
Maxillary Sinusitis as a Complication of Zygomatic Implants Placement: A Narrative Review



Abstract
1. Introduction
2. Research Method
- Presence of maxillary sinusitis (clinical and/or radiological signs and symptoms).
- Correlation between sinusitis and extra or intra-sinusal surgical technique.
- Need for pharmacological and/or surgical treatment of sinusitis.
- Presence of protocol for the treatment of the patients.
- P: Participants. Adult patients that underwent ZI placement to rehabilitate the superior dental arch in the case of maxillary atrophy (Cawood-Howell V–VI) alone or combined with conventional implants.
- I: Intervention. Zygomatic implant placement (all surgical techniques were considered in the study)
- C: Comparison control. Not applicable
- O: Outcomes. Presence of maxillary sinusitis; clinical and/or radiological signs and symptoms; correlation between sinusitis and extra or intra-sinusal surgical technique; need for pharmacological and/or surgical treatment of sinusitis
- T:Time. Between 1 year and 3 year after intervention
- S: Studies. All clinical studies were included. Reviews and meta-analyses were excluded.
3. Results
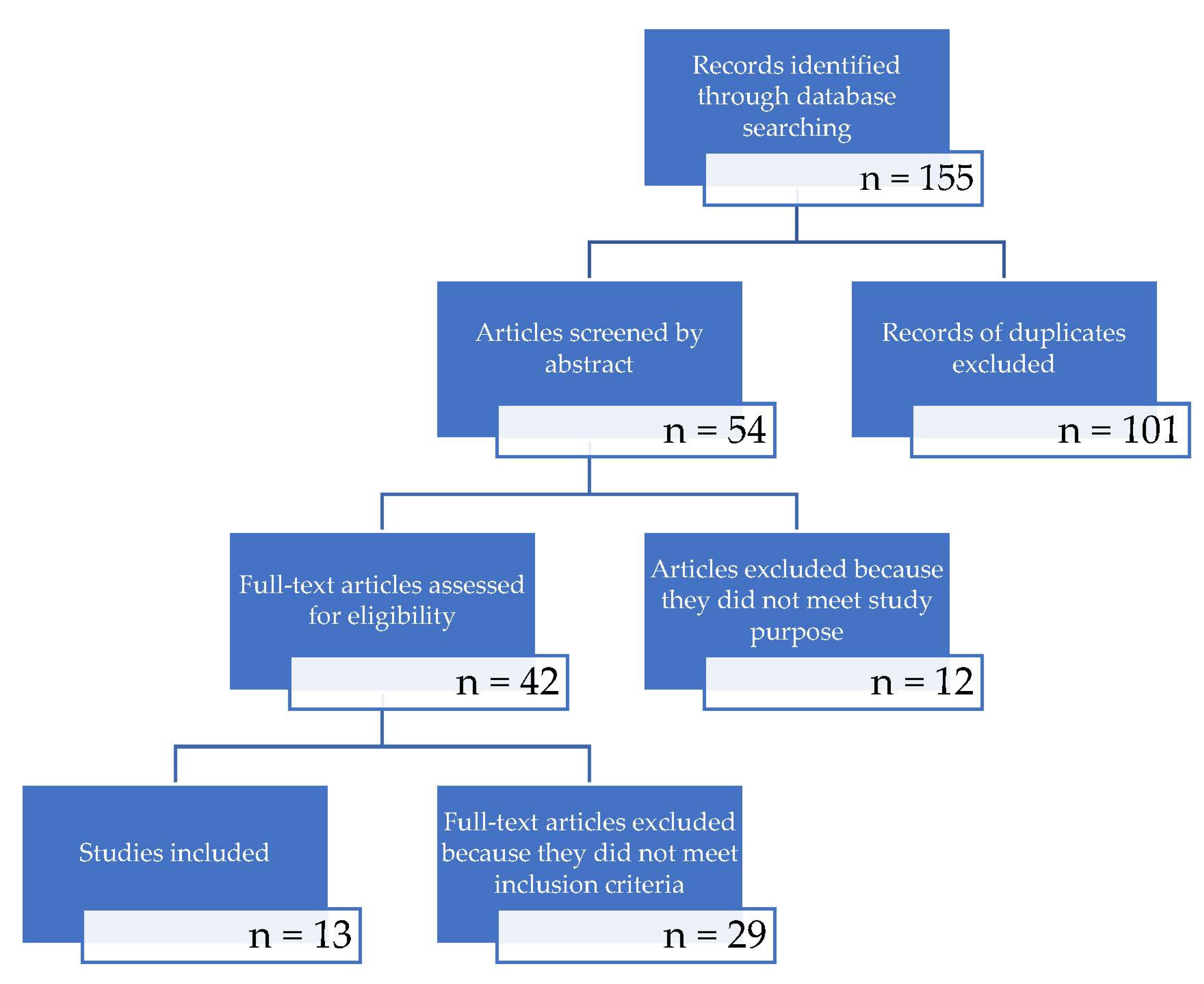
3.1. Literature Research
3.2. Description of the Studies and Analysis

{kind=link}
| Author | Paper Design | Year | N° of Patients | Mean Age | Risk Factors for Sinus Pathologies | N° of Zygomatic Implants | Pre-op Sinusitis | Pre-op Imaging | Post-op Sinusitis | Post-op Imaging | Post-op Symptoms | Treatment | Results after Treatment | Follow-up | Surgical Technique |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Urgell et al. [26] | Retrospective | 2008 | 54 | 56 (38–75) | Smokers (8/54 < 10 sigg, 1/54 > 10 sigg). 1/54 HIV + | 101 | 0/54 | HRCT + OPG | 1.9% (1/54) | OPG | N.A. | Antibiotics | Regression (1/1) | 72 months | Extrasinusal |
| Davò et al. [27] | Retrospective | 2008 | 42 | 57 (34–79) | Smokers < 10 sigg | 81 | 0/42 | Yes (not specified) | 2.3% (intra-op oro-antral communication) (1/42) | OPG + A-P Teleradiograph | Fluid drainage from nasal to oral cavity | Antibiotics + FESS antrostomy | Regression (1/1) | 20.5 (12–42) months | Extrasinusal, sinus slot, minimally invasive |
| Davò et al. [35] | Retrospective | 2008 | 36 | N.A. | Smokers (4/36 < 10 sigg) | 71 | 0/36 | CT paranasal sinuses | 0% clinical, 5.6% radiologic (2/36) | CT paranasal sinuses | No symptoms | Follow-up | No treatment | 21.9 (13–42) months | Extrasinusal (61/71), sinus slot (10/71) |
| Davò et al. [28] | Retrospective | 2009 | 24 | 51.4 (36–72) | Smokers | 45 | 0/24 | N.A. | 20.8% (5/24) | OPG + A-P teleradiograph + CT (5/24) | N.A. | Antibiotics (2/5), FESS (2/5), Caldwell-Luc approach (1/5) | Regression (5/5) | 60 months | Extrasinusal |
| Chow et al. [14] | Prospective | 2010 | 16 | 60 (no range) | Smokers (2/16) | 37 | No | CBCT | 0% | CBCT | No symptoms | Follow-up | No treatment | 12 months | Extrasinusal |
