
Evaluation of the Operation Process of Medical Equipment to Enhance Ergonomic Reliability Based on FRAM–Moran’s I and CREAM

 , ,
, , 
Abstract
:1. Introduction
2. Operation Process Evaluation of Medical Equipment Based on Ergonomic Reliability Analysis
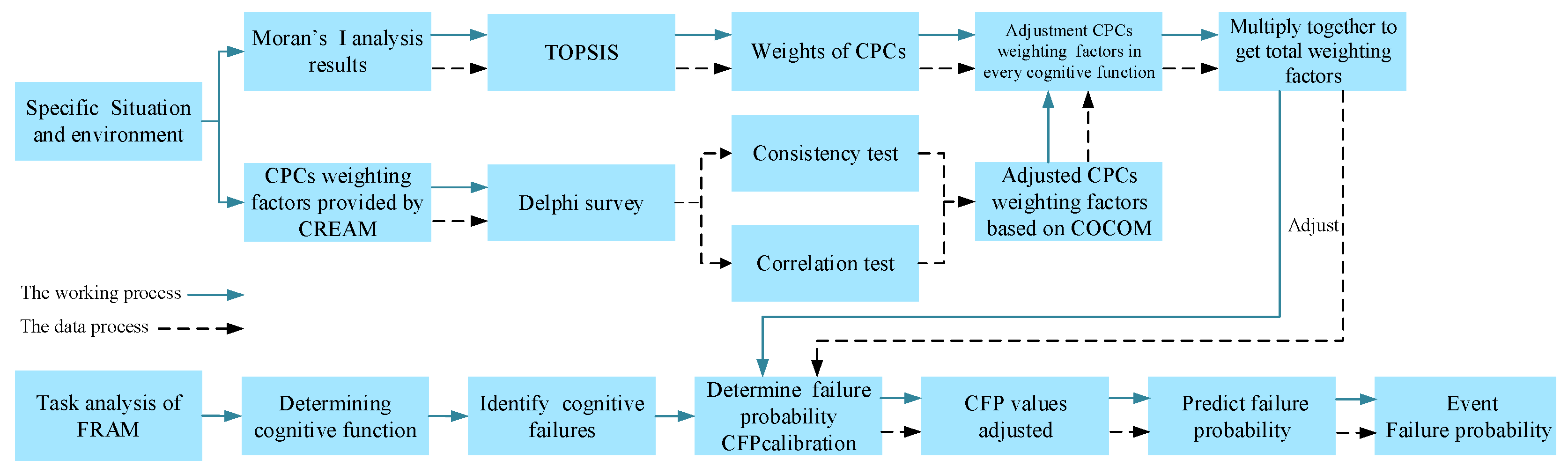
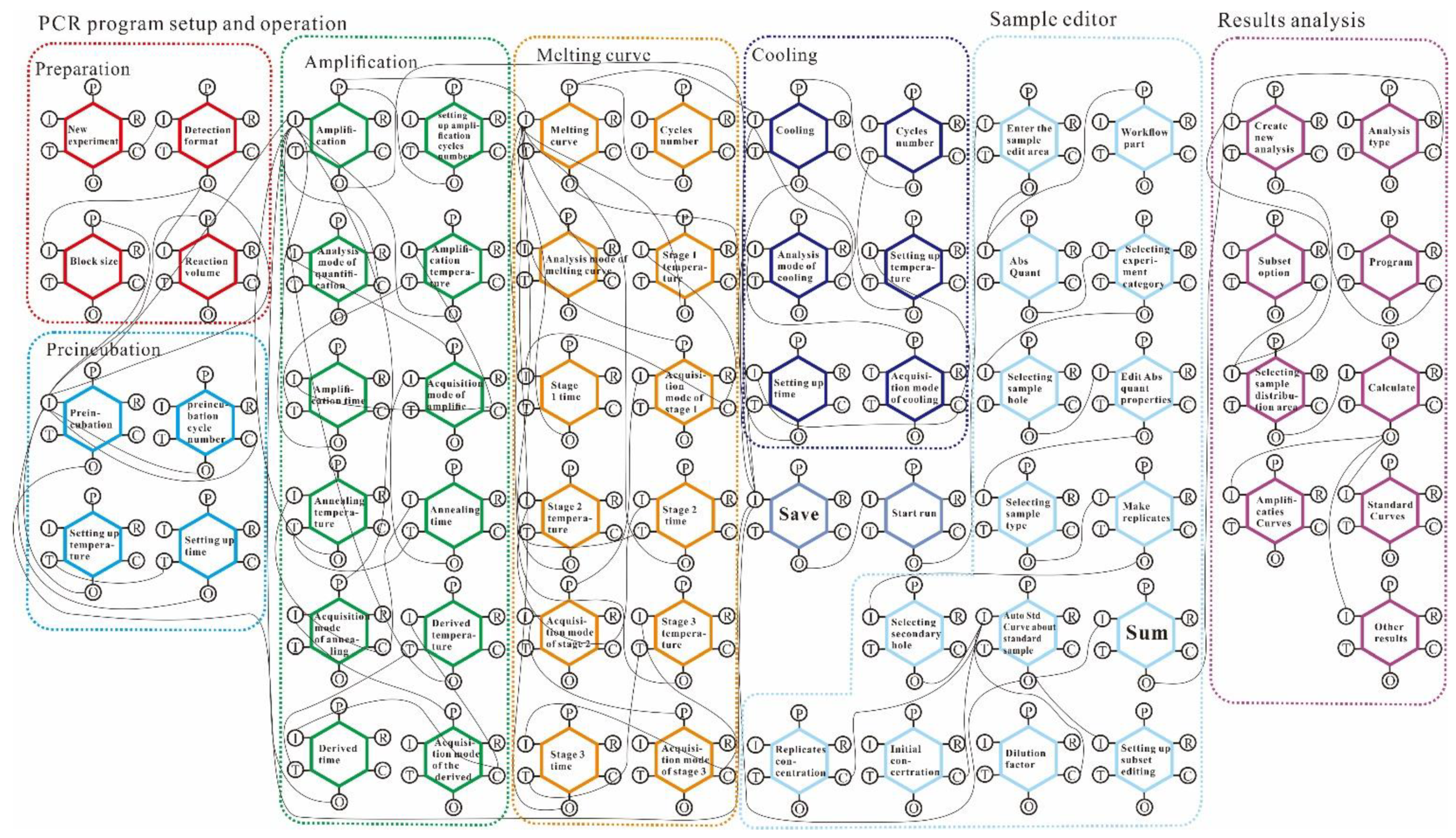
2.1. Operation Process Analysis Based on FRAM–Moran’s I
2.2. Ergonomics Reliability Analysis Based on Improved CREAM
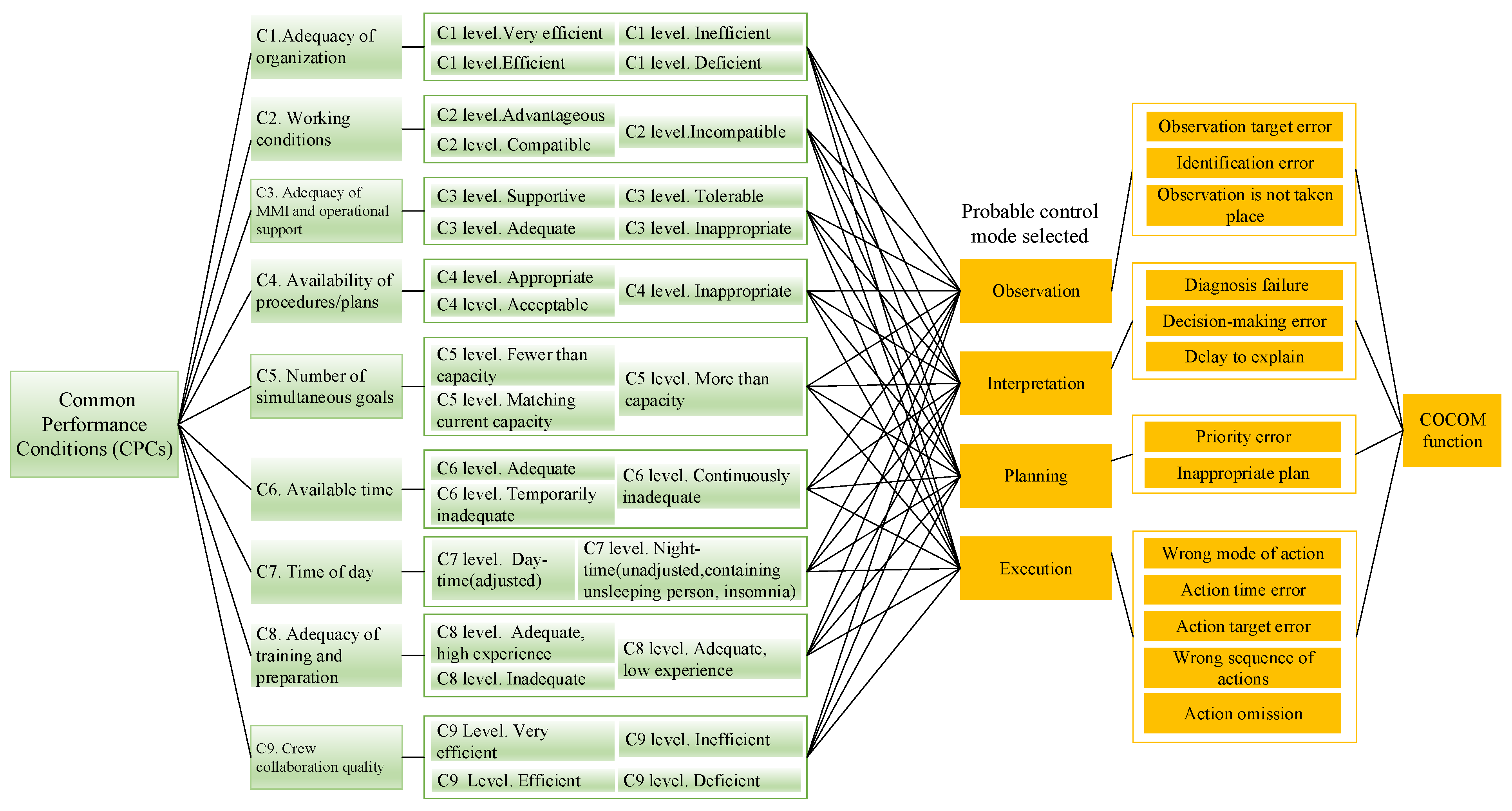
2.2.1. Assessment of Common Performance Conditions
2.2.2. Probability Adjustment Based on Cognitive Failure
3. Operation Process Evaluation in the Ergonomic Medical Equipment Interface
4. Verification Based on Ergonomic Reliability Experiments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Moran’s I | Moran’s Index |
| CREAM | Cognitive Reliability and Error Analysis Method |
| HRA | Human Reliability Analysis |
| FAHP | Fuzzy Analytic Hierarchy Process |
| FTA | Fault Tree Analysis |
| CPCs | Common performance conditions |
| FRAM | Functional Resonance Analysis Method |
| COCOM | Cognitive Control Mode |
| HEART | Human Error Assessment and Reduction Technique |
| TOPSIS | Technique for Order Preference by Similarity to an Ideal Solution |
| CFP | Cognitive Failure Probability |
| PCR | Polymerase Chain Reaction |
| ANOVA | Analysis of Variance |
| RMS | Root Mean Square |
| EMG | Electromyogram |
References
- Alvarenga, M.A.B.; E Melo, P.F. A review of the cognitive basis for human reliability analysis. Prog. Nucl. Energy 2019, 117, 103050. [Google Scholar] [CrossRef]
- Carayon, P.; Xie, A.; Kianfar, S. Human factors and ergonomics as a patient safety practice. BMJ Qual. Saf. 2014, 23, 196–205. [Google Scholar] [CrossRef]
- Sujan, M.A.; Embrey, D.; Huang, H. On the application of human reliability analysis in healthcare: Opportunities and challenges. Reliab. Eng. Syst. Saf. 2020, 194, 106189. [Google Scholar] [CrossRef] [Green Version]
- Zaitseva, E.; Levashenko, V.; Rabcan, J.; Krsak, E. Application of the structure function in the evaluation of the human factor in healthcare. Symmetry 2020, 12, 93. [Google Scholar] [CrossRef] [Green Version]
