
Bone Marrow Aspirate Concentrate Is More Effective Than Hyaluronic Acid and Autologous Conditioned Serum in the Treatment of Knee Osteoarthritis: A Retrospective Study of 505 Consecutive Patients


Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
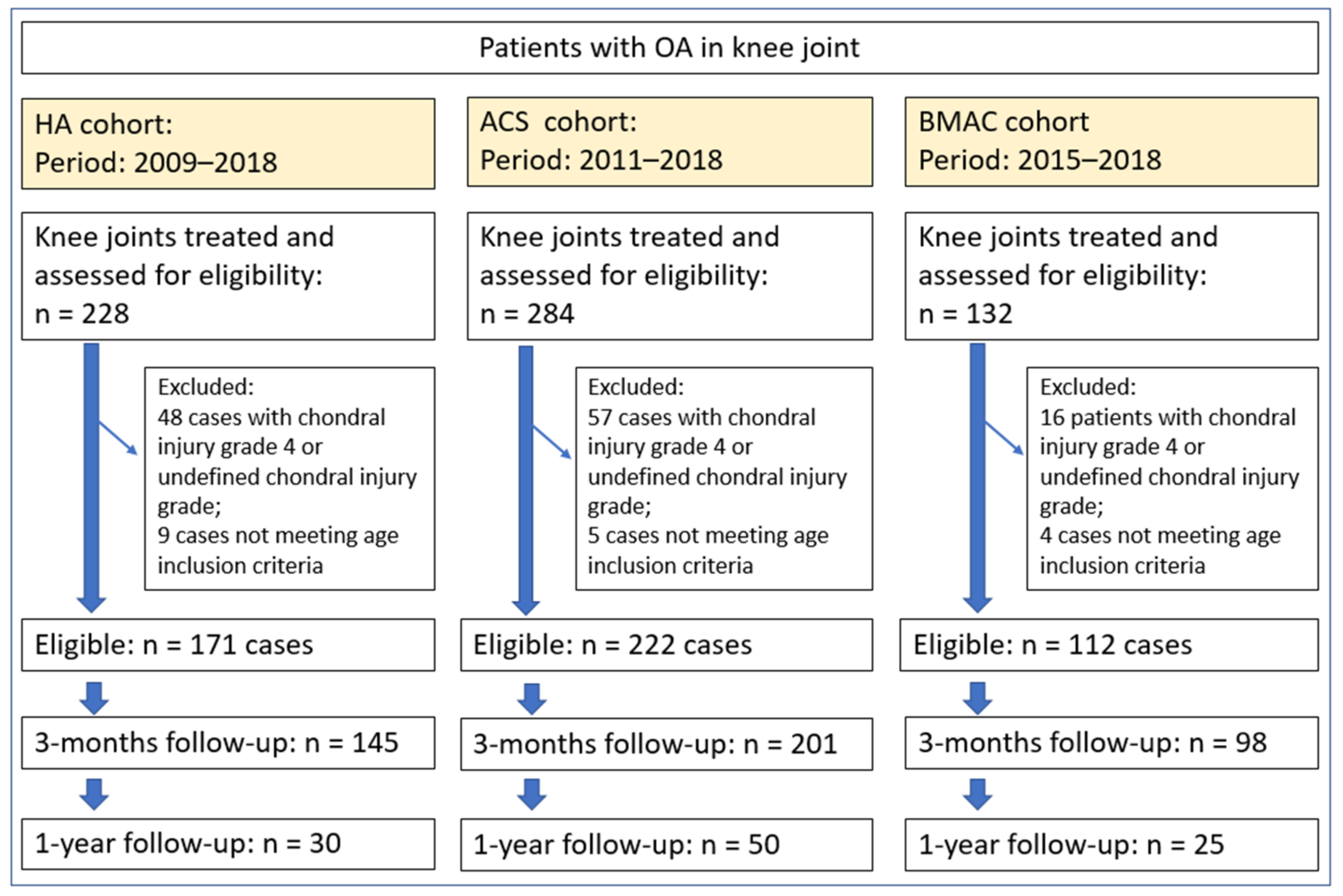
2.1. Inclusion and Exclusion Criteria
2.2. Treatment Procedures
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Treatment Groups
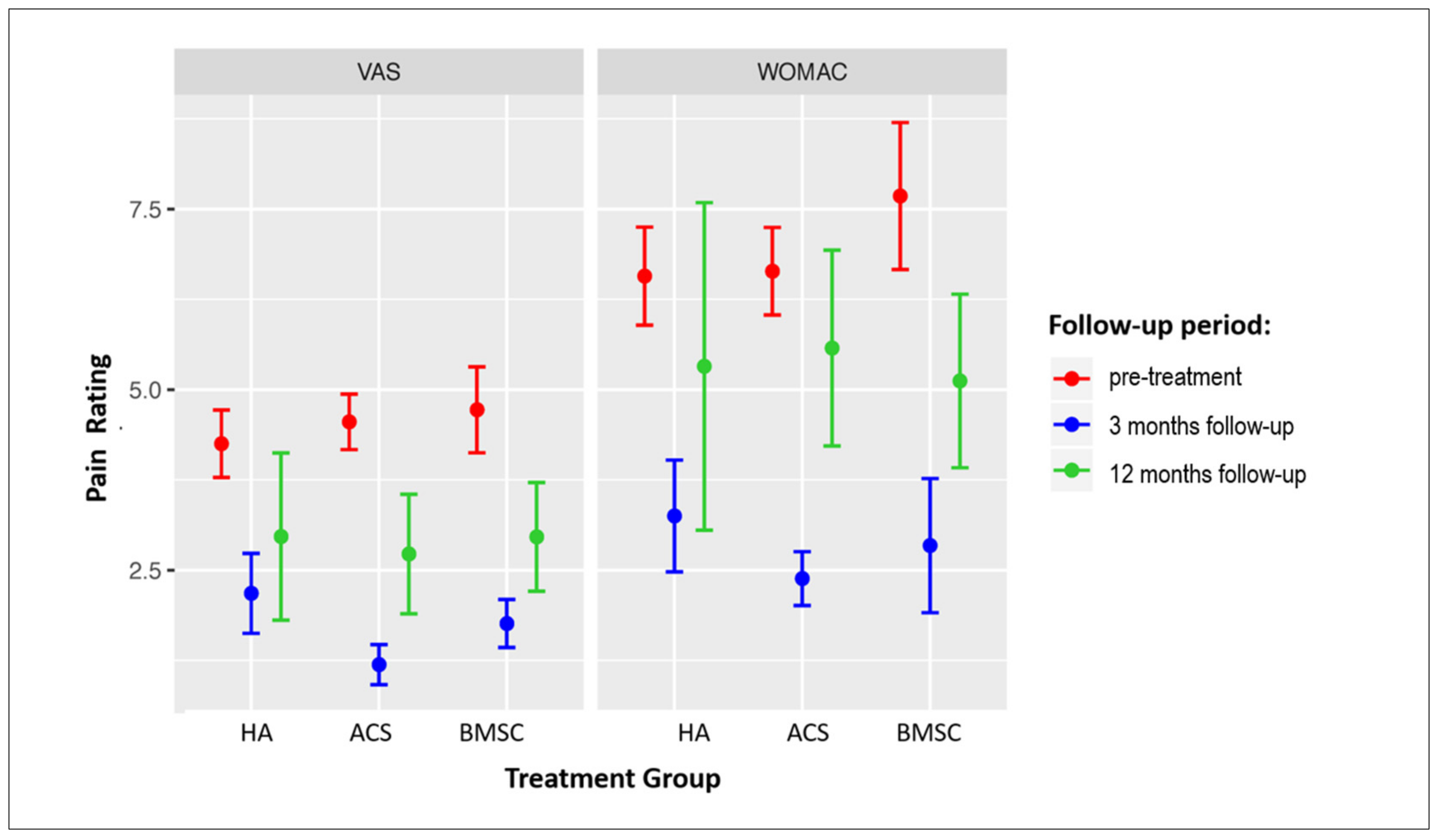
3.2. Follow-Up Outcomes
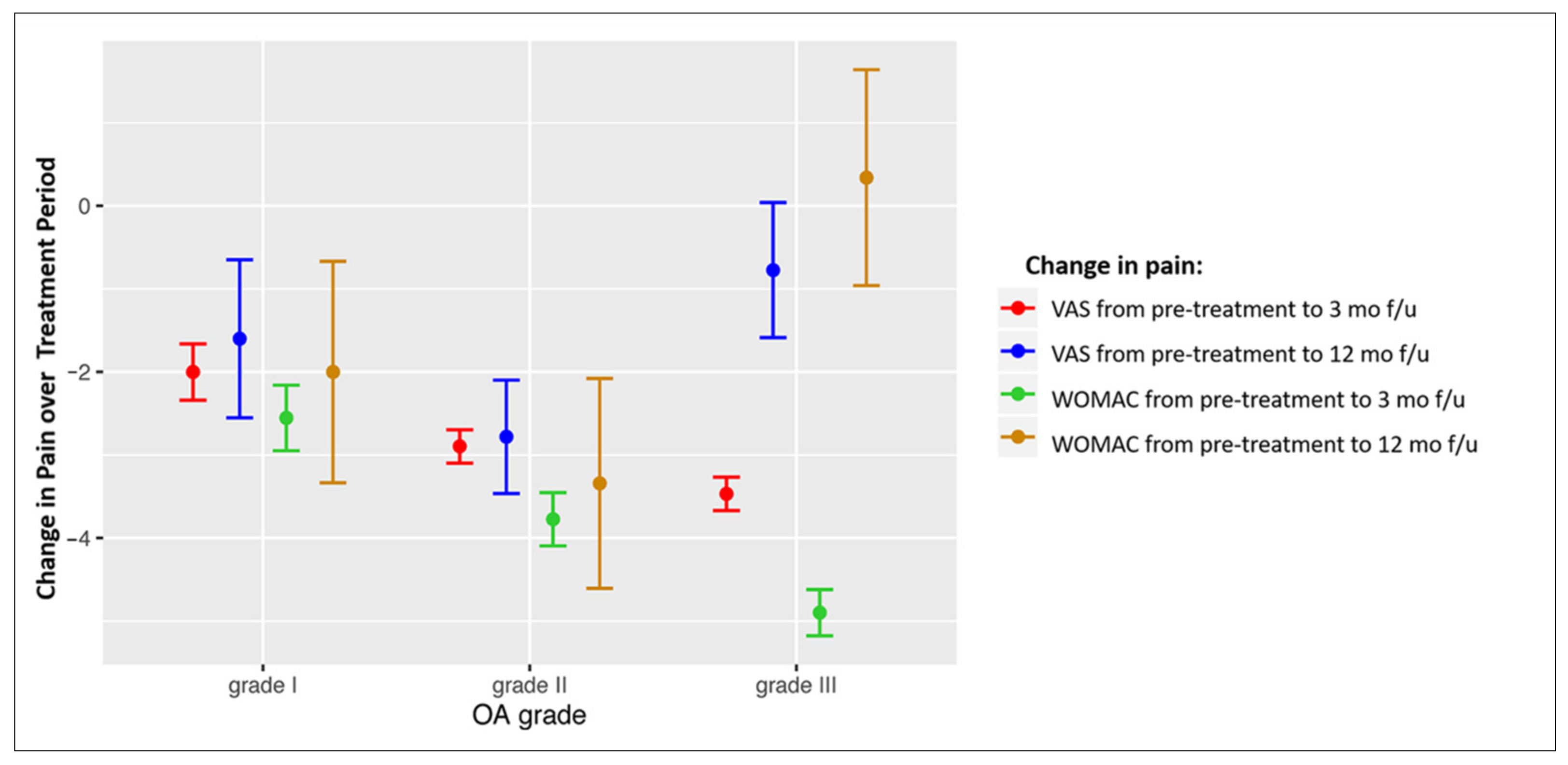
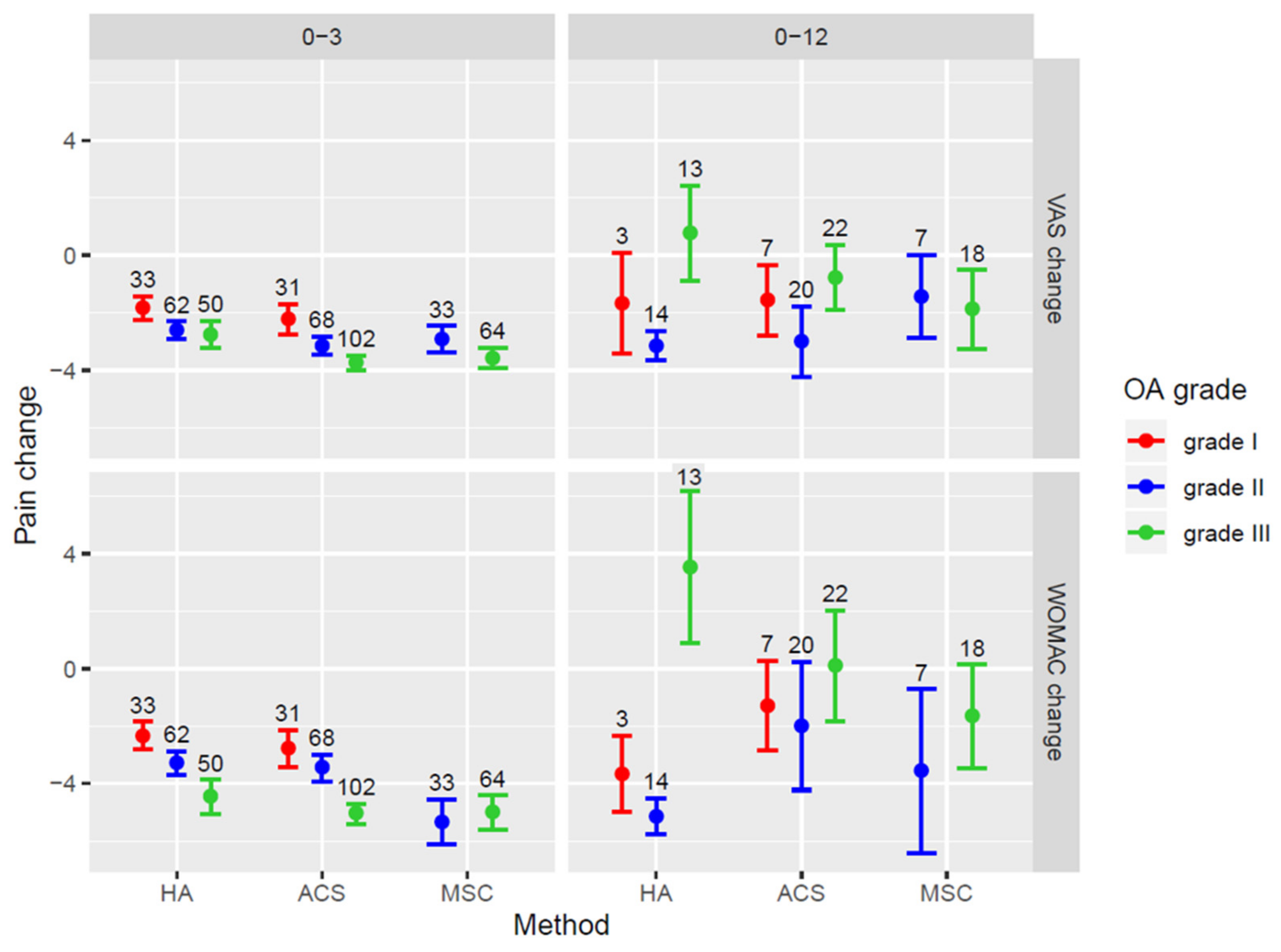
3.3. Association of Pain Score Changes with OA Grade
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAOS | American Academy of Orthopaedic Surgeons |
| ACS | autologous conditioned serum |
| BMAC | bone marrow aspirate concentrate |
| HA | hyaluronic acid |
| MSCs | mesenchymal stem cells |
| OA | osteoarthritis |
| PRP | platelet rich plasma |
| SEM | standard error of the mean |
| VAS | Visual Analogue Scale |
| WOMAC | Western Ontario and McMaster Universities Osteoarthritis Index |
References
- Hesper, T.; Bittersohl, B.; Schleich, C.; Hosalkar, H.; Krauspe, R.; Krekel, P.; Zilkens, C. Automatic cartilage segmentation for delayed gadolinium-enhanced magnetic resonance imaging of hip joint cartilage: A feasibility study. Cartilage 2020, 11, 32–37. [Google Scholar] [CrossRef]
- Conrozier, T.; Monfort, J.; Chevalier, X.; Raman, R.; Richette, P.; Diraçoglù, D.; Bard, H.; Baron, D.; Jerosch, J.; Migliore, A.; et al. EUROVISCO recommendations for optimizing the clinical results of viscosupplementation in osteoarthritis. Cartilage 2020, 11, 47–59. [Google Scholar] [CrossRef]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [CrossRef]
- Henrotin, Y.; Chevalier, X.; Raman, R.; Richette, P.; Montfort, J.; Jerosch, J.; Baron, D.; Bard, H.; Carrillon, Y.; Migliore, A.; et al. EUROVISCO guidelines for the design and conduct of clinical trials assessing the disease-modifying effect of knee viscosupplementation. Cartilage 2020, 11, 60–70. [Google Scholar] [CrossRef]
- Cotter, E.J.; Frank, R.M.; Mandelbaum, B. Management of osteoarthritis—Biological approaches: Current concepts. J. ISAKOS 2020, 5, 27–31. [Google Scholar] [CrossRef]
