
An Innovative and Cost-Advantage CAD Solution for Cubitus Varus Surgical Planning in Children

 , ,
, ,  , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
1.1. Cubitus Varus Syndrome
1.2. Cutting Guides for Surgery
2. Materials and Methods
2.1. Study Design and Clinical Case
2.2. Computer Aided Surgical Simulation
- ✓
- The plane of the distal osteotomy, approximately parallel to the distal articular surface, is placed approximately 10 mm above the olecranon fossa;
- ✓
- The proximal osteotomy plane forms an angle of 22° with the distal osteotomy plane.
2.3. Surgical Guide Planning
2.4. CAD Design of the Surgical Guide
2.5. 3D Printing of the Surgical Guide
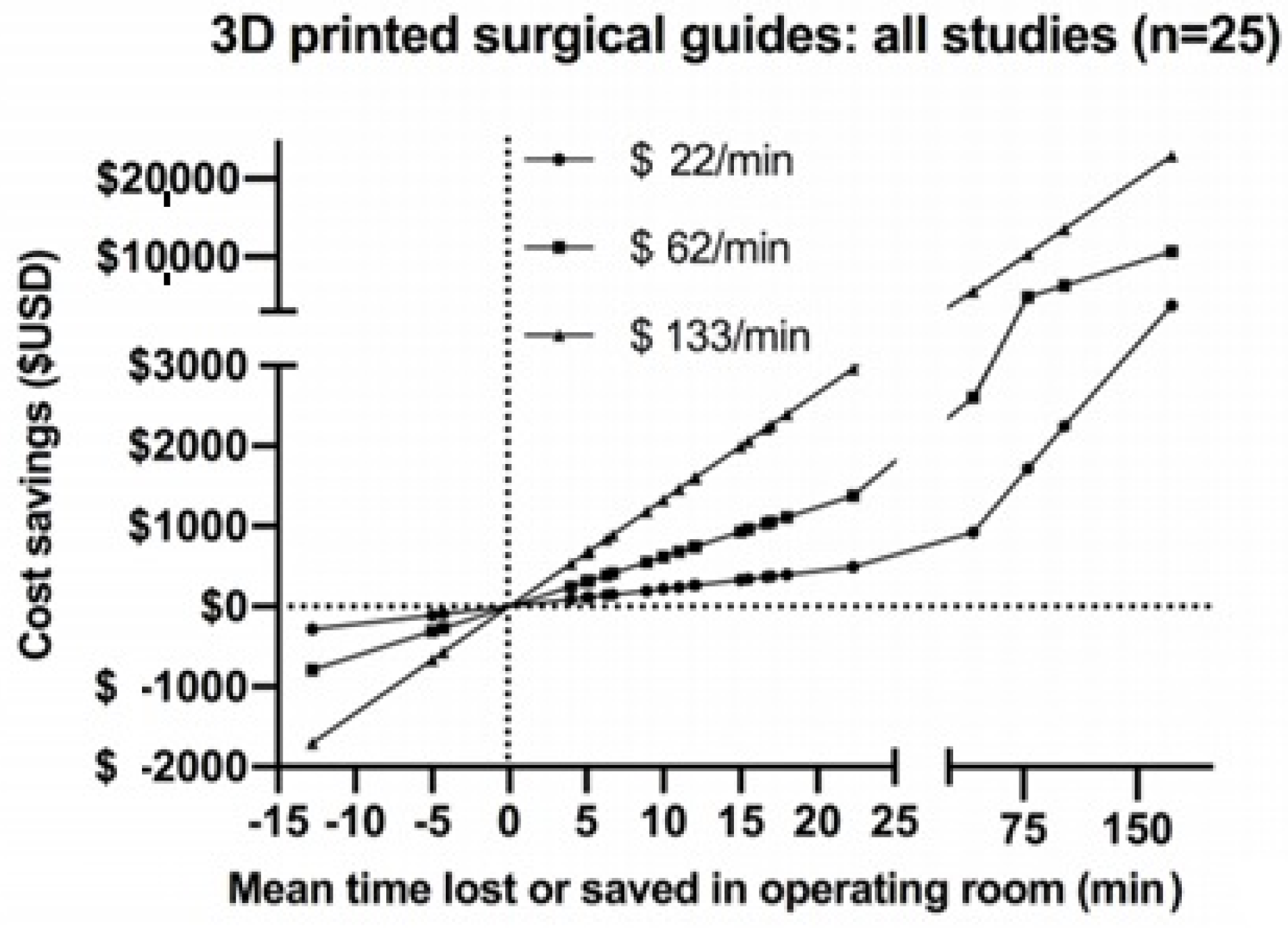
3. Results and Discussion
- the cost of materials;
- the purchase of the 3D printer;
- the cost of the software used;
- the cost of qualified personnel.