- Foster, J.D.; Miskovic, D.; Allison, A.S.; Conti, J.A.; Ockrim, J.; Cooper, E.J.; Hanna, G.B.; Francis, N.K. Application of objective clinical human reliability analysis (OCHRA) in assessment of technical performance in laparoscopic rectal cancer surgery. Tech. Coloproctol. 2016, 20, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Yuan, R.; Meng, D.; Li, H. Multidisciplinary reliability design optimization using an enhanced saddlepoint approximation in the framework of sequential optimization and reliability analysis. Proc. Inst. Mech. Engineers. Part O J. Risk Reliab. 2016, 230, 570–578. [Google Scholar] [CrossRef]
- Liu, X.; Liu, Z.; Liang, Z.; Zhu, S.-P.; Correia, J.A.F.O.; De Jesus, A.M.P. PSO-BP neural network-based strain prediction of wind turbine blades. Materials 2019, 12, 1889. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.F.; Huang, H.Z.; Mi, J.; Peng, W.; Han, X. Reliability analysis of multi-state systems with common cause failures based on Bayesian network and fuzzy probability. Ann. Oper. Res. 2019, 2019, 1–15. [Google Scholar] [CrossRef]
- Zheng, X.; Bolton, M.L.; Daly, C. Extended SAFPH℞ (Systems Analysis for Formal Pharmaceutical Human Reliability): Two approaches based on extended CREAM and a comparative analysis. Saf. Sci. 2020, 132, 104944. [Google Scholar] [CrossRef]
- Huang, C.; Huang, H.; Li, Y. A bidirectional LSTM prognostics method under multiple operational conditions. IEEE Trans. Ind. Electron. 2019, 66, 8792–8802. [Google Scholar] [CrossRef]
- Yuan, R.; Li, H. A multidisciplinary coupling relationship coordination algorithm using the hierarchical control methods of complex systems and its application in multidisciplinary design optimization. Adv. Mech. Eng. 2016, 9, 2071837610. [Google Scholar] [CrossRef] [Green Version]
- Mi, J.; Beer, M.; Li, Y.F.; Broggi, M.; Cheng, Y. Reliability and importance analysis of uncertain system with common cause failures based on survival signature. Reliab. Eng. Syst. Saf. 2020, 201, 106988. [Google Scholar] [CrossRef]
- Peng, W.; Ye, Z.; Chen, N. Bayesian deep-learning-based health prognostics toward prognostics uncertainty. IEEE Trans. Ind. Electron. 2020, 67, 2283–2293. [Google Scholar] [CrossRef]
- Zhou, Q.; Wong, Y.D.; Xu, H.; Van Thai, V.; Loh, H.S.; Yuen, K.F. An enhanced CREAM with stakeholder-graded protocols for tanker shipping safety application. Saf. Sci. 2017, 95, 140–147. [Google Scholar] [CrossRef]