| Aparicio et al. [29] | Retrospective | 2012 | 22 | 63 (48–80) | Smokers (17/22 nonsmokers, 2/22 11–20 sigg, 3/22 > 20 sigg) | 41 | 0/22 | CBCT | 27.3% clinical (6/22), 54.6% radiologic (12/22) | CBCT | According to Lanza-Kennedy scale | Antibiotics + antihistamine (5/6), partial implant removal (1/6) | Regression (4/6) | 120 months | Extrasinusal |
| Bothur er al. [36] | Retrospective | 2015 | 14 | 60 (51–78) | Smokers (3/14), allergic rhinitis (1/14) | 58 | 0/14 | Standard X-rays | 28.5% (4/14 clinical)100% (14/14 radiological signs | CBCT | Yes (self-administered questionnaire) | Antibiotic | Regression (47) | 117.6 months | Extrasinusal |
| Bertolai et al. [30] | Retrospective | 2015 | 31 | 62 (52–82) | Smokers (0/31), Diabetes (0/31) | 78 | 0/31 | CT + OPG | 6.5% (2/31) | CT (in patients w. Clinical sinusitis) | N.A. | FESS 1/31, FESS + Caldwell-Luc approach 1/31 | Regression (2/2) | 20–60 months | Extrasinusal (27/31), Extra-maxillary (4/31) |
| Araujo et al. [31] | Retrospective | 2017 | 37 | 55.64 | N.A. | 129 | 0/37 | CBCT | 21.62% (8/37) | CBCT, OPG | Congestion, cough, purulent nasal drainage, chronic pain | Antibiotics 5/37, Antibiotics + FESS 3/37 | Regression (7/8), Recurrence (1/8) | >12 months | Sinus Slot |
| D’Agostino et al. [37] | Prospective | 2019 | 13 | 58 | No risk factors | 52 | 0/13 clinical, 0/26 sinuses w. Radiologic LMS = 0 | CBCT | 23% (3/13)/11.5% (3/26) of sinuses w. Radiologic LMS 1 | CBCT | No symptoms | FESS | SNOT20 1.2 (average) | 45 months | Extrasinusal |
| Perla Della Nave et al. [32] | Retrospective | 2020 | 102 | N.A. | N.A. | 206 | 0/102 | N.A. | 4.9% (5/102) | OPG, periapical radiographs, CBCT | N.A. | Antibiotics, conservative approach, implant removal | Regression after 8 months of antibiotic therapy (1/8), spontaneous after less than 1y. (1/8), implant removal after 2 y (1/8)–5 y (1/8)–10 y (1/8) | 12–144 months | ZAGA |
| Yalcin et al. [33] | Retrospective | 2020 | 45 | 51.76 | N.A. | 141 | 0/45 | CBCT | 4.44% (2/45) | OPG (+CT/CBCT) | N.A. | Removal (3/141 ZI) | N.A. | 6–36 months | Intrasinusal, extrasinusal, sinus slot |
| D’Agostino et al. [38] | Retrospective | 2021 | 42 | 63 (29–81) | Smokers (8/42) | 116 | 0/42 clinical, 13/84 sinuses w. radiologic LMS > 1 | CT | 19% clinical 8/42) (29/82 sinuses with radiologic LMS > 1) | CT | Yes (not specified) | Antibiotic and/or FESS | Regression (8/8) | 60 (12–162) months | Intrasinusal (32) Extrasinusal (10) |
4. Discussion
- Alterations of the natural ostium of the maxillary sinus.
- Presence of the accessory ostium, which could modify the physiological drainage capacity from the maxillary sinus as well as (in the case of surgical treatment )modify the approach to setting up at typical antrostomy.
- Alteration of the middle meatus with consequent difficulty of sinus drainage due to a paradoxical curvature of the middle turbinate or its pneumatization with a concha bullosa, which, in both cases, would drastically reduce the space of the middle meatus resulting in the condition of dysventilation.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brånemark, P.I.; Gröndahl, K.; Öhrnell, L.O.; Nilsson, P.; Petrusen, B.; Svensson, B.; Engstrand, P.; Nannmark, U. Zygoma fixture in the management of advanced atrophy of the maxilla: Technique and long-term results. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2004, 38, 70–85. [Google Scholar] [CrossRef]