Proposed Improvements
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fini, M. Computer-Aided Surgery. ISTITUTO ORTOPEDICO RIZZOLI. (s.d.). Available online: http://www.ior.it/laboratori/lab-studi-precli-chirurg/computer-aided-surgery (accessed on 21 April 2021).
- Frizziero, L.; Santi, G.M.; Liverani, A.; Napolitano, F.; Papaleo, P.; Maredi, E.; Gennaro, G.L.D.; Zarantonello, P.; Stallone, S.; Stilli, S.; et al. Computer-Aided Surgical Simulation for Correcting Complex Limb Deformities in Children. Appl. Sci. 2020, 10, 5181. [Google Scholar] [CrossRef]
- Hafez, M. Custom-Made Cutting Guides for Total Knee Arthroplasty. Insall Scott Surg. Knee 2012, 1240–1254. [Google Scholar] [CrossRef]
- Ballard, D.H.; Mills, P.; Duszak, R.; Weisman, J.A.; Rybicki, F.J.; Woodard, P.K. Medical 3D Printing Cost-Savings in Orthopedic and Maxillofacial Surgery: Cost Analysis of Operating Room Time Saved with 3D Printed Anatomic Models and Surgical Guides. Acad. Radiol. 2020, 27, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Z.; Chen, B.; Lu, S.; Yang, Y.; Zhao, J.M.; Liu, R.; Li, Y.B.; Pei, G.X. Preliminary application of computer-assisted patient-specific acetabular navigational template for total hip arthroplasty in adult single development dysplasia of the hip: Computer-assisted surgery planning navigation template hip. Int. J. Med. Robot. Comput. Assist. Surg. 2011, 7, 469–474. [Google Scholar] [CrossRef]
- Hsu, A.R.; Davis, W.H.; Cohen, B.E.; Jones, C.P.; Ellington, J.K.; Anderson, R.B. Radiographic Outcomes of Preoperative CT Scan–Derived Patient-Specific Total Ankle Arthroplasty. Foot Ankle Int. 2015, 36, 1163–1169. [Google Scholar] [CrossRef]
- Chareancholvanich, K.; Narkbunnam, R.; Pornrattanamaneewong, C. A prospective randomised controlled study of patient-specific cutting guides compared with conventional instrumentation in total knee replacement. Bone Jt. J. 2013, 95-B, 354–359. [Google Scholar] [CrossRef]
- Abane, L.; Anract, P.; Boisgard, S.; Descamps, S.; Courpied, J.P.; Hamadouche, M. A comparison of patient-specific and conventional instrumentation for total knee arthroplasty. Bone Jt. J. 2015, 97-B, 56–63. [Google Scholar] [CrossRef]
- Barrack, R.L.; Ruh, E.L.; Williams, B.M.; Ford, A.D.; Foreman, K.; Nunley, R.M. Patient specific cutting blocks are currently of no proven value. J. Bone Jt. Surg. Br. 2012, 94-B, 95–99. [Google Scholar] [CrossRef]
- Barrett, W.; Hoeffel, D.; Dalury, D.; Mason, J.B.; Murphy, J.; Himden, S. In-Vivo Alignment Comparing Patient Specific Instrumentation with both Conventional and Computer Assisted Surgery (CAS) Instrumentation in Total Knee Arthroplasty. J. Arthroplast. 2014, 29, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Boonen, B.; Schotanus, M.G.M.; Kort, N.P. Preliminary experience with the patient-specific templating total knee arthroplasty. Acta Orthop. 2012, 83, 387–393. [Google Scholar] [CrossRef]
- Boonen, B.; Schotanus, M.G.M.; Kerens, B.; van der Weegen, W.; van Drumpt, R.A.M.; Kort, N.P. Intra-operative results and radiological outcome of conventional and patient-specific surgery in total knee arthroplasty: A multicentre, randomised controlled trial. Knee Surgery, Sports Traumatology. Arthroscopy 2013, 21, 2206–2212. [Google Scholar] [CrossRef]