- Chen, D.; Fan, Y.; Ye, C.; Zhang, S. Human reliability analysis for manned submersible diving process based on CREAM and Bayesian network. Qual. Reliab. Eng. Int. 2019, 35, 2261–2277. [Google Scholar] [CrossRef]
- He, Y.; Kuai, N.-S.; Deng, L.-M.; He, X.-Y. A method for assessing human error probability through physiological and psychological factors tests based on CREAM and its applications. Reliab. Eng. Syst. Saf. 2021, 215, 107884. [Google Scholar] [CrossRef]
- Ung, S.-T. A weighted CREAM model for maritime human reliability analysis. Saf. Sci. 2015, 72, 144–152. [Google Scholar] [CrossRef]
- He, X.; Wang, Y.; Shen, Z.; Huang, X. A simplified CREAM prospective quantification process and its application. Reliab. Eng. Syst. Saf. 2008, 93, 298–306. [Google Scholar] [CrossRef]
- Marseguerra, M.; Zio, E.; Librizzi, M. Quantitative developments in the cognitive reliability and error analysis method (CREAM) for the assessment of human performance. Ann. Nucl. Energy 2006, 33, 894–910. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, X.; Zeng, J. Application of modified extended method in CREAM for safety inspector in coal mines. IOP Conf. Ser. Earth Environ. Sci. 2018, 108, 32042. [Google Scholar] [CrossRef] [Green Version]
- Yuan, R.; Li, H.; Wang, Q. An enhanced genetic algorithm–based multi-objective design optimization strategy. Adv. Mech. Eng. 2018, 10, 2072047571. [Google Scholar] [CrossRef] [Green Version]
- Zupančič, J.; Marn, J. The synthesis of human-error analysis using the cognitive reliability and error analysis method and fault-tree analysis. Stroj. Vestn.-J. Mech. Eng. 2002, 48, 418–437. [Google Scholar]
- Alvarenga, M.A.B.; e Melo, P.F.; Fonseca, R.A. A critical review of methods and models for evaluating organizational factors in human reliability analysis. Prog. Nucl. Energy 2014, 75, 25–41. [Google Scholar] [CrossRef]
- Mi, J.; Li, Y.-F.; Peng, W.; Huang, H.-Z. Reliability analysis of complex multi-state system with common cause failure based on evidential networks. Reliab. Eng. Syst. Saf. 2018, 174, 71–81. [Google Scholar] [CrossRef]
