
Intake Differences between Subsequent 24-h Dietary Recalls Create Significant Reporting Bias in Adults with Obesity

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of Subjects
2.2. Dietary Intake Assessment
2.3. Anthropometry, Biochemistry, and Diagnostic of Chronic Diseases
2.4. Data Analysis
3. Results
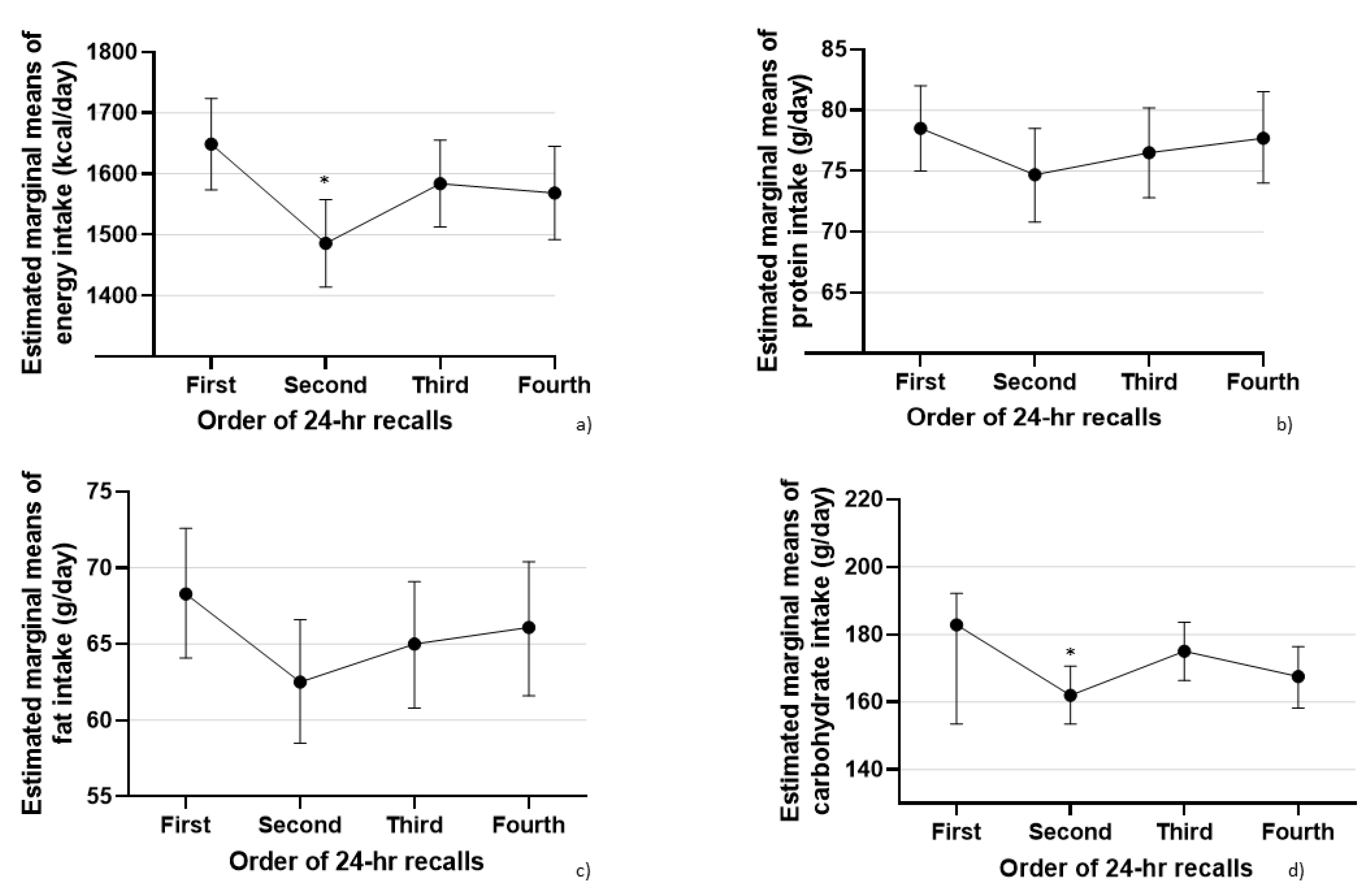
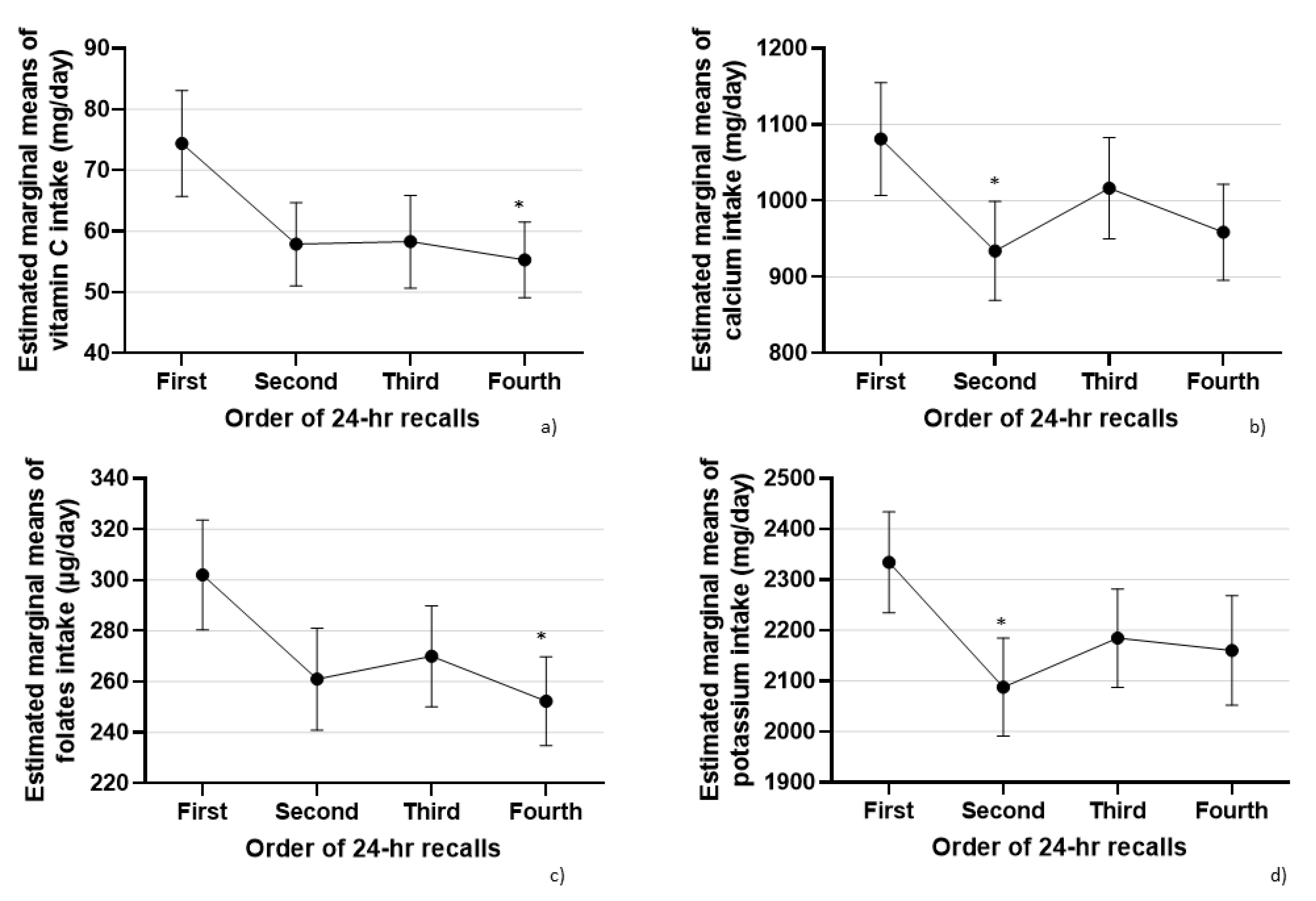
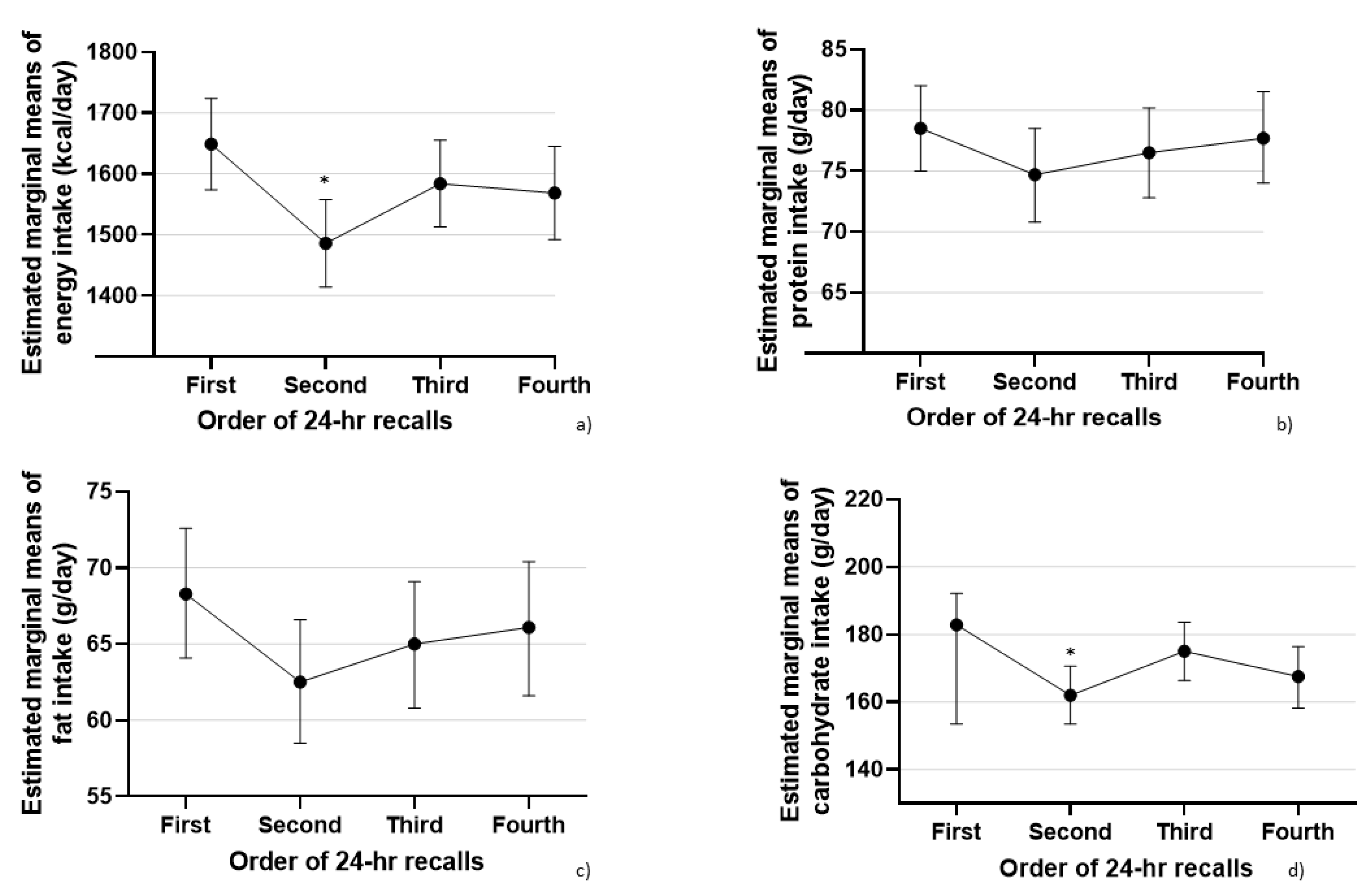
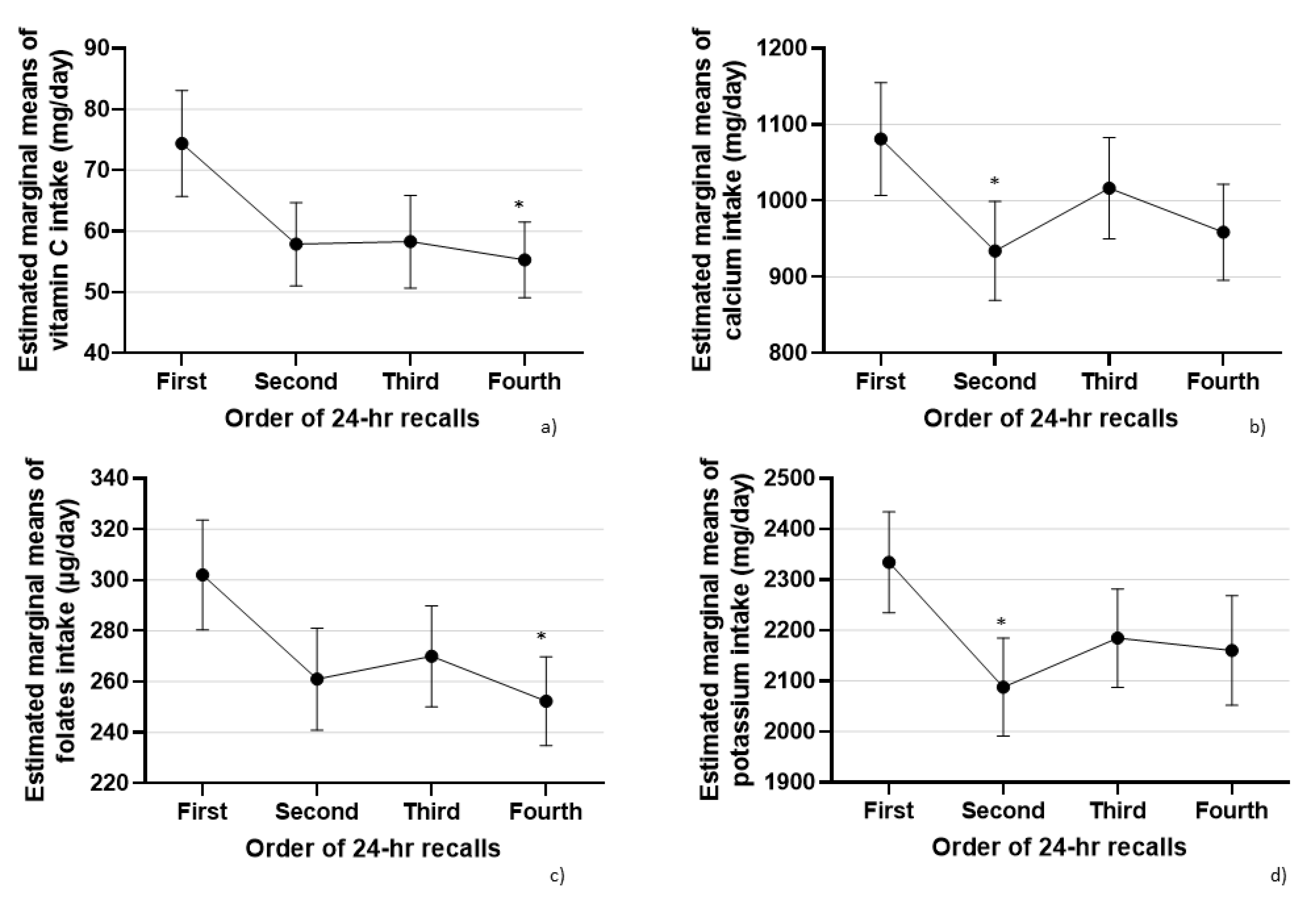
3.1. Model 1: Order of 24-h Recalls and Nutrient Intakes
3.2. Model 2: Weekend vs. Weekday Intakes
3.3. Model 3: Exclusion of the First 24-h Recall
3.4. Model 4: Exclusion of the Second 24-h Recall
3.5. Model 5: Exclusion of the Third 24-h Recall
3.6. Model 6: Exclusion of the Fourth 24-h Recall
4. Discussion
4.1. Misreporting in Food and Drink Consumption
4.2. Controlling for Systematic Bias across Multiple Days
4.3. Controlling for Systematic Bias across Weekday versus Weekend 24-h Dietary Recalls
4.4. Controlling for Systematic Bias across First Time versus Repeated and Face-to-Face versus Phone Call 24-h Dietary Recalls
4.5. Suggestions for Improvement of Repeated 24-h Dietary Recalls Method
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, J.M.; Ingwersen, L.A.; Moshfegh, A.J. Accuracy of dietary recall using the USDA five-step multiple-pass method in men: An observational validation study. J. Am. Diet. Assoc. 2004, 104, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Crispim, S.P.; de Vries, J.H.M.; Geelen, A.; Souverein, O.W.; Hulshof, P.J.M.; Lafay, L.; Rousseau, A.