
Effects of an Adapted Sports Intervention on Elderly Women in Need of Long-Term Care: A Pilot Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
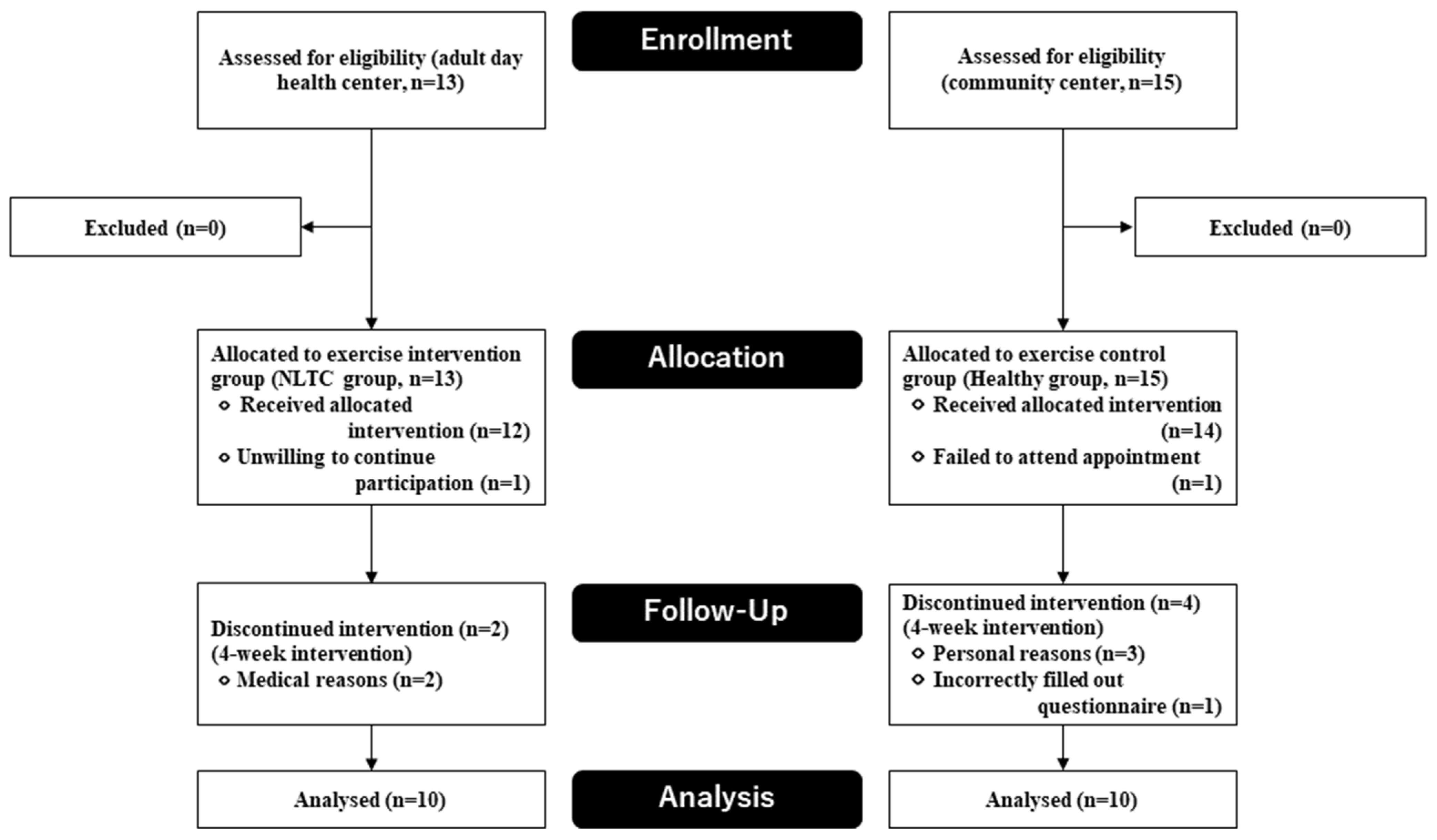
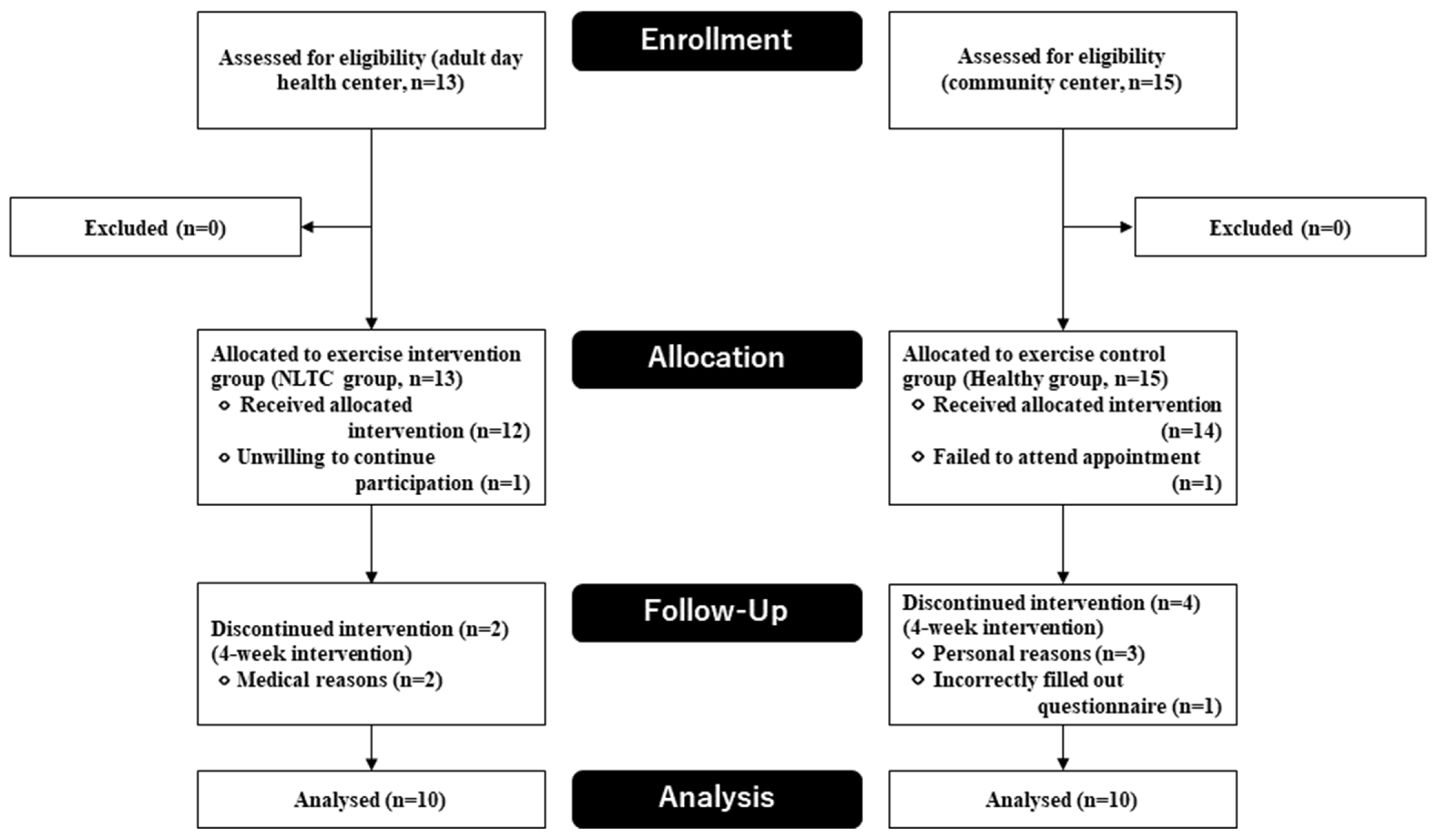
2.1. Participants
2.1.1. Elderly Women in Need of Long-Term Care Group: NLTC Group
2.1.2. Healthy Elderly Women Group; Healthy Group
2.2. Exercise Intervention
2.2.1. Adapted Sport Event
2.2.2. Boccia Exercise Intervention
2.3. Measurement
2.3.1. Baseline Variables
2.3.2. Outcomes
Profile of Moods States
Health-Related Quality of Life
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Health Observatory Data Repository: Healthy Life Expectancy (HALE) Data by Country 2019. 2021. Available online: https://apps.who.int/gho/data/node.main.HALE?lang=en (accessed on 20 December 2021).