- Li, H.; Guedes Soares, C.; Huang, H. Reliability analysis of a floating offshore wind turbine using Bayesian Networks. Ocean Eng. 2020, 217, 107827. [Google Scholar] [CrossRef]
- PPatriarca, R.; Di Gravio, G.; Woltjer, R.; Costantino, F.; Praetorius, G.; Ferreira, P.; Hollnagel, E. Framing the FRAM: A literature review on the functional resonance analysis method. Saf. Sci. 2020, 129, 104827. [Google Scholar] [CrossRef]
- França, J.E.; Hollnagel, E.; dos Santos, I.J.; Haddad, A.N. Analysing human factors and non-technical skills in offshore drilling operations using FRAM (functional resonance analysis method). Cogn. Technol. Work 2020, 23, 553–566. [Google Scholar] [CrossRef]
- Salehi, V.; Hanson, N.; Smith, D.; McCloskey, R.; Jarrett, P.; Veitch, B. Modeling and analyzing hospital to home transition processes of frail older adults using the functional resonance analysis method (FRAM). Appl. Ergon. 2021, 93, 103392. [Google Scholar] [CrossRef]
- Salehi, V.; Veitch, B.; Smith, D. Modeling complex socio-technical systems using the FRAM: A literature review. Hum. Factors Ergon. Manuf. Serv. Ind. 2021, 31, 118–142. [Google Scholar] [CrossRef]
- Clay-Williams, R.; Hounsgaard, J.; Hollnagel, E. Where the rubber meets the road: Using FRAM to align work-as-imagined with work-as-done when implementing clinical guidelines. Implement. Sci. 2015, 10, 125. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.; Veitch, B.; Khan, F.; Taylor, R. Understanding industrial safety: Comparing Fault tree, Bayesian network, and FRAM approaches. J. Loss Prev. Process Ind. 2017, 45, 88–101. [Google Scholar] [CrossRef]
- Haddad, A.N.; Rosa, L.V. Construction sustainability evaluation using AHP and FRAM methods. In Proceedings of the 2015 Industrial and Systems Engineering Research Conference, Nashville, TN, USA, 1 June 2015. [Google Scholar]
- Gattola, V.; Patriarca, R.; Tomasi, G.; Tronci, M. Functional resonance in industrial operations: A case study in a manufacturing plant. IFAC Pap. Line 2018, 51, 927–932. [Google Scholar] [CrossRef]
- Anvarifar, F.; Voorendt, M.Z.; Zevenbergen, C.; Thissen, W. An application of the Functional Resonance Analysis Method (FRAM) to risk analysis of multifunctional flood defences in the Netherlands. Reliab. Eng. Syst. Saf. 2017, 158, 130–141. [Google Scholar] [CrossRef]