- Sherman, B.J.; Chahla, J.; Glowney, J.; Frank, R.M. The role of orthobiologics in the management of osteoarthritis and focal cartilage defects. Orthopedics 2019, 42, 66–73. [Google Scholar] [CrossRef]
- Pereira, H.; Sousa, D.A.; Cunha, A.; Andrade, R.; Espregueira-Mendes, J.; Oliveira, J.M.; Reis, R.L. Hyaluronic acid. Adv. Exp. Med. Biol. 2018, 1059, 137–153. [Google Scholar] [CrossRef]
- Jevsevar, D.S.; Brown, G.A.; Jones, D.L.; Matzkin, E.G.; Manner, P.A.; Mooar, P.; Gross, L. The American Academy of Orthopaedic Surgeons evidence-based guideline on: Treatment of osteoarthritis of the knee. JBJS 2013, 95, 1885–1886. [Google Scholar] [CrossRef] [PubMed]
- Kingery, M.T.; Manjunath, A.K.; Anil, U.; Strauss, E.J. Bone marrow mesenchymal stem cell therapy and related bone marrow-derived orthobiologic therapeutics. Curr. Rev. Musculoskelet. Med. 2019, 12, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Centeno, C.J.; Pastoriza, S.M. Past, current and future interventional orthobiologics techniques and how they relate to regenerative rehabilitation: A clinical commentary. Int. J. Sports Phys. Ther. 2020, 15, 301–325. [Google Scholar] [CrossRef]
- Osterman, C.; McCarthy, M.B.R.; Cote, M.P.; Beitzel, K.; Bradley, J.; Polkowski, G.; Mazzocca, A.D. Platelet-rich plasma increases anti-inflammatory markers in a human coculture model for osteoarthritis. Am. J. Sports Med. 2015, 43, 1474–1484. [Google Scholar] [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-rich plasma: New performance understandings and therapeutic considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.-J.; Rothrauff, B.B.; Alexander, P.G.; Tuan, R.S. Effect of platelet-rich plasma on chondrogenic differentiation of adipose- and bone marrow-derived mesenchymal stem cells. Tissue Eng. Part A 2018, 24, 1432–1443. [Google Scholar] [CrossRef] [PubMed]
- Fice, M.P.; Miller, J.C.; Christian, R.; Hannon, C.P.; Smyth, N.; Murawski, C.D.; Cole, B.J.; Kennedy, J.G. The role of platelet-rich plasma in cartilage pathology: An updated systematic review of the basic science evidence. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 961–976.e3. [Google Scholar] [CrossRef]
