
Neuromuscular Stimulation as an Intervention Tool for Recovery from Upper Limb Paresis after Stroke and the Neural Basis


Abstract
:1. Introduction
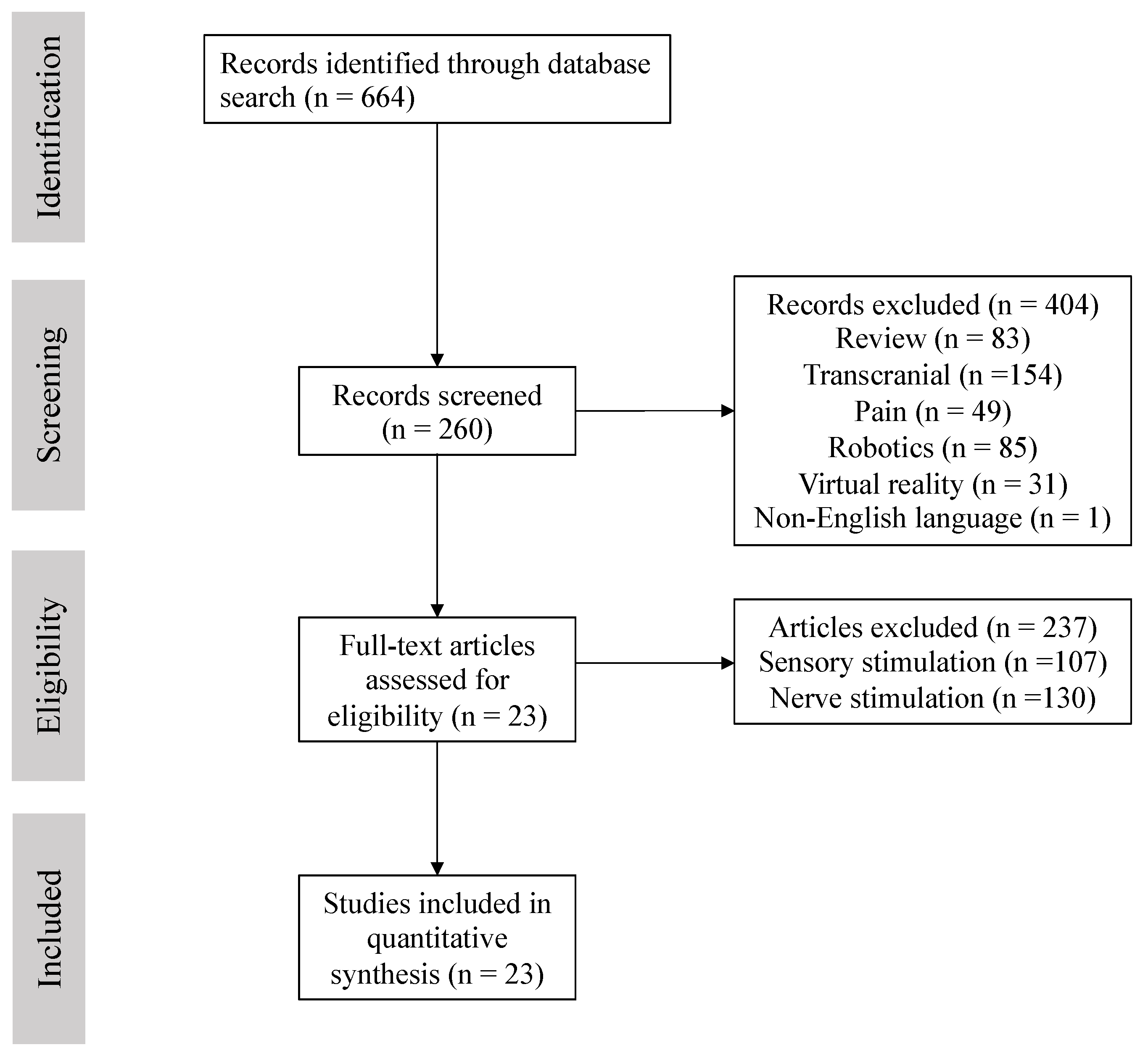
2. Materials and Methods
Search Strategy
3. Results
3.1. Heterogeneous NMES Conditions
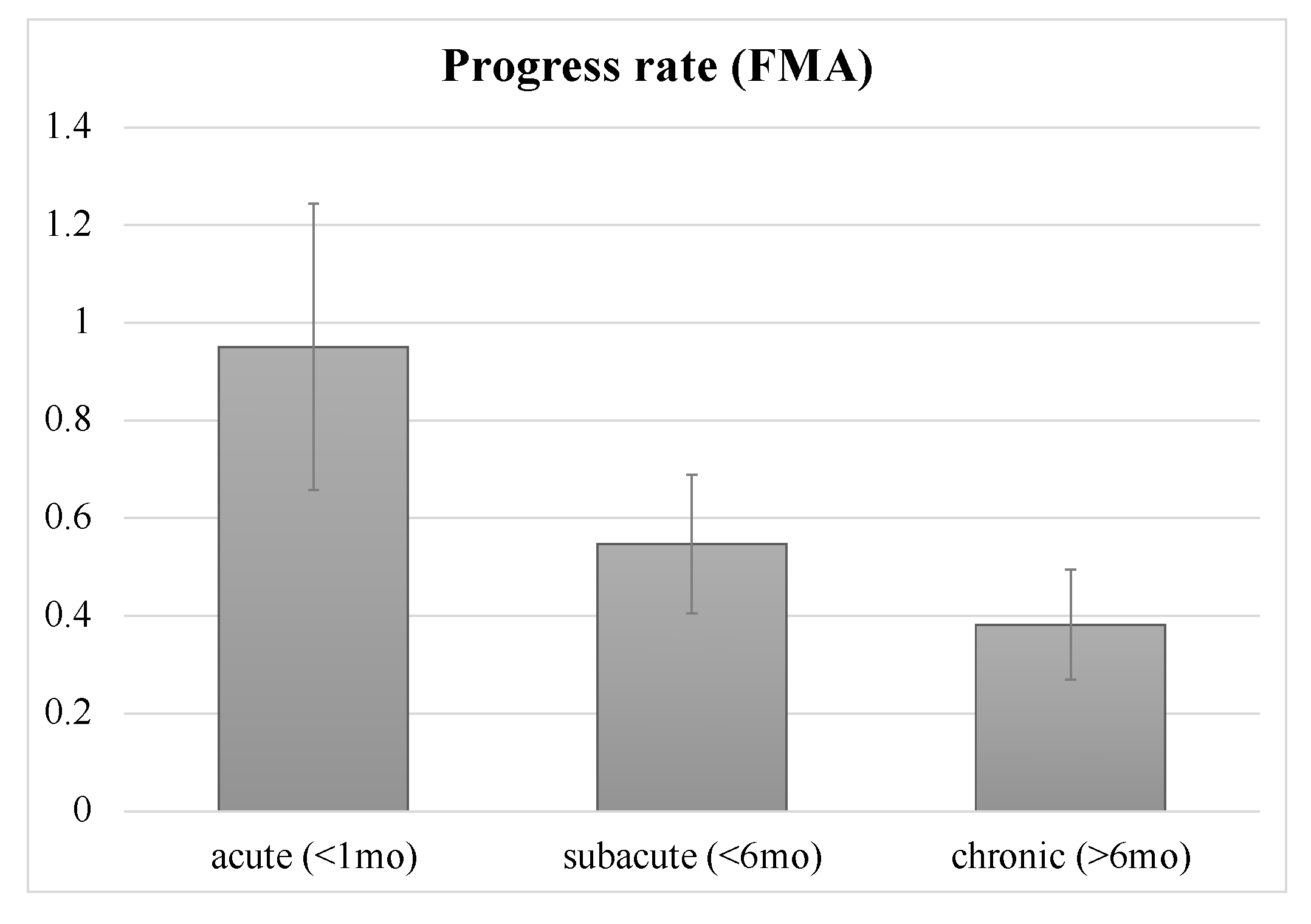
3.2. Effects of Time Post-Stroke on NMES Benefits
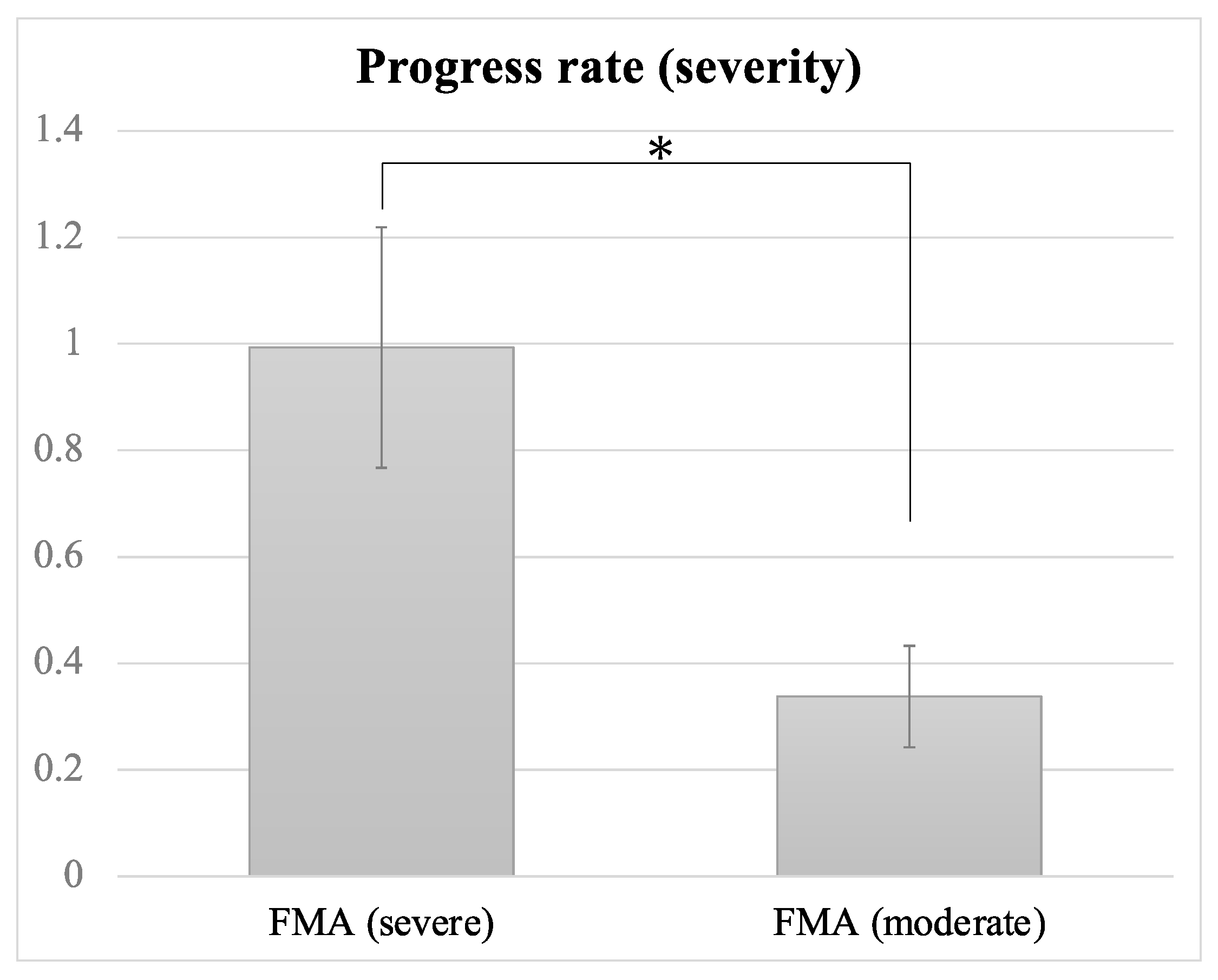
3.3. Influence of Stroke Severity
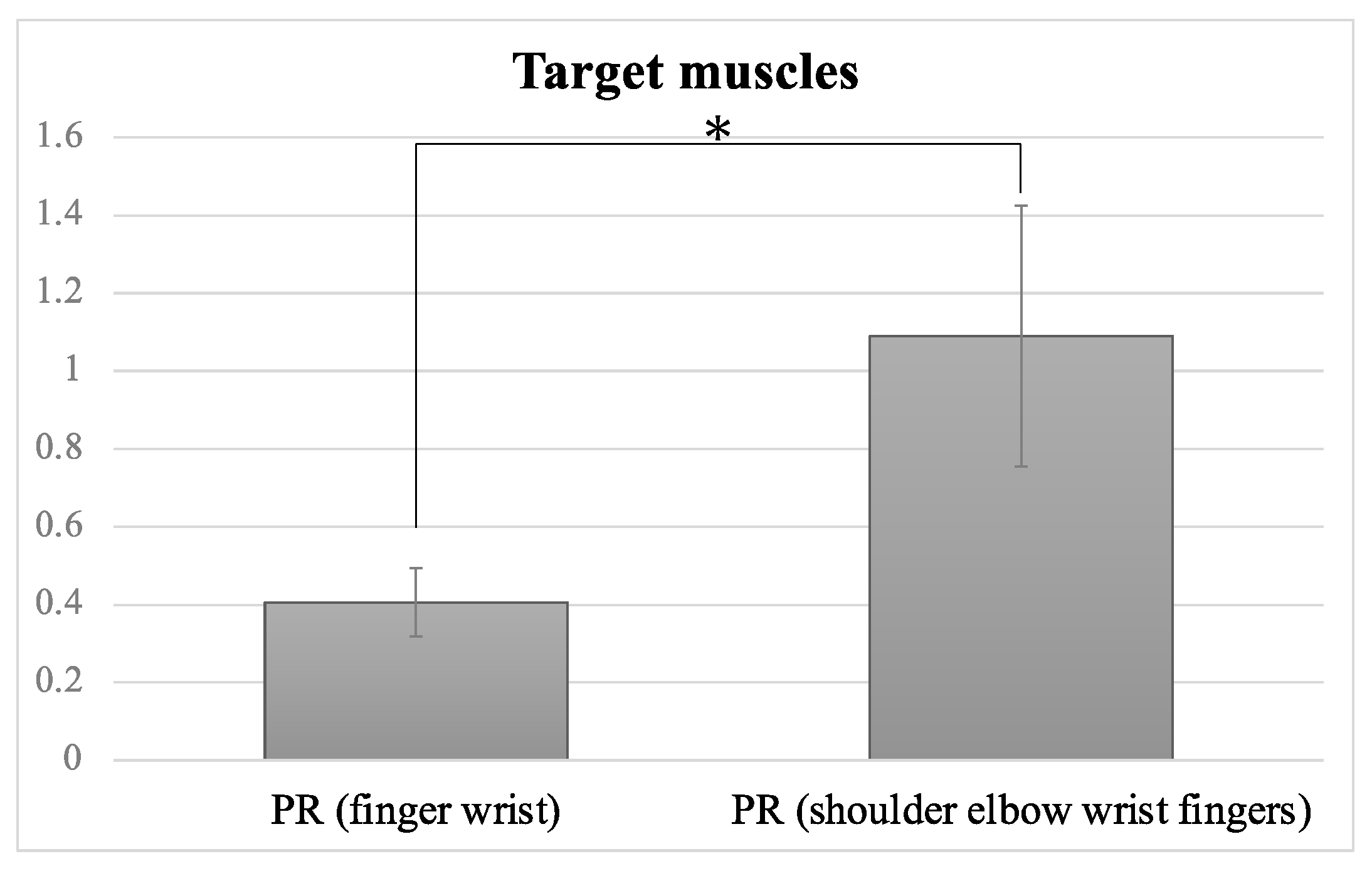
3.4. Target Muscles: Whole UE Versus Wrist/Finger Extensors
3.5. Influence of Dose and Duration on NMES Benefit
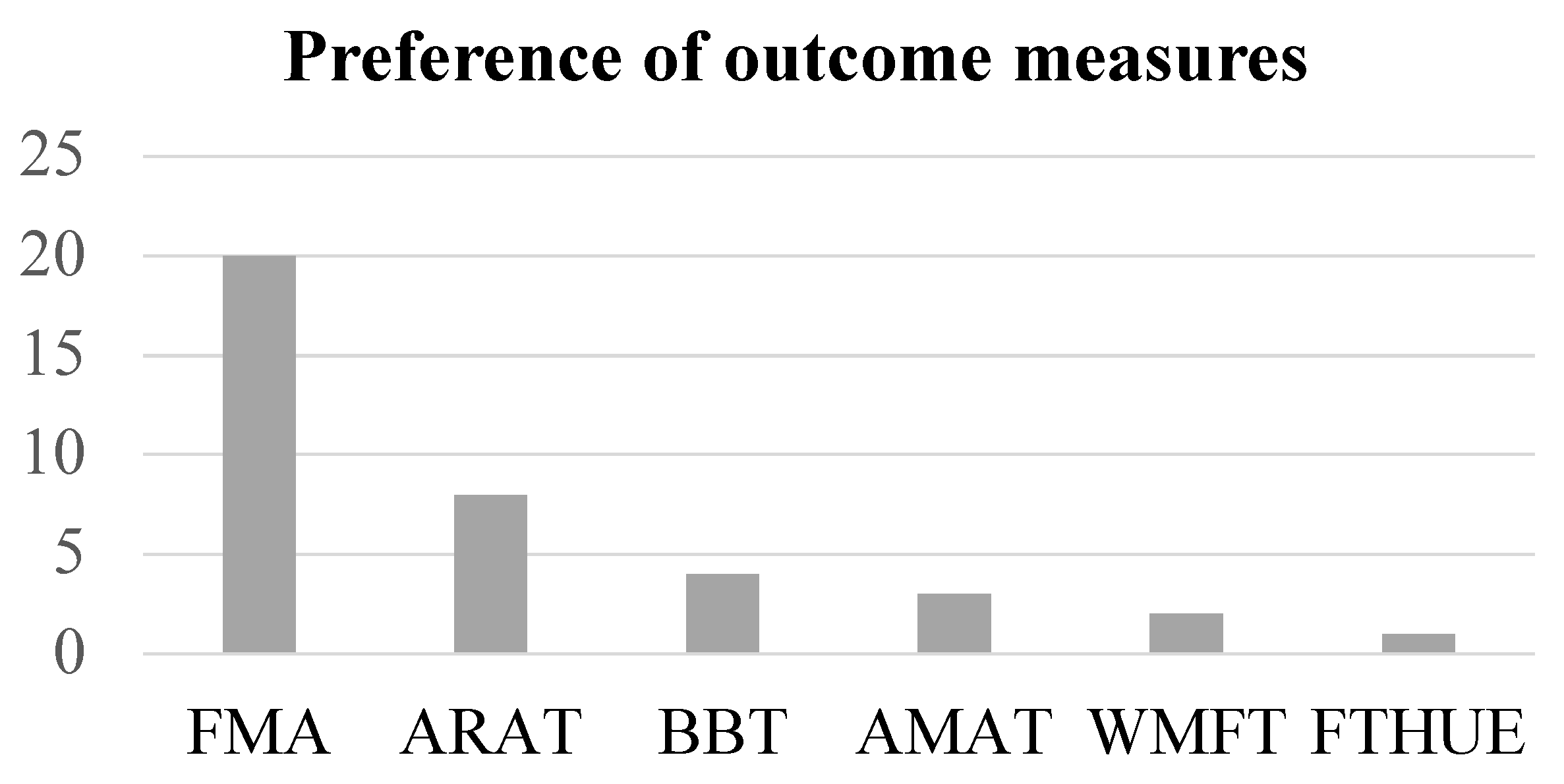
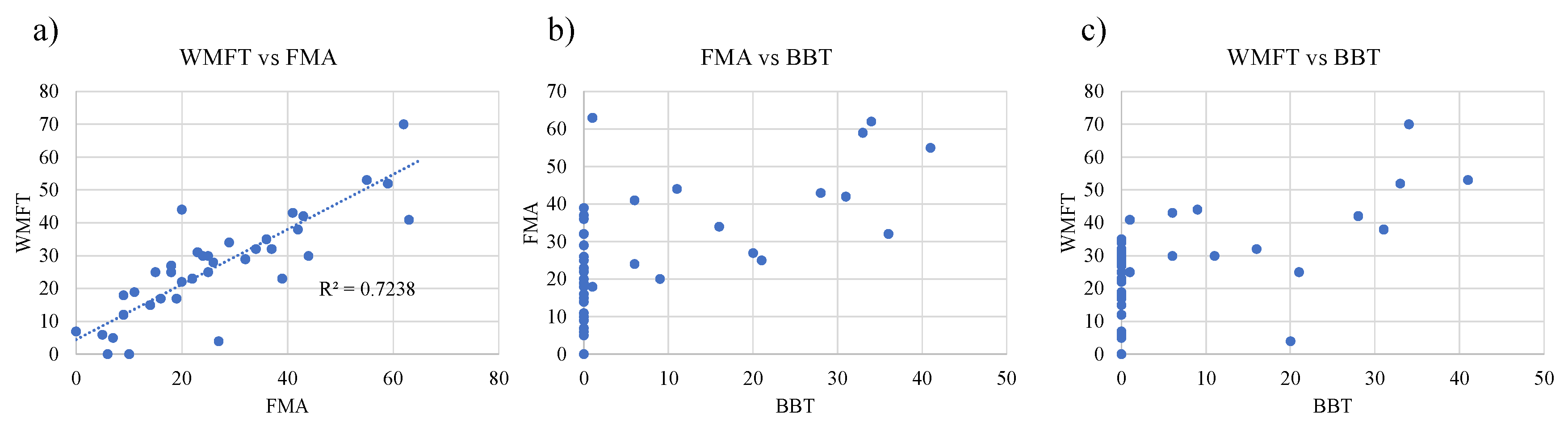
3.6. Sensitivity of Measure Outcomes to Motor Function
4. Discussion
4.1. Time to NMES following Stroke: Is Earlier Intervention More Effective?
4.2. Stroke Severity
4.3. Target Muscles
4.4. Is a Higher Dose of NMES More Beneficial?
4.5. Which of the NMES Modes Is More Effective?
4.6. Sensitivity of Measure Outcomes to Motor Function
4.7. Possibility of rPMS for Recovery from UE Paresis
4.8. Effects of Neuromodulators: Long-Term and Long-Lasting?
4.9. Other Possible Factors: Gender Difference
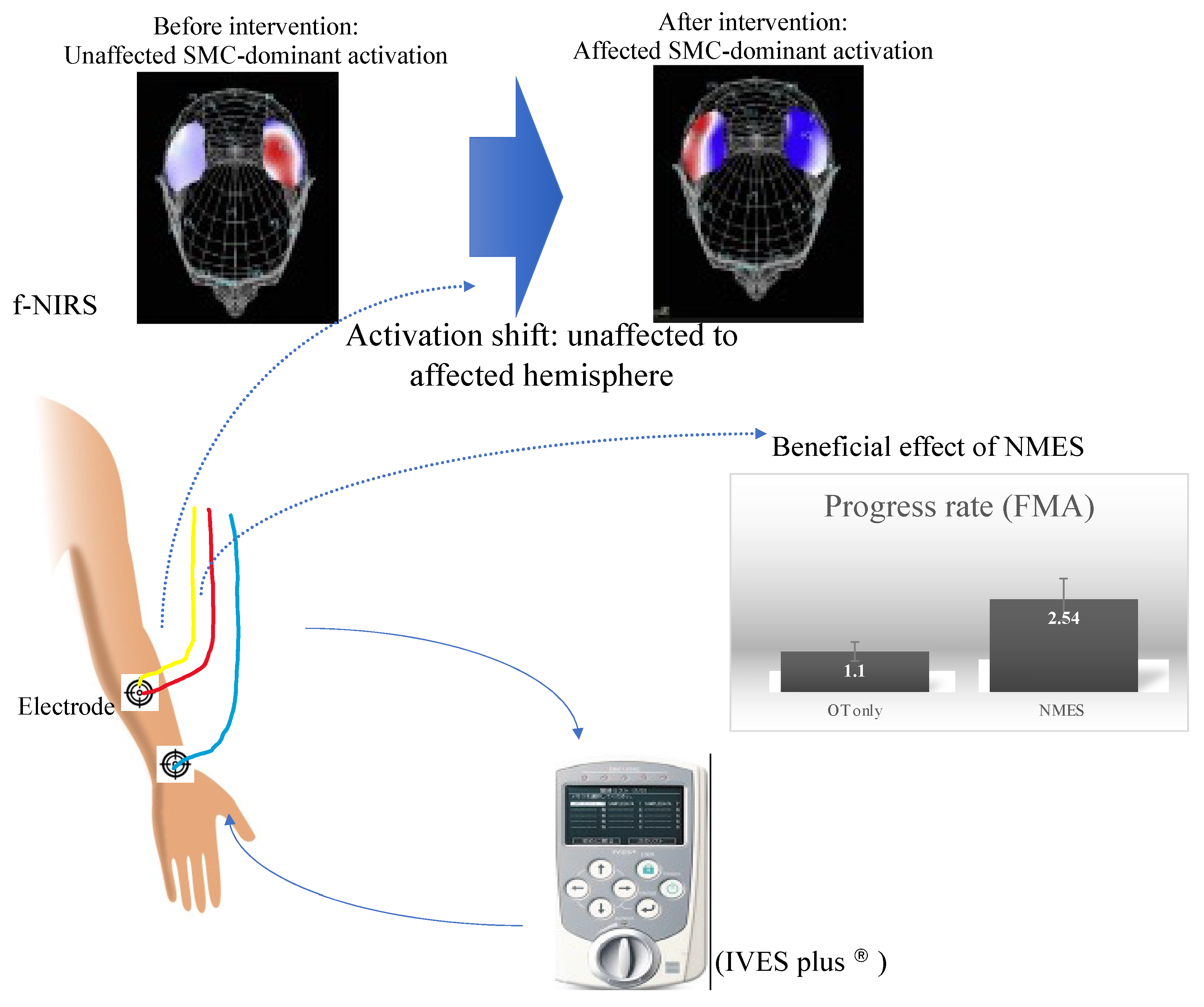
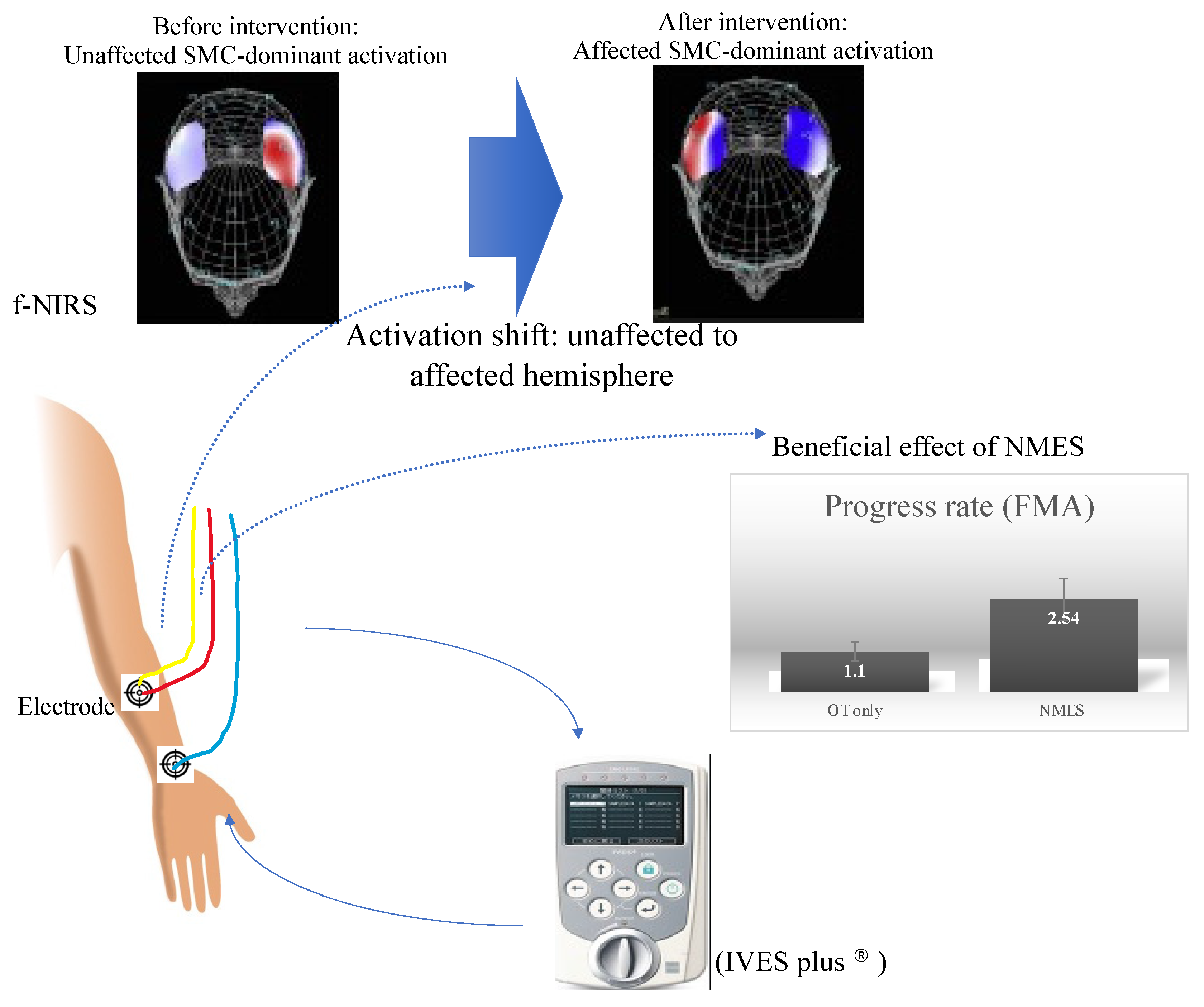
4.10. Neural Basis for the Benefits from Neuromodulators
4.11. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hsu, W.Y.; Cheng, C.H.; Liao, K.K.; Lee, I.H.; Lin, Y.Y. Effects of repetitive transcranial magnetic stimulation on motor functions in patients with stroke: A meta-analysis. Stroke 2012, 43, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Le, Q.; Qu, Y.; Tao, Y.; Zhu, S. Effects of repetitive transcranial magnetic stimulation on hand function recovery and excitability of the motor cortex after stroke: A meta-analysis. Am. J. Phys. Med. Rehabil. 2014, 93, 422–430. [Google Scholar] [CrossRef]
- Hummel, F.; Celnik, P.; Giraux, P.; Floel, A.; Wu, W.H.; Gerloff, C.; Cohen, L.G. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 2005, 128, 490–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlaug, G.; Renga, V.; Nair, D. Transcranial direct current stimulation in stroke recovery. Arch. Neurol. 2008, 65, 1571–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, J.J.; Hogan, N.; Perepezko, E.M.; Krebs, H.I.; Rogers, J.M.; Goyal, K.S.; Dohring, M.E.; Fredrickson, E.; Nethery, J.; Ruff, R.L. Response to upper-limb robotics and functional neuromuscular stimulation following stroke. J. Rehabil. Res. Dev. 2005, 42, 723–736. [Google Scholar] [CrossRef]
- Popovic, D.B.; Popovic, M.B.; Sinkjaer, T. Neurorehabilitation of upper extremities in humans with sensory-motor impairment. Neuromodulation 2002, 5, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Eraifej, J.; Clark, W.; France, B.; Desando, S.; Moore, D. Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: A systematic review and meta-analysis. Syst. Rev. 2017, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Wattchow, K.A.; McDonnell, M.N.; Hillier, S.L. Rehabilitation Interventions for Upper Limb Function in the First Four Weeks Following Stroke: A Systematic Review and Meta-Analysis of the Evidence. Arch. Phys. Med. Rehabil. 2018, 99, 367–382. [Google Scholar] [CrossRef]
- Howlett, O.A.; Lannin, N.A.; Ada, L.; McKinstry, C. Functional electrical stimulation improves activity after stroke: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Whitall, J. Stroke rehabilitation research: Time to answer more specific questions? NeuroRehabilit. Neural Repair 2004, 18, 3–8. [Google Scholar] [CrossRef]