- Organisation for Economic Cooperation and Development (OECD). How’s Life? Well-Being: Perceived Health Status. 2019. Available online: https://stats.oecd.org/Index.aspx?datasetcode=HSL (accessed on 20 December 2021).
- Paffenbarger, R.S.; Hyde, R.; Wing, A.L.; Hsieh, C.C. Physical activity, all-cause mortality, and longevity of college alumni. N. Engl. J. Med. 1986, 314, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Rejeski, W.J.; Pandya, J.; Miller, M.E.; Di Bari, M.; Applegate, W.B.; Pahor, M. Exercise and depressive symptoms: A comparison of aerobic and resistance exercise effects on emotional and physical function in older persons with high and low depressive symptomatology. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, 124–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ukawa, S.; Tamakoshi, A.; Sakamoto, A. A systematic review of intervention programs for frail elderly people enrolled in the Japanese social long-term care insurance system. Jpn. J. Public Health 2015, 62, 3–19, (In Japanese with English abstract). [Google Scholar]
- Latham, N.K.; Bennett, D.A.; Stretton, C.M.; Anderson, C.S. Systematic review of progressive resistance strength training in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, M48–M61. [Google Scholar] [CrossRef] [PubMed]
- Crocker, T.; Young, J.; Forster, A.; Brown, L.; Ozer, S.; Greenwood, D.C. The effect of physical rehabilitation on activities of daily living in older residents of long-term care facilities: Systematic review with meta-analysis. Age Ageing 2013, 42, 682–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conradsson, M.; Littbrand, H.; Lindelöf, N.; Gustafson, Y.; Rosendahl, E. Effects of a high-intensity functional exercise programme on depressive symptoms and psychological well-being among older people living in residential care facilities: A cluster-randomized controlled trial. Aging Ment. Health 2010, 14, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Heesch, K.C.; Miller, Y.D.; Brown, W.J. Relationship between physical activity and stiff or painful joints in mid-aged women and older women: A 3-year prospective study. Arthritis Res. Ther. 2007, 9, R34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binder, E.F.; Schechtman, K.B.; Ehsani, A.A.; Steger-May, K.; Brown, M.; Sinacore, D.R.; Holloszy, J.O. Effects of exercise training on frailty in community-dwelling older adults: Results of a randomized, controlled trial. J. Am. Geriatr. Soc. 2002, 50, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Izquierdo, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age 2014, 36, 773–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawano, T. Effects of the Adapted Sport on the Physical, Mental, and Social Health Status among Community-Dwelling Middle-Aged and Elderly Individuals. Ph.D. Thesis, University of Kyushu, Kyushu, Japan, 2015. (In Japanese with English abstract). [Google Scholar]
- Kawano, T.; Moriki, G.; Bono, S.; Kaji, N.; Jung, H. Effects of Household Composition on Health-Related Quality of Life among the Japanese middle-aged and elderly: Analysis from a gender perspective. Jpn. J. Soc. Welf. 2019, 60, 1–12. [Google Scholar]
- Yabe, K. Recommendations of Adapted Sports. Normalizat. Welf. Pers. Disabil. 1997, 12, 17–19. (In Japanese) [Google Scholar]