- Ferdinando, F.; Antonio, C.; Nicola, M.; Santi, R.; Vincenzo, D.S.; Aaron, B.; Antonio, L.; Lorenzo, B. Implant Positioning in TKA: Comparison Between Conventional and Patient-Specific Instrumentation. Orthopedics 2015, 38, e271–e280. [Google Scholar] [CrossRef]
- Gan, Y.; Ding, J.; Xu, Y.; Hou, C. Accuracy and efficacy of osteotomy in total knee arthroplasty with patient-specific navigational template. Int. J. Clin. Exp. Med. 2015, 8, 12192–12201. [Google Scholar] [PubMed]
- Hamilton, W.G.; Parks, N.L.; Saxena, A. Patient-Specific Instrumentation Does Not Shorten Surgical Time: A Prospective, Randomized Trial. J. Arthroplasty 2013, 28, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Kassab, S.; Pietrzak, W.S. Patient-specific positioning guides versus manual instrumentation for total knee arthroplasty: An intraoperative comparison. J. Surg. Orthop. Adv. 2014, 23, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Kerens, B.; Schotanus, M.G.M.; Boonen, B.; Kort, N.P. No radiographic difference between patient-specific guiding and conventional Oxford UKA surgery. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1324–1329. [Google Scholar] [CrossRef]
- Nankivell, M.; West, G.; Pourgiezis, N. Operative efficiency and accuracy of patient-specific cutting guides in total knee replacement. ANZ J. Surg. 2015, 85, 452–455. [Google Scholar] [CrossRef]
- Noble, J.W.; Moore, C.A.; Liu, N. The Value of Patient-Matched Instrumentation in Total Knee Arthroplasty. J. Arthroplasty 2012, 27, 153–155. [Google Scholar] [CrossRef]
- Nunley, R.M.; Ellison, B.S.; Ruh, E.L.; Williams, B.M.; Foreman, K.; Ford, A.D.; Barrack, R.L. Are Patient-specific Cutting Blocks Cost-effective for Total Knee Arthroplasty? Clin. Orthop. Relat. Res. 2012, 470, 889–894. [Google Scholar] [CrossRef]
- Pfitzner, T.; Abdel, M.P.; von Roth, P.; Perka, C.; Hommel, H. Small Improvements in Mechanical Axis Alignment Achieved with MRI versus CT-based Patient-specific Instruments in TKA: A Randomized Clinical Trial. Clin. Orthop. Relat. Res. 2014, 472, 2913–2922. [Google Scholar] [CrossRef]
- Pietsch, M.; Djahani, O.; Zweiger, C.; Plattner, F.; Radl, R.; Tschauner, C.; Hofmann, S. Custom-fit minimally invasive total knee arthroplasty: Effect on blood loss and early clinical outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2234–2240. [Google Scholar] [CrossRef]
- Rathod, P.A.; Deshmukh, A.J.; Cushner, F.D. Reducing Blood Loss in Bilateral Total Knee Arthroplasty with Patient-Specific Instrumentation. Orthop. Clin. N. Am. 2015, 46, 343–350. [Google Scholar] [CrossRef]
- Renson, L.; Poilvache, P.; den Wyngaert, H.V. Improved alignment and operating room efficiency with patient-specific instrumentation for TKA. Knee 2014, 21, 1216–1220. [Google Scholar] [CrossRef] [PubMed]