- Obayashi, S.; Takahashi, R. Repetitive peripheral magnetic stimulation improves severe upper limb paresis in early acute phase stroke survivors. NeuroRehabilitation 2020, 46, 569–575. [Google Scholar] [CrossRef]
- Francisco, G.; Chae, J.; Chawla, H.; Kirshblum, S.; Zorowitz, R.; Lewis, G.; Pang, S. Electromyogram-triggered neuromuscular stimulation for improving the arm function of acute stroke survivors: A randomized pilot study. Arch. Phys. Med. Rehabil. 1998, 79, 570–575. [Google Scholar] [CrossRef]
- Chae, J.; Bethoux, F.; Bohine, T.; Dobos, L.; Davis, T.; Friedl, A. Neuromuscular stimulation for upper extremity motor and functional recovery in acute hemiplegia. Stroke 1998, 29, 975–979. [Google Scholar] [CrossRef] [Green Version]
- Powell, J.; Pandyan, A.D.; Granat, M.; Cameron, M.; Stott, D.J. Electrical stimulation of wrist extensors in poststroke hemiplegia. Stroke 1999, 30, 1384–1389. [Google Scholar] [CrossRef] [Green Version]
- Cauraugh, J.; Light, K.; Kim, S.; Thigpen, M.; Behrman, A. Chronic motor dysfunction after stroke: Recovering wrist and finger extension by electromyography-triggered neuromuscular stimulation. Stroke 2000, 31, 1360–1364. [Google Scholar] [CrossRef]
- Mann, G.E.; Burridge, J.H.; Malone, L.J.; Strike, P.W. A pilot study to investigate the effects of electrical stimulation on recovery of hand function and sensation in subacute stroke patients. Neuromodulation 2005, 8, 193–202. [Google Scholar] [CrossRef]
- Thrasher, T.A.; Zivanovic, V.; McIlroy, W.; Popovic, M.R. Rehabilitation of reaching and grasping function in severe hemiplegic patients using functional electrical stimulation therapy. NeuroRehabilit. Neural Repair 2008, 22, 706–714. [Google Scholar] [CrossRef]
- Chan, M.K.; Tong, R.K.; Chung, K.Y. Bilateral upper limb training with functional electric stimulation in patients with chronic stroke. NeuroRehabilit. Neural Repair 2009, 23, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Hsu, S.S.; Hu, M.H.; Wang, Y.H.; Yip, P.K.; Chiu, J.W.; Hsieh, C.L. Dose-response relation between neuromuscular electrical stimulation and upper-extremity function in patients with stroke. Stroke 2010, 41, 821–824. [Google Scholar] [CrossRef] [Green Version]
- Yun, G.J.; Chun, M.H.; Park, J.Y.; Kim, B.R. The synergic effects of mirror therapy and neuromuscular electrical stimulation for hand function in stroke patients. Ann. Rehabil. Med. 2011, 35, 316–321. [Google Scholar] [CrossRef]
- Shindo, K.; Fujiwara, T.; Hara, J.; Oba, H.; Hotta, F.; Tsuji, T.; Hase, K.; Liu, M. Effectiveness of hybrid assistive neuromuscular dynamic stimulation therapy in patients with subacute stroke: A randomized controlled pilot trial. NeuroRehabilit. Neural Repair 2011, 25, 830–837. [Google Scholar] [CrossRef]
- Page, S.J.; Levin, L.; Hermann, V.; Dunning, K.; Levine, P. Longer versus shorter daily durations of electrical stimulation during task-specific practice in moderately impaired stroke. Arch. Phys. Med. Rehabil. 2012, 93, 200–206. [Google Scholar] [CrossRef]
- Hara, Y.; Obayashi, S.; Tsujiuchi, K.; Muraoka, Y. The effects of electromyography-controlled functional electrical stimulation on upper extremity function and cortical perfusion in stroke patients. Clin. Neurophysiol. 2013, 124, 2008–2015. [Google Scholar] [CrossRef]
- Boyaci, A.; Topuz, O.; Alkan, H.; Ozgen, M.; Sarsan, A.; Yildiz, N.; Ardic, F. Comparison of the effectiveness of active and passive neuromuscular electrical stimulation of hemiplegic upper extremities: A randomized, controlled trial. Int. J. Rehabil. Res. 2013, 36, 315–322. [Google Scholar] [CrossRef]
