
Designing Personalized Persuasive Game Elements for Older Adults in Health Apps

Abstract
:1. Introduction
2. Related Work
3. Materials and Methods
3.1. Research Questions
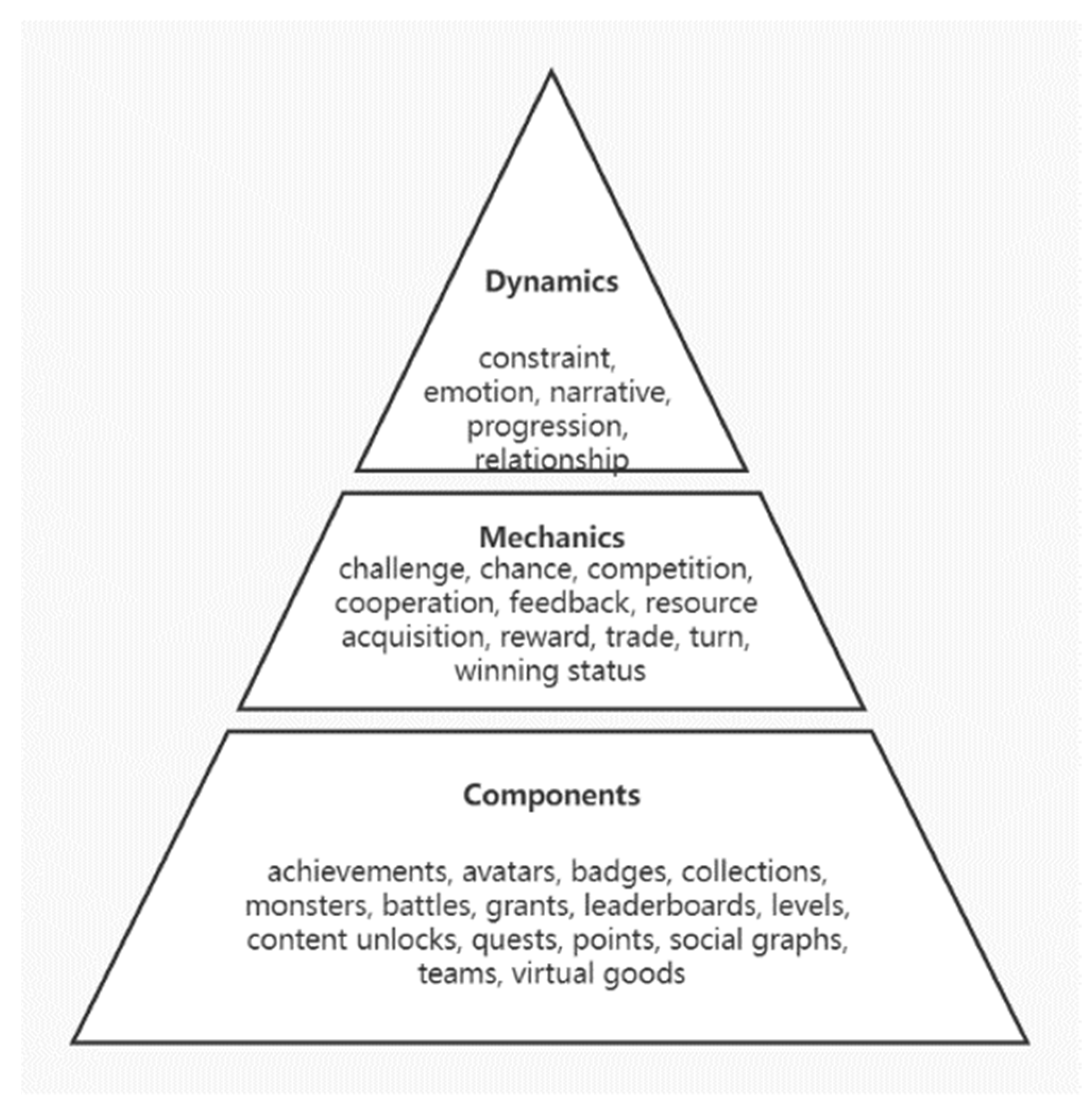
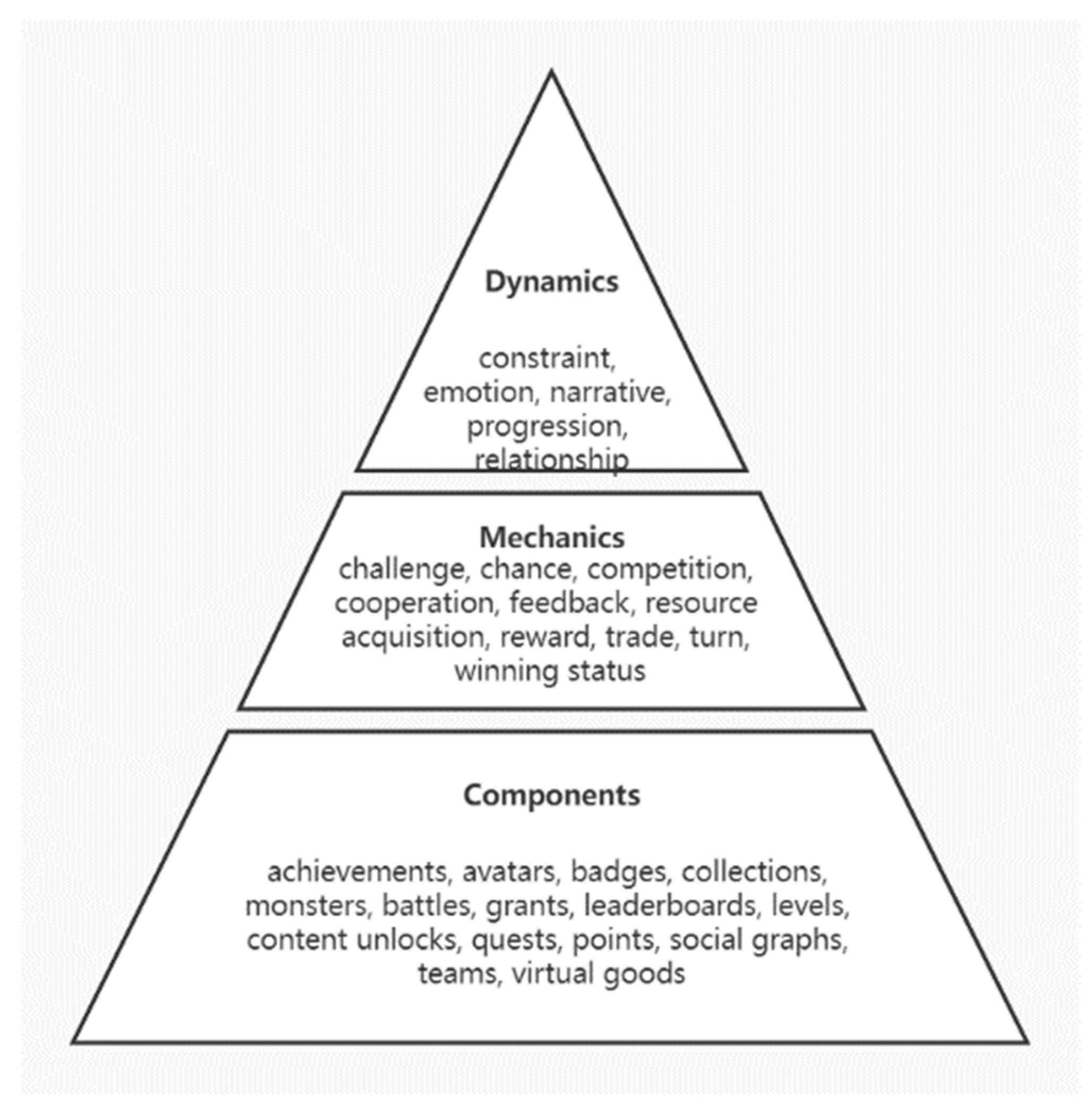
3.2. The DMC Model
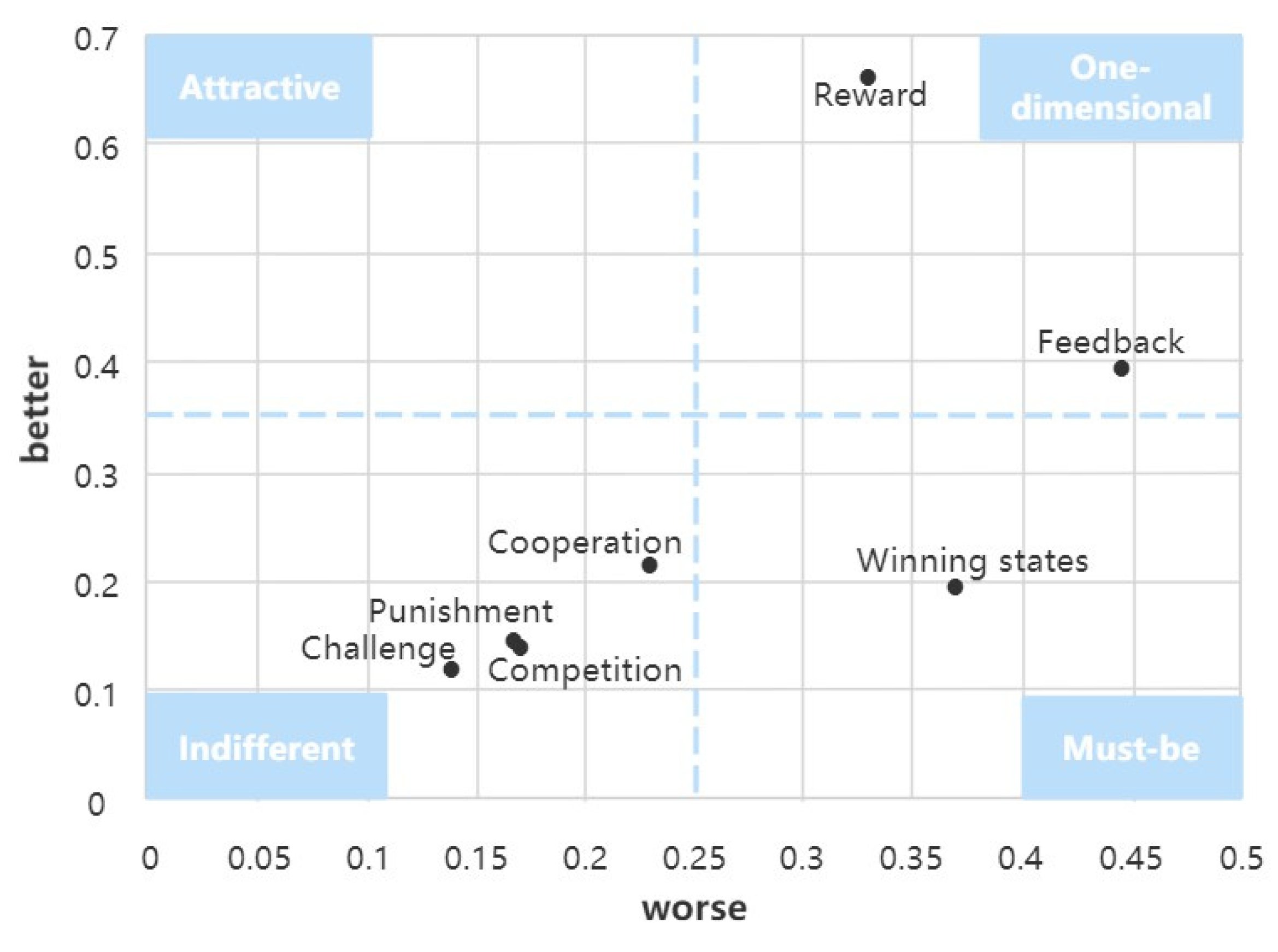
3.3. Kano Model
3.4. Conjoint Analysis Method
- (1)
- Determination of product features and feature levels: Joint analysis starts with the identification of the features of the product or service.