- Cooper, C.; Rannou, F.; Richette, P.; Bruyère, O.; Al-Daghri, N.; Altman, R.D.; Brandi, M.L.; Collaud Basset, S.; Herrero-Beaumont, G.; Migliore, A.; et al. Use of intraarticular hyaluronic acid in the management of knee osteoarthritis in clinical practice. Arthritis Care Res. 2017, 69, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Hermans, J.; Bierma-Zeinstra, S.M.A.; Bos, P.K.; Niesten, D.D.; Verhaar, J.A.N.; Reijman, M. The effectiveness of high molecular weight hyaluronic acid for knee osteoarthritis in patients in the working age: A randomised controlled trial. BMC Musculoskelet. Disord. 2019, 20, 196. [Google Scholar] [CrossRef]
- He, W.-W.; Kuang, M.-J.; Zhao, J.; Sun, L.; Lu, B.; Wang, Y.; Jian-Xiong, M.; Ma, X.-L. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. Int. J. Surg. 2017, 39, 95–103. [Google Scholar] [CrossRef]
- Dhillon, M.S.; Patel, S.; John, R. PRP in OA knee—Update, current confusions and future options. Sicot. J. 2017, 3, 27. [Google Scholar] [CrossRef]
- Richards, M.M.; Maxwell, J.S.; Weng, L.; Mathew, G.; Golzarian, J. Inflammatories to products of regenerative medicine. Phys. Sportsmed. 2017, 44, 101–108. [Google Scholar] [CrossRef]
- Baltzer, A.W.A.; Moser, C.; Jansen, S.A.; Krauspe, R. Autologous conditioned serum (orthokine) is an effective treatment for knee osteoarthritis. Osteoarthr. Cartil. 2009, 17, 152–160. [Google Scholar] [CrossRef]
- Pishgahi, A.; Abolhasan, R.; Shakouri, S.K.; Zangbar, M.S.S.; Dareshiri, S.; Kiyakalayeh, S.R.; Khoeilar, A.; Zamani, M.; Khiavi, F.M.; Kheiraddin, B.P.; et al. Effect of dextrose prolotherapy, platelet rich plasma and autologous conditioned serum on knee osteoarthritis: A randomized clinical trial. Iran. J. Allergy Asthma Immunol. 2020, 19, 243–252. [Google Scholar] [CrossRef]
- Jeyaraman, M.; Muthu, S.; Ganie, P.A. Does the source of mesenchymal stem cell have an effect in the management of osteoarthritis of the knee? Meta-analysis of randomized controlled trials. Cartilage 2020. [Google Scholar] [CrossRef]
- Wang, A.T.; Feng, Y.; Jia, H.H.; Zhao, M.; Yu, H. Application of mesenchymal stem cell therapy for the treatment of osteoarthritis of the knee: A concise review. World J. Stem Cells 2019, 11, 222–235. [Google Scholar] [CrossRef]