-S.; Lillegaard, I.T.L.; Andersen, L.F.; Huybrechts, I.; et al. Two non-consecutive 24 h recalls using EPIC-Soft software are sufficiently valid for comparing protein and potassium intake between five European centres—Results from the European Food Consumption Validation (EFCOVAL) study. Br. J. Nutr. 2011, 105, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Stote, K.S.; Radecki, S.V.; Moshfegh, A.J.; Ingwersen, L.A.; Baer, D.J. The number of 24 h dietary recalls using the US Department of Agriculture’s automated multiple-pass method required to estimate nutrient intake in overweight and obese adults. Public Health Nutr. 2011, 14, 1736–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, K.A.; Byrne, N.M.; Magarey, A.M.; Hills, A.P. Minimizing random error in dietary intakes assessed by 24-h recall, in overweight and obese adults. Eur. J. Clin. Nutr. 2008, 62, 537–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, R.S.; Charrondiere, U.R.; Bell, W. Measurement Errors in Dietary Assessment Using Self-Reported 24-h Recalls in Low-Income Countries and Strategies for Their Prevention. Adv. Nutr. 2017, 8, 980–991. [Google Scholar] [CrossRef] [Green Version]
- Thompson, F.E.; Kirkpatrick, S.I.; Krebs-Smith, S.M.; Reedy, J.; Schap, T.E.; Subar, A.F.; Wilson, M.M. The National Cancer Institute’s Dietary Assessment Primer: A Resource for Diet Research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, P.; Slimani, N.; Ciampi, A.; Trichopoulou, A.; Naska, A.; Lauria, C.; Veglia, F.; Buenode-Mesquita, H.B.; Ocke, M.C.; Brustad, M.; et al. Evaluation of under- and overreporting of energy intake in the 24-h diet recalls in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2002, 5, 1329–1345. [Google Scholar] [CrossRef] [Green Version]
- Novotny, J.A.; Rumpler, W.V.; Riddick, H.; Hebert, J.R.; Rhodes, D.; Judd, J.T.; Baer, D.J.; McDowell, M.; Briefel, R. Personality characteristics as predictors of underreporting of energy intake on 24-h dietary recall interviews. J. Am. Diet. Assoc. 2003, 103, 1146–1151. [Google Scholar] [CrossRef]