- Aparicio, C.; Brånemark, P.-I.; Keller, E.E.; Olivé, J. Reconstruction of the premaxilla with autogenous iliac bone in combination with osseointegrated implants. Int. J. Oral Maxillofac. Implant. 1993, 8, 1–15. [Google Scholar]
- Wallace, S.S.; Froum, S.J. Effect of Maxillary Sinus Augmentation on the Survival of Endosseous Dental Implants. A Systematic Review. Ann. Periodontol. 2003, 8, 328–343. [Google Scholar] [CrossRef] [PubMed]
- Hallman, M.; Hedin, M.; Sennerby, L.; Lundgren, S. A prospective 1-year clinical and radiographic study of implants placed after maxillary sinus floor augmentation with bovine hydroxyapatite and autogenous bone. J. Oral Maxillofac. Surg. 2002, 60, 277–284. [Google Scholar] [CrossRef]
- Candel-Martí, E.; Carrillo-García, C.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Rehabilitation of Atrophic Posterior Maxilla with Zygomatic Implants: Review. J. Oral Implantol. 2011, 38, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Pedrosa, A.R.; Custódio, A.L.N. Zygomatic implants: A critical review of the surgical techniques. Oral Maxillofac. Surg. 2013, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Manresa, C.; Francisco, K.; Aparicio, A.; Nunes, J.; Claros, P.; Potau, J.M. Zygomatic Implants Placed Using the Zygomatic Anatomy-Guided Approach versus the Classical Technique: A Proposed System to Report Rhinosinusitis Diagnosis. Clin. Implant Dent. Relat. Res. 2014, 16, 627–642. [Google Scholar] [CrossRef] [PubMed]
- Stella, J.; Warner, M. Sinus slot technique for simplification and improved orientation of zygomaticus dental implants: A technical note. Int. J. Oral Maxillofac. Implant 2000, 15, 889–893. [Google Scholar]
- Bothur, S.; Jonsson, G. SL Modified technique using zygomatic implants in reconstruction of the atrophic maxilla: A technical note. Int. J. Oral Maxillofac. Implant 2003, 18, 902–904. [Google Scholar]
- Davó, R.; David, L. Quad Zygoma: Technique and Realities. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 285–297. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Survival and Complications of Zygomatic Implants: An Updated Systematic Review. J. Oral Maxillofac. Surg. 2016, 74, 1949–1964. [Google Scholar] [CrossRef] [PubMed]
- Sartori, E.M.; Padovan, L.E.M.; De Mattias Sartori, I.A.; Ribeiro, P.D.; Gomes De Souza Carvalho, A.C.; Goiato, M.C. Evaluation of satisfaction of patients rehabilitated with zygomatic fixtures. J. Oral Maxillofac. Surg. 2012, 70, 314–319. [Google Scholar] [CrossRef]
- Olarte, H.; Gómez-Delgado, A.; Trujillo-Saldarriaga, S.; Castro-Núñez, J. Inferior Meatal Antrostomy as a Prophylactic Maneuver to Prevent Sinusitis After Zygomatic Implant Placement Using the Intrasinusal Technique. Int. J. Oral Maxillofac. Implant 2015, 30, 862–867. [Google Scholar] [CrossRef]