- McCabe, J.; Monkiewicz, M.; Holcomb, J.; Pundik, S.; Daly, J.J. Comparison of robotics, functional electrical stimulation, and motor learning methods for treatment of persistent upper extremity dysfunction after stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2015, 96, 981–990. [Google Scholar] [CrossRef] [Green Version]
- Amasyali, S.Y.; Yaliman, A. Comparison of the effects of mirror therapy and electromyography-triggered neuromuscular stimulation on hand functions in stroke patients: A pilot study. Int. J. Rehabil. Res. 2016, 39, 302–307. [Google Scholar] [CrossRef]
- Kwakkel, G.; Winters, C.; van Wegen, E.E.; Nijland, R.H.; van Kuijk, A.A.; Visser-Meily, A.; de Groot, J.; de Vlugt, E.; Arendzen, J.H.; Geurts, A.C.; et al. Effects of Unilateral Upper Limb Training in Two Distinct Prognostic Groups Early After Stroke: The EXPLICIT-Stroke Randomized Clinical Trial. NeuroRehabilit. Neural Repair 2016, 30, 804–816. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.D.; Page, S.J.; Delahanty, M.; Knutson, J.S.; Gunzler, D.D.; Sheffler, L.R.; Chae, J. Upper-Limb Recovery After Stroke: A Randomized Controlled Trial Comparing EMG-Triggered, Cyclic, and Sensory Electrical Stimulation. NeuroRehabilit. Neural Repair 2016, 30, 978–987. [Google Scholar] [CrossRef] [Green Version]
- Carda, S.; Biasiucci, A.; Maesani, A.; Ionta, S.; Moncharmont, J.; Clarke, S.; Murray, M.M.; Millan, J.D.R. Electrically Assisted Movement Therapy in Chronic Stroke Patients With Severe Upper Limb Paresis: A Pilot, Single-Blind, Randomized Crossover Study. Arch. Phys. Med. Rehabil. 2017, 98, 1628–1635.e2. [Google Scholar] [CrossRef] [Green Version]
- Jonsdottir, J.; Thorsen, R.; Aprile, I.; Galeri, S.; Spannocchi, G.; Beghi, E.; Bianchi, E.; Montesano, A.; Ferrarin, M. Arm rehabilitation in post stroke subjects: A randomized controlled trial on the efficacy of myoelectrically driven FES applied in a task-oriented approach. PLoS ONE 2017, 12, e0188642. [Google Scholar] [CrossRef]
- Qian, Q.; Hu, X.; Lai, Q.; Ng, S.C.; Zheng, Y.; Poon, W. Early Stroke Rehabilitation of the Upper Limb Assisted with an Electromyography-Driven Neuromuscular Electrical Stimulation-Robotic Arm. Front. Neurol. 2017, 8, 447. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, S.; Takahashi, R.; Onuki, M. Upper limb recovery in early acute phase stroke survivors by coupled EMG-triggered and cyclic neuromuscular electrical stimulation. NeuroRehabilitation 2020, 46, 417–422. [Google Scholar] [CrossRef]
- Lin, Z.; Yan, T. Long-term effectiveness of neuromuscular electrical stimulation for promoting motor recovery of the upper extremity after stroke. J. Rehabil. Med. 2011, 43, 506–510. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Park, J.H.; Jung, M.Y.; Yoo, E.Y. Effects of Task-Oriented Training as an Added Treatment to Electromyogram-Triggered Neuromuscular Stimulation on Upper Extremity Function in Chronic Stroke Patients. Occup. Ther. Int. 2016, 23, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Kwakkel, G.; Kollen, B.; Twisk, J. Impact of time on improvement of outcome after stroke. Stroke 2006, 37, 2348–2353. [Google Scholar] [CrossRef] [Green Version]
- Wahl, A.S.; Omlor, W.; Rubio, J.C.; Chen, J.L.; Zheng, H.; Schroter, A.; Gullo, M.; Weinmann, O.; Kobayashi, K.; Helmchen, F.; et al. Neuronal repair. Asynchronous therapy restores motor control by rewiring of the rat corticospinal tract after stroke. Science 2014, 344, 1250–1255. [Google Scholar] [CrossRef]
- Nishibe, M.; Urban, E.T., 3rd; Barbay, S.; Nudo, R.J. Rehabilitative training promotes rapid motor recovery but delayed motor map reorganization in a rat cortical ischemic infarct model. NeuroRehabilit. Neural Repair 2015, 29, 472–482. [Google Scholar] [CrossRef]