- Johansson, G.; Wikman, Å.; Åhrén, A.-M.; Hallmans, G.; Johansson, I. Underreporting of energy intake in repeated 24-h recalls related to gender, age, weight status, day of interview, educational level, reported food intake, smoking habits and area of living. Public Health Nutr. 2001, 4, 919–927. [Google Scholar] [CrossRef] [Green Version]
- Ard, J.D.; Desmond, R.A.; Allison, D.B.; Conway, J.M. Dietary restraint and disinhibition do not affect accuracy of 24-h recall in a multiethnic population. J. Am. Diet. Assoc. 2006, 106, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Hendrikse, J.J.; Cachia, R.L.; Kothe, E.J.; McPhie, S.; Skouteris, H.; Hayden, M.J. Attentional biases for food cues in overweight and individuals with obesity: A systematic review of the literature. Obes. Rev. 2015, 16, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.; Treffiletti, A.; Bailey, P.E.; Moustafa, A.A. The effect of attentional bias modification training on food intake in overweight and obese women. J. Health Psychol. 2020, 25, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Cui, L.; Sun, X.; Zhang, Q. The effect of attentional bias modification on eating behavior among women craving high-calorie food. Appetite 2018, 129, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Șerban, C.L.; Sima, A.; Hogea, C.M.; Chiriță-Emandi, A.; Perva, I.T.; Vlad, A.; Albai, A.; Nicolae, G.; Putnoky, S.; Timar, R.; et al. Assessment of Nutritional Intakes in Individuals with Obesity under Medical Supervision. A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Software for Dietitians and Nutritionists: Nutrition Analysis, Meal Planning, Communication. Available online: https://nutritioapp.com/ (accessed on 5 April 2019).