- Winnick, J.; Porretta, D. (Eds.) Adapted Physical Education and Sport, 6th ed.; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Muraki, S.; Tsunawake, N.; Hiramatsu, S.; Yamasaki, M. The effect of frequency and mode of sports activity on the psychological status in tetraplegics and paraplegics. Spin. Cord. 2000, 38, 309–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yazicioglu, K.; Yavuz, F.; Goktepe, A.S.; Tan, A.K. Influence of adapted sports on quality of life and life satisfaction in sport participants and non-sport participants with physical disabilities. Disabil. Health J. 2012, 5, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Côté-Leclerc, F.; Duchesne, G.B.; Bolduc, P.; Gélinas-Lafrenière, A.; Santerre, C.; Desrosiers, J.; Levasseur, M. How does playing adapted sports affect quality of life of people with mobility limitations? Results from a mixed-method sequential explanatory study. Health Qual. Life Outcomes 2017, 15, 22. [Google Scholar] [CrossRef] [Green Version]
- Shinkai, S.; Fujita, K.; Fujiwara, Y.; Kumagai, S.; Amano, H.; Yoshida, H.; Wang, D.G.; Watanabe, S. Prevalence and characteristics of different types of homeboundness among community-living older adults. Jpn. J. Public Health 2005, 52, 443–455, (In Japanese with English abstract). [Google Scholar]
- Łosień, T.; Mędrak, A.; Plaskacz, P.; Bajerska, I.; Reut, M.; Dragon, E.; Polko, M.; Cebula, A. The influence of boccia on self-esteem and increasing the functional capabilities of disabled people. J. Phys. Educ. Sport 2018, 8, 1099–1105. [Google Scholar]
- Barak, S.; Mendoza-Laiz, N.; Gutiérrez Fuentes, M.T.; Rubiera, M.; Hutzler, Y. Psychosocial effects of competitive Boccia program in persons with severe chronic disability. J. Rehabil. Res. Dev. 2016, 53, 973–988. [Google Scholar] [CrossRef] [PubMed]
- Kawano, T.; Moriki, G.; Bono, S.; Kaji, N.; Yamasaki, M.; Muraki, S. Effects of the boccia as an adapted sport on the Mood states and Health-related quality of Life of elderly women in need of nursing care and assistance. Jpn. J. Adapt. Sport Sci. 2020, 18, 43–54. [Google Scholar]
- Japan Boccia Association. The Japan Boccia Association’s Competition Rules. 2021. Available online: https://japan-boccia.com/pdf/jboarules.pdf (accessed on 20 December 2021).
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG index of competence. Arch. Gerontol. Geriatr. 1999, 13, 103–116. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Long-Term Care Insurance System of Japan. 2016. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/index.html (accessed on 20 December 2021).
- World Health Organization (WHO). Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Group; WHO: Geneva, Switzerland, 1994. [Google Scholar]
- Lubben, J.; Blozik, E.; Gillmann, G.; Iliffe, S.; von Renteln Kruse, W.; Beck, J.C.; Stuck, A.E. Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. Gerontologist 2006, 46, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heuchert, J.P.; McNair, D.M. Profile of Mood States, POMS-2; Multi-Health Systems Inc.: North Tonawanda, NY, USA, 2012. [Google Scholar]
- Fukuhara, S. Manual of SF-36v2 Japanese Version; Institute for Health Outcomes and Process Evaluation Research: Kyoto, Japan, 2004; pp. 7–145. [Google Scholar]
- Japan Sports Agency. Public Opinion Survey on the Implementation of Sports. 2019. Available online: https://www.mext.go.jp/sports/b_menu/toukei/chousa04/sports/1415963.htm (accessed on 20 December 2021).
- Kishimoto, Y.; Suzuki, E.; Iwase, T.; Doi, H.; Takao, S. Group involvement and self-rated health among the Japanese elderly: An examination of bonding and bridging social capital. BMC Public Health 2013, 13, 1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaitsu, M.; Kawachi, I.; Ashida, T.; Kondo, K.; Kondo, N. Participation in Community Group Activities Among Older Adults: Is Diversity of Group Membership Associated with Better Self-rated Health? J. Epidemiol. 2018, 28, 452–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Federation of Adapted Physical Activity (IFAPA). What Is APA. Available online: https://ifapa.net/what-is-apa/ (accessed on 20 December 2021).
