1. Introduction
A key component of the Fourth Industrial Revolution is the convergence of information and communication technology (ICT). Artificial intelligence and big data comprise the ICT field and is highly expected to be future growth industries. As such, the scope in which data are used is rapidly changing. In the past, research using data was applied in controlled environments in which resources could be collected. The range of artificial intelligence and big data has expanded the data application to the medical imaging domain [
1,
2]. Therefore, artificial intelligence and big data are applied to medical imaging.
As the range in which data could be applied expanded from a single institution to multiple institutions, a uniform data standard was important, and data collectors faced challenges in controlling the entire process by which data were collected and applied [
3]. Medical imaging standards such as Health Level Seven (HL7), Digital Imaging and Communications in Medicine (DICOM), and other standards were implemented with multiple institutions using the same standards [
4]. There is also research being conducted in developing de-identifying methods in order to protect any personal information present in medical imaging collected from environments in which collectors are unable to monitor the entire data collection process. De-identifying methods process any personal information that could potentially be used to specify an individual and retain any data necessary for research. In the case of de-identifying methods, as any personal identifiers are removed, it does not conflict with personal information protection laws. These methods minimize the risk of personal information leaks and maximize accessibility towards data [
5].
Multiple medical institutions have their medical specialists review medical imaging that have different measurement values due to differing medical equipment. As interest in artificial intelligence capable of deciphering medical imaging increases, there is a need for quantifying medical imaging for more precise diagnoses [
6]. Currently, a large amount of artificial research in the medical imaging field is being conducted with magnetic resonance imaging (MRI), which is used to identify and predict diseases and to provide forecasts after prognosis, among others [
7]. In the case of MRI, different environments at medical institutions and the conditions of the patient may affect the magnetic field, resulting in vastly different measurement values even with the same subject. Such results are defined as measurement uncertainty, and other medical imaging measurement equipment have similar occurrences of measurement uncertainty. If measurement uncertainty can be minimized, medical imaging data can have a meaningful value regardless of which institution collected it. To minimize uncertainty, the measurement value of phantoms, which are standard materials, can be used as standardized values in a process that supplements actual measured values.
In order to establish the interoperability of medical imaging and allow for medical imaging to be used at different institutions, this study aimed to propose an interoperability reference model that uses methods which minimize measurement uncertainty, enable de-identifiers, and standardize pre-existing data used for research.
The contributions of this study can be summarized as follows:
It proposes an approach to increase interoperability of medical imaging measurements from different medical institutions by using methods reference phantoms.
It addresses the systematic compatibility issue by applying pre-existing medical data specification standards in HL7 and personal information protection methods in the Health Insurance Portability and Accountability Act (HIPAA) and DICOM.
It follows the characteristics of interoperability as defined by the Healthcare Information and Management Systems Society, Inc. (HIMSS), and applied in medical imaging.