- (2)
- Product simulation: The conjoint analysis considers all the features and feature levels of the product, and uses the orthogonal design method to combine these features and feature levels to generate a series of virtual products.
- (3)
- Data collection: Respondents are asked to evaluate the virtual products, and respondents’ preferences for the virtual products are investigated by scoring and ranking, etc.
- (4)
- Calculating the utility of features: Separate the consumer’s preference values for each feature and the level of the feature from the collected information, and these preference values are also the utility of the feature.
- (5)
- Product prediction: Utility values are used to predict how consumers will choose from different products and thus decide what should be done.
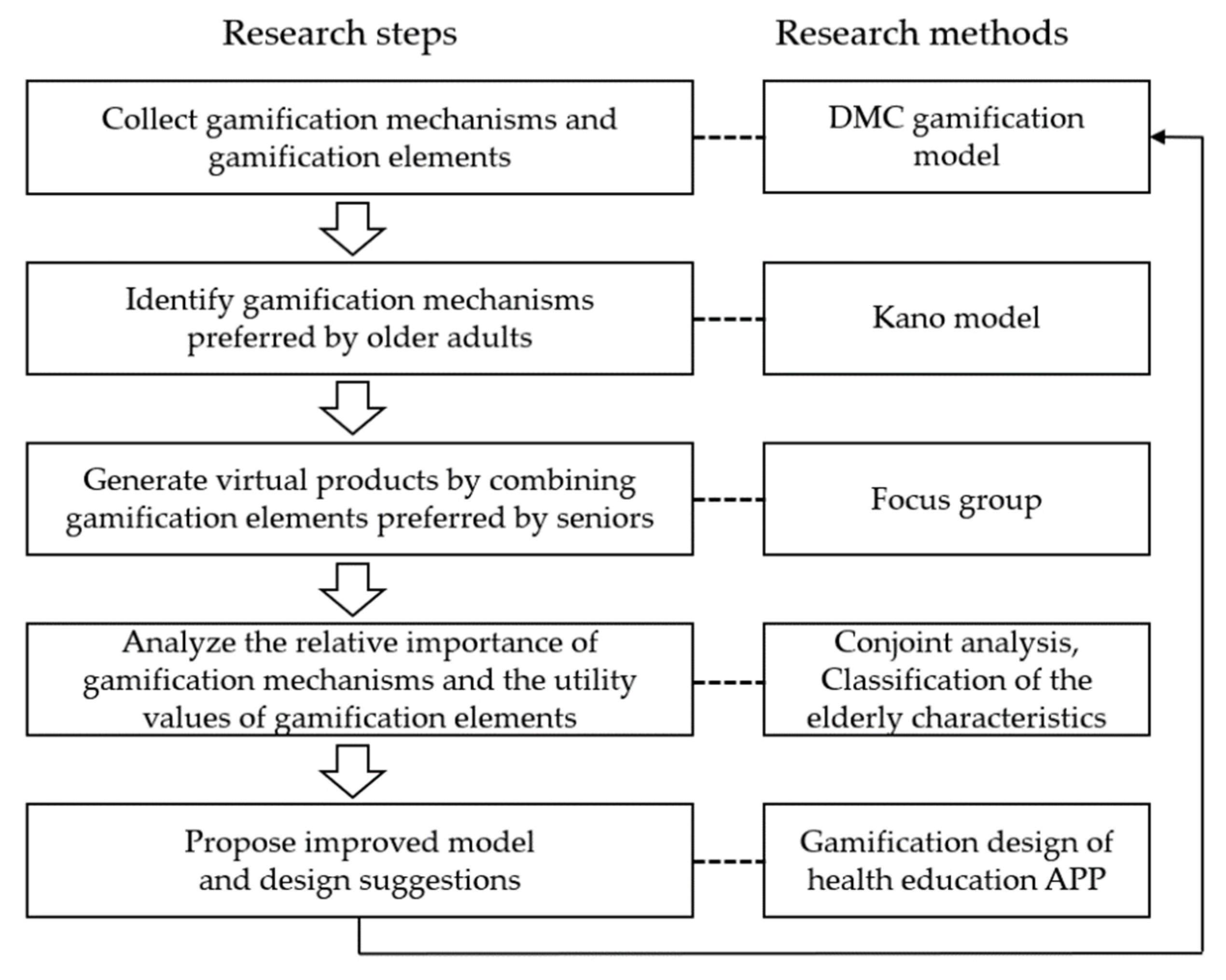
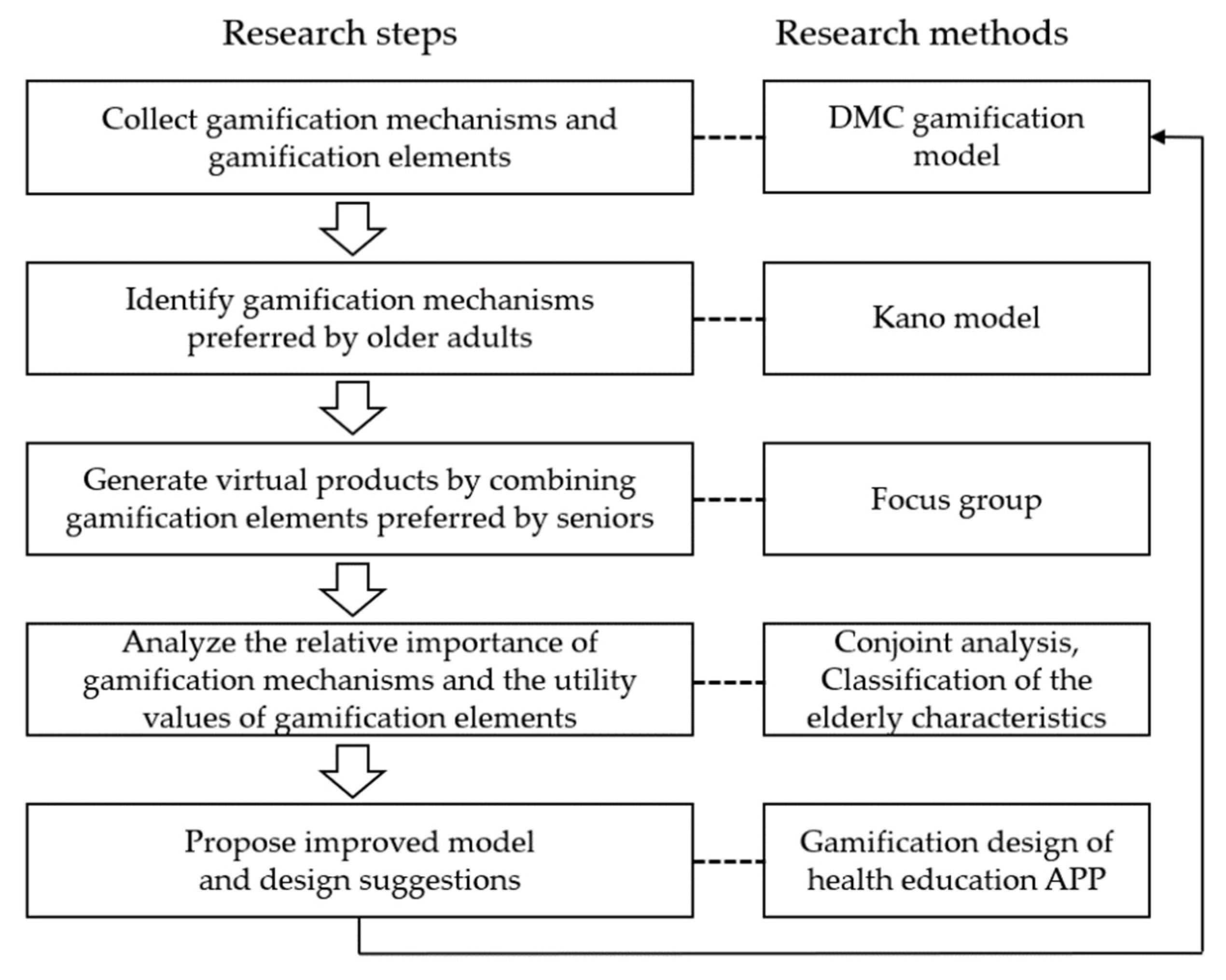
3.5. Research Framework
- (1)
- Screening the preferred gamification mechanics of the elderly. The demand attributes of gamification mechanisms were identified by the Kano model based on the DMC model.
