
Anterior Incisal Onlay—A Minimally Invasive Non-Surgical Approach to Correct an Esthetic Complication of an Implant Supported Crown in the Anterior Zone

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
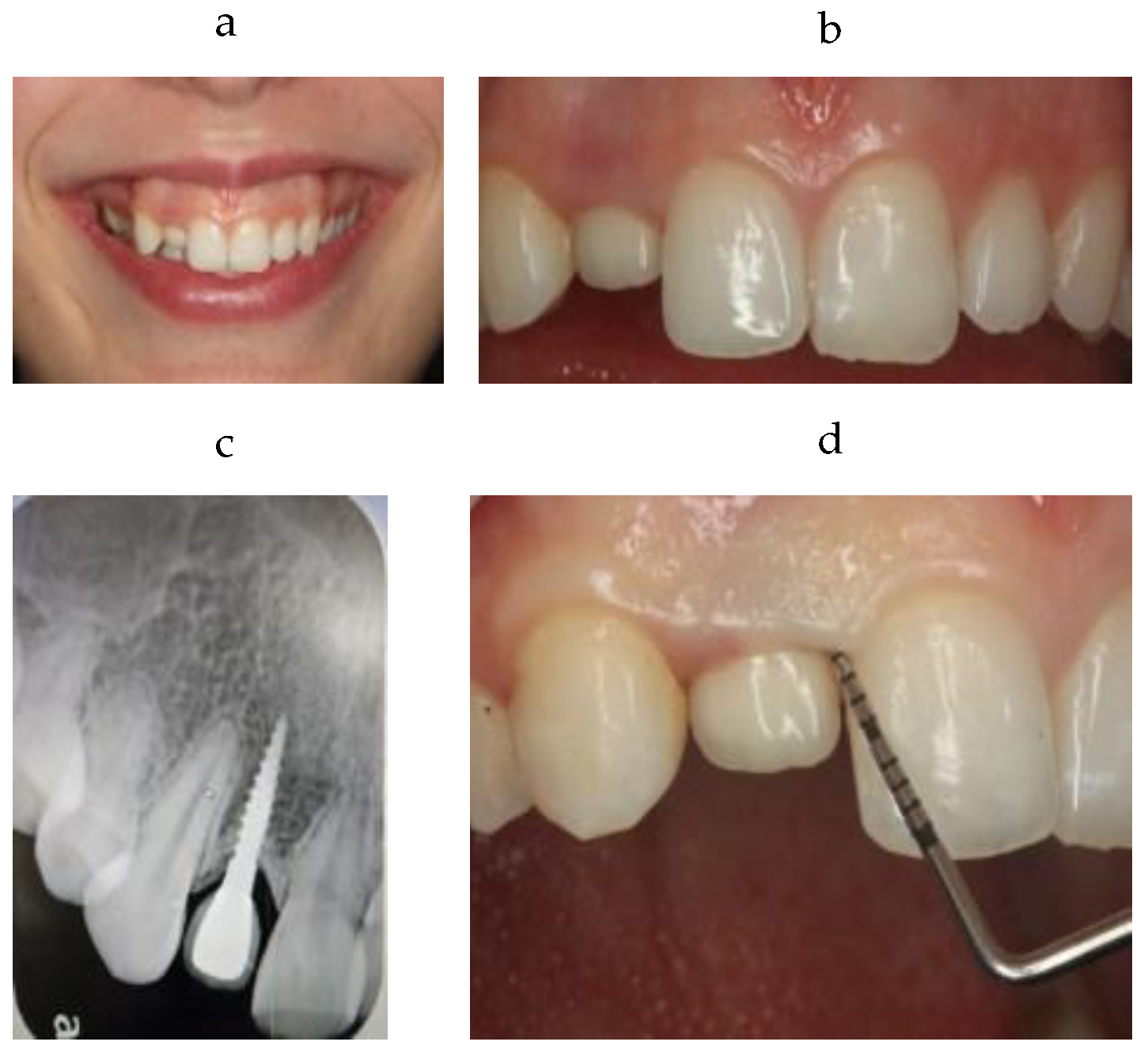
2. Clinical Case
3. Treatment Plan
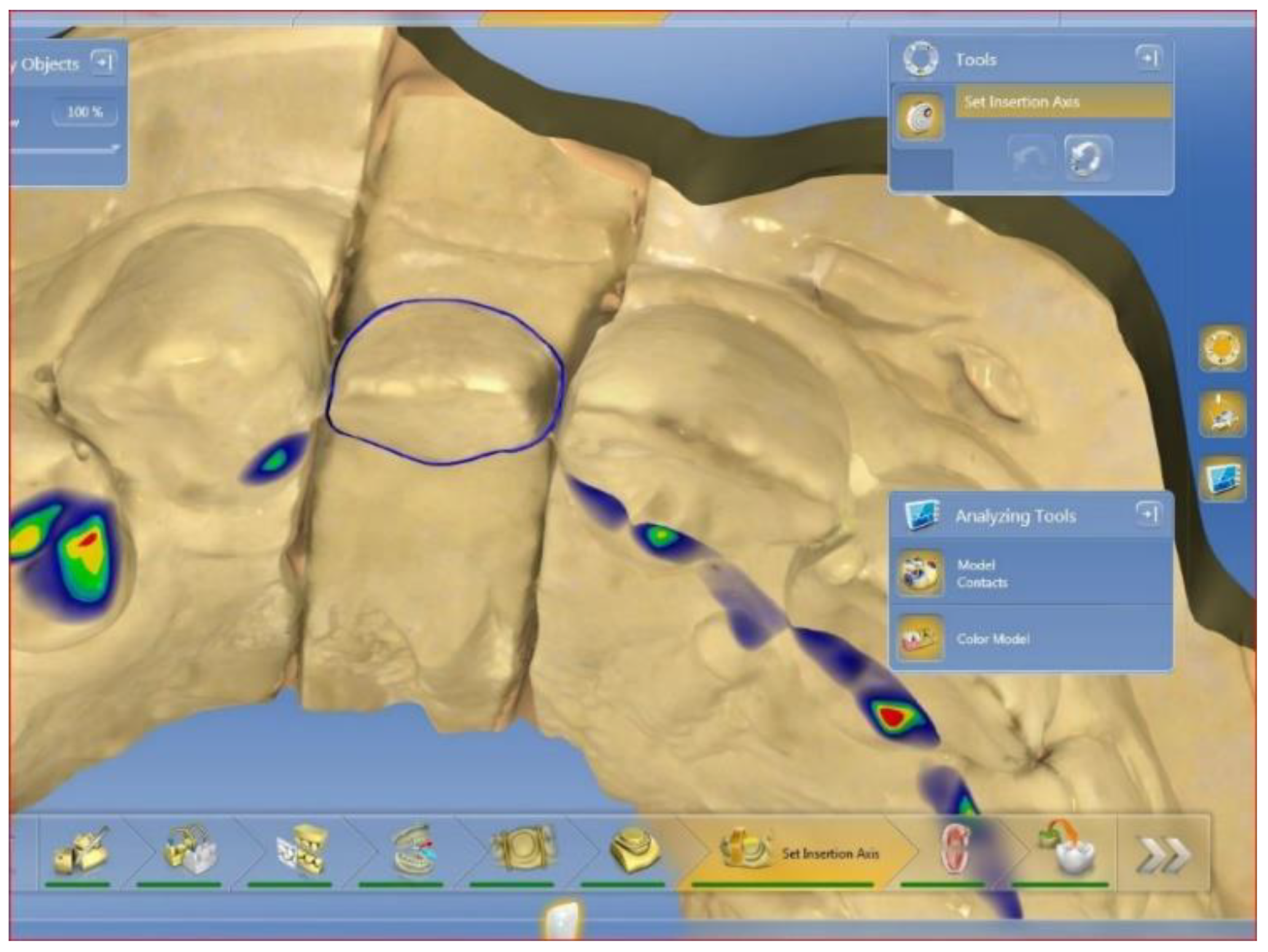
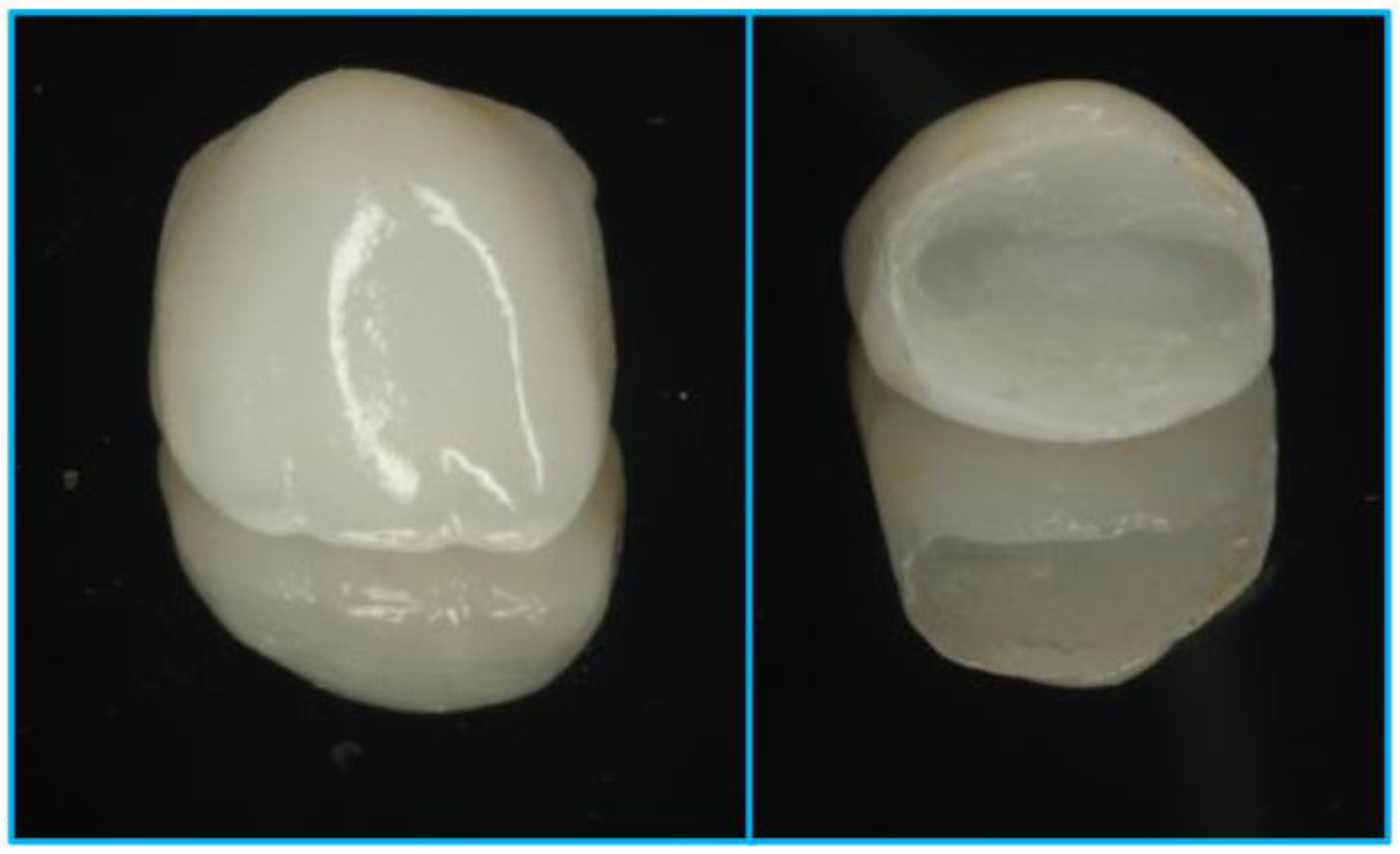
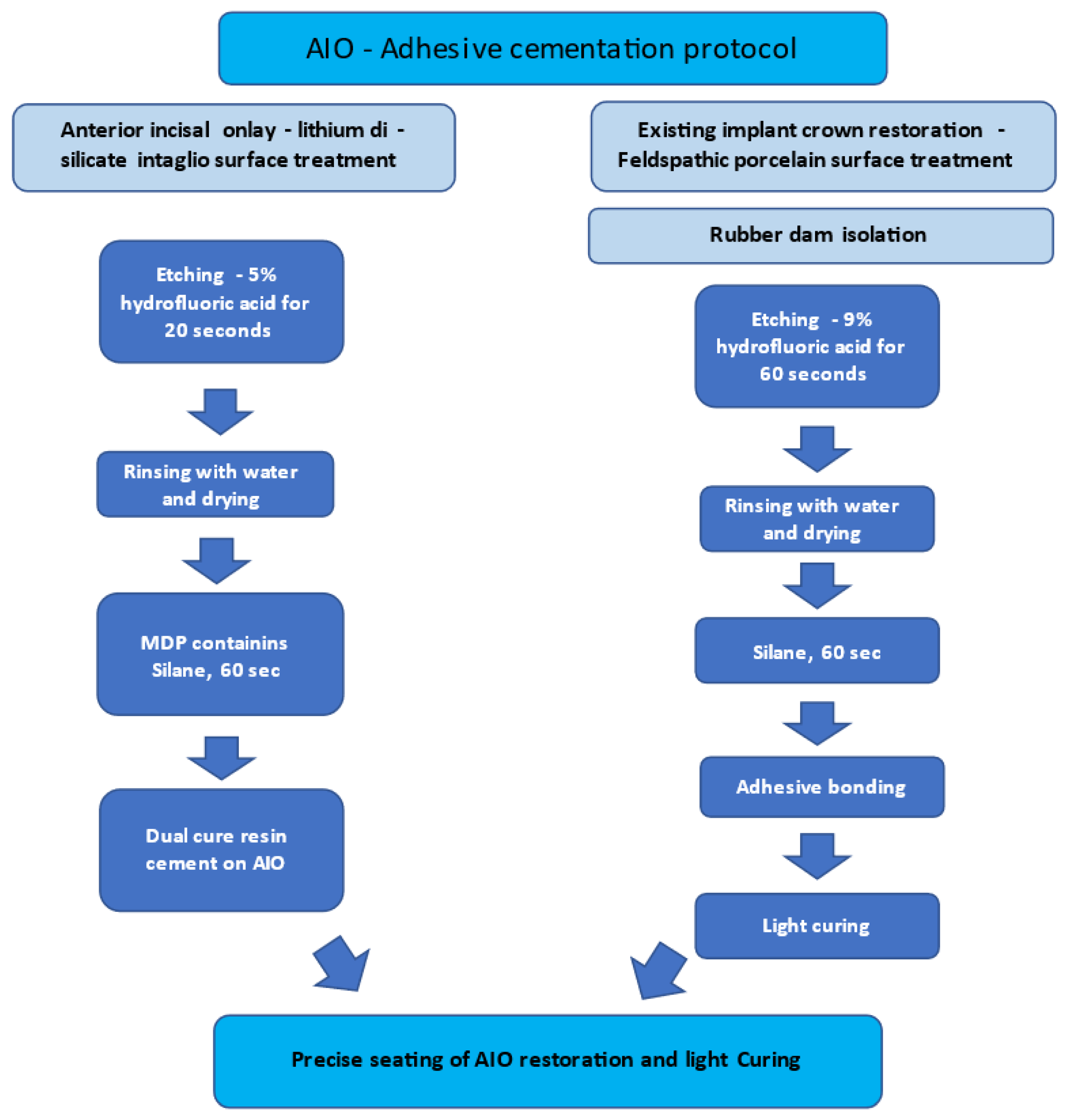
4. Treatment Sequence
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Op Heij, D.G.; Opdebeeck, H.; van Steenberghe, D.; Quirynen, M. Age as compromising factor for implant insertion. Periodontology 2000 2003, 33, 172–844. [Google Scholar] [CrossRef] [PubMed]
- Daftary, F.; Mahallati, R.; Bahat, O.; Sullivan, R.M. Lifelong craniofacial growth and the implications for Osseo integrated implants. Int. J. Oral Maxillofac. Implant. 2013, 28, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Cocchetto, R.; Pradies, G.; Celletti, R.; Canullo, L. Continuous craniofacial growth in adult patients treated with