- Serafim, V.; Tiugan, D.-A.; Andreescu, N.; Mihailescu, A.; Paul, C.; Velea, I.; Puiu, M.; Niculescu, M.D. Development and Validation of a LC–MS/MS-Based Assay for Quantification of Free and Total Omega 3 and 6 Fatty Acids from Human Plasma. Molecules 2019, 24, 360. [Google Scholar] [CrossRef] [Green Version]
- Phillips, D.L.; Pirkle, J.L.; Burse, V.W.; Bernert, J.T.; Henderson, L.O.; Needham, L.L. Chlorinated hydrocarbon levels in human serum: Effects of fasting and feeding. Arch. Environ. Contam. Toxicol. 1989, 18, 495–500. [Google Scholar] [CrossRef]
- False Discovery Rate Online Calculator|Tools. Available online: https://tools.carbocation.com/FDR (accessed on 10 October 2019).
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Heitmann, B.L.; Lissner, L. Dietary underreporting by obese individuals—Is it specific or non-specific? BMJ 1995, 311, 986–989. [Google Scholar] [CrossRef] [Green Version]
- Lopes, T.S.; Luiz, R.R.; Hoffman, D.J.; Ferriolli, E.; Pfrimer, K.; Moura, A.S.; Sichieri, R.; Pereira, R.A. Misreport of energy intake assessed with food records and 24-h recalls compared with total energy expenditure estimated with DLW. Eur. J. Clin. Nutr. 2016, 70, 1259–1264. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Kipnis, V.; Troiano, R.P.; Midthune, D.; Schoeller, D.A.; Bingham, S.; Sharbaugh, C.O.; Trabulsi, J.; Runswick, S.; Ballard-Barbash, R.; et al. Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN study. Am. J. Epidemiol. 2003, 158, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Poslusna, K.; Ruprich, J.; de Vries, J.H.M.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 h recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101, S73–S85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossato, S.L.; Fuchs, S.C. Handling random errors and biases in methods used for short-term dietary assessment. Rev. Saúde Pública 2014, 48, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Validation|Dietary Assessment Primer. Available online: https://dietassessmentprimer.cancer.gov/profiles/recall/validation.html (accessed on 3 August 2020).
- Arab, L.; Wesseling-Perry, K.; Jardack, P.; Henry, J.; Winter, A. Eight Self-Administered 24-h Dietary Recalls Using the Internet are Feasible in African Americans and Caucasians: The Energetics Study. J. Am. Diet. Assoc. 2010, 110, 857–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whybrow, S.; Horgan, G.W.; Macdiarmid, J.I. Self-reported food intake decreases over recording period in the National Diet and Nutrition Survey. Br. J. Nutr. 2020, 124, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galasso, R.; Panico, S.; Celentano, E.; Del Pezzo, M. Relative validity of multiple telephone versus face-to-face 24-h dietary recalls. Ann. Epidemiol. 1994, 4, 332–336. [Google Scholar] [CrossRef]
- Tran, K.M.; Johnson, R.K.; Soultanakis, R.P.; Matthews, D.E. In-person vs Telephone-administered Multiple-pass 24-h Recalls in Women: Validation with Doubly Labeled Water. J. Am. Diet. Assoc. 2000, 100, 777–783. [Google Scholar] [CrossRef]
- Bogle, M.; Stuff, J.; Davis, L.; Forrester, I.; Strickland, E.; Casey, P.H.; Ryan, D.; Champagne, C.; McGee, B.; Mellad, K.; et al. Validity of a telephone-administered 24-h dietary recall in telephone and non-telephone households in the rural Lower Mississippi Delta region. J. Am. Diet. Assoc. 2001, 101, 216–222. [Google Scholar] [CrossRef]
- Brustad, M.; Skeie, G.; Braaten, T.; Slimani, N.; Lund, E. Comparison of telephone vs face-to-face interviews in the assessment of dietary intake by the 24 h recall EPIC SOFT program--the Norwegian calibration study. Eur. J. Clin. Nutr. 2003, 57, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Brassard, D.; Laramée, C.; Robitaille, J.; Lemieux, S.; Lamarche, B. Differences in Population-Based Dietary Intake Estimates Obtained From an Interviewer-Administered and a Self-Administered Web-Based 24-h Recall. Front. Nutr. 2020, 7, 137. [Google Scholar] [CrossRef] [PubMed]