- (2)
- Investigate the gamification elements preferred by older adults. The virtual products were designed with the gamification elements, and data from user evaluations were collected by the questionnaire.
- (3)
- Calculate the relative importance of game mechanics and the utility value of game elements using conjoint analysis. The preferred gamification elements were analyzed by comparing four characteristics of older adults (age, gender, income, and education).
- (4)
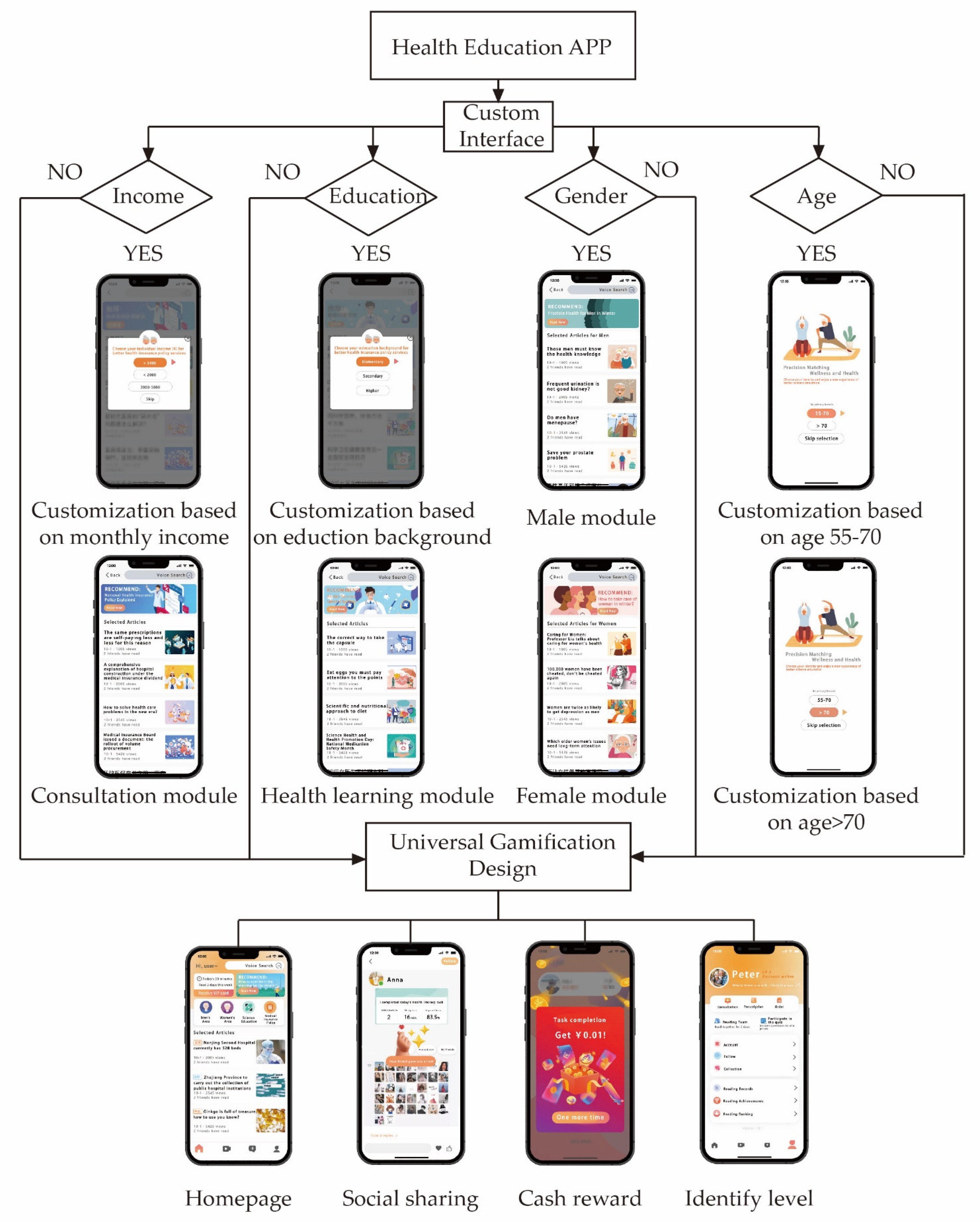
- Propose a modified gamification model and personalized gamification design suggestions for the senior health education app.
4. Results
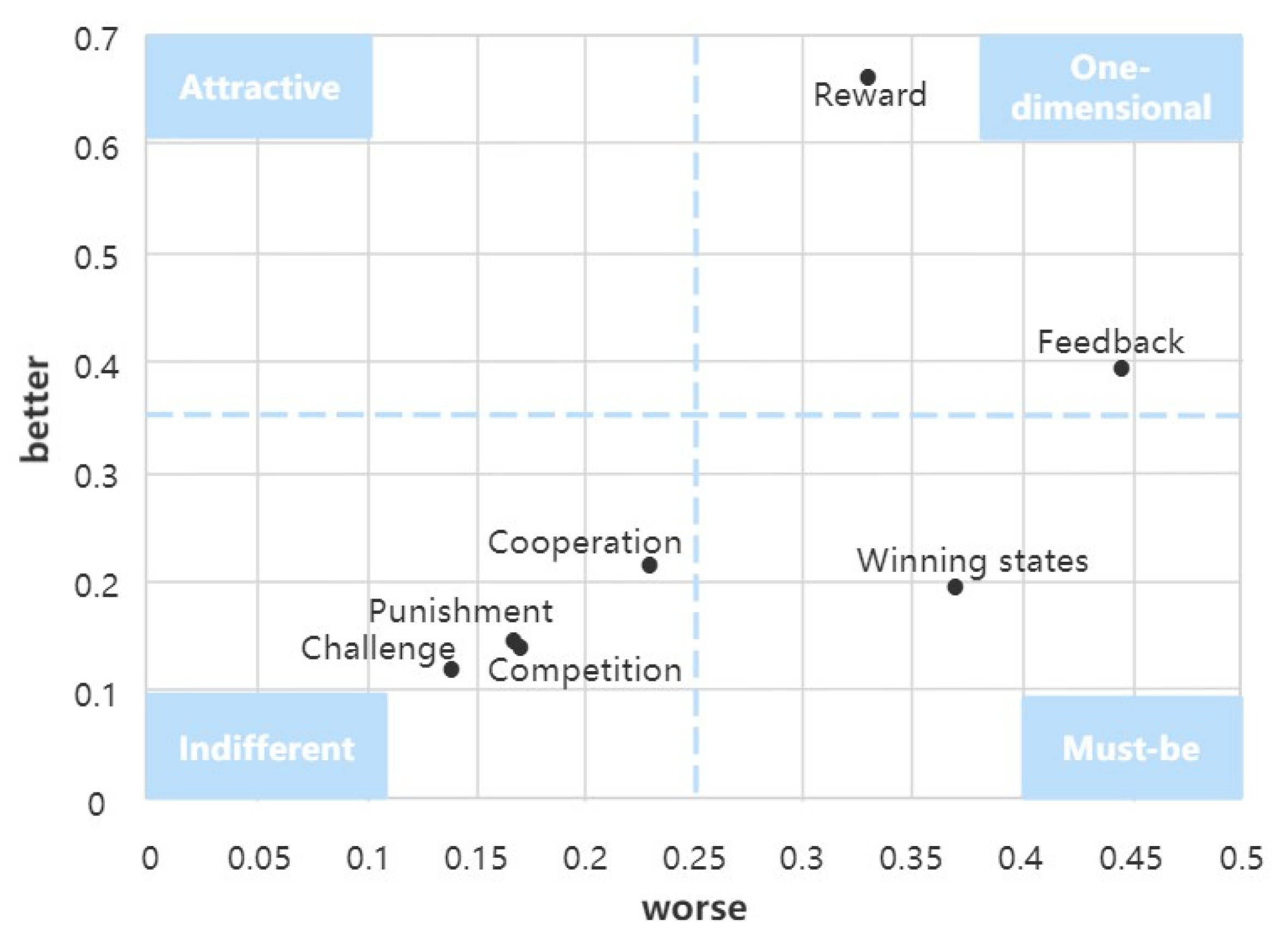
4.1. Screening the Gamification Mechanics Preferred by the Elderly
4.2. Conjoint Analysis Questionnaire
4.3. Conjoint Analysis Method to Analyze Gamification Elements
4.3.1. Overall Conjoint Analysis of the Elderly Population
4.3.2. Conjoint Analysis by Age Classification
4.3.3. Conjoint Analysis by Gender Classification
4.3.4. Conjoint Analysis by Educational Background
4.3.5. Conjoint Analysis by Income
4.3.6. Summary of the Conjoint Analysis Results
5. Discussion
5.1. Discussion of Study Results
- (1)
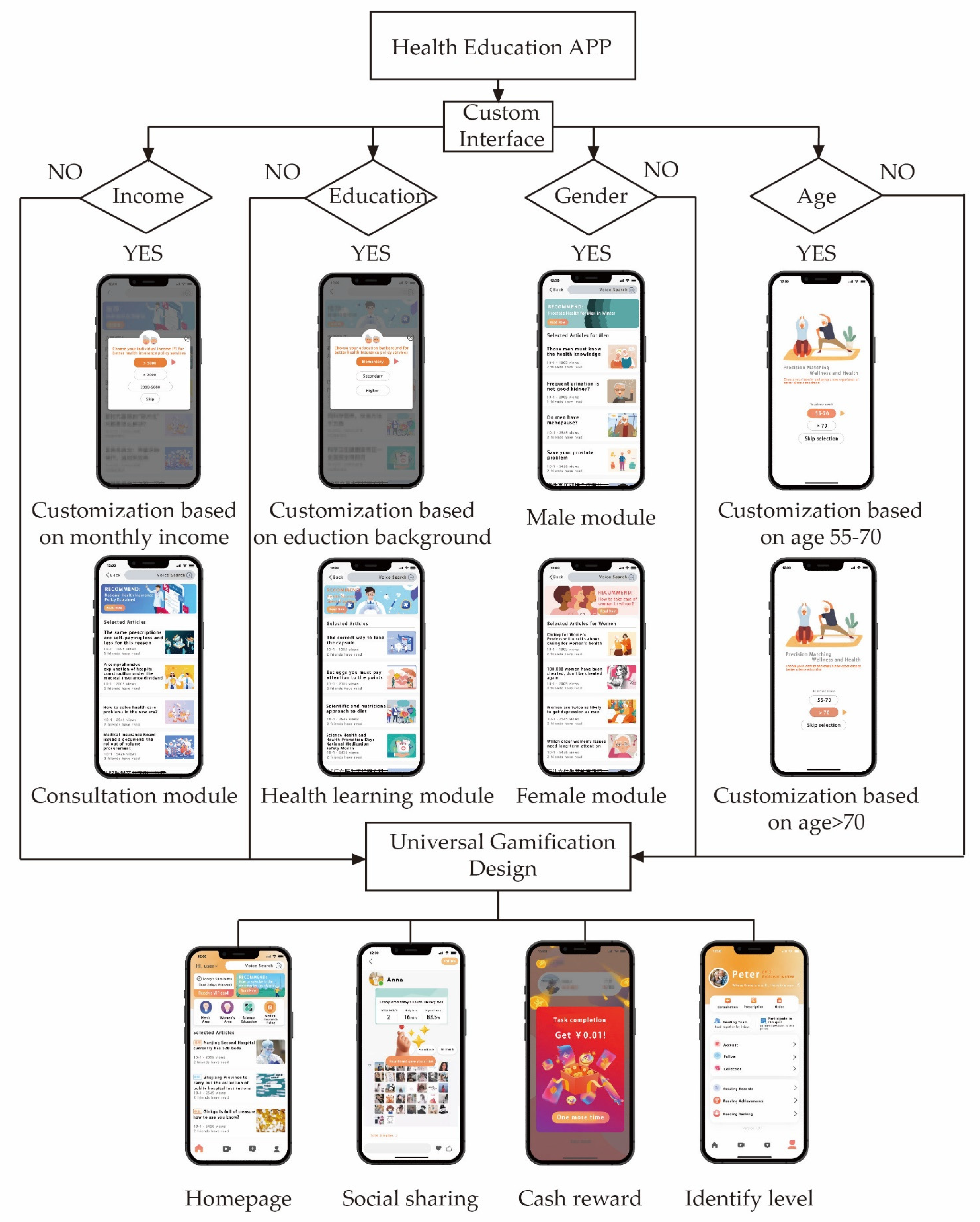
- Analysis by age characteristics. The results of the study (Table 7) show that lower-aged seniors (55–70 years old) preferred feedback mechanisms (46.939%), while higher-aged seniors (70 years old and above) preferred reward mechanisms (52.542%); and, in terms of gamification elements, they preferred status level feedback and cash rewards, respectively. The reason may be that the lower-aged seniors focused more on their personal social image, while the higher-aged seniors focused more on practical benefits. Design suggestions: Various virtual levels should be used to motivate the younger seniors, such as giving identity authentication and increasing the corresponding usage rights. Financial rewards should be used for the older seniors, such as issuing red packet rewards, or using points to exchange with gifts, etc.
- (2)
- Analysis by gender characteristics. Table 8 shows that both males and females preferred the winning status mechanism with a relative importance of 58.491% and 45.833%, respectively. However, males preferred the social sharing element and females preferred the leaderboard element. This indicates that female seniors were happy to show their status in a group, while male seniors felt pressured to display their personal status on the leaderboard because they were afraid of failing and would be embarrassed about it. Male older adults prefer to share personal achievements through socializing with friends and gaining appreciation. This indicates that females are susceptible to virtual gamification elements, and this finding is similar to that of other researchers [37], indicating the credibility of the results of this study. Design suggestions: Different winning status mechanisms should be used in the design for males and females to meet the psychological needs of older adults. In addition, designers should design cash rewards for male users and status level feedback for female users.
- (3)
- Analysis by educational background. Educational background not only limits the comprehension ability and prevalence of use of health education apps by older users [41], but also affects users’ preferences for game elements. The results of the study showed (Table 9) that those in the group with less than secondary educational background were more interested in cash reward, which is a material persuasion element. The group with higher education preferred social sharing on the winning status mechanism, which is a spiritual persuasion element. Design suggestions: Cash rewards or red packet rewards should be used for users with a primary education background, followed by graphic feedback. For users with a secondary education background, a leaderboard element is recommended in addition to designing cash rewards. Multiple social sharing elements should be used for users with higher education background, followed by rewards of random gifts and status rank feedback.
- (4)
- Analysis by monthly income. Income affects human needs to some extent. The results of the study (Table 10) indicate that both groups with low income and high income preferred feedback mechanisms with a relative importance of 46.154% and 50.000%, respectively. However, low-income people preferred visual feedback, which is a utility functional need, while high-income people preferred status rank feedback, which is a need to satisfy self-esteem psychology. The group with middle income preferred the winning status mechanism (53.488%), preferred the social sharing element, and wanted to receive praise from friends for their winning status. According to Maslow’s hierarchical needs theory [57], as income increases, users’ needs change from functional needs to social and self-esteem needs, and users tend to show their personal status as their income grows. Design suggestions: Visual feedback elements should be designed for low-income groups, followed by cash rewards. Social sharing in winning status should be designed for middle-income groups, followed by cash rewards. Status level feedback should be designed for higher income groups, followed by point rewards and leaderboards.