- Chow, J.; Wat, P.; Hui, E.; Lee, P.; Li, W. A new method to eliminate the risk of maxillary sinusitis with zygomatic implants. Int. J. Oral Maxillofac. Implant 2010, 25, 1233–1240. [Google Scholar]
- Stiévenart, M.; Malevez, C. Rehabilitation of totally atrophied maxilla by means of four zygomatic implants and fixed prosthesis: A 6–40-month follow-up. Int. J. Oral Maxillofac. Surg. 2010, 39, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Hinze, M.; Vrielinck, L.; Thalmair, T.; Wachtel, H.; Bolz, W. Zygomatic Implant Placement in Conjunction with Sinus Bone Grafting: The “Extended Sinus Elevation Technique.” A Case-Cohort Study. Int. J. Oral Maxillofac. Implant 2013, 28, e376–e385. [Google Scholar] [CrossRef][Green Version]
- Boyes-Varley, J.G.; Howes, D.G.; Davidge-Pitts, K.D.; Mcalpine, J.A. A protocol for maxillary reconstruction following oncology resection using zygomatic implants. Int. J. Prosthodont. 2007, 20, 521. [Google Scholar]
- Becktor, J.P.; Isaksson, S.; Abrahamsson, P.; Sennerby, L. Evaluation of 31 zygomatic implants and 74 regular dental implants used in 16 patients for prosthetic reconstruction of the atrophic maxilla with cross-arch fixed bridges. Clin. Implant Dent. Relat. Res. 2005, 7, 159–165. [Google Scholar] [CrossRef]
- Kahnberg, K.E.; Henry, P.J.; Hirsch, J.M.; Öhrnell, L.O.; Andreasson, L.; Brånemark, P.I.; Chiapasco, M.; Gynther, G.; Finne, K.; Higuchi, K.W.; et al. Clinical Evaluation of the Zygoma Implant: 3-Year Follow-Up at 16 Clinics. J. Oral Maxillofac. Surg. 2007, 65, 2033–2038. [Google Scholar] [CrossRef]
- Lombardo, G.; D’Agostino, A.; Trevisiol, L.; Romanelli, M.G.; Mascellaro, A.; Gomez-Lira, M.; Pardo, A.; Favero, V.; Nocini, P.F. Clinical, microbiologic and radiologic assessment of soft and hard tissues surrounding zygomatic implants: A retrospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 537–546. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Altman, D.G. Systematic Reviews in Health Care: Meta-Analysis in Context; BMJ Publishing Group: London, UK, 2001; ISBN 0470693142. [Google Scholar]
- Migliorana, R.M.; Sotto-Maior, B.S.; Senna, P.M.; Francischone, C.E.; Cury, A.A.D.B. Immediate occlusal loading of extrasinus zygomatic implants: A prospective cohort study with a follow-up period of 8 years. Int. J. Oral Maxillofac. Surg. 2012, 41, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Maló, P.; Nobre Mde, A.; Lopes, A.; Ferro, A.; Moss, S. Five-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded zygomatic implants placed extra-maxillary. Eur. J. Oral Implantol. 2014, 7, 267–281. [Google Scholar] [PubMed]
- Nocini, P.F.; D’Agostino, A.; Chiarini, L.; Trevisiol, L.; Procacci, P. Simultaneous le fort I osteotomy and zygomatic implants placement with delayed prosthetic rehabilitation. J. Craniofac. Surg. 2014, 25, 1021–1024. [Google Scholar] [CrossRef]
- Urgell, J.P.; Gutiérrez, V.R.; Escoda, C.G. Rehabilitation of atrophic maxilla: A review of 101 zygomatic implants. Med. Oral Patol. Oral Cir. Bucal 2008, 13, 363–370. [Google Scholar]