- Rothausen, B.W.; Matthiessen, J.; Hoppe, C.; Brockhoff, P.B.; Andersen, L.F.; Tetens, I. Differences in Danish children’s diet quality on weekdays v. weekend days. Public Health Nutr. 2012, 15, 1653–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothausen, B.W.; Matthiessen, J.; Andersen, L.F.; Brockhoff, P.B.; Tetens, I. Dietary patterns on weekdays and weekend days in 4-14-year-old Danish children. Br. J. Nutr. 2013, 109, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Czlapka-Matyasik, M.; Lonnie, M.; Wadolowska, L.; Frelich, A. “Cutting Down on Sugar” by Non-Dieting Young Women: An Impact on Diet Quality on Weekdays and the Weekend. Nutrients 2018, 10, 1463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahns, L.; Conrad, Z.; Johnson, L.K.; Scheett, A.J.; Stote, K.S.; Raatz, S.K. Diet Quality Is Lower and Energy Intake Is Higher on Weekends Compared with Weekdays in Midlife Women: A 1-Year Cohort Study. J. Acad. Nutr. Diet. 2017, 117, 1080–1086.e1. [Google Scholar] [CrossRef] [PubMed]
- An, R. Weekend-weekday differences in diet among U.S. adults, 2003–2012. Ann. Epidemiol. 2016, 26, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Haines, P.S.; Hama, M.Y.; Guilkey, D.K.; Popkin, B.M. Weekend eating in the United States is linked with greater energy, fat, and alcohol intake. Obes. Res. 2003, 11, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.H.W.; Black, J.L.; Barr, S.I.; Vatanparast, H. Examining differences in nutrient intake and dietary quality on weekdays versus weekend days in Canada. Appl. Physiol. Nutr. Metab. 2014, 39, 1413–1417. [Google Scholar] [CrossRef]
- Racette, S.B.; Weiss, E.P.; Schechtman, K.B.; Steger-May, K.; Villareal, D.T.; Obert, K.A.; Holloszy, J.O. Influence of Weekend Lifestyle Patterns on Body Weight. Obesity 2008, 16, 1826–1830. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Male (n1 = 189) | Female (n2 = 197) | Total (n = 386) |
|---|---|---|---|
| Age (years) * | 54.0 (29.0) | 57.0 (19.0) | 56.0 (23.0) |
| BMI (kg/m2) * | 33.9 (14.2) | 36.7 (14.7) | 35.2 (14.7) |
| Abdominal circumference (cm) * | 119.0 (30.0) | 117.0 (27.5) | 118.0 (29.0) |
| TSL (g/L) * | 6.9 (5.2) | 7.0 (5.5) | 7.0 (5.4) |
| Diabetes mellitus ** | 123 (65.1%) | 148 (75.1%) | 271 (70.2%) |
| Type II diabetes mellitus ** | 107 (56.6%) | 137 (69.5%) | 244 (68.7%) |
| Hypercholesterolemia ** | 132 (69.8%) | 139 (70.6%) | 271 (63.2%) |
| Hypertriglyceridemia ** | 59 (31.2%) | 37 (18.9%) | 96 (24.9%) |
| Arterial hypertension ** | 112 (60.5%) | 130 (66.3%) | 242 (63.5%) |
| Hepatic steatosis ** | 43 (22.8%) | 54 (27.4%) | 97 (25.1%) |
| Nutrients | Mean of First 24-h Recall and 95% CI of the Mean | Mean of Second 24-h Recall and 95% CI of the Mean | Mean of Third 24-h Recall and 95% CI of the Mean | Mean of Fourth 24-h Recall and 95% CI of the Mean | ||||
|---|---|---|---|---|---|---|---|---|
| Energy (kcal) | 1641.7 | 1557.7–1725.7 | 1480.4 | 1401.2–1559.5 | 1578.3 | 1498.5–1658.1 | 1561.6 | 1475.7–1647.6 |
| Protein (g) | 78.1 | 74.3–82.0 | 74.4 | 70.2–78.6 | 76.3 | 72.3–80.3 | 77.4 | 73.3–81.5 |
| Fat (g) | 68.0 | 63.4–72.6 | 62.2 | 57.8–66.6 | 64.7 | 60.2–69.2 | 65.7 | 61.0–70.4 |
| Carbohydrates (g) | 182.1 | 172.0–192.2 | 161.5 | 152.4–170.6 | 174.5 | 165.2–183.8 | 166.9 | 157.0–176.8 |
| Vitamin C (mg) | 74.0 | 65.0–83.0 | 57.6 | 50.6–64.6 | 58.2 | 50.5–65.9 | 55.1 | 48.8–61.4 |
| Vitamin D (IU) | 67.6 | 58.6–76.6 | 65.6 | 52.8–78.5 | 82.3 | 65.7–99.0 | 70.2 | 58.8–81.6 |
| Vitamin A (µg) | 602.4 | 480.1–724.7 | 599.0 | 490.1–708.0 | 594.0 | 480.2–707.8 | 499.6 | 412.8–586.3 |