- Song, Y.; Du, H.; Dai, C.; Zhang, L.; Li, S.; Hunter, D.J.; Lu, L.; Bao, C. Human adipose-derived mesenchymal stem cells for osteoarthritis: A pilot study with long-term follow-up and repeated injections. Regen. Med. 2018, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Bansal, H.; Comella, K.; Leon, J.; Verma, P.; Agrawal, D.; Koka, P.; Ichim, T. Intra-articular injection in the knee of adipose derived stromal cells (stromal vascular fraction) and platelet rich plasma for osteoarthritis. J. Transl. Med. 2017, 15, 141. [Google Scholar] [CrossRef] [PubMed]
- Centeno, C.; Pitts, J.; Al-Sayegh, H.; Freeman, M. Efficacy of autologous bone marrow concentrate for knee osteoarthritis with and without adipose graft. Biomed Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-D.; Lee, G.W.; Jung, G.H.; Kim, C.K.; Kim, T.; Park, J.H.; Cha, S.S.; You, Y.-B. Clinical outcome of autologous bone marrow aspirates concentrate (BMAC) injection in degenerative arthritis of the knee. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 1505–1511. [Google Scholar] [CrossRef]
- Hede, K.; Christensen, B.B.; Jensen, J.; Foldager, C.B.; Lind, M. Combined bone marrow aspirate and platelet-rich plasma for cartilage repair: Two-year clinical results. Cartilage 2019. [Google Scholar] [CrossRef]
- Zhao, X.; Zhao, Y.; Sun, X.; Xing, Y.; Wang, X.; Yang, Q. Immunomodulation of MSCs and MSC-derived extracellular vesicles in osteoarthritis. Front. Bioeng. Biotechnol. 2020, 8, 575057. [Google Scholar] [CrossRef]
- Durant, T.J.S.; Dwyer, C.R.; McCarthy, M.B.R.; Cote, M.P.; Bradley, J.P.; Mazzocca, A.D. Protective nature of platelet-rich plasma against chondrocyte death when combined with corticosteroids or local anesthetics. Am. J. Sports Med. 2017, 45, 218–225. [Google Scholar] [CrossRef]
- Krakowski, P.; Karpiński, R.; Jonak, J.; Maciejewski, R.; Jurkiewicz, A. Short-term Effects of arthroscopic microfracturation of knee chondral defects in osteoarthritis. Appl. Sci. 2020, 10, 8312. [Google Scholar] [CrossRef]