- Hutzler, Y.; Bar-Eli, M. How to cope with bias while adapting for inclusion in physical education and sports: A judgment and decision-making perspective. Quest 2013, 65, 57–71. [Google Scholar] [CrossRef]

{kind=link}
| Variables | NLTC Group (n = 10) | Healthy Group (n = 10) | p Value | ||
|---|---|---|---|---|---|
| Age (years) | 80.6 | ±8.2 | 81.8 | ±5.2 | |
| Body mass index (kg/m2) | 22.5 | ±2.2 | 22.2 | ±3.4 | |
| Total score of TMIG-IC (range, 0–13) | 9.2 | ±3.7 | 12.6 | ±0.7 | * a |
| Instrumental Self-Maintenance (range, 0–5) | 3.5 | ±1.9 | 5.0 | ±0.0 | |
| Intellectual Activity (range, 0–4) | 3.4 | ±0.8 | 3.9 | ±0.3 | |
| Social Role (range, 0–4) | 2.3 | ±1.4 | 3.7 | ±0.7 | * a |
| Certification of needed long-term care or support | ** b | ||||
| Not certified | 0 | 0% | 10 | 100% | |
| Support levels 1 | 4 | 40% | 0 | 0% | |
| Support levels 2 | 2 | 20% | 0 | 0% | |
| Care levels 1 | 2 | 20% | 0 | 0% | |
| Care levels 2 | 2 | 20% | 0 | 0% | |
| Care levels 3 | 0 | 0% | 0 | 0% | |
| Care levels 4 | 0 | 0% | 0 | 0% | |
| Care levels 5 | 0 | 0% | 0 | 0% | |
| Quantitative ultrasound | |||||
| Speed of sound (m/s) | 1491.6 | ±13.4 | 1505.4 | ±10.7 | * a |
| Broadband ultrasound attenuation (-dB/MHz) | 69.3 | ±6.3 | 67.5 | ±10.2 | |
| T-score (SD) | −1.1 | ±0.5 | −1.0 | ±0.6 | |
| Normal (T-score more than −1.0) | 3 | 30% | 4 | 40% | |
| Osteopenia (T-score between −2.5 and −1.0) | 7 | 70% | 6 | 60% | |
| Osteoporosis (T-score less than −2.5) | 0 | 0% | 0 | 0% | |
| Household composition | |||||
| Single person | 2 | 20% | 2 | 20% | |
| Married couple | 2 | 20% | 3 | 30% | |
| Other | 6 | 60% | 5 | 50% | |
| Lubben Social Network Scale-6 score (range, 0–30) | 11.3 | ±5.4 | 20.2 | ±3.5 | *** a |
| Normal (score more than 12) | 6 | 60% | 10 | 100% | |
| Social isolation (score less than 12) | 4 | 40% | 0 | 0% | |
| Variables | NLTC Group (n = 10) | Healthy Group (n = 10) | Interaction (Group × Time) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post | Baseline | Post | F | p Value | η2 | ||||||||
| Score of POMS2-SF (Profile of Mood States) | ||||||||||||||
| AH | 54.4 | ±2.6 | 45.4 | ±1.5 | *** | 53.2 | ±4.3 | 53.2 | ±4.3 | 9.643 | 0.006 | ** | 0.349 | |
| CB | 63.2 | ±6.3 | 56.8 | ±5.1 | 56.4 | ±4.7 | 56.4 | ±4.7 | 1.075 | 0.314 | 0.560 | |||
| DD | 65.8 | ±6.4 | 49.9 | ±3.2 | 62.7 | ±5.8 | 51.1 | ±4.2 | 0.527 | 0.477 | 0.028 | |||
| FI | 55.7 | ±5.3 | 45.1 | ±2.1 | 49.9 | ±4.0 | 63.3 | ±2.8 | * | 7.825 | 0.012 | * | 0.303 | |