| Iron (mg) | 12.3 | 11.5–13.0 | 11.3 | 10.5–12.0 | 11.8 | 11.0–12.5 | 11.4 | 10.6–12.2 |
| Calcium (mg) | 1078.2 | 1002.4–1153.9 | 931.2 | 864.5–998.0 | 1013.9 | 945.4–1082.3 | 955.4 | 889.6–1021.1 |
| Magnesium (mg) | 241.8 | 225.5–258.2 | 223.2 | 208.3–238.0 | 224.7 | 211.3–238.0 | 216.6 | 202.1–231.0 |
| Total water (g) | 2704.5 | 2590.5–2818.5 | 2528.8 | 2426.1–2631.5 | 2664.3 | 2567.6–2760.9 | 2615.8 | 2510.2–2721.4 |
| Fiber (g) | 17.3 | 16.3–18.4 | 15.4 | 14.4–16.4 | 16.2 | 15.0–17.3 | 15.8 | 14.6–16.9 |
| Vitamin K (µg) | 96.7 | 78.4–115.0 | 78.0 | 64.5–91.4 | 76.6 | 63.1–90.0 | 70.5 | 60.2–80.8 |
| Thiamine (mg) | 1.5 | 1.4–1.6 | 1.4 | 1.3–1.5 | 1.4 | 1.3–1.5 | 1.4 | 1.3–1.5 |
| Riboflavin (mg) | 1.3 | 1.2–1.4 | 1.2 | 1.2–1.3 | 1.3 | 1.2–1.4 | 1.2 | 1.1–1.2 |
| Niacin (mg) | 17.2 | 16.0–18.4 | 16.8 | 15.5–18.2 | 17.0 | 15.7–18.3 | 16.2 | 15.1–17.4 |
| Vitamin B6 (mg) | 1.4 | 1.3–1.5 | 1.4 | 1.2–1.5 | 1.3 | 1.2–1.4 | 1.3 | 1.2–1.4 |
| Folates (µg) | 300.7 | 278.2–323.3 | 260.1 | 239.2–280.9 | 268.9 | 248.2–289.7 | 251.3 | 232.9–269.6 |
| Vitamin B12 (µg) | 3.6 | 3.0–4.1 | 3.9 | 3.2–4.5 | 4.0 | 3.4–4.7 | 3.8 | 3.2–4.4 |
| Pantothenic acid (mg) | 4.1 | 3.8–4.3 | 3.9 | 3.6–4.2 | 4.0 | 3.7–4.2 | 3.6 | 3.4–3.9 |
| Betaine (mg) | 32.0 | 14.6–49.5 | 14.9 | 11.6–18.2 | 18.9 | 9.1–28.7 | 14.1 | 11.4–16.7 |
| Choline (mg) | 250.3 | 234.0–266.6 | 224.7 | 206.7–242.7 | 245.0 | 226.5–263.5 | 253.3 | 234.0–272.6 |
| Copper (mg) | 1.0 | 0.9–1.1 | 0.9 | 0.9–1.0 | 0.9 | 0.9–1.0 | 0.9 | 0.8–1.0 |
| Fluor (µg) | 444.1 | 380.6–507.6 | 386.2 | 329.8–442.6 | 403.4 | 344.6–462.2 | 336.3 | 282.9–389.8 |
| Phosphor (mg) | 952.4 | 896.7–1008.0 | 886.5 | 831.3–941.7 | 917.4 | 864.5–970.2 | 884.5 | 829.2–939.7 |
| Manganese (mg) | 2.0 | 1.8–2.2 | 2.4 | 1.1–3.7 | 2.0 | 1.6–2.3 | 2.1 | 1.5–2.8 |
| Selenium (µg) | 80.5 | 75.0–85.9 | 78.0 | 72.3–83.6 | 82.1 | 76.6–87.7 | 78.0 | 72.6–83.4 |
| Zinc (mg) | 7.1 | 6.6–7.5 | 6.7 | 6.2–7.3 | 6.7 | 6.3–7.2 | 6.6 | 6.1–7.2 |
| Potassium (mg) | 2327.1 | 2221.2–2432.9 | 2081.4 | 1978.7–2184.0 | 2179.7 | 2077.9–2281.5 | 2153.8 | 2040.4–2267.3 |
| Sodium (mg) | 3428.5 | 3195.0–3662.1 | 3072.6 | 2860.6–3284.5 | 3246.3 | 3039.0–3453.6 | 3212.7 | 3005.2–3420.3 |
| EPA (mg) | 0.0 | 0.0–0.0 | 0.0 | 0.0–0.1 | 0.0 | 0.0–0.1 | 0.0 | 0.0–0.0 |
| DHA (mg) | 0.1 | 0.0–0.1 | 0.1 | 0.0–0.1 | 0.1 | 0.1–0.1 | 0.1 | 0.0–0.1 |
| Vitamin E (g) | 4.8 | 4.4–5.3 | 4.8 | 4.4–5.3 | 4.5 | 4.1–4.9 | 4.3 | 3.9–4.7 |
| LA (g) | 3.1 | 2.5–3.6 | 2.7 | 2.2–3.2 | 3.2 | 2.8–3.7 | 3.1 | 2.6–3.6 |
| ALA (g) | 0.3 | 0.2–0.4 | 0.3 | 0.2–0.3 | 0.3 | 0.3–0.4 | 0.3 | 0.3–0.4 |
| Fatty acids total saturated (g) | 24.0 | 22.1–25.9 | 21.4 | 19.7–23.1 | 22.6 | 20.8–24.4 | 22.5 | 20.7–24.3 |
| Sugars total (g) | 52.7 | 48.5–56.9 | 46.3 | 42.5–50.1 | 49.4 | 44.7–54.1 | 44.3 | 40.3–48.3 |
| Nutrients | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|
| Weekend | Weekday | Weekend | Weekday | |||||
| Mean | 95% Confidence Interval | Mean | 95% Confidence Interval | Mean | 95% Confidence Interval | Mean | 95% Confidence Interval | |
| Energy (kcal) | 1989.2 | 1841.2–2137.3 | 1807.8 | 1704.2–1911.5 | 1305.1 | 1232.8–1377.4 | 1288.0 | 1219.5–1356.5 |
| Protein (g) | 95.3 | 88.9–101.6 | 87.4 | 83.0–91.9 | 65.1 | 60.9–69.4 | 64.1 | 60.5–67.6 |
| Fat (g) | 84.8 | 76.7–92.9 | 76.7 | 71.3–82.0 | 53.6 | 49.5–57.8 | 51.9 | 48.1–55.7 |
| Carbohydrates (g) | 206.2 | 188.3–224.0 | 193.2 | 181.7–204.7 | 146.9 | 137.6–156.2 | 147.5 | 139.3–155.6 |
| Vitamin C (mg) | 64.4 | 52.7–76.1 | 71.9 | 63.6–80.2 | 53.9 | 45.3–62.6 | 52.5 | 46.8–58.3 |
| Vitamin D (IU) | 90.1 | 69.3–110.8 | 87.9 | 73.8–101.9 | 55.5 | 44.2–66.8 | 55.3 | 47.0–63.5 |
| Vitamin A (µg) | 545.8 | 432.6–659.0 | 693.3 | 570.9–815.6 | 410.3 | 344.4–476.2 | 523.6 | 443.2–604.0 |