3. Results
3.1. Results of the Medical Imaging Data Exchange System
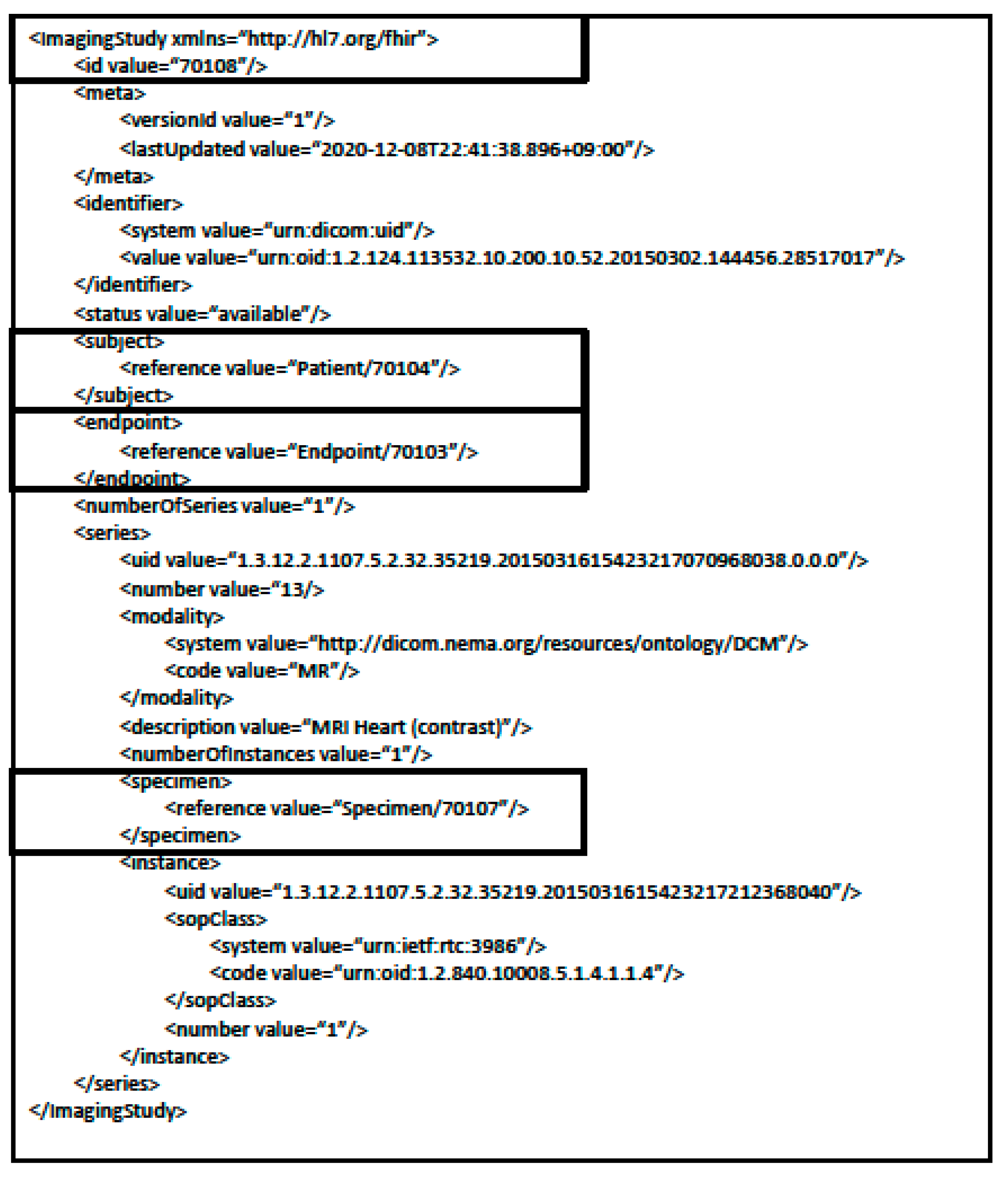
Using the HAPI FHIR server composed based on the HL7 medical data standard, the results of transmitted XML information from ImagingStudy, Patient, and Endpoint were confirmed. Data were successfully saved only in cases in which the actual resource structure classified by the FHIR was used, and its results can be seen in
Figure 6.
In the case of the ImagingStudy resource, the ID references the Patient, Endpoint, and Specimen resource. The referenced IDs are 70104 for the Patient resource, 70103 for the Endpoint resource, and 70107 for the Specimen resource. The Specimen resource was used as the resource to store information regarding the phantom. Below the respective section, UIDs related to the series and instance are included as information on the medical imaging.
In the Patient resource sample XML transmission results in
Figure 7, the id 70104 can be seen as referenced in the ImagingStudy in
Figure 6. Moreover, basic patient-related information is included.