| TA | 58.8 | ±5.7 | 43.6 | ±2.3 | * | 51.1 | ±4.2 | 62.0 | ±4.0 | 8.035 | 0.011 | * | 0.309 | |
| VA | 48.1 | ±3.0 | 61.7 | ±1.9 | 63.3 | ±2.8 | 62.7 | ±5.8 | 2.428 | 0.137 | 0.119 | |||
| F | 50.4 | ±2.9 | 58.3 | ±2.3 | 62.0 | ±4.0 | 49.9 | ±4.0 | * | 7.209 | 0.015 | * | 0.286 | |
| TMD | 59.5 | ±5.5 | 44.2 | ±2.3 | ** | 49.6 | ±4.8 | 49.6 | ±4.8 | 7.611 | 0.013 | * | 0.297 | |
| Score of SF-36v2 (HRQOL) | ||||||||||||||
| PF | 19.6 | ±7.5 | 20.3 | ±6.2 | 44.5 | ±4.4 | 44.8 | ±3.8 | 0.007 | 0.934 | 0.000 | |||
| RP | 34.1 | ±5.1 | 35.1 | ±4.3 | 40.1 | ±3.8 | 46.4 | ±3.5 | 0.485 | 0.495 | 0.026 | |||
| BP | 40.5 | ±3.4 | 40.1 | ±3.3 | 43.2 | ±3.3 | 49.7 | ±3.1 | * | 4.710 | 0.044 | * | 0.207 | |
| GH | 44.7 | ±4.2 | 52.0 | ±3.9 | 51.4 | ±2.9 | 56.4 | ±2.8 | 0.520 | 0.480 | 0.028 | |||
| VT | 45.7 | ±5.0 | 47.6 | ±2.9 | 55.0 | ±2.9 | 56.9 | ±2.8 | 0.000 | 1.000 | 0.000 | |||
| SF | 41.5 | ±5.4 | 48.0 | ±3.4 | 50.6 | ±2.9 | 49.9 | ±3.1 | 2.333 | 0.144 | 0.115 | |||
| RE | 40.3 | ±3.6 | 41.9 | ±4.9 | 43.6 | ±4.2 | 49.8 | ±3.1 | 0.758 | 0.395 | 0.040 | |||
| MH | 41.9 | ±5.5 | 50.8 | ±3.7 | 53.7 | ±2.3 | 56.4 | ±2.6 | 2.088 | 0.166 | 0.104 | |||
| PCS | 27.3 | ±5.2 | 25.3 | ±5.1 | 41.1 | ±4.5 | 45.3 | ±3.0 | 1.986 | 0.176 | 0.099 | |||
| MCS | 52.7 | ±4.5 | 59.7 | ±2.7 | 58.3 | ±1.8 | 60.2 | ±2.5 | 1.576 | 0.225 | 0.080 | |||
| RCS | 41.5 | ±3.7 | 43.7 | ±4.1 | 43.7 | ±4.5 | 46.2 | ±3.1 | 0.002 | 0.962 | 0.000 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawano, T.; Moriki, G.; Bono, S.; Masumoto, J.; Kaji, N.; Jung, H.; Yamasaki, M. Effects of an Adapted Sports Intervention on Elderly Women in Need of Long-Term Care: A Pilot Study. Appl. Sci. 2022, 12, 3097. https://doi.org/10.3390/app12063097
Kawano T, Moriki G, Bono S, Masumoto J, Kaji N, Jung H, Yamasaki M. Effects of an Adapted Sports Intervention on Elderly Women in Need of Long-Term Care: A Pilot Study. Applied Sciences. 2022; 12(6):3097. https://doi.org/10.3390/app12063097
Chicago/Turabian StyleKawano, Takashi, Goro Moriki, Shinya Bono, Junya Masumoto, Nobuyuki Kaji, Hungu Jung, and Masahiro Yamasaki. 2022. "Effects of an Adapted Sports Intervention on Elderly Women in Need of Long-Term Care: A Pilot Study" Applied Sciences 12, no. 6: 3097. https://doi.org/10.3390/app12063097
APA StyleKawano, T., Moriki, G., Bono, S., Masumoto, J., Kaji, N., Jung, H., & Yamasaki, M. (2022). Effects of an Adapted Sports Intervention on Elderly Women in Need of Long-Term Care: A Pilot Study. Applied Sciences, 12(6), 3097. https://doi.org/10.3390/app12063097