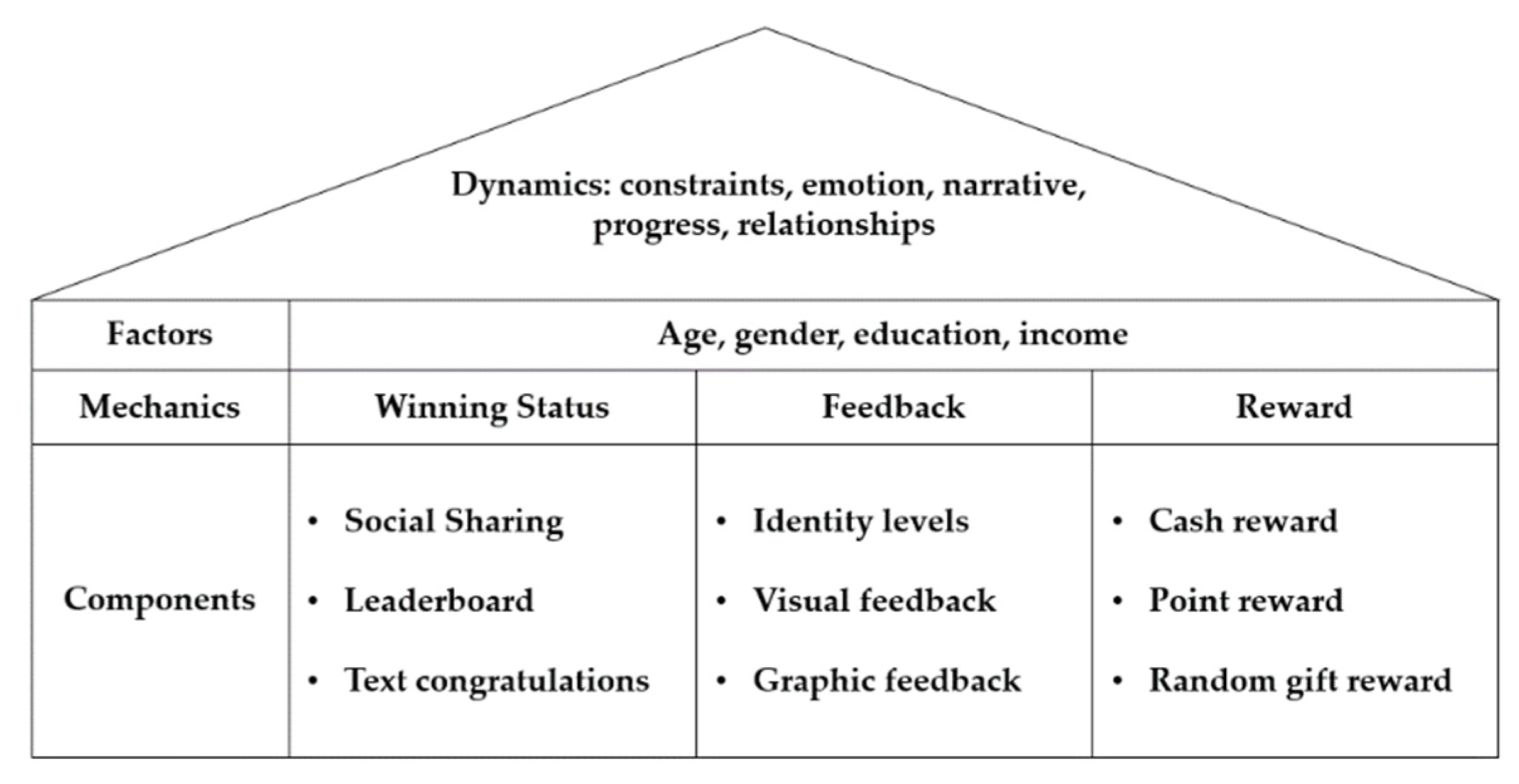
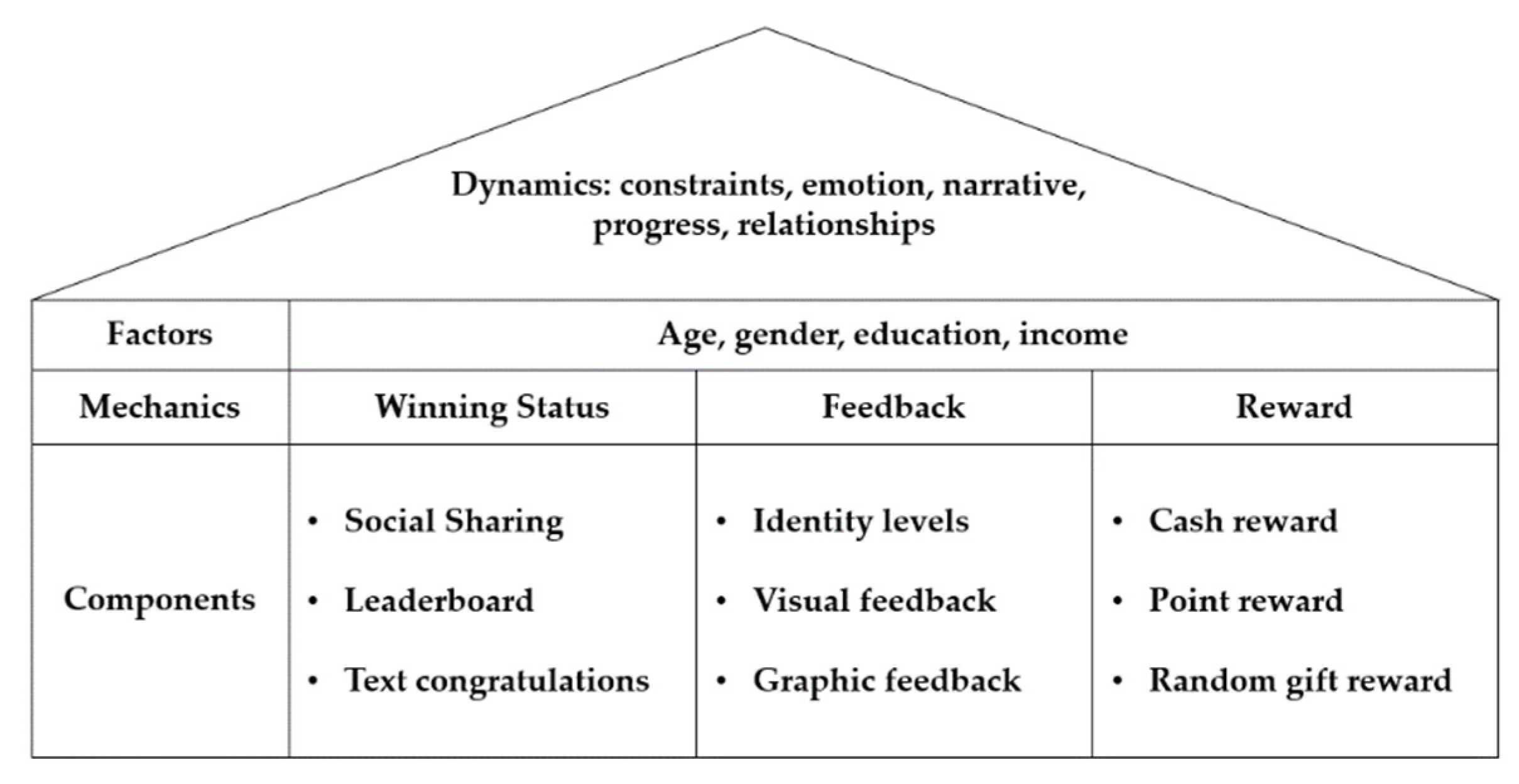
5.2. DMC Pyramid Improvement Model for Aging
- (1)
- The mechanism layer is simplified. The modified model is facilitated design applications for older users. There are three main gamification mechanisms preferred by the elderly, namely winning status, reward, and feedback. Winning status means the user demonstrates the status of personal victory. Reward means some achievements and benefits brought by the user through actions or operations. Feedback means that the progress of the operation is displayed to the user during the operation, so that the user can understand the process.
- (2)
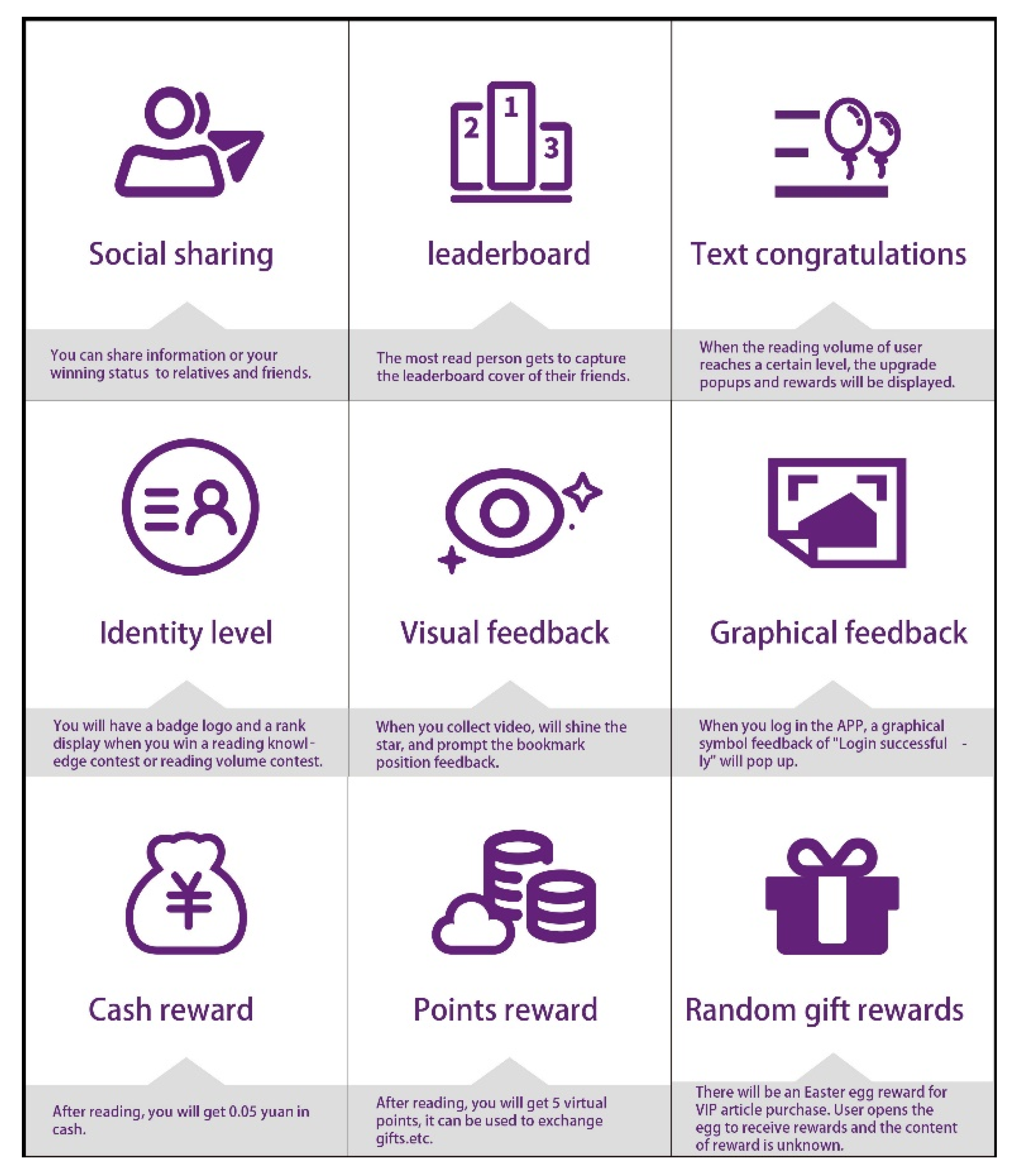
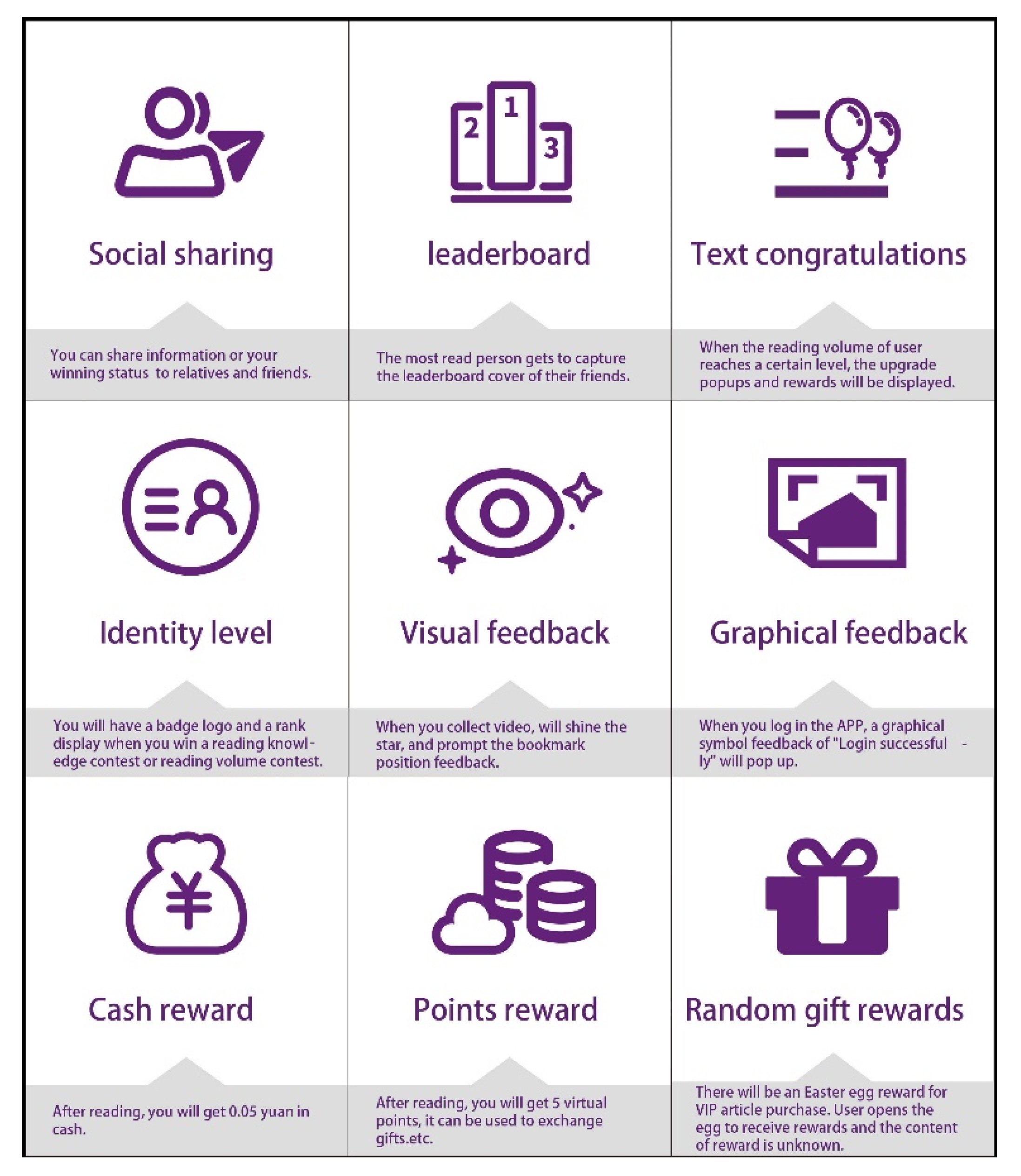
- The relationship between the mechanism layer and components layer was established. In this paper, the mechanism layer includes feedback, reward, and winning status. The component layer is the visual representation of the mechanism layer. The nine gamification elements are classified by the three mechanisms: social sharing, leaderboard, and text congratulations are the elements of winning status; cash rewards, point reward, and random gift rewards are the elements of the reward mechanism; and visual feedback, identity level, and graphic symbol feedback are the elements of the feedback mechanism.
- (3)
- In the designed application, the recommended gamification elements should be adopted according to four characteristics of the elderly (age, gender, monthly income, and educational background). The selection of elements for practical applications can refer to Table 12.
6. Conclusions
6.1. Research Conclusions and Contributions
6.2. Limitations and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fang, E.F.; Xie, C.; Schenkel, J.A.; Wu, C.; Long, Q.; Cui, H.; Aman, Y.; Frank, J.; Liao, J.; Zou, H.; et al. A research agenda for ageing in China in the 21st century (2nd edition): Focusing on basic and translational research, long-term care, policy and social networks. Ageing Res. Rev. 2020, 64, 101174. [Google Scholar] [CrossRef] [PubMed]
- China Country Assessment Report on Ageing and Health. Available online: https://www.who.int/publications-detail-redirect/9789241509312 (accessed on 1 January 2022).
- Ye, P.; Jin, Y.; Er, Y.; Duan, L.; Palagyi, A.; Fang, L.J.; Li, B.Q.; Ivers, R.; Keay, L.; Tian, M.Y. A scoping review of national policies for healthy ageing in mainland China from 2016 to 2020. Lancet Reg. Health-West. Pac. 2021, 12, 100168. [Google Scholar] [CrossRef] [PubMed]
- Busch, P.A.; Hausvik, G.I.; Ropstad, O.K.; Pettersen, D. Smartphone usage among older adults. Comput. Hum. Behav. 2021, 121, 106783. [Google Scholar] [CrossRef]
- Berenguer, A.; Goncalves, J.; Hosio, S.; Ferreira, D.; Anagnostopoulos, T.; Kostakos, V. Are smartphones ubiquitous? An in-depth survey of smartphone adoption by seniors. IEEE Trans. Consum. Electron. 2017, 6, 104–110. [Google Scholar] [CrossRef] [Green Version]
- John, P. Smartphone applications for patients’ health and fitness. Am. J. Med. 2016, 129, 11–19. [Google Scholar]
- Huang, G.; Ren, Y. Linking technological functions of fitness mobile apps with continuance usage among Chinese users: Moderating role of exercise self-efficacy. Comput. Hum. Behav. 2020, 103, 151–160. [Google Scholar] [CrossRef]
- Fogg, B.J. Persuasive technology: Using computers to change what we think and do. Ubiquity 2002, 2002, 763957. [Google Scholar] [CrossRef] [Green Version]
- Orji, R.; Mandryk, R.L.; Vassileva, J. Selecting Effective Strategies for Tailoring Persuasive Health Games to Gamer Types. In Proceedings of the GRAND 2014, Ottawa, ON, Canada, 14–16 May 2014. [Google Scholar]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From Game Design Elements to Gamefulness: Defining “Gamification”. In Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, New York, NY, USA, 28 September 2011; pp. 9–15. [Google Scholar]
- Werbach, K. Defining Gamification: A Process Approach, Persuasive Technology; Springer International Publishing: Cham, Switzerland, 2014; pp. 266–272. [Google Scholar]
- Johnson, D.; Deterding, S.; Kuhn, K.A.; Staneva, A.; Stoyanov, S.; Hides, L. Gamification for health and wellbeing: A systematic review of the literature. Internet Interv. 2016, 6, 89–106. [Google Scholar] [CrossRef] [Green Version]