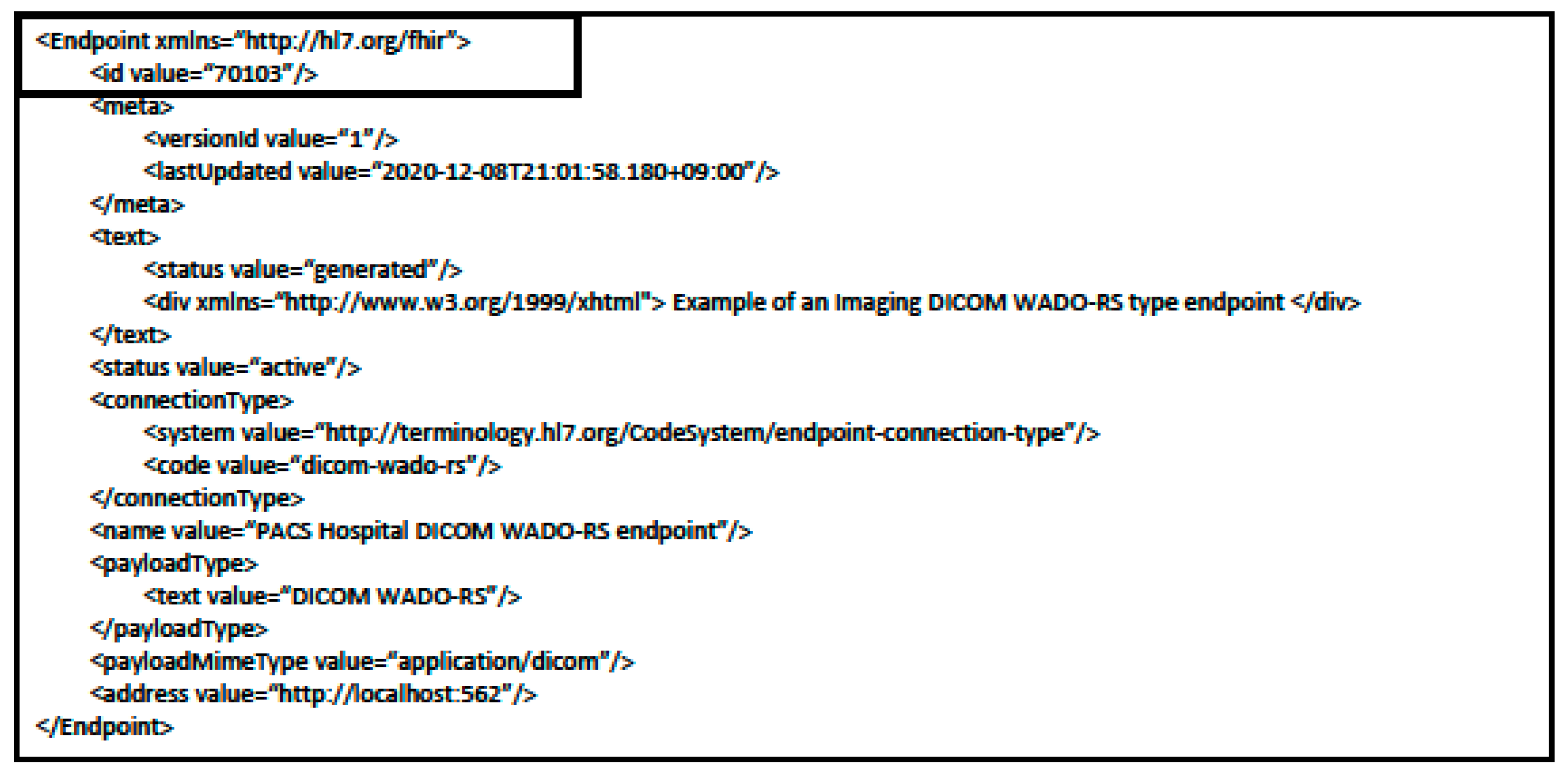
In the Endpoint resource sample XML transmission results in
Figure 8, the data related to Endpoint id 70103 referenced by the ImagingStudy resource in
Figure 6 can be seen. In this resource, the server address where the medical image is saved and information regarding the server’s connection method can be confirmed.