- Roh, Y.W.; Kim, T.W.; Lee, S.; Seong, S.C.; Lee, M.C. Is TKA Using Patient-specific Instruments Comparable to Conventional TKA? A Randomized Controlled Study of One System. Clin. Orthop. Relat. Res. 2013, 471, 3988–3995. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, I.; Ishii, S.; Usui, M.; Ogino, T.; Kaneda, K. Cubitus varus deformity following supracondylar fracture of the humerus. A method for measuring rotational deformity. Clin. Orthop. Relat. Res. 1985, 201, 179–185. [Google Scholar]
- Jiang, H.; Li, M.; Wu, Y. Application of computer simulation in the treatment of traumatic cubitus varus deformity in children. Medicine 2019, 98, e13882. [Google Scholar] [CrossRef] [PubMed]
- Murase, T.; Takeyasu, Y.; Oka, K.; Kataoka, T.; Tanaka, H.; Yoshikawa, H. Three-Dimensional Corrective Osteotomy for Cubitus Varus Deformity with Use of Custom-Made Surgical Guides. JBJS Essent. Surg. Tech. 2014, 4, e6. [Google Scholar] [CrossRef] [PubMed]
- Omori, S.; Murase, T.; Oka, K.; Kawanishi, Y.; Oura, K.; Tanaka, H.; Yoshikawa, H. Postoperative accuracy analysis of three-dimensional corrective osteotomy for cubitus varus deformity with a custom-made surgical guide based on computer simulation. J. Shoulder Elb. Surg. 2015, 24, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Tricot, M.; Duy, K.T.; Docquier, P.-L. 3D-corrective osteotomy using surgical guides for posttraumatic distal humeral deformity. Acta Orthop. Belg. 2012, 78, 538–542. [Google Scholar] [PubMed]
- Zhang, Y.Z.; Lu, S.; Chen, B.; Zhao, J.M.; Liu, R.; Pei, G.X. Application of computer-aided design osteotomy template for treatment of cubitus varus deformity in teenagers: A pilot study. J. Shoulder Elb. Surg. 2011, 20, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhong, M.; Lou, Y.; Xu, P.; Jiang, B.; Mao, F.; Chen, D.; Zheng, P. Clinical application of individualized 3D-printed navigation template to children with cubitus varus deformity. J. Orthop. Surg. Res. 2020, 15, 111. [Google Scholar] [CrossRef] [PubMed]
- Maróti, P.; Kocsis, B.; Ferencz, A.; Nyitrai, M.; Lőrinczy, D. Differential thermal analysis of the antibacterial effect of PLA-based materials planned for 3D printing. J. Therm. Anal. Calorim. 2020, 139, 367–374. [Google Scholar] [CrossRef]
- Aguado-Maestro, I.; De Frutos-Serna, M.; González-Nava, A.; Merino-De Santos, A.B.; García-Alonso, M. Are the common sterilization methods completely effective for our in-house 3D printed biomodels and surgical guides? Injury 2020. [Google Scholar] [CrossRef] [PubMed]
- Barbier, N.; de Wouters, S.; Traore, S.; Duy, K.T.; Docquier, P.-L. Patient specific instrumentation for corrective osteotomy in case of posttraumatic cubitus varus in children. Acta Orthop. Belg. 2019, 85, 297–304. [Google Scholar] [PubMed]
- Feng, L.; Wang, Y.; Wei, Q. PA12 Powder Recycled from SLS for FDM. Polymers 2019, 11, 727. [Google Scholar] [CrossRef]
- Lindberg, A.; Alfthan, J.; Pettersson, H.; Flodberg, G.; Yang, L. Mechanical performance of polymer powder bed fused objects: FEM simulation and verification. Addit. Manuf. 2018, 24, 577–586. [Google Scholar] [CrossRef]
- Zarringhalam, H.; Hopkinson, N.; Kamperman, N.F.; de Vlieger, J.J. Effects of processing on microstructure and properties of SLS Nylon 12. Mater. Sci. Eng. A 2006, 172–180. [Google Scholar] [CrossRef]