dental implants in the anterior maxilla. Clin. Implant Dent. Relat. Res. 2019, 21, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Schwartz-Arad, D.; Bichacho, N. Effect of Age on Single Implant Submersion Rate in the Central Maxillary Incisor Region: A Long-Term Retrospective Study. Clin. Implant Dent. Relat. Res. 2013, 17, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Barrachina-Diez, J.M.; Tashkandi, E.; Stampf, S.; Att, W. Long-term outcome of one-piece implants. Part I: Implant characteristics and loading protocols. A systematic literature review with meta-analysis. Int. J. Oral Maxillofac. Implant. 2013, 28, 503–518. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tallarico, M.; Caneva, M.; Meloni, S.M.; Xhanari, E.; Omori, Y.; Canullo, L. Survival and Success Rates of Different Shoulder Designs: A Systematic Review of the Literature. Int. J. Dent. 2018, 2018, 6812875. [Google Scholar] [CrossRef] [PubMed]
- Silberberg, N.; Goldstein, M.; Smidt, A. Excessive gingival display–etiology, diagnosis, and treatment modalities. Quintessence Int. 2009, 40, 809–818. [Google Scholar] [PubMed]
- Strasding, M.; Fehmer, V.; Pjetursson, B.E.; Sailer, I. Extending the service life of existing dental restorations with esthetic and functional limitations. J. Prosthet. Dent. 2018, 119, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Blum, I.R.; Jagger, D.C.; Wilson, N.H. Defective dental restorations: To repair or not to repair? Part 2: All–ceramics and porcelain fused to metal systems. Dent. Update 2011, 38, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Zandinejad, A.; Lin, W.S.; Atarodi, M.; Abdel-Azim, T.; Metz, M.J.; Morton, D. Digital workflow for virtually designing and milling ceramic lithium disilicate veneers: A clinical report. Oper. Dent. 2015, 40, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Vidal, P.C.; Utrilla, T.M.; Souza, A.J. Surface Treatment of Lithium Disilicate with Different Concentrations of Hydrofluoric Acid and Orthophosphoric Acid. J. Dent. Sci. 2019, 18, 1128–1137. [Google Scholar]