In
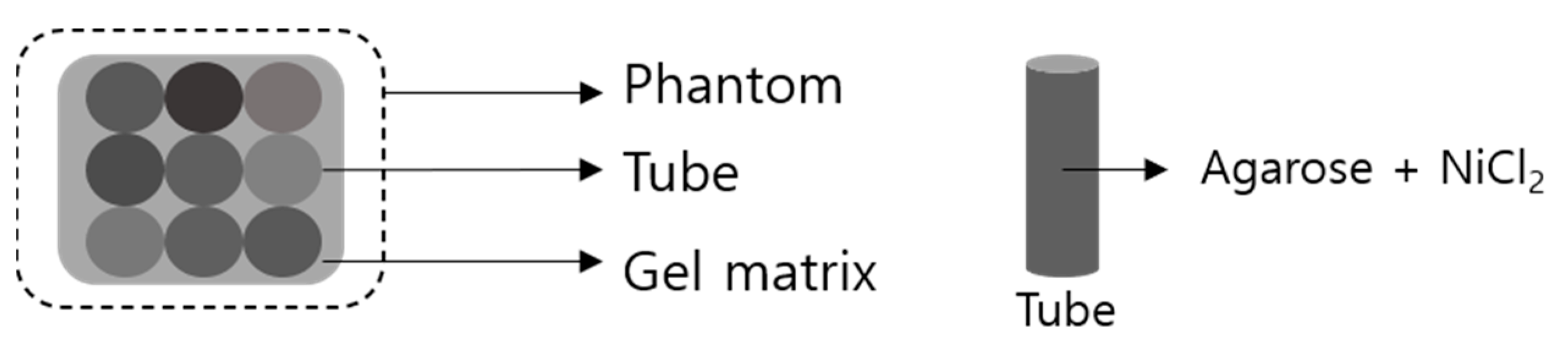
Figure 9, the specimen resource example of the XML transmission results using the Phantom resource includes information on the phantom using the Extension. The Specimen id 70107 referenced by the ImagingStudy resource in
Figure 6 can be deduced as the relevant data.
Each data element complies to the StructureDefinition rules set within the server when designing the Phantom resource. As such, it includes the StructureDefinition URL information that defines each element per extension that relates to the phantom data element.
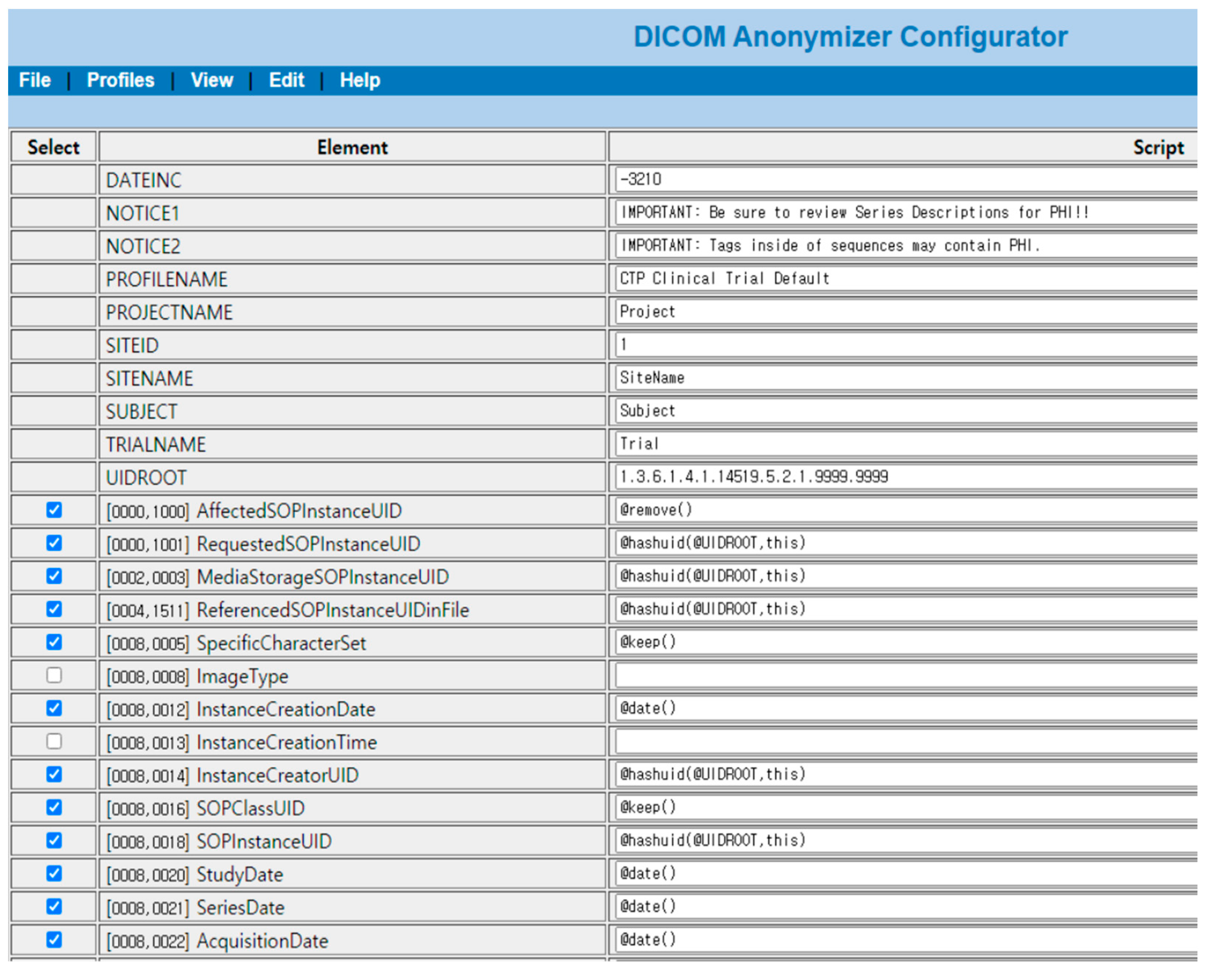
3.2. Results of Personal Information Protection within Medical Imaging
When comparing MRI data using the CTP from the original to the data after the de-identifier process, data that are at risk of personal information leaks are either removed or de-identified.
In
Figure 10, data that needs to be protected for personal information related issues is redacted in the cardiovascular MRI original image. Redacted information are items related to DICOM de-identifier methods and basic profile and include the patient’s name, MR imaging location, name of the specialist, and date of imaging, among others. Information processes by de-identifier processes are shown in
Figure 11.
In
Figure 11, data elements that were shown in the original are nonexistent or changed to different value. The risk of personal information leaks are minimized and only information needed for research is retained.
3.3. Minimization Process of Measurement Uncertainty in Medical Imaging
Figure 12 displays the measurement uncertainty minimization process using standardized phantom data and results from an analysis of measurement uncertainty from medical imaging.
Environmental variables that are classified as uncertainty elements when measuring medical imaging can have an effect on MRI T1 values. In order to calibrate the measurement values, the phantom T1 value can be calibrated based on the phantom’s standardized T1 value affected by environmental variables. Through this process, the measurement value calibration function can be deduced and applied to the patient’s measured MRI T1 value. As a result, the calibrated MRI T1 value is attained with the respective value being the same regardless of where the MRI T1 medical imaging was collected as long as the same standardized phantom T1 value is applied.