| Iron (mg) | 14.0 | 12.6–15.3 | 13.3 | 12.5–14.1 | 9.5 | 8.7–10.2 | 10.1 | 9.5–10.8 |
| Calcium (mg) | 1113.4 | 1002.3–1224.4 | 1122.3 | 1044.3–1200.3 | 798.7 | 722.3–875.1 | 901.2 | 835.9–966.5 |
| Magnesium (mg) | 263.8 | 240.1–287.5 | 261.3 | 244.6–278.0 | 188.7 | 171.9–205.5 | 194.4 | 182.2–206.6 |
| Total water (g) | 2811.3 | 2646.3–2976.4 | 2854.1 | 2734.9–2973.2 | 2397.8 | 2264.4–2531.2 | 2432.9 | 2329.2–2536.6 |
| Fiber (g) | 18.8 | 16.7–20.9 | 18.2 | 17.1–19.4 | 13.6 | 12.6–14.6 | 14.2 | 13.3–15.2 |
| Vitamin K (µg) | 80.9 | 63.6–98.2 | 97.9 | 82.0–113.7 | 71.0 | 53.2–88.8 | 66.9 | 55.4–78.3 |
| Thiamine (mg) | 1.7 | 1.6–1.9 | 1.6 | 1.5–1.7 | 1.2 | 1.1–1.2 | 1.2 | 1.1–1.3 |
| Riboflavin (mg) | 1.4 | 1.3–1.6 | 1.4 | 1.3–1.5 | 1.0 | 0.9–1.1 | 1.1 | 1.0–1.2 |
| Niacin (mg) | 21.0 | 19.0–23.1 | 19.5 | 18.2–20.9 | 13.9 | 12.6–15.1 | 13.9 | 12.8–14.9 |
| Vitamin B6 (mg) | 1.7 | 1.6–1.9 | 1.6 | 1.5–1.7 | 1.1 | 1.0–1.2 | 1.1 | 1.0–1.2 |
| Folates (µg) | 305.7 | 276.2–335.2 | 318.0 | 293.9–342.1 | 209.7 | 190.4–229.1 | 233.9 | 216.7–251.1 |
| Vitamin B12 (µg) | 4.4 | 3.6–5.3 | 4.8 | 4.1–5.4 | 3.0 | 2.3–3.8 | 3.0 | 2.5–3.4 |
| Pantothenic acid (mg) | 4.5 | 4.1–4.9 | 4.3 | 4.1–4.6 | 3.4 | 3.1–3.6 | 3.5 | 3.3–3.7 |
| Betaine (mg) | 19.6 | 14.2–25.0 | 23.0 | 13.2–32.8 | 14.6 | 10.7–18.6 | 19.0 | 6.5–31.5 |
| Choline (mg) | 308.8 | 278.5–339.1 | 277.2 | 257.0–297.5 | 211.3 | 192.9–229.7 | 201.1 | 187.3–214.9 |
| Copper (mg) | 1.1 | 1.0–1.2 | 1.1 | 1.0–1.1 | 0.9 | 0.8–0.9 | 0.8 | 0.8–0.9 |
| Fluor (µg) | 422.4 | 335.7–509.2 | 442.4 | 373.4–511.3 | 356.1 | 285.7–426.5 | 347.9 | 289.3–406.4 |
| Phosphor (mg) | 1112.4 | 1024.1–1200.7 | 1042.4 | 976.8–1108.0 | 762.9 | 708.5–817.4 | 769.7 | 723.0–816.4 |
| Manganese (mg) | 2.3 | 1.9–2.6 | 2.1 | 1.9–2.4 | 2.4 | 1.1–3.6 | 2.0 | 1.1–2.9 |
| Selenium (µg) | 101.0 | 92.4–109.6 | 92.9 | 87.3–98.6 | 65.3 | 59.3–71.3 | 65.0 | 60.3–69.7 |
| Zinc (mg) | 8.3 | 7.5–9.1 | 7.9 | 7.4–8.4 | 5.8 | 5.2–6.3 | 5.6 | 5.3–6.0 |
| Potassium (mg) | 2551.5 | 2372.8–2730.2 | 3832.9 | 3566.6–4099.3 | 1983.5 | 1862.5–2104.5 | 2630.1 | 2463.3–2796.9 |
| Sodium (mg) | 4003.6 | 3674.3–4332.8 | 2417.1 | 2294.1–2540.1 | 2655.4 | 2450.5–2860.3 | 1916.9 | 1828.8–2005.1 |
| EPA (mg) | 0.0 | 0.0–0.1 | 0.0 | 0.0–0.1 | 0.0 | 0.0–0.1 | 0.0 | 0.0–0.0 |
| DHA (mg) | 0.1 | 0.1–0.1 | 0.1 | 0.1–0.1 | 0.1 | 0.0–0.1 | 0.0 | 0.0–0.1 |
| Vitamin E (g) | 5.3 | 4.5–6.0 | 5.1 | 4.7–5.6 | 4.3 | 3.6–4.9 | 4.1 | 3.8–4.4 |
| LA (g) | 3.6 | 2.8–4.4 | 3.1 | 2.5–3.6 | 3.1 | 2.5–3.7 | 2.8 | 2.3–3.3 |
| ALA (g) | 0.4 | 0.3–0.5 | 0.4 | 0.3–0.5 | 0.3 | 0.2–0.3 | 0.2 | 0.2–0.3 |
| Fatty acids total saturated (g) | 29.2 | 26.0–32.3 | 26.6 | 24.4–28.7 | 17.4 | 15.8–18.9 | 18.5 | 17.0–20.1 |
| Sugars total (g) | 52.0 | 44.7–59.4 | 52.6 | 47.4–57.8 | 44.0 | 39.7–48.2 | 44.2 | 40.7–47.7 |
| Nutrients | Difference between Mean of Four 24-h Recall and Mean of Three 24-h Recall after Exclusion of: | |||||||
|---|---|---|---|---|---|---|---|---|
| First 24-h Recall | Second 24-h Recall | Third 24-h Recall | Fourth 24-h Recall | |||||
| Size Effect r | p-Value | Size Effect r | p-Value | Size Effect r | p-Value | Size Effect r | p-Value | |
| Energy (kcal) | 0.12 | 0.018 | 0.21 | <0.001 * | 0.02 | 0.738 | 0.05 | 0.312 |
| Protein (g) | 0.03 | 0.528 | 0.13 | 0.010 * | 0.04 | 0.402 | 0.00 | 0.951 |
| Fat (g) | 0.07 | 0.159 | 0.15 | 0.003 * | 0.06 | 0.216 | 0.07 | 0.179 |
| Carbohydrates (g) | 0.12 | 0.023 | 0.24 | <0.001 * | 0.00 | 0.952 | 0.10 | 0.040 |
| Vitamin C (mg) | 0.11 | 0.034 | 0.16 | 0.001 * | 0.18 | <0.001 * | 0.18 | <0.001 * |
| Vitamin D (IU) | 0.08 | 0.128 | 0.26 | <0.001 * | 0.01 | 0.900 | 0.12 | 0.021 * |
| Vitamin A (µg) | 0.02 | 0.740 | 0.05 | 0.355 | 0.10 | 0.061 | 0.25 | <0.001 * |