- Zhang, L.; Xing, G.; Fan, Y.; Guo, Z.; Chen, H.; Mu, Q. Short- and Long-term Effects of Repetitive Transcranial Magnetic Stimulation on Upper Limb Motor Function after Stroke: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2017, 31, 1137–1153. [Google Scholar] [CrossRef]
- Morizawa, Y.M.; Hirayama, Y.; Ohno, N.; Shibata, S.; Shigetomi, E.; Sui, Y.; Nabekura, J.; Sato, K.; Okajima, F.; Takebayashi, H.; et al. Reactive astrocytes function as phagocytes after brain ischemia via ABCA1-mediated pathway. Nat. Commun. 2017, 8, 28. [Google Scholar] [CrossRef]
- Jorgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Vive-Larsen, J.; Stoier, M.; Olsen, T.S. Outcome and time course of recovery in stroke. Part II: Time course of recovery. The Copenhagen Stroke Study. Arch. Phys. Med. Rehabil. 1995, 76, 406–412. [Google Scholar] [CrossRef]
- Duncan, P.W.; Lai, S.M.; Keighley, J. Defining post-stroke recovery: Implications for design and interpretation of drug trials. Neuropharmacology 2000, 39, 835–841. [Google Scholar] [CrossRef]
- Barker, A.T. An introduction to the basic principles of magnetic nerve stimulation. J. Clin. Neurophysiol. 1991, 8, 26–37. [Google Scholar] [CrossRef]
- Krewer, C.; Hartl, S.; Muller, F.; Koenig, E. Effects of repetitive peripheral magnetic stimulation on upper-limb spasticity and impairment in patients with spastic hemiparesis: A randomized, double-blind, sham-controlled study. Arch. Phys. Med. Rehabil. 2014, 95, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, L.D.; Schneider, C. Effects of repetitive peripheral magnetic stimulation on normal or impaired motor control. A review. Neurophysiol. Clin. 2013, 43, 251–260. [Google Scholar] [CrossRef]
- Struppler, A.; Binkofski, F.; Angerer, B.; Bernhardt, M.; Spiegel, S.; Drzezga, A.; Bartenstein, P. A fronto-parietal network is mediating improvement of motor function related to repetitive peripheral magnetic stimulation: A PET-H2O15 study. Neuroimage 2007, 36 (Suppl. 2), T174–T186. [Google Scholar] [CrossRef] [PubMed]
- Struppler, A.; Angerer, B.; Gundisch, C.; Havel, P. Modulatory effect of repetitive peripheral magnetic stimulation on skeletal muscle tone in healthy subjects: Stabilization of the elbow joint. Exp. Brain Res. 2004, 157, 59–66. [Google Scholar] [CrossRef]
- Struppler, A.; Havel, P.; Muller-Barna, P. Facilitation of skilled finger movements by repetitive peripheral magnetic stimulation (RPMS)—A new approach in central paresis. NeuroRehabilitation 2003, 18, 69–82. [Google Scholar] [CrossRef]
- Beaulieu, L.D.; Schneider, C. Repetitive peripheral magnetic stimulation to reduce pain or improve sensorimotor impairments: A literature review on parameters of application and afferents recruitment. Neurophysiol. Clin. 2015, 45, 223–237. [Google Scholar] [CrossRef]
- Lindenberg, R.; Zhu, L.L.; Schlaug, G. Combined central and peripheral stimulation to facilitate motor recovery after stroke: The effect of number of sessions on outcome. NeuroRehabilit. Neural Repair 2012, 26, 479–483. [Google Scholar] [CrossRef] [Green Version]
- Lisabeth, L.D.; Reeves, M.J.; Baek, J.; Skolarus, L.E.; Brown, D.L.; Zahuranec, D.B.; Smith, M.A.; Morgenstern, L.B. Factors influencing sex differences in poststroke functional outcome. Stroke 2015, 46, 860–863. [Google Scholar] [CrossRef] [Green Version]
- Di Lazzaro, V.; Pellegrino, G.; Di Pino, G.; Ranieri, F.; Lotti, F.; Florio, L.; Capone, F. Human Motor Cortex Functional Changes in Acute Stroke: Gender Effects. Front. Neurosci. 2016, 10, 10. [Google Scholar] [CrossRef] [Green Version]