- Straface, A.; Rupp, L.; Gintaute, A.; Fischer, J.; Zitzmann, N.U.; Rohr, N. HF etching of CAD/CAM materials: Influence of HF concentration and etching time on shear bond strength. Head Face Med. 2019, 15, 21. [Google Scholar] [CrossRef] [PubMed]
- Moura, D.M.D.; Araújo, A.M.M.D.; Souza, K.B.D.; Veríssimo, A.H.; Tribst, J.P.M.; Souza, R.O.D.A. Hydrofluoric acid concentration, time and use of phosphoric acid on the bond strength of feldspathic ceramics. Braz. Oral Res. 2020, 34, e018. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in non-surgical periodontal therapy: Clinical and microbiological aspects in a 6-month follow-up domiciliary protocol for oral hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized water administration in peri-implant mucositis sites: A randomized clinical trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zabrovsky, A.; Bar-on, H.; Beyth, N.; Smidt, A.; Ben-Gal, G. Anterior Incisal Onlay—A Minimally Invasive Non-Surgical Approach to Correct an Esthetic Complication of an Implant Supported Crown in the Anterior Zone. Appl. Sci. 2022, 12, 3808. https://doi.org/10.3390/app12083808
Zabrovsky A, Bar-on H, Beyth N, Smidt A, Ben-Gal G. Anterior Incisal Onlay—A Minimally Invasive Non-Surgical Approach to Correct an Esthetic Complication of an Implant Supported Crown in the Anterior Zone. Applied Sciences. 2022; 12(8):3808. https://doi.org/10.3390/app12083808
Chicago/Turabian StyleZabrovsky, Asher, Hilit Bar-on, Nurit Beyth, Ami Smidt, and Gilad Ben-Gal. 2022. "Anterior Incisal Onlay—A Minimally Invasive Non-Surgical Approach to Correct an Esthetic Complication of an Implant Supported Crown in the Anterior Zone" Applied Sciences 12, no. 8: 3808. https://doi.org/10.3390/app12083808
APA StyleZabrovsky, A., Bar-on, H., Beyth, N., Smidt, A., & Ben-Gal, G. (2022). Anterior Incisal Onlay—A Minimally Invasive Non-Surgical Approach to Correct an Esthetic Complication of an Implant Supported Crown in the Anterior Zone. Applied Sciences, 12(8), 3808. https://doi.org/10.3390/app12083808