- Davó, R.; Malevez, C.; Rojas, J.; Rodríguez, J.; Regolf, J. Clinical outcome of 42 patients treated with 81 immediately loaded zygomatic implants: A 12- to 42-month retrospective study. Eur. J. Oral Implantol. 2008, 1, 141–150. [Google Scholar]
- Davó, R. Zygomatic implants placed with a two-stage procedure: A 5-year retrospective study. Eur. J. Oral Implantol. 2009, 2, 115–124. [Google Scholar]
- Aparicio, C.; Manresa, C.; Francisco, K.; Ouazzani, W.; Claros, P.; Potau, J.M.; Aparicio, A. The Long-Term Use of Zygomatic Implants: A 10-Year Clinical and Radiographic Report. Clin. Implant Dent. Relat. Res. 2014, 16, 447–459. [Google Scholar] [CrossRef]
- Bertolai, R.; Aversa, A.; Catelani, C.; Rossi, A.; Giannini, D. Treatment of extreme maxillary atrophy with Zygoma implants. Minerva Stomatol. 2015, 64, 253–264. [Google Scholar]
- Araújo, R.; Sverzut, A.; Trivellato, A.; Sverzut, C. Retrospective Analysis of 129 Consecutive Zygomatic Implants Used to Rehabilitate Severely Resorbed Maxillae in a Two-Stage Protocol. Int. J. Oral Maxillofac. Implant. 2017, 32, 377–384. [Google Scholar] [CrossRef]
- Nave, P.; Queralt, A. Zygomatic Implants for the Rehabilitation of Atrophic Maxillae: A Retrospective Study on Survival Rate and Biologic Complications of 206 Implants with a Minimum Follow-up of 1 Year. Int. J. Oral Maxillofac. Implant. 2020, 35, 1177–1186. [Google Scholar] [CrossRef]
- Yalçın, M.; Can, S.; Akbaş, M.; Dergin, G.; Garip, H.; Aydil, B.; Varol, A. Retrospective Analysis of Zygomatic Implants for Maxillary Prosthetic Rehabilitation. Int. J. Oral Maxillofac. Implant. 2020, 35, 750–756. [Google Scholar] [CrossRef]
- D’Agostino, A.; Luciano, U.; Zangani, A.; Iurlaro, A.; Zarantonello, M.; Zotti, F.; Poscolere, A.; Modena, N.; Alberti, C.; Capocasale, G.; et al. Zygomatic implants supported rehabilitations in atrophic maxilla: Sinus complications, radiological, periodontal and prosthodontic evaluations: A one year follow up retrospective longitudinal study. J. Biol. Regul. Homeost. Agents 2020, 34, 89–100. [Google Scholar]
- Davó, R.; Malevez, C.; López-Orellana, C.; Pastor-Beviá, F.; Rojas, J. Sinus reactions to immediately loaded zygoma implants: A clinical and radiological study. Eur. J. Oral Implantol. 2008, 1, 53–60. [Google Scholar] [PubMed]
- Bothur, S.; Kullendorff, B.; Olsson-Sandin, G. Asymptomatic Chronic Rhinosinusitis and Osteitis in Patients Treated with Multiple Zygomatic Implants: A Long-Term Radiographic Follow-up. Int. J. Oral Maxillofac. Implant. 2015, 30, 161–168. [Google Scholar] [CrossRef]
- D’Agostino, A.; Favero, V.; Nocini, R.; Venco, J.; Nocini, P.F.; Trevisiol, L. Does Middle Meatal Antrostomy Prevent the Onset of Maxillary Sinusitis After Zygomatic Implant Placement? J. Oral Maxillofac. Surg. 2019, 77, 2475–2482. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, A.; Lombardo, G.; Favero, V.; Signoriello, A.; Bressan, A.; Lonardi, F.; Nocini, R.; Trevisiol, L. Complications related to zygomatic implants placement: A retrospective evaluation with 5 years follow-up. J. Cranio-Maxillofac. Surg. 2021, 49, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Parel, S.M.; Brånemark, P.I.; Ohrnell, L.O.; Svensson, B. Remote implant anchorage for the rehabilitation of maxillary defects. J. Prosthet. Dent. 2001, 86, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Manresa, C.; Franch, M. Extrasinus zygomatic implants: Three year experience from a new surgical approach for patients with pronounced buccal concavities in the edentulous maxilla. Clin. Implant Dent. Relat. Res. 2010, 12, 55–61. [Google Scholar] [CrossRef]
- Fakitsas, I.; Bountaniotis, F.; Fakitsas, D.; Theologie-Lygidakis, N.; Tzerbos, F. Complications of Zygomatic Implants: Our Clinical Experience with 4 Cases. Acta Stomatol. Croat. 2016, 50, 251–257. [Google Scholar] [CrossRef]
- Maló, P.; Nobre, M.D.; Lopes, A.; Francischone, C.; Rigolizzo, M. Three-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded extra-maxillary zygomatic implants. Eur. J. Oral Implantol. 2012, 5, 37–46. [Google Scholar] [PubMed]
- De Araújo Nobre, M.; Maló, P.; Gonçalves, I. Evaluation of Clinical Soft Tissue Parameters for Extramaxillary Zygomatic Implants and Conventional Implants in All-on-4 Hybrid Rehabilitations. Implant Dent. 2015, 24, 267–274. [Google Scholar] [CrossRef]
- Annino, D.J., Jr.; Laura, A. Goguen. Silent sinus syndrome. BMJ Case Rep. 2012, 2012, 18–21. [Google Scholar] [CrossRef]
- Hlaváčová, R.; Kuběna, T.Č. Silent Sinus Syndrome. Ces. Slov. Oftalmol. 2019, 74, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Messerkingler, W. Endoscopy of the Nose; Urban und Schwarzenberg: Baltimore, MD, USA, 1978. [Google Scholar]
- Davó, R.; Bankauskas, S.; Laurincikas, R.; Koçyigit, I.D.; Mate Sanchez de Val, J.E. Clinical Performance of Zygomatic Implants—Retrospective Multicenter Study. J. Clin. Med. 2020, 9, 480. [Google Scholar] [CrossRef]
- Duarte, L.R.; Filho, H.N.; Francischone, C.E.; Peredo, L.G.; Brånemark, P.I. The establishment of a protocol for the total rehabilitation of atrophic maxillae employing four zygomatic fixtures in an immediate loading system—A 30-month clinical and radiographic follow-up. Clin. Implant Dent. Relat. Res. 2007, 9, 186–196. [Google Scholar] [CrossRef]
- Doud Galli, S.K.; Lebowitz, R.A.; Giacchi, R.J.; Glickman, R.; Jacobs, J.B. Chronic Sinusitis Complicating Sinus Lift Surgery. Am. J. Rhinol. 2001, 15, 181–186. [Google Scholar] [CrossRef]
- Bedrossian, E. Rehabilitation of the edentulous maxilla with the zygoma concept: A 7-year prospective study. Int. J. Oral Maxillofac. Implant. 2010, 25, 1213. [Google Scholar]
- Magomedov, M.M.; Zeinalova, D.F.; Magomedova, N.M.; Starostina, A.E. The functional conditions of nasal cavity mucosa and paranasal sinuses following radical and minimally invasive surgical interventions. Vestn. Otorinolaringol. 2016, 81, 88–92. [Google Scholar] [CrossRef]
- Park, W.B.; Herr, Y.; Chung, J.H.; Shin, S.I.; Han, J.Y.; Lim, H.C. Long-term effects of sinus membrane perforation on dental implants placed with transcrestal sinus floor elevation: A case–control study. Clin. Implant Dent. Relat. Res. 2021, 23, 758–768. [Google Scholar] [CrossRef]