- Albery, S.; Borys, D.; Tepe, S. Advantages for risk assessment: Evaluating learnings from question sets inspired by the FRAM and the risk matrix in a manufacturing environment. Saf. Sci. 2016, 89, 180–189. [Google Scholar] [CrossRef]
- Liu, Z.; Liu, X.; Wang, K.; Liang, Z.; Correia, J.A.; De Jesus, A.M. GA-BP neural network-based strain prediction in full-scale static testing of wind turbine blades. Energies 2019, 12, 1026. [Google Scholar] [CrossRef] [Green Version]
- Yuan, R.; Li, H.; Gong, Z.; Tang, M.; Li, W. An enhanced Monte Carlo simulation–based design and optimization method and its application in the speed reducer design. Adv. Mech. Eng. 2017, 9, 2071941952. [Google Scholar] [CrossRef] [Green Version]
- de Andrade Lima, R.C.; Resende, G.M. Using the Moran’s I to detect bid rigging in Brazilian procurement auctions. The Ann. Reg. Sci. 2020, 66, 237. [Google Scholar] [CrossRef]
- Mazhar, N.; Shirazi, S.A.; Stringer, L.C.; Carrie, R.H.; Dallimer, M. Spatial patterns in the adaptive capacity of dryland agricultural households in South Punjab, Pakistan. J. Arid Environ. 2021, 194, 104610. [Google Scholar] [CrossRef]
- Hirose, T.; Sawaragi, T. Development of FRAM model based on structure of complex adaptive systems to visualize safety of socio-technical systems. IFAC Pap. Line 2019, 52, 13–18. [Google Scholar] [CrossRef]
- Hirose, T.; Sawaragi, T.; Horiguchi, Y. Safety analysis of aviation flight-deck procedures using systemic accident model. IFAC Pap. Line 2016, 49, 19–24. [Google Scholar] [CrossRef]
- Yuan, R.; Li, H.; Wang, Q. Simulation-based design and optimization and fatigue characteristics for high-speed backplane connector. Adv. Mech. Eng. 2019, 11, 2072154763. [Google Scholar] [CrossRef] [Green Version]
- Sievert, A.; Witzki, A.; Nitzschner, M.M. Reliability and validity of low temporal resolution eye tracking systems in cognitive performance tasks. Int. J. Mob. Hum. Comput. Interact. 2018, 10, 40–51. [Google Scholar] [CrossRef] [Green Version]
- TOskouei, S.T.; Malliaras, P.; Hill, K.D.; Garofolini, A.; Clark, R.; Perraton, L. Assessment of ankle plantar flexor neuromuscular properties: A reliability study. J. Electromyogr. Kinesiol. 2021, 61, 102603. [Google Scholar]