- Osti, F.; Santi, G.M.; Neri, M.; Liverani, A.; Frizziero, L.; Stilli, S.; Maredi, E.; Zarantonello, P.; Gallone, G.; Stallone, S.; et al. CT conversion workflow for intraoperative usage of bony models: From DICOM data to 3D printed models. Appl. Sci. 2019, 9, 708. [Google Scholar] [CrossRef]
- Frizziero, L.; Liverani, A.; Donnici, G.; Osti, F.; Neri, M.; Maredi, E.; Trisolino, G.; Stilli, S. New Methodology for Diagnosis of Orthopedic Diseases through Additive Manufacturing Models. Symmetry 2019, 11, 542. [Google Scholar] [CrossRef]
- Caligiana, P.; Liverani, A.; Ceruti, A.; Santi, G.M.; Donnici, G.; Osti, F. An Interactive Real-Time Cutting Technique for 3D Models in Mixed Reality. Technologies 2020, 8, 23. [Google Scholar] [CrossRef]
- Frizziero, L.; Santi, G.M.; Liverani, A.; Giuseppetti, V.; Trisolino, G.; Maredi, E.; Stilli, S. Paediatric Orthopaedic Surgery with 3D Printing: Improvements and Cost Reduction. Symmetry 2019, 11, 1317. [Google Scholar] [CrossRef]
- Napolitano, F.; Frizziero, L.; Santi, G.M.; Donnici, G.; Liverani, A.; Papaleo, P.; Giuseppetti, V. Description of the CAD-AM Process for 3D Bone Printing: The Case Study of a Flat Foot. In Proceedings of the 5th NA International Conference on Industrial Engineering and Operations Management, Detroit, MI, USA, 10–14 August 2020; pp. 2248–2257. [Google Scholar]
- Frizziero, L.; Donnici, G.; Liverani, A.; Santi, G.; Neri, M.; Papaleo, P.; Napolitano, F. Description of the CAD-AM Process for 3D Bone Printing: The Case Study of a Femur. In Proceedings of the 5th NA International Conference on Industrial Engineering and Operations Management, Detroit, MI, USA, 10–14 August 2020; pp. 2258–2266. [Google Scholar]
- Akhoundi, B.; Nabipour, M.; Hajami, F.; Shakoori, D. An Experimental Study of Nozzle Temperature and Heat Treatment (Annealing) Effects on Mechanical Properties of High-Temperature Polylactic Acid in Fused Deposition Modeling. Polym. Eng. Sci. 2020, 60, 979–987. [Google Scholar] [CrossRef]
- Chen, J.V.; Tanaka, K.S.; Dang, A.B.C.; Dang, A. Identifying a commercially-available 3D printing process that minimizes model distortion after annealing and autoclaving and the effect of steam sterilization on mechanical strength. 3D Print. Med. 2020, 6. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Operative Minutes Saved in Experimental Groups Compared to Control Group | Patients in Experimental Group | Patients in Control Group | |
|---|---|---|---|---|
| 1 | Zhang et al. [5] | 78 | 11 | 11 |
| 2 | Hsu et al. [6] | −12 | 42 | 29 |
| 3 | Chareancholvanich et al. [7] | −5.1 | 40 | 40 |
| 4 | Abane et al. [8] | −6.3 | 59 | 67 |
| 5 | Barrack et al. [9] | −11 | 100 | 100 |
| 6 | Barrett et al. [10] | −5.2 | 66 | 86 |
| 7 | Boonen et al. [11] | −10 | 39 | 40 |
| 8 | Boonen et al. [12] | −5 | 90 | 90 |
| 9 | Ferrara et al. [13] | −22.3 | 15 | 15 |
| 10 | Gan et al. [14] | −15 | 35 | 35 |
| 11 | Hamilton et al. [15] | 4.3 | 26 | 26 |
| 12 | Kassab and Pietrzak, [16] | −16.7 | 270 | 595 |
| 13 | Kerens et al. [17] | 5 | 30 | 30 |
| 14 | Nankivell et al. [18] | −4 | 40 | 45 |
| 15 | Noble et al. [19] | −6.7 | 19 | 15 |