- Nudo, R.J.; Wise, B.M.; SiFuentes, F.; Milliken, G.W. Neural substrates for the effects of rehabilitative training on motor recovery after ischemic infarct. Science 1996, 272, 1791–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grefkes, C.; Fink, G.R. Connectivity-based approaches in stroke and recovery of function. Lancet Neurol. 2014, 13, 206–216. [Google Scholar] [CrossRef]
- Blickenstorfer, A.; Kleiser, R.; Keller, T.; Keisker, B.; Meyer, M.; Riener, R.; Kollias, S. Cortical and subcortical correlates of functional electrical stimulation of wrist extensor and flexor muscles revealed by fMRI. Hum. Brain Mapp. 2009, 30, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Flamand, V.H.; Schneider, C. Noninvasive and painless magnetic stimulation of nerves improved brain motor function and mobility in a cerebral palsy case. Arch. Phys. Med. Rehabil. 2014, 95, 1984–1990. [Google Scholar] [CrossRef]
- Burnett, M.G.; Shimazu, T.; Szabados, T.; Muramatsu, H.; Detre, J.A.; Greenberg, J.H. Electrical forepaw stimulation during reversible forebrain ischemia decreases infarct volume. Stroke 2006, 37, 1327–1331. [Google Scholar] [CrossRef]
- Rothwell, J.C. Techniques and mechanisms of action of transcranial stimulation of the human motor cortex. J. Neurosci. Methods 1997, 74, 113–122. [Google Scholar] [CrossRef]
- Amassian, V.E.; Stewart, M.; Quirk, G.J.; Rosenthal, J.L. Physiological basis of motor effects of a transient stimulus to cerebral cortex. Neurosurgery 1987, 20, 74–93. [Google Scholar] [CrossRef]
- Volz, L.J.; Hamada, M.; Rothwell, J.C.; Grefkes, C. What Makes the Muscle Twitch: Motor System Connectivity and TMS-Induced Activity. Cereb. Cortex 2015, 25, 2346–2353. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Design | Numbers | Phase | Time to start | Duration | Dose | Target Muscles | Disability Pretreatment | Outcome Measures | Progress Rate | Results |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Francisco et al. | 1998 | RCT | Infarct (n = 9) NMES (n = 4) Contr. (n = 5) | acute (<1 mo) | NMES 17.5 day Contr. 18.2 day | length of stay: NMES 33.0 days Contr. 25.8 days | 5 times/week 30 min × 2 sessions/day | ECRL ECRB | severe: NMES 12.5 Contr.21 | FMA 12.5 vs. 21.2→37 vs. 31 | 1.039 (NMES) 0.54 (contr.) | Significant improvement in Exp Upper extremity Fugl-Meyer motor assessment (p = 0.05) |
| Chae et al. | 1998 | RCT | NMES (n = 14) Contr. (n = 14) | acute (<1 mo) | 15.7 days | Total of 15 sessions | 60 min session/day | EDC ECR | severe: NMES11.1 Contr.8.3 | FMA 11.1 vs. 8.3 (cotr.)→13.1 6.5 | 0.13 (NMES) | Significant improvement in Exp/FMA Before treatment (p = 0.05) 4 weeks (p = 0.05) 12 weeks (p = 0.06) No significant difference was found in FIM |
| Powell et al. | 1999 | RCT | Stroke (n = 60) NMES (n = 30) Contr. (n = 30) | acute (<1mo) | NMES 23.9 days Con 22.9 days | 8 weeks | 30 min × 3 sessions/day | ECRL ECRB ECU EDC | severe: NMES 6 Contr. 0 | ARAT 6 vs. 0 | Significant improvement in Exp Isometric strength of wrist extensors (4 weeks; p = 0.004, 32 weeks; p = 0.014) ARAT (4 weeks-Grasp/Grip; p = 0.013, 32 weeks-Grasp/Grip; p = 0.02) | |
| Cauraugh et al. | 2000 | RCT | Infarct (n = 11) NMES (n = 7) Contr. (n = 4) | chronic (>6mo) | 3.49 years | 2 weeks | 3 times/week 30 min × 2 sessions/day | EDC ECU | moderate: NMES 7 Contr.3 | BBT 7 vs. 3→15 vs. 4 | 1.33 (NMES) | Significant improvement in Exp BBT (p < 0.05) Force-generation task; sustained muscular contraction (p < 0.05) |