- Kim, M.; Seong, P.; Hollnagel, E. A probabilistic approach for determining the control mode in CREAM. Reliab. Eng. Syst. Saf. 2006, 91, 191–199. [Google Scholar] [CrossRef]
- Williams, J.C. A data-based method for assessing and reducing human error to improve operational performance. In Proceedings of the Conference Record for 1988 IEEE Fourth Conference on Human Factors and Power Plants, Monterey, CA, USA, 5–9 June 1988. [Google Scholar]
- Li, H.; Teixeira, A.P.; Guedes Soares, C. A two-stage failure mode and effect analysis of offshore wind turbines. Renew. Energy 2020, 162, 1438–1461. [Google Scholar] [CrossRef]
- Yuan, R.; Tang, M.; Wang, H.; Li, H. A reliability analysis method of accelerated performance degradation based on Bayesian strategy. IEEE Access 2019, 7, 169047–169054. [Google Scholar] [CrossRef]
- Silva, A.G.; Simões, P.; Santos, R.; Queirós, A.; Rocha, N.P.; Rodrigues, M. A scale to assess the methodological quality of studies assessing usability of electronic health products and services: Delphi study followed by validity and reliability testing. J. Med. Internet Res. 2019, 21, e14829. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.K.; Oh, H.S.; Venture, J.A.; Kim, J.K.; Yoon, Y.J. Service reliability improvement in manufacturing and operating systems. Int. J. Precis. Eng. Manuf. 2013, 14, 1401–1406. [Google Scholar] [CrossRef]
- Li, H.; Díaz, H.; Guedes Soares, C. A failure analysis of floating offshore wind turbines using AHP-FMEA methodology. Ocean Eng. 2021, 234, 109261. [Google Scholar] [CrossRef]
- Koumantakis, G.A.; Arnall, F.; Cooper, R.G.; Oldham, J.A. Paraspinal muscle EMG fatigue testing with two methods in healthy volunteers. Reliability in the context of clinical applications. Clin. Biomech. 2001, 16, 263–266. [Google Scholar] [CrossRef]
- Scott, B.R.; Slattery, K.M.; Sculley, D.V.; Lockie, R.G.; Dascombe, B.J. Reliability of telemetric electromyography and near-infrared spectroscopy during high-intensity resistance exercise. J. Electromyogr. Kinesiol. 2014, 24, 722–730. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| C1 Levels | C2 Levels | C3 Levels | C4 Levels | C5 Levels | C6 Levels | C7 Levels | C8 Levels | C9 Levels | |
|---|---|---|---|---|---|---|---|---|---|
| Value of Kendall’s W | 0.102 | 0.164 | 0.112 | 0.117 | 0.121 | 0.186 | 0.075 | 0.148 | 0.147 |