- Treiblmaier, H.; Putz, L.M. Gamification as a moderator for the impact of intrinsic motivation: Findings from a multigroup field experiment. Learn. Motiv. 2020, 71, 101655. [Google Scholar] [CrossRef]
- Giráldez, V.A.; Sanmiguel-Rodríguez, A.; Álvarez, O.R.; Navarro-Patón, R. Can gamification influence the academic performance of students? Sustainability 2022, 14, 5115. [Google Scholar] [CrossRef]
- Dichev, C.; Dicheva, D. Gamifying education: What is known, what is believed and what remains uncertain: A critical review. Int. J. Educ. Technol. High. Educ. 2017, 14, 9. [Google Scholar] [CrossRef] [Green Version]
- Gentry, S.V.; Gauthier, A.; Ehrstrom, B.L.; Wortley, D.; Lilienthal, A.; Car, L.T.; Dauwels-Okutsu, S.; Nikolaou, C.K.; Zary, N.; Campbell, J.; et al. Serious gaming and gamification education in health professions: Systematic review. J. Med. Internet Res. 2019, 21, e12994. [Google Scholar] [CrossRef] [Green Version]
- Lister, C.; West, J.H.; Cannon, B.; Sax, T.; Brodegard, D. Just a fad? Gamification in health and fitness apps. JMIR Serious Games 2014, 2, e3413. [Google Scholar] [CrossRef] [PubMed]
- McCallum, S. Gamification and serious games for personalized health. Stud. Health Technol. Inform. 2012, 177, 85–96. [Google Scholar]
- Cafazzo, J.A.; Casselman, M.; Hamming, N.; Katzman, D.K.; Palmert, M.R. Design of an mhealth app for the self-management of adolescent type 1 diabetes: A pilot study. J. Med. Internet Res. 2012, 14, e2058. [Google Scholar] [CrossRef]
- Fijačko, N.; Gosak, L.; Cilar, L.; Novšak, A.; Creber, R.M.; Skok, P.; Štiglic, G. The effects of gamification and oral self-care on oral hygiene in children: Systematic search in app stores and evaluation of apps. JMIR Mhealth Uhealth 2020, 8, e16365. [Google Scholar] [CrossRef] [PubMed]
- Sarker, U.; Kanuka, H.; Norris, C.; Raymond, C.; Yonge, O.; Davidson, S. Gamification in nursing literature: An integrative review. Int. J. Nurs. Educ. Scholarsh. 2021, 1, 18. [Google Scholar] [CrossRef] [PubMed]
- Sailer, M.; Hense, J.U.; Mayr, K.S.; Mandl, H. How gamification motivates: An experimental study of the effects of specific game design elements on psychological need satisfaction. Comput. Hum. Behav. 2017, 69, 371–380. [Google Scholar] [CrossRef]
- Carrión-Toro, M.; Santorum, M.; Acosta-Vargas, P.; Aguilar, J.; Pérez, M. Iplus a user-centered methodology for serious games design. Appl. Sci. 2020, 10, 9007. [Google Scholar] [CrossRef]
- Gamecho, B.; Silva, H.; Guerreiro, J.; Gardeazabal, L.; Abascal, J. A context-aware application to increase elderly users compliance with physical rehabilitation exercises at home via animatronic biofeedback. J. Med. Syst. 2015, 39, 135. [Google Scholar] [CrossRef] [Green Version]
- Sardi, L.; Idri, A.; Fernández-Alemán, J.L. A systematic review of gamification in e-Health. J. Biomed. Inform. 2017, 71, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Kappen, D.L.; Mirza-Babaei, P.; Nacke, L.E. Technology facilitates physical activity through gamification: A thematic analysis of an 8-week study. Front. Comput. Sci. 2020, 2, 530309. [Google Scholar] [CrossRef]
- Koivisto, J.; Malik, A. Gamification for older adults: A systematic literature review. Gerontologist 2021, 61, e360–e372. [Google Scholar] [CrossRef] [PubMed]
- Toda, A.; Oliveira, W.; Shi, L.; Bittencourt, I.I.; Isotani, S.; Cristea, A. Planning Gamification Strategies Based on User Characteristics and DM: A Gender-Based Case Study. In Proceedings of the 12th International Conference on Educational Data Mining, Montreal, QC, Canada, 2–5 July 2019; pp. 438–443. [Google Scholar]
- Hanus, M.D.; Fox, J. Assessing the effects of gamification in the classroom: A longitudinal study on intrinsic motivation, social comparison, satisfaction, effort, and academic performance. Comput. Educ. 2015, 80, 152–161. [Google Scholar] [CrossRef]
- Santos, A.C.G.; Oliveira, W.; Hamari, J.; Rodrigues, L.; Toda, A.M.; Palomino, P.T.; Isotani, S. The relationship between user types and gamification designs. User Model. User-Adapt. Interact. 2021, 31, 907–940. [Google Scholar] [CrossRef]
- Vette, F.; Tabak, M.; Hermens, H.J.; Vollenbroek, M. Mapping Game Preferences of Older Adults: A Field Study towards Tailored Gamified Applications. In Proceedings of the 10th Nordic Conference on Human-Computer Interaction, Oslo, Norway, 29 September–3 October 2018; pp. 93–101. [Google Scholar]
- Kuo, C.M.; Chen, H.J. The Gamer Types of Seniors and Gamification Strategies toward Physical Activity. In International Conference on Human-Computer Interaction; Zhou, J., Salvendy, G., Eds.; Springer: Cham, Switzerland, 2019; pp. 177–188. [Google Scholar]
- Kappen, D.L.; Nacke, L.E.; Gerling, K.M.; Tsotsos, L.E. Design Strategies for Gamified Physical Activity Applications for Older Adults. In Proceedings of the 49th Hawaii International Conference on System Sciences, Washington, DC, USA, 5–8 January 2016. [Google Scholar]