- Lamo-Espinosa, J.M.; Mora, G.; Blanco, J.F.; Granero-Moltó, F.; Núñez-Córdoba, J.M.; López-Elío, S.; Andreu, E.; Sánchez-Guijo, F.; Aquerreta, J.D.; Bondía, J.M.; et al. Intra-articular injection of two different doses of autologous bone marrow mesenchymal stem cells versus hyaluronic acid in the treatment of knee osteoarthritis: Long-term follow up of a multicenter randomized controlled clinical trial (phase I/II). J. Transl. Med. 2018, 16, 1–5. [Google Scholar] [CrossRef]
- Cole, B.; Karas, V.; Kristen, H. Hyaluronic acid versus platelet-rich plasma: A prospective, double-blind randomized controlled trial comparing clinical outcomes and effects on intra-articular biology for the treatment of knee osteoarthritis. Am. J. Sport. Med. 2017, 45, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Lamo-Espinosa, J.M.; Blanco, J.F.; Sánchez, M.; Moreno, V.; Granero-Moltó, F.; Sánchez-Guijo, F.; Crespo-Cullel, Í.; Mora, G.; San Vicente, D.D.; Pompei-Fernández, O.; et al. Phase II multicenter randomized controlled clinical trial on the efficacy of intra-articular injection of autologous bone marrow mesenchymal stem cells with platelet rich plasma for the treatment of knee osteoarthritis. J. Transl. Med. 2020, 18, 1–9. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheumat. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Rheumatism in miners. II. X-ray study. Br. J. Ind. Med. 1952, 9, 197–207. [Google Scholar] [CrossRef][Green Version]
- Bellamy, N.; Campbell, J.; Robinson, V.; Gee, T.; Bourne, R.; Wells, G. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst. Rev. 2006, 2, CD005321. [Google Scholar] [CrossRef]
- Yang, K.G.A.; Raijmakers, N.J.H.; van Arkel, E.R.A.; Caron, J.J.; Rijk, P.C.; Willems, W.J.; Zijl, J.A.C.; Verbout, A.J.; Dhert, W.J.A.; Saris, D.B.F. Autologous interleukin-1 receptor antagonist improves function and symptoms in osteoarthritis when compared to placebo in a prospective randomized controlled trial. Osteoarthr. Cartil. 2008, 16, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Lamo-Espinosa, J.M.; Mora, G.; Blanco, J.F.; Granero-Moltó, F.; Nuñez-Córdoba, J.M.; Sánchez-Echenique, C.; Bondía, J.M.; Aquerreta, J.D.; Andreu, E.J.; Ornilla, E.; et al. Intra-articular injection of two different doses of autologous bone marrow mesenchymal stem cells versus hyaluronic acid in the treatment of knee osteoarthritis: Multicenter randomized controlled clinical trial (phase I/II). J. Transl. Med. 2016, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gulotta, L.V.; Kovacevic, D.; Ehteshami, J.R.; Dagher, E.; Packer, J.D.; Rodeo, S.A. Application of bone marrow-derived mesenchymal stem cells in a rotator cuff repair model. Am. J. Sports Med. 2009, 37, 2126–2133. [Google Scholar] [CrossRef]