| Mann et al. | 2005 | RCT | Stroke (n = 22): 21 infarct 1 ICH cyclic NMES (n = 11) Contr. (n = 11) | chronic | 12 months | 12 weeks | 10 to 30 min twice sessions/ day | triceps brachialis ECR EDC | moderate: NMES20.0 Contr.14.3 | ARAT 20.0 14.3→34.4 24.4 | 0.17 (NMES) | Nonparametric tests of covariance (ancova) identified a significant between-group difference between the beginning and end of the treatment period. |
| Thrasher et al. | 2008 | RCT | stroke (n = 21) subacute: NMES (n = 10) Contr. (n = 11) chronic (n = 7) | subacute chronic | subacute FES 29.8 ± 11.8 days control 28.5 ± 9.0 days chronic 2.7 ± 1.8 years | 13 weeks (acute) 16 weeks (chronic) | 5 days/week 45 min/session 45 min of NMES | anterior deltoid triceps brachii posterior deltoid biceps brachii flexor carpi radialis and flexor capri ulnaris (wrist flexion); extensor carpi radialis longus and brevis, and extensor carpi ulnaris (wrist extension); flexor digitorum superficialis and flexor digitorum profundus (finger flexion), thenar (thumb flexion); extensor digitorum and lumbricals | not available | baseline unknown | FMA 0.61 (subacute) 0.125 (chronic) | The acute FES group also improved more than the control group in terms of the BI, FMA, and CMSMR (p < 0.05). The chronic group tended to score slightly higher after FES therapy as compared with baseline for most measures, but the differences were not statistically significant. |
| Chan et al. | 2009 | RCT | stroke (n = 20) NMES (n = 10) Contr. (n = 10) | chronic | NMES 18.1 months Contr. 12.1 months | 15 sessions in total | 10 min stretching +20 min bilateral UE training with FES or placebo ES+ 60 min SC | EDS abductor pollicis longus | severe NMES18.2 Contr.20.0 | FMA 18.2 20.0→25.9 22.1 FTHUE | 0.513 (NMES) | After 15 training sessions, the FES group had significant improvement in FMA, FTHUE, and active range of motion of wrist extension, compared with the contr. |
| Hsu et al. | 2010 | RCT | Stroke (n = 66) Infarct (n = 33) Low-NMES (n = 13) High-NMES (n = 8) Contr. (n = 12) ICH (n = 33) Low-NMES (n = 9) High-NMES (n = 14) Contr. (n = 10) | acute (<1mo) | NMES (23.9 days) | 4 weeks | 5 times/week Low-NMES 30 min session/day High-NMES 60 min session/day | Spasticity/ Completely Paralyzed EDC ECR Completely Paralyzed FDC Shoulder Subluxation supraspinatus post. deltoid | severe: L-NMES 8.3 H-NMES 7.5 Conr.6.6 | FMA 6.6 (ctr.) 8.3 (L) 7.5 (H)→14.2 28.1 25.5 (after) ARAT 0.5 0.7 0.5→3.5 8.6 8.5 (after) | 0.99 (Low NMES) 0.9 (High) 0.38 (control) | Significant improvement in Low-NMES & High-NMES at 4 weeks and 12 weeks (follow up), when compared with the Contr. No significant difference was found between the 2 Exp groups. Motor Activity Log: no significant difference was found among the 3 groups. |
| Yun et al. | 2011 | RCT | stroke (n = 60) infarct 46 MT + NMES (n = 20) NMES (n = 20) MT (n = 20) | acute (<1mo) | MT + NMSE 25.6 ± 14.4 days MT 23.9 ± 10.5 days NMES 28.1 ± 12.8 days | 3 weeks | 30 min/session 5 days/week | EDC extensor pollicis brevis | severe MT + NMES 4.3 MT 5.3 NMES 5.3 | FMA 4.3 5.3 5.3→20.7 11.2 15.3 grip power 1.2 1.3 1.2→2.8 2.4 2.5 | (MT + NM) 1.09 (MT) 0.39 (NM) 0.66 | |
| Shindo et al. | 2011 | RCT | stroke (n = 20) infarct 15 HANDS (n = 10) Contr. (n = 10) | subacute | HANDS 34.4 days Contr. 37.0 days | 3 weeks | 8h h/day+ 1 h SC 5 days/week | EDC | moderate: NMES 31.3 Contr. 30.5 | FMA 31.3 30.5→43.5 36.0 ARAT17.7 22.8→30.9 31.1 MAL | (HANDS) 0.83 (control) 0.37 | Compared with the control group, the HANDS group showed significantly greater gains in distal (wrist/hand) portion of FMA and ARAT. |