| 16 | Nunley et al. [20] | −12.1 | 57 | 57 |
| 17 | Pfitzner et al. [21] | −15.5 | 60 | 30 |
| 18 | Pietsch et al. [22] | −12 | 40 | 40 |
| 19 | Rathod et al. [23] | −18 | 15 | 14 |
| 20 | Renson et al. [24] | −8.9 | 71 | 60 |
| 21 | Roh et al. [25] | 12.8 | 50 | 50 |
| Mean (median) | −12 (−10) | 56 (40) | 70 (40) | |
| PARAMETERS | VALUES |
|---|---|
| Nozzle Temperature [°C] | 210 |
| Heated Bed Temperature [°C] | 60 |
| Print Speed [mm/s] | 25–45 |
| Extrusion Width [mm] | 0.5 mm larger than the size of the nozzle |
| Volume Flow [mm³/s] | 2–3 |
| Printing Technique | Materials | Materials Cost (€/kg) | Printing Cost (€) |
|---|---|---|---|
| FDM | ABS | 32.50 | from 150 to 800 |
| PLA | 37.30 | ||
| HTPLA | 68.00 | ||
| PETG | 45.30 | ||
| SLS | Nylon (PA12) | 85.70 | from 7000 to 145,000 |
| SLA | Medical-grade resin | 429.99 | from 250 to 1000 |
| SLA/PoliJet (Viper SLA Si2 3D System + Objet Eden 250) | Resin | 58.99 | 13,500 + 41,000 |
| Ref. | Production | Informatic Procedure | Material | Sterilization | 3D Printing Technology |
|---|---|---|---|---|---|
| THIS PROCEDURE | In-house | Invesalius, MeshLab/Meshmixer, PTC Creo | HTPLA | Autoclave | FDM |
| Zhang et al. 2011 [31] | In-house | Materialise Mimics, Imageware | Acrylate Resin | Sterilization is not mentioned | SLA |
| Murase et al. 2013 [32] | Nakashima Medical | Bone Simulator (ORTHREE), Magics | Resin | Sterilization is not mentioned | SLA/PoliJet |
| Barbier et al. 2019 [36] | In-house | Materialise Mimics | Nylon | The sterilization method used is not specified | SLS |
| Hu et al. 2020 [33] | In-house | Materialise Mimics 17.0 | PLA | Sterilization is not mentioned | FDM |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frizziero, L.; Santi, G.M.; Leon-Cardenas, C.; Donnici, G.; Liverani, A.; Napolitano, F.; Papaleo, P.; Pagliari, C.; Antonioli, D.; Stallone, S.; et al. An Innovative and Cost-Advantage CAD Solution for Cubitus Varus Surgical Planning in Children. Appl. Sci. 2021, 11, 4057. https://doi.org/10.3390/app11094057
Frizziero L, Santi GM, Leon-Cardenas C, Donnici G, Liverani A, Napolitano F, Papaleo P, Pagliari C, Antonioli D, Stallone S, et al. An Innovative and Cost-Advantage CAD Solution for Cubitus Varus Surgical Planning in Children. Applied Sciences. 2021; 11(9):4057. https://doi.org/10.3390/app11094057
Chicago/Turabian StyleFrizziero, Leonardo, Gian Maria Santi, Christian Leon-Cardenas, Giampiero Donnici, Alfredo Liverani, Francesca Napolitano, Paola Papaleo, Curzio Pagliari, Diego Antonioli, Stefano Stallone, and et al. 2021. "An Innovative and Cost-Advantage CAD Solution for Cubitus Varus Surgical Planning in Children" Applied Sciences 11, no. 9: 4057. https://doi.org/10.3390/app11094057
APA StyleFrizziero, L., Santi, G. M., Leon-Cardenas, C., Donnici, G., Liverani, A., Napolitano, F., Papaleo, P., Pagliari, C., Antonioli, D., Stallone, S., Di Gennaro, G. L., Trisolino, G., & Zarantonello, P. (2021). An Innovative and Cost-Advantage CAD Solution for Cubitus Varus Surgical Planning in Children. Applied Sciences, 11(9), 4057. https://doi.org/10.3390/app11094057