- Vette, A.F.A.; Weering, M.; Tabak, M.; Vollenbroek-Hutten, M.M.R. Exploring Personality and Game Preferences in the Younger and Older Population: A Pilot Study. In Proceedings of the International Conference on Information and Communication Technologies for Ageing Well and e-Health, Rome, Italy, 21 April 2016; pp. 99–106. [Google Scholar]
- Shih, L.H.; Jheng, Y.C. Selecting persuasive strategies and game design elements for encouraging energy saving behavior. Sustainability 2017, 9, 1281. [Google Scholar] [CrossRef] [Green Version]
- Gerling, K.M.; Schulte, F.P.; Smeddinck, J.; Masuch, M. Game Design for Older Adults: Effects of Age-Related Changes on Structural Elements of Digital Games. In Entertainment Computing—ICEC 2012; Herrlich, M., Malaka, R., Masuch, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 7522, pp. 235–242. [Google Scholar]
- Denden, M.; Tlili, A.; Essalmi, F.; Jemni, M.; Chen, N.-S.; Burgos, D. Effects of gender and personality differences on students’ perception of game design elements in educational gamification. Int. J. Hum.-Comput. Stud. 2021, 154, 102674. [Google Scholar] [CrossRef]
- Yuan, T.; Guo, Y. Gamification Design of Health Apps for the Elderly Based on the Kano Model and Conjoint Analysis Method. In Human Aspects of IT for the Aged Population. Supporting Everyday Life Activities; Gao, Q., Zhou, J., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Abdullahi, A.M.; Orji, R.; Kawu, A.A. Gender, age and subjective well-being: Towards personalized persuasive health interventions. Information 2019, 10, 301. [Google Scholar] [CrossRef] [Green Version]
- Abdullahi, A.M.; Oyibo, K.; Orji, R.; Kawu, A.A. The influence of age, gender, and cognitive ability on the susceptibility to persuasive strategies. Information 2019, 10, 352. [Google Scholar] [CrossRef] [Green Version]
- Radhakrishnan, K.; Baranowski, T.; O’Hair, M.; Fournier, C.A.; Spranger, C.B.; Kim, M.T. Personalizing sensor-controlled digital gaming to self-management needs of older adults with heart failure: A qualitative study. Games Health J. 2020, 9, 304–310. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Y.; Liang, F.; Chen, Y.; Liu, L.; Li, Y.; Yao, H.; Chu, Q. The health literacy status and influencing factors of older population in xinjiang. Iran. J. Public Health 2015, 44, 913–919. [Google Scholar] [PubMed]
- Werbach, K.; Hunter, D. The Gamification Toolkit: Dynamics, Mechanics, and Components for the Win; Wharton School Press: Philadelphia, PA, USA, 2015. [Google Scholar]
- Kano, N.; Seraku, N.; Takahashi, F.; Tsuji, S. Attractive quality and must-be quality. J. Jpn. Soc. Qual. Control 1984, 14, 147–156. [Google Scholar]
- Green, P.E.; Srinivasan, V. Conjoint analysis in consumer research: Issues and outlook. J. Consum. Res. 1978, 5, 103–123. [Google Scholar] [CrossRef]
- Yin, S.; Cai, X.; Wang, Z.; Zhang, Y.; Luo, S.; Ma, J. Impact of gamification elements on user satisfaction in health and fitness applications: A comprehensive approach based on the Kano model. Comput. Hum. Behav. 2022, 128, 107106. [Google Scholar] [CrossRef]
- Min, S.H.; Kim, H.Y.; Kwon, Y.J.; Sohn, S.Y. Conjoint analysis for improving the e-book reader in the Korean market. Expert Syst. Appl. 2011, 38, 12923–12929. [Google Scholar] [CrossRef]
- Knudsen, J.K.; Havens, J.R. Using conjoint analysis to study health policy changes: An example from a cohort of persons who use drugs. Int. J. Drug Policy 2021, 98, 103425. [Google Scholar] [CrossRef]
- Pleger, L.E.; Mertes, A.; Rey, A.; Brüesch, C. Allowing users to pick and choose: A conjoint analysis of end-user preferences of public e-services. Gov. Inf. Q. 2020, 37, 101473. [Google Scholar] [CrossRef]
- Anand, A.; Bansal, G.; Aggrawal, D. Choice based diffusion model for predicting sales of mobile phones using conjoint analysis. J. High Technol. Manag. Res. 2018, 29, 216–226. [Google Scholar] [CrossRef]
- Zhang, J.; Wei, X.; Fukuda, H.; Zhang, L.; Ji, X. A Choice-based conjoint analysis of social media picture posting and souvenir purchasing preference: A case study of social analytics on tourism. Inf. Process. Manag. 2021, 58, 102716. [Google Scholar] [CrossRef]
- Chen, L. Research on consumer preference of remanufactured products based on conjoint analysis method. Shanghai Manag. Sci. 2020, 42, 46–53. [Google Scholar]
- Ho, H.H.; Tzeng, S.Y. Using the Kano model to analyze the user interface needs of middle-aged and older adults in mobile reading. Comput. Hum. Behav. 2021, 3, 100074. [Google Scholar] [CrossRef]
- Tabak, M.; Vette, F.; Dijk, H.; Vollenbroek-Hutten, M. A game-based, physical activity coaching application for older adults: Design approach and user experience in daily life. Games Health J. 2020, 9, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Motivation, Personality, and Development within Embedded Social Contexts: An Overview of Self-Determination Theory. In The Oxford Handbook of Human Motivation; Ryan, R.M., Ed.; Oxford University Press: Oxford, UK, 2012; p. 1e59. [Google Scholar]