| Lin and Yan | 2011 | RCT | stroke (n = 37) infarct 25 NMES (n = 19) Contr. (n = 18) | subacute | NMES 43.5 days Contr. 41.3 days | 3 weeks | NES 30 min/day Once a day 5 day/w, 3 weeks PT 30 min/day OT 30 min/day 5 day/w, 3 weeks | deltoid muscle middle of the supraspinatus muscle wrist extensor | severe NMES 8.4 Contr. 8.2 | FMA 8.4 8.2→15.9 12.5 | NMES 0.5 | |
| Page et al. | 2012 | RCT | stroke (n = 32) 30 min-NMES (n = 9) 60 min-NMES (n = 8) 120 min-NMES (n = 8) 30 min home ex. (n = 7) | chronic | >6 months | 8 weeks | 5 sessions/week | extensor digitorum extensor pollicis brevis flexor digitorum superficialis flexor pollicis longus thenar muscles | moderate: 30 min-NMES 21.6 60 min-NMES 26.6 120 min-NMES 27.1 Contr. 25.6 | FMA21.6 26.6 27.1 25.6→22.9 27.9 31.3 26.9 ARAT AMAT BBT0.7 5.6 9.8 7.9→1.6 4.8 12.5 7.7 | (30 NM) 0.03 (60 NM) 0.03 (120 NM) 0.105 (home) 0.03 | 120 min a day of RTP augmented by ESN use elicits the largest and most consistent UE motor changes in moderately impaired stroke subjects. |
| Hara et al. | 2013 | CT | Infarct (n = 10) ICH (n = 6) active ROM cyclic NMES EMG-NMES | chronic | Contr. (22.9 days) | 5 months | 1−2 times/week 40 min session/day | FDC EDC | moderate:24 | FMA 24→44 grip power 6.3→18.4 | 0.5~1 | Significant improvement in EMG-FES, when compared with voluntary muscle contraction (VOL) and simple electrical muscle stimulation (ES) |
| Boyaci et al. | 2013 | RCT | EMG NMES (n = 11) Cyclic NMES (n = 10) Placebo Contr. (n = 10) | chronic | Active-NMES (38.1 weeks) Passive-NMES (33.7 weeks) Contr. (22.1 weeks) | 3 weeks: 15 sessions in total | 5 time/week 45 min session/day | Wrist and Fingers extensor | moderate:active N29.27 passive 34.80 contr. 33.70 | FMA active N29.27 passive 34.80 contr. 33.70→37.27 39.80 34.70 MAL | (A-NM) 0.53 (p-NM) 0.33 (contr.) 0.07 | No significant difference was found in FMA-UE and MAL-AOU |
| Kim et al. | 2015 | RCT | stroke (n = 20) NMES (n = 10) Contr. (n = 10) | chronic | NMES 10.9 months Contr. 15.4 months | 4 weeks | EMG-NMES+TOT: 30 min/day, 5 days/week EMG-NMES only 20 min per day, 5 days per week | EDC | moderte 48.6 | FMA 48.6 49.7→54.6 50.5 | NMES+TOT 0.3 | |
| McCabe et al. | 2015 | RCT | stroke (n = 35) robotics + ML (n = 12) NMES+ML (n = 12) ML (n = 11) | chronic | over 1 years | 60 sessions | 5 sessions/week 5 h session/day | wrist&fingers flexors/extensors forearm supinators/ pronatorss | moderate: robot 22.62 FES 22.85 ML 23.58 | FMA robot 22.62 NMES 22.85 ML 23.58→31.3 32.3 33.5 AMAT | Robot 0.14 NMES 0.15 ML 0.165 | No significant difference among 3 conditions was found in FMA-UE and AMAT |
| Amasyali et al. | 2016 | RCT | Infarct (n = 24) NMES (n = 7) MT (n = 9) Contr. (n = 8) | subacute (1mo to 6mo) | NMES (5.29 months) Mirror T. (4.11 months) Contr. (6.50 months) | 3 weeks: 15 sessions in total | 5 time/week 30 min session/day | Wrist and Fingers extensor | moderate: mirror 36.5 NMES 41.0 contr. 39.8 | FMA mirror 36.5 NMES 41.0 Contr. 39.8→48.6 50.7 51.4 BBT 12.0 12.5→15.7 16.0 | mirror 0.80 NMES 0.71 contr. 0.77 | Increments in the FMA and BBT scores for the Exp group were significantly higher than the control group. |
| Kwakkel et al. | 2016 | RCT | Infarct (n = 101) NMES (n = 50) Contr. (n = 51) | acute (<1 mo) | NMES (0.3 months) Contr. (0.3 months) | 3 weeks | 7 times/week 30 min session/day | Wrist and Fingers extensor | moderate: mCIMT 42.7 Contr.35.6 severe: NMES 6.5 Contr.7.3 | FMA NMES 6.5 Contr.7.3→15 19.5 ARAT 0.62 0.8→5.5 8.14 FMA mCIMT 42.7 Contr.35.6→58.8 53.2 ARAT 23.9 vs. 20.97→45.2 39.0 | NMES 0.4 contr. 0.58 | No significant difference was found in FMA-UE, ARAT and MAL-AOU |
