 120.1 | 477.8 ± 192.2 | 700.0 ± 531.1 | 0.02 | 0.03 |
| Latency (ms) | 4.9 ± 0.3 | 5.1 ± 0.3 | 4.9 ± 0.3 | 5.1 ± 0.3 | 0.1 | 0.1 | ||
| BB | Amplitude (µV) | 1166.7 ± 122.5 | 1188.9 ± 161.6 | 1066.7 ± 878.9 | 1311.1 ± 873.9 | 0.1 | 0.07 | |
| Latency (ms) | 5.5 ± 0.4 | 5.6 ± 0.4 | 5.9 ± 0.8 | 6.1 ± 0.6 | 0.02 | 0.03 | ||
| APB | Amplitude (µV) | 1200.0 ± 165.8 | 1200.0 ± 200.0 | 866.6 ± 878.9 | 511.1 ± 275.8 | 0.03 | 0.02 | |
| Latency (ms) | 13.6 ± 0.3 | 13.5 ± 0.4 | 14.1 ± 1.1 | 14.0 ± 0.9 | 0.1 | 0.1 | ||
| ADM | Amplitude (µV) | 1211.1 ± 161.5 | 1155.6 ± 113.4 | 677.8 ± 108.3 | 644.4 ± 339.5 | 0.03 | 0.02 | |
| Latency (ms) | 13.2 ± 0.5 | 13.4 ± 0.5 | 14.2 ± 1.6 | 14.5 ± 0.9 | 0.09 | 0.1 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajczewski, A.; Daroszewski, P.; Fabijański, A.; Bogusławski, K.; Kaźmierczak, M.; Huber, J. Incidence of Carpal Tunnel Syndrome and Other Coexisting Brachial Plexus Neuropathies in Bullseye Shooters—A Pilot Retrospective Clinical and Neurophysiological Assessment. Appl. Sci. 2023, 13, 8020. https://doi.org/10.3390/app13148020
Rajczewski A, Daroszewski P, Fabijański A, Bogusławski K, Kaźmierczak M, Huber J. Incidence of Carpal Tunnel Syndrome and Other Coexisting Brachial Plexus Neuropathies in Bullseye Shooters—A Pilot Retrospective Clinical and Neurophysiological Assessment. Applied Sciences. 2023; 13(14):8020. https://doi.org/10.3390/app13148020
Chicago/Turabian StyleRajczewski, Aleksander, Przemysław Daroszewski, Artur Fabijański, Ksawery Bogusławski, Michał Kaźmierczak, and Juliusz Huber. 2023. "Incidence of Carpal Tunnel Syndrome and Other Coexisting Brachial Plexus Neuropathies in Bullseye Shooters—A Pilot Retrospective Clinical and Neurophysiological Assessment" Applied Sciences 13, no. 14: 8020. https://doi.org/10.3390/app13148020
APA StyleRajczewski, A., Daroszewski, P., Fabijański, A., Bogusławski, K., Kaźmierczak, M., & Huber, J. (2023). Incidence of Carpal Tunnel Syndrome and Other Coexisting Brachial Plexus Neuropathies in Bullseye Shooters—A Pilot Retrospective Clinical and Neurophysiological Assessment. Applied Sciences, 13(14), 8020. https://doi.org/10.3390/app13148020