| Step | General Activities | Specific Activities |
|---|---|---|
| I | Formation of working group | Two otolaryngologists selected as experts in head and neck anatomy and sinusitis surgery, as clinical and methodological operators. |
| Two maxillofacial surgeons selected as expert in zygomatic implant surgery and in maxillary sinus anatomy, as clinical and methodological operators. | ||
| II | Formulation of the review questions | Evaluation of the state of art treatment of sinusitis, and complications following zygomatic implant surgery. Analysis of main complications of zygomatic implant surgery and their treatment |
| III | Identification of relevant studies on PubMed and PMC | 1. Identification of keywords in the field of interest |
| 2. Use of Boolean operator (AND) | ||
| 3. Inclusion criteria: no time limitation for works published; language: English; all types of full text articles. Exclusion criteria: no full text available, reviews of the literature and reviews of the literature with meta-analyses | ||
| 4. Elimination of duplicates | ||
| 5. Manual search through the references in selected articles | ||
| IV | Anaysis and presentation | Extrapolation of data from all revised studies and their presentation in the form of a narrative review |
| Search | Database |
|---|---|
| (zygomatic implants) AND (maxillary sinusitis) | PMC, PubMed, Ovid Scopus |
| (zygomatic surgery) AND (maxillary sinusitis) | PMC, PubMed, Ovid, Scopus |
| (zygomatic surgery) AND (sinusitis) | PMC, PubMed, Ovid, Scopus |
| (intrasinusal technique zygomatic implants) AND (maxillary sinusitis) | PMC, PubMed, Ovid, Scopus |
| (extrasinusal technique zygomatic implants) AND (maxillary sinusitis) | PMC, PubMed, Ovid, Scopus |
| (extrasinus zygomatic implants) AND (maxillary sinusitis) | PMC, PubMed, Ovid, Scopus |
| (extrasinus zygomatic implants) AND (complications) | PMC, PubMed, Ovid, Scopus |
| (intrasinusal zygomatic implants) AND (complications) | PMC, PubMed, Ovid, Scopus |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nocini, R.; Panozzo, G.; Trotolo, A.; Sacchetto, L. Maxillary Sinusitis as a Complication of Zygomatic Implants Placement: A Narrative Review. Appl. Sci. 2022, 12, 789. https://doi.org/10.3390/app12020789
Nocini R, Panozzo G, Trotolo A, Sacchetto L. Maxillary Sinusitis as a Complication of Zygomatic Implants Placement: A Narrative Review. Applied Sciences. 2022; 12(2):789. https://doi.org/10.3390/app12020789
Chicago/Turabian StyleNocini, Riccardo, Giorgio Panozzo, Alessandro Trotolo, and Luca Sacchetto. 2022. "Maxillary Sinusitis as a Complication of Zygomatic Implants Placement: A Narrative Review" Applied Sciences 12, no. 2: 789. https://doi.org/10.3390/app12020789
APA StyleNocini, R., Panozzo, G., Trotolo, A., & Sacchetto, L. (2022). Maxillary Sinusitis as a Complication of Zygomatic Implants Placement: A Narrative Review. Applied Sciences, 12(2), 789. https://doi.org/10.3390/app12020789