- Tizuka, M.M.; Clua, E.W.G.; de Castro Salgado, L.C. Investigating m-Health Gamification Rewards Elements for Adults 50+. In Proceedings of the 2020 IEEE 8th International Conference on Serious Games and Applications for Health (SeGAH), Vancouver, BC, Canada, 12–14 August 2020. [Google Scholar]
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 50, 370–396. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.X.; Feng, L.N.; Li, S.X. The correlation between socioeconomic status and health self-management in the elderly. Int. J. Nurs. Stud. 2014, 1, 410–415. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| How Users Feel When This Feature Is Provided | ||||
|---|---|---|---|---|
| Very useful | More useful | Does not matter | Impractical | Very impractical |
| ⚪ | ⚪ | ⚪ | ⚪ | ⚪ |
| How users feel when this feature is not available | ||||
| Very useful | More useful | Does not matter | Impractical | Very impractical |
| ⚪ | ⚪ | ⚪ | ⚪ | ⚪ |
| Gamification Mechanics | Better–Worse Coefficient | Kano Attributes |
|---|---|---|
| Challenge | 0.1428, 0.1290 | Indifferent |
| Feedback | 0.4467, 0.3933 | One-dimensional |
| Competition | 0.1712, 0.1369 | Indifferent |
| Reward | 0.3377, 0.6623 | One-dimensional |
| Punishment | 0.1704, 0.1481 | Indifferent |
| Cooperation | 0.2353, 0.2157 | Indifferent |
| Winning status | 0.3701, 0.1948 | Must-be |
| Gamification Mechanics | Gamification Elements | Explanation |
|---|---|---|
| Winning status | Social sharing | Share personal achievements with familiar people and receive praise. |
| Leaderboard | Display the user’s ranking in the community. | |
| Text congratulations | A text pop-up appears to congratulate the user on completing the task. | |
| Reward | Cash reward | Give cash rewards when users complete operational tasks. |
| Point reward | Use points as a virtual currency and long-term points to provide exchange rewards. | |
| Random gift reward | Gift rewards for user actions, where the type and value of the gift are randomized to increase novelty and anticipation. | |
| Feedback | Identity level | The more tasks the user achieves, the higher the status level; feedback on the progress status of the individual. |
| Visual feedback | Color change (text or icon) to indicate the user’s operation status. | |
| Graphic feedback | Graphic descriptions of user operations. |
| Virtual Products | Feedback | Reward | Winning Status |
|---|---|---|---|
| 1 | Graphic feedback | Point reward | Text congratulations |
| 2 | Graphic feedback | Random gift reward | Social sharing |
| 3 | Identity level | Cash reward | Text congratulations |
| 4 | Identity level | Random gift reward | Leaderboard |
| 5 | Identity level | Point reward | Social sharing |
| 6 | Visual feedback | Random gift reward | Text congratulations |
| 7 | Visual feedback | Cash reward | Social sharing |
| 8 | Graphic feedback | Cash reward | Leaderboard |
| 9 | Visual feedback | Point reward | Leaderboard |
| Characteristic | Category | Number | Percentage |
|---|---|---|---|
| Gender | Male | 45 | 43.69% |
| Female | 58 | 56.31% | |
| Age | 55–70 years old | 79 | 76.70% |
| >70 years old | 24 | 23.30% | |
| Income (CNY) | <2000 | 16 | 15.53% |
| 2000–5000 | 52 | 50.49% | |
| >5000 | 35 | 33.98% | |
| Education | Elementary education (primary school) | 19 | 18.45% |
| Secondary education (middle school, high school, vocational high school, etc.) | 50 | 48.54% | |
| Higher education (university degree or higher) | 34 | 33.01% |
| Attribute | Attribute Level | Utility Value | Relative Importance |
|---|---|---|---|
| Feedback | Visual feedback | −0.03 | 10.204% |
| Identity level | 0.010 | ||
| Graphic feedback | −0.06 | ||
| Reward | Cash reward | 0.42 | 40.816% |
| Point reward | −0.023 | ||
| Random gift reward | −0.019 | ||
| Winning Status | Social sharing | 0.036 | 48.980% |
| Leaderboard | −0.042 | ||
| Text congratulations | 0.006 | ||
| Pearson’s R | 0.869 | p = 0.001 | |
| Kendall’s tau | 0.648 | p = 0.008 |
| Attribute | Attribute Level | Utility Value | |
|---|---|---|---|
| (Age 55–70) | (Age > 70) | ||
| Feedback | Visual feedback | −0.042 | 0.125 |
| Identity level | 0.055 | −0.139 | |
| Graphic feedback | −0.013 | 0.014 | |
| Relative importance | 46.939% | 32.203% | |
| Reward | Cash reward | −0.021 | 0.250 |
| Point reward | 0.025 | −0.181 | |
| Random gift reward | −0.004 | −0.069 | |
| Relative importance | 22.449% | 52.542% | |
| Winning Status | Social sharing | 0.03 | 0.069 |
| Leaderboard | −0.038 | −0.056 | |
| Text congratulations | 0.013 | −0.014 | |
| Relative importance | 30.612% | 15.254% | |
| Pearson’s R | 0.740 (p = 0.011) | 0.975 (p = 0.000) | |
| Kendall’s tau | 0.704 (p = 0.004) | 0.889 (p = 0.000) | |
| Attribute | Gamification Elements | Utility Value | |
|---|---|---|---|
| (Male) | (Female) | ||