- Kim, G.B.; Kim, J.D.; Choi, Y.; Choi, C.H.; Lee, G.W. Intra-articular bone marrow aspirate concentrate injection in patients with knee osteoarthritis. Appl. Sci. 2020, 10, 5945. [Google Scholar] [CrossRef]
- Goyal, D.; Keyhani, S.; Lee, E.H.; Hui, J.H.P. Evidence-based status of microfracture technique: A systematic review of level I and II studies. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1579–1588. [Google Scholar] [CrossRef] [PubMed]
- Behery, O.A.; Harris, J.D.; Karnes, J.M.; Siston, R.A.; Flanigan, D.C. Factors influencing the outcome of autologous chondrocyte implantation: A systematic review. J. Knee Surg. 2013, 26, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, P.; El-Jawhari, J.J.; Giannoudis, P.V.; Burska, A.N.; Ponchel, F.; Jones, E.A. Age-related changes in bone marrow mesenchymal stromal cells: A potential impact on osteoporosis and osteoarthritis development. Cell Transplant. 2017, 26, 1520–1529. [Google Scholar] [CrossRef] [PubMed]
- Stolzing, A.; Jones, E.; McGonagle, D.; Scutt, A. Age-related changes in human bone marrow-derived mesenchymal stem cells: Consequences for cell therapies. Mech. Ageing Dev. 2008, 129, 163–173. [Google Scholar] [CrossRef]
- Yang, Y.H.K. Aging of mesenchymal stem cells: Implication in regenerative medicine. Regen. Ther. 2018, 9, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Momaya, A.M.; McGee, A.S.; Dombrowsky, A.R.; Wild, A.J.; Faroqui, N.M.; Waldrop, R.P.; He, J.K.; Brabston, E.W.; Ponce, B.A. The cost variability of orthobiologics. Sports Health 2020, 12, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Wartolowska, K.A.; Gerry, S.; Feakins, B.G.; Collins, G.S.; Cook, J.; Judge, A.; Carr, A.J. A meta-analysis of temporal changes of response in the placebo arm of surgical randomized controlled trials: An update. Trials 2017, 18, 1–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Sex | Laterality | |||