| Adjusted value of Kendall’s W | 0.183 | 0.314 | 0.151 | 0.184 | 0.18 | 0.233 | 0.203 | 0.225 | 0.292 |
| Value of chi-square | 24.431 | 28.892 | 26.995 | 20.663 | 21.346 | 32.75 | 8.391 | 25.985 | 35.179 |
| Adjusted value of chi-square | 32.997 | 45.038 | 27.261 | 24.244 | 23.697 | 30.725 | 17.044 | 29.685 | 52.561 |
| P values | 0.058 | 0.002 | 0.029 | 0.037 | 0.03 | 0.001 | 0.299 | 0.007 | 0.002 |
| Adjusted P values | 0.05 | <0.005 | 0.027 | 0.012 | 0.014 | 0.001 | 0.017 | 0.002 | <0.005 |
| Degrees of freedom | 15 | 11 | 15 | 11 | 11 | 11 | 7 | 11 | 15 |
| Source | Sum of Squares | Degree of Freedom | Mean Square | F Test Statistic | P Value |
|---|---|---|---|---|---|
| Between group | 2403.87879 | 2 | 1201.93939 | 22.15 | <0.005 |
| Within group | 1628 | 30 | 54.2666667 | ||
| Total | 4031.87879 | 32 | 125.996212 |
| Comparison Group (1 and 2) | |
|---|---|
| B and A | 20.7273 (P = 0.000) |
| C and A | 8.0000 (P = 0.049) |
| B and C | 12.7273 (P = 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Liu, Z.; Lin, K.-C.; Huang, Z.-L.; Ling, M.-Y.; Chen, P.-Q.; Huang, X.-M.; Zhai, Y.-J. Evaluation of the Operation Process of Medical Equipment to Enhance Ergonomic Reliability Based on FRAM–Moran’s I and CREAM. Appl. Sci. 2022, 12, 200. https://doi.org/10.3390/app12010200
Liu X, Liu Z, Lin K-C, Huang Z-L, Ling M-Y, Chen P-Q, Huang X-M, Zhai Y-J. Evaluation of the Operation Process of Medical Equipment to Enhance Ergonomic Reliability Based on FRAM–Moran’s I and CREAM. Applied Sciences. 2022; 12(1):200. https://doi.org/10.3390/app12010200
Chicago/Turabian StyleLiu, Xin, Zheng Liu, Kang-Chao Lin, Zhi-Lin Huang, Ming-Yu Ling, Peng-Qing Chen, Xiao-Min Huang, and Yu-Jia Zhai. 2022. "Evaluation of the Operation Process of Medical Equipment to Enhance Ergonomic Reliability Based on FRAM–Moran’s I and CREAM" Applied Sciences 12, no. 1: 200. https://doi.org/10.3390/app12010200
APA StyleLiu, X., Liu, Z., Lin, K.-C., Huang, Z.-L., Ling, M.-Y., Chen, P.-Q., Huang, X.-M., & Zhai, Y.-J. (2022). Evaluation of the Operation Process of Medical Equipment to Enhance Ergonomic Reliability Based on FRAM–Moran’s I and CREAM. Applied Sciences, 12(1), 200. https://doi.org/10.3390/app12010200