| Wilson et al. | 2016 | RCT | Cyclic NMES (n = 39) NMES (n = 41) Sensory stim. (n = 42) | subacute | Cyclic NMES (2.0 months) EMG-Triggered (2.9 months) Sensory (3.2 months) | 8 weeks | 7 times/week 40 min × 2 sessions/day | ECR EDC | moderate: 26.8 (S) 29.8 (EMG) 27.5 (Cyc) | FMA 26.8 (S) 29.8 (EMG) 27.5 (Cyc)→30.4 32.6 31.8 AMAT | NMES 0.05 cyclic 0.077 sensory 0.064 | There was no significant difference in the improvement among groups in the FMA, FMA Wrist and Hand or the mAMAT |
| Carda et al. | 2017 | RCT | Infarct (n = 11) NMES (n = 5) Contr. (n = 6) | chronic | NMES (52 months) Contr. (41.5 months) | 2 weeks: 10 sessions in total crossover: NMES-SC(NS) or SC-NMES(SN) | 5 times/week 90 min/sessions/day | Not noted | severe: 11 (NS) 13.2 (SN) | FMA 11 (NS) 13.2 (SN)→23.2 17.5→27.4 20.4 WMFT MAL | N-S 1.22 S-N 0.43 | Significant improvement in Exp Fugl-Meyer Motor Assessment (p < 0.05) No significant difference was found in Wolf Motor Function Test and Motor Activity Log |
| Jonsdottir et al. | 2017 | RCT | Infarct (n = 56) Hemorrhage (n = 12) NMES (n = 32) Contr. (n = 36) | subacute (<6 M) chronic (>6 M) | NMES (4.5 months) Contr. (3 months) | 5–6 weeks: 25 sessions in total | 5 times/week 45 min session/day | wrist extensor ant. deltoid | moderate: NMES 28.0 Contr. 32.0 | FMA NMES28.0 Contr.32.0→39.0 36.0 ARAT 6.0 6.5→21.0 12.5 | NMES 0.44 contr. 0.16 | Significant improvement in both groups FMA Upper extremity, ARAT No significant difference in Exp, when compared with the Con |
| Qian et al. | 2017 | RCT | Infarct (n = 9) ICH (n = 15) NMES (n = 14) Contr. (n = 10) | subacute | NMES (25–148 days) Contr. (14–142 days) | 4 weeks: 20 sessions in total | 5 times/week 40 min session/day for NMES 60 h/day for control training | biceps brachii triceps brachii FCR ECU EDC | severe: NMES 22.3 Contr. 20.3 | FMA NMES 22.3 Contr. 20.3→43.6 30.1 ARAT 15.7 12.0→29.2 24.2 | NMES 1.06 contr. 0.49 | Significant improvement in both groups FMA, ARAT and FIM (p < 0.001, effect sizes > 0.279) |
| Obayashi et al. | 2020 | RCT | Infarct (n = 15) ICH (n = 2) NMES (n = 8) Contr. (n = 9) | acute (<10 days) | coupled NMES (7 days) Contr. (5.8 days) | coupledNMES (10.87 sessions) Contr. (16.5 sessions) progress rate | 5 sessions/week 40 minSC or 20 min NMES +20 minSC)/session/ day | ant. deltoid triceps brachii EDC ECR EIP FDS | severe: coupledNMES 20.2 Contr. 19.0 | FMA coupledNMES 20.2 Contr. 19.0→42.0 36.5 WMFT 22.3 18.2→38.1 30.4 BBT 5.6 3.4→11.1 6.0 | NMES 2.54 contr. 1.10 | Significantly different in Exp Progress rate; FMAt upper extremity (p = 0.036, r = 0.50) No significant difference was found in WMFT and BBT. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obayashi, S.; Saito, H. Neuromuscular Stimulation as an Intervention Tool for Recovery from Upper Limb Paresis after Stroke and the Neural Basis. Appl. Sci. 2022, 12, 810. https://doi.org/10.3390/app12020810
Obayashi S, Saito H. Neuromuscular Stimulation as an Intervention Tool for Recovery from Upper Limb Paresis after Stroke and the Neural Basis. Applied Sciences. 2022; 12(2):810. https://doi.org/10.3390/app12020810
Chicago/Turabian StyleObayashi, Shigeru, and Hirotaka Saito. 2022. "Neuromuscular Stimulation as an Intervention Tool for Recovery from Upper Limb Paresis after Stroke and the Neural Basis" Applied Sciences 12, no. 2: 810. https://doi.org/10.3390/app12020810
APA StyleObayashi, S., & Saito, H. (2022). Neuromuscular Stimulation as an Intervention Tool for Recovery from Upper Limb Paresis after Stroke and the Neural Basis. Applied Sciences, 12(2), 810. https://doi.org/10.3390/app12020810