|---|---|---|---|---|---|
| Treatment Group | Mean ± SD | Male N (%) | Female N (%) | Left N (%) | Right N (%) |
| HA | 51 ± 15 | 88 (52) | 83 (48) | 76 (44) | 95 (56) |
| ACS | 51 ± 13 | 121 (57) | 101 (43) | 109 (49) | 113 (51) |
| BMAC | 52 ± 10 | 66 (59) | 46 (41) | 52 (46) | 60 (54) |
| Total | 52 ± 13 | 287 (54) | 247 (46) | 251 (47) | 283 (53) |
| Baseline differences between groups | p = 0.689 | p = 0.469 | p = 0.654 | ||
| Treatment Group | HA | ACS | BMAC | Significance |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | p Value | |
| OA grade | 2.13 ± 0.74 | 2.35 ± 0.73 | 2.62 ± 0.54 | † p = 0.007, ‡ p = 0.003, ⫩ p < 0.001 |
| VAS | 3.94 ± 1.55 | 4.51 ±1.32 | 5.13 ± 1.28 | † p < 0.001, ‡ p < 0.001, ⫩ p < 0.001 |
| WOMAC | 5.82 ± 1.92 | 6.52 ± 1.96 | 7.92 ± 2.24 | † p = 0.002, ‡ p < 0.001, ⫩ p < 0.001 |
| Correlation between OA Grade & VAS | Correlation between OA Grade & WOMAC | |||
|---|---|---|---|---|
| Treatment Group | Spearman Correlation Coefficient (r) | p Value | Spearman Correlation Coefficient (r) | p Value |
| HA | 0.53 † | <0.001 | 0.67 † | <0.001 |
| ACS | 0.35 † | <0.001 | 0.46 † | <0.001 |
| BMAC | 0.39 † | <0.001 | −0.26 | 0.788 |
| Total | 0.47 † | <0.001 | 0.48 † | <0.001 |
| Pretreatment | 3-Month Follow-Up | 1-Year Follow-Up | Significance of Change in VAS Score after Treatment | |
|---|---|---|---|---|
| Treatment Group | Mean ± SD (N) | Mean ± SD (N) | Mean ± SD (N) | p Value |
| HA | 4.3 ± 1.2 (171) | 2.2 ± 1.4 (145) | 2.9 ± 3.0 (30) | † p < 0.001, ‡ p = 0.017, p = 0.164 |
| ACS | 4.5 ± 1.3 (222) | 1.9 ± 1.0 (201) | 2.7 ± 2.8 (50) | † p < 0.001, ‡ p < 0.001, p < 0.001 |
| BMAC | 4.7 ± 1.5 (112) | 1.8 ± 0.8 (98) | 3.0 ± 0.8 (25) | † p < 0.001, ‡ p = 0.003, p = 0.003 |
| Total | 4.5 ± 1.3 (505) | 1.6 ± 1.15 (444) | 2.9 ± 2.7 (105) | † p < 0.001, ‡ p < 0.001, p < 0.001 |
| Pretreatment | 3-Month Follow-Up | 1-Year Follow-Up | Significance of Change in VAS Score after Treatment | |
|---|---|---|---|---|
| Treatment Group | Mean ± SD (N) | Mean ± SD (N) | Mean ± SD (N) | p Value |
| HA | 6.25 ± 1.78 (171) | 3.24 ± 2.01 (145) | 5.32 ± 6.0 (30) | † p < 0.001, ‡ p = 0.278, ⫩ p = 0.055 |
| ACS | 6.64 ± 2.08 (222) | 2.38 ± 1.27 (201) | 5.57 ± 4.65 (50) | † p < 0.001, ‡ p = 0.143, ⫩ p < 0.001 |