| Iron (mg) | 0.09 | 0.076 | 0.16 | 0.001 * | 0.03 | 0.506 | 0.14 | 0.005 * |
| Calcium (mg) | 0.11 | 0.034 | 0.18 | <0.001 * | 0.02 | 0.666 | 0.13 | 0.008 * |
| Magnesium (mg) | 0.07 | 0.176 | 0.11 | 0.029 * | 0.05 | 0.292 | 0.15 | 0.004 * |
| Total water (g) | 0.09 | 0.075 | 0.11 | 0.028 * | 0.04 | 0.376 | 0.02 | 0.735 |
| Fiber (g) | 0.14 | 0.006 * | 0.18 | <0.001 * | 0.06 | 0.255 | 0.13 | 0.010 * |
| Vitamin K (µg) | 0.06 | 0.258 | 0.17 | 0.001 * | 0.15 | 0.003 * | 0.20 | <0.001 * |
| Thiamine (mg) | 0.08 | 0.131 | 0.11 | 0.032 | 0.09 | 0.088 | 0.12 | 0.016 * |
| Riboflavin (mg) | 0.08 | 0.139 | 0.10 | 0.056 | 0.04 | 0.431 | 0.22 | <0.001 * |
| Niacin (mg) | 0.01 | 0.796 | 0.08 | 0.135 | 0.06 | 0.256 | 0.08 | 0.117 |
| Vitamin B6 (mg) | 0.01 | 0.877 | 0.08 | 0.137 | 0.10 | 0.056 | 0.06 | 0.252 |
| Folates (µg) | 0.16 | 0.002 * | 0.19 | <0.001 * | 0.09 | 0.080 | 0.18 | 0.001 * |
| Vitamin B12 (µg) | 0.14 | 0.004 ** | 0.17 | 0.001 * | 0.08 | 0.095 | 0.12 | 0.014 * |
| Pantothenic acid (mg) | 0.05 | 0.287 | 0.06 | 0.216 | 0.03 | 0.564 | 0.18 | <0.001 * |
| Betaine (mg) | 0.05 | 0.352 | 0.27 | <0.001 * | 0.19 | <0.001 * | 0.19 | <0.001 * |
| Choline (mg) | 0.01 | 0.790 | 0.24 | <0.001 * | 0.06 | 0.234 | 0.01 | 0.900 |
| Copper (mg) | 0.06 | 0.227 | 0.12 | 0.020 * | 0.03 | 0.521 | 0.18 | <0.001 * |
| Fluor (µg) | 0.06 | 0.259 | 0.10 | 0.051 | 0.07 | 0.184 | 0.22 | <0.001 * |
| Phosphor (mg) | 0.07 | 0.154 | 0.11 | 0.027 * | 0.02 | 0.642 | 0.11 | 0.032 * |
| Manganese (mg) | 0.00 | 0.922 | 0.12 | 0.015 * | 0.01 | 0.860 | 0.19 | <0.001 * |
| Selenium (µg) | 0.01 | 0.775 | 0.07 | 0.169 | 0.00 | 0.940 | 0.06 | 0.206 |
| Zinc (mg) | 0.07 | 0.188 | 0.09 | 0.071 | 0.05 | 0.308 | 0.11 | 0.025 * |
| Potassium (mg) | 0.16 | 0.001* | 0.20 | <0.001 * | 0.06 | 0.265 | 0.08 | 0.121 |
| Sodium (mg) | 0.06 | 0.276 | 0.17 | 0.001 * | 0.05 | 0.371 | 0.04 | 0.433 |
| EPA (mg) | 0.25 | <0.001 ** | 0.19 | <0.001 * | 0.15 | 0.002 * | 0.16 | 0.002 * |
| DHA (mg) | 0.24 | <0.001 ** | 0.20 | <0.001 * | 0.18 | <0.001 * | 0.16 | 0.002 * |
| Sugars total (g) | 0.10 | 0.051 | 0.15 | 0.004 * | 0.05 | 0.310 | 0.19 | <0.001 * |
| Vitamin E (g) | 0.01 | 0.885 | 0.08 | 0.118 | 0.10 | 0.048 | 0.18 | <0.001 * |
| Fatty acids total saturated (g) | 0.07 | 0.180 | 0.19 | <0.001 * | 0.06 | 0.226 | 0.09 | 0.068 |
| LA (g) | 0.12 | 0.014 | 0.23 | <0.001 * | 0.04 | 0.451 | 0.09 | 0.062 |
| ALA (g) | 0.18 | 0.001 ** | 0.27 | <0.001 * | 0.05 | 0.349 | 0.11 | 0.027 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serban, C.L.; Chirita-Emandi, A.; Perva, I.T.; Sima, A.; Andreescu, N.; Putnoky, S.; Niculescu, M.D.; Puiu, M. Intake Differences between Subsequent 24-h Dietary Recalls Create Significant Reporting Bias in Adults with Obesity. Appl. Sci. 2022, 12, 2728. https://doi.org/10.3390/app12052728
Serban CL, Chirita-Emandi A, Perva IT, Sima A, Andreescu N, Putnoky S, Niculescu MD, Puiu M. Intake Differences between Subsequent 24-h Dietary Recalls Create Significant Reporting Bias in Adults with Obesity. Applied Sciences. 2022; 12(5):2728. https://doi.org/10.3390/app12052728
Chicago/Turabian StyleSerban, Costela Lacrimioara, Adela Chirita-Emandi, Iulia Teodora Perva, Alexandra Sima, Nicoleta Andreescu, Salomeia Putnoky, Mihai Dinu Niculescu, and Maria Puiu. 2022. "Intake Differences between Subsequent 24-h Dietary Recalls Create Significant Reporting Bias in Adults with Obesity" Applied Sciences 12, no. 5: 2728. https://doi.org/10.3390/app12052728
APA StyleSerban, C. L., Chirita-Emandi, A., Perva, I. T., Sima, A., Andreescu, N., Putnoky, S., Niculescu, M. D., & Puiu, M. (2022). Intake Differences between Subsequent 24-h Dietary Recalls Create Significant Reporting Bias in Adults with Obesity. Applied Sciences, 12(5), 2728. https://doi.org/10.3390/app12052728