| Feedback | Visual feedback | −0.022 | 0.011 |
| Identity level | 0.000 | 0.017 | |
| Graphic feedback | 0.022 | −0.029 | |
| Relative importance | 11.321% | 33.333% | |
| Reward | Cash reward | 0.074 | 0.017 |
| Point reward | −0.044 | −0.006 | |
| Random gift reward | −0.030 | −0.011 | |
| Relative importance | 30.189% | 20.833% | |
| Winning Status | Social sharing | 0.089 | −0.006 |
| Leaderboard | −0.141 | 0.034 | |
| Text congratulations | 0.052 | −0.029 | |
| Relative importance | 58.491% | 45.833% | |
| Pearson’s R | 0.860 (p = 0.001) | 0.975 (p = 0.000) | |
| Kendall’s tau | 0.889 (p = 0.000) | 0.923 (p = 0.001) | |
| Attribute | Gamification Elements | Utility Value | ||
|---|---|---|---|---|
| Primary Education | Secondary Education | Higher Education | ||
| Feedback | Visual feedback | 0.129 | −0.039 | −0.029 |
| Identity level | −0.170 | 0.020 | 0.071 | |
| Graphic feedback | 0.041 | 0.020 | −0.042 | |
| Relative importance | 38.636% | 11.765% | 22.973% | |
| Reward | Cash reward | 0.199 | 0.118 | −0.069 |
| Point reward | −0.170 | 0.000 | 0.018 | |
| Random gift reward | −0.029 | −0.118 | 0.051 | |
| Relative importance | 47.727% | 47.059% | 24.324% | |
| Winning Status | Social sharing | 0.041 | −0.078 | 0.111 |
| Leaderboard | −0.064 | 0.127 | −0.149 | |
| Text congratulations | 0.023 | −0.049 | 0.038 | |
| Relative importance | 13.636% | 41.176% | 52.703% | |
| Pearson’s R | 0.999 (p = 0.000) | 0.965 (p = 0.000) | 0.936 (p = 0.000) | |
| Kendall’s tau | 1.000 (p = 0.000) | 0.837 (p = 0.001) | 0.771 (p = 0.002) | |
| Attribute | Gamification Elements | Utility Value | ||
|---|---|---|---|---|
| <2000 | 2000–5000 | >5000 | ||
| Feedback | Visual feedback | 0.174 | 0.002 | −0.092 |
| Identity level | −0.201 | 0.009 | 0.108 | |
| Graphic feedback | 0.028 | −0.011 | −0.016 | |
| Relative importance | 46.154% | 6.977% | 50.000% | |
| Reward | Cash reward | 0.174 | 0.066 | −0.054 |
| Point reward | −0.139 | −0.043 | 0.060 | |
| Random gift reward | −0.035 | −0.024 | −0.006 | |
| Relative importance | 38.462% | 39.535% | 28.571% | |
| Winning Status | Social sharing | 0.028 | 0.060 | 0.003 |
| Leaderboard | −0.076 | −0.088 | 0.041 | |
| Text congratulations | 0.049 | 0.028 | −0.044 | |
| Relative importance | 15.385% | 53.488% | 21.429% | |
| Pearson’s R | 0.992 (p = 0.000) | 0.890 (p = 0.001) | 0.987 (p = 0.000) | |
| Kendall’s tau | 0.971 (p = 0.000) | 0.807 (p = 0.002) | 0.836 (p = 0.001) | |
| Characteristic | Category | Gamification Mechanics Recommendation |
|---|---|---|
| Overall | 103 subjects | Winning Status, Rewards, Feedback |
| Age | 55–70 years old | Feedback, Winning Status, Reward |
| >70 years old | Reward, Feedback, Winning Status | |
| Gender | Male | Winning Status, Reward, Feedback |
| Female | Winning Status, Feedback, Reward | |
| Educational background | Elementary education | Reward, Feedback, Winning Status |
| Secondary education | Reward/Winning Status, Feedback | |
| Higher education | Winning Status, Reward/Feedback | |
| Personal monthly income (CNY) | <2000 | Feedback, Reward, Winning Status |
| 2000–5000 | Winning Status, Reward, Feedback | |
| >5000 | Feedback, Reward/Winning Status |
| Characteristic | Category | Feedback | Rewards | Winning Status |
|---|---|---|---|---|
| Overall | 103 subjects | Identity level | Cash reward | Social sharing |
| Age | 55–70 years old | Identity level | Point reward | Social sharing |
| >70 years old | Visual feedback | Cash reward | Social sharing | |
| Gender | Male | Graphic feedback | Cash reward | Social sharing |
| Female | Identity level | Cash reward | Leaderboard | |
| Educational background | Elementary education | Visual feedback | Cash reward | Social sharing |
| Secondary education | Identity level/Graphic feedback | Cash reward | Leaderboard | |
| Higher education | Identity level | Random gift reward | Social sharing | |
| Income (CNY) | <2000 | Visual feedback | Cash reward | Text congratulations |
| 2000–5000 | Identity level | Cash reward | Social sharing | |
| >5000 | Identity level | Point reward | Leaderboard |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Yuan, T.; Yue, S. Designing Personalized Persuasive Game Elements for Older Adults in Health Apps. Appl. Sci. 2022, 12, 6271. https://doi.org/10.3390/app12126271
Guo Y, Yuan T, Yue S. Designing Personalized Persuasive Game Elements for Older Adults in Health Apps. Applied Sciences. 2022; 12(12):6271. https://doi.org/10.3390/app12126271
Chicago/Turabian StyleGuo, Yongyan, Tongyao Yuan, and Siyu Yue. 2022. "Designing Personalized Persuasive Game Elements for Older Adults in Health Apps" Applied Sciences 12, no. 12: 6271. https://doi.org/10.3390/app12126271
APA StyleGuo, Y., Yuan, T., & Yue, S. (2022). Designing Personalized Persuasive Game Elements for Older Adults in Health Apps. Applied Sciences, 12(12), 6271. https://doi.org/10.3390/app12126271