For example, in order to detect diseases in specific areas such as cardiovascular symptoms, the patient MR imaging and phantom are captured together. In this case, environmental variables such as sequence design or protocol parameters can be applied as factors of uncertainty and affect the MRI T1 value. We can use a standardized phantom that displays the MRI T1 based value on cardiovascular symptoms. By using the phantom standardized MRI T1 value of cardiovascular symptoms saved on a HL7 FHIR server, we can calibrate the phantom MRI T1 value. By applying the same level of calibration as the phantom MRI T1 value to the patient’s MRI T1 measurement value, we can derive the patient’s calibrated MRI T1 value.
Figure 13 shows that when such a process is applied, different medical imaging from different institutions can be decoded on the same quantifiable levels.
If there is information about the phantom that reflects the characteristics of the other measurement site, it can save the phantom data and use the same method.
Through the quantified phantom, which minimizes measurement uncertainty elements, MRI results can be translated into quantitative MRI (qMRI) and provide high quality data to artificial intelligence medical imaging diagnosis equipment. Moreover, this process would contribute greatly to clinical practices by allowing the earlier detection of diseases, the replacement and supplementation of biopsies, and precise differentiation of diseases due to numerical differences among others [
24].
3.4. Interoperability Reference Model
The final interoperability reference model structure is displayed in
Figure 14. Centered on the medical data exchange system, the medical imaging measurement calibration system, which is an uncertainty minimization system, and personal information de-identifier system are connected with one another with the three systems comprising the interoperability reference model.
The collecting institution applies to the system collecting medical imaging including hospital Picture Archiving Communication System (PACS). Medical imaging received through the medical data exchange system is processed through the de-identifier and measurement uncertainty minimization system, quantified and saved as de-identifier-based medical imaging data. Medical imaging data that minimizes the accessibility limitations of data due to personal information protection regulations and uses a quantified measurement value with standardized data structures will enable use in environments that require large amounts of data, such as in artificial intelligence research.
4. Discussion
The application range of data including medical imaging is quickly expanding, and the need for data collected and used in limited locations is now being demanded in multiple different locations. As such, the need to establish an environment that enables the exchange and use of medical imaging among different institutions is becoming more important and is the main goal of establishing interoperability.
In approaching medical imaging from the concept of interoperability, this study allowed for the exchange of medical data between two systems through an HL7 FHIR server and designated the exchange format and structure through resources and XML according to HL7 FHIR standards. Moreover, for the safe exchange of data, it used a CTP module using de-identifier methods by HIPAA and DICOM in order to minimize personal information related issues that could occur systematically. It also designed a process that minimized measurement uncertainty through the use of phantoms in order to display meaningful values regardless of the institution in which the medical imaging data derived from and simultaneously confirmed the de-identifier and medical data standards currently being used.
In the case of medical imaging, as different measurement standards are used for each hospital and medical equipment, it is normal for a medical professional to perform a qualitative review. Uncertainty minimization methods using standardized phantoms allow medical imaging to be displayed in a qualitative manner and also allows for the use of quantitative medical imaging between different institutions when the same standards are used.
Pre-existing medical data standards such as HL7 FHIR can be used for multiple medical institutions to use the same medical data standards and guarantee compatibility between systems. Moreover, by using non-identifier methods such as HIPAA and DICOM for the protection of personal information in medical data, legal issues can be minimized as well.
When applying the interoperability features as defined by HIMSS, the first basic feature is defined as such that medical data should be able to be shared between two systems. We confirmed that medical imaging related data such as imaging study, patient, endpoint, and phantom data can be transferred through a medical data exchange server based on HL7 standards.
The second feature as defined by HIMSS states that formats and structures must be defined so that data cannot be tampered with or modified. The data formats within the HL7 FHIR server are defined as XML and JSON with the data structure following Resource.
The third feature states that no issues should arise in the safe exchange, use and interpretation of medical information between two or more medical systems. By using phantom data, medical images collected from different locations can be used