| BMAC | 7.68 ± 2.54 (112) | 2.84 ± 2.32 (98) | 5.12 ± 3.00 (25) | † p < 0.001, ‡ p = 0.005, ⫩ p = 0.003 |
| Total | 6.86 ± 2.16 (505) | 2.74 ± 1.82 (444) | 5.39 ± 4.70 (105) | † p < 0.001, ‡ p = 0.003, ⫩ p < 0.001 |
| Spearman Correlation Coefficient between OA Grade & VAS Change r (p Value) | Spearman Correlation Coefficient between OA Grade & WOMAC Change r (p Value) | |||
|---|---|---|---|---|
| Treatment Group | Pretreatment to 3 mo f/u | Pretreatment to 12 mo f/u | Pretreatment to 3 mo f/u | Pretreatment to 12 mo f/u |
| HA | −0.20 (0.015) † | 0.50 (0.005) † | −0.42 (<0.001) † | 0.68 (<0.001) † |
| ACS | −0.36 (<0.001) † | 0.26 (0.069) | −0.44 (<0.001) † | 0.17 (0.056) |
| BMAC | −0.27 (0.006) † | −0.06 (0.78) | 0.06 (0.592) | 0.16 (0.459) |
| Total | −0.33 (<0.001) † | 0.28 (0.004) † | −0.39 (0.001) † | 0.34 (<0.001) † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, M.; van Eck, C.F.; Kregar Velikonja, N. Bone Marrow Aspirate Concentrate Is More Effective Than Hyaluronic Acid and Autologous Conditioned Serum in the Treatment of Knee Osteoarthritis: A Retrospective Study of 505 Consecutive Patients. Appl. Sci. 2021, 11, 2932. https://doi.org/10.3390/app11072932
Hussein M, van Eck CF, Kregar Velikonja N. Bone Marrow Aspirate Concentrate Is More Effective Than Hyaluronic Acid and Autologous Conditioned Serum in the Treatment of Knee Osteoarthritis: A Retrospective Study of 505 Consecutive Patients. Applied Sciences. 2021; 11(7):2932. https://doi.org/10.3390/app11072932
Chicago/Turabian StyleHussein, Mohsen, Carola F. van Eck, and Nevenka Kregar Velikonja. 2021. "Bone Marrow Aspirate Concentrate Is More Effective Than Hyaluronic Acid and Autologous Conditioned Serum in the Treatment of Knee Osteoarthritis: A Retrospective Study of 505 Consecutive Patients" Applied Sciences 11, no. 7: 2932. https://doi.org/10.3390/app11072932
APA StyleHussein, M., van Eck, C. F., & Kregar Velikonja, N. (2021). Bone Marrow Aspirate Concentrate Is More Effective Than Hyaluronic Acid and Autologous Conditioned Serum in the Treatment of Knee Osteoarthritis: A Retrospective Study of 505 Consecutive Patients. Applied Sciences, 11(7), 2932. https://doi.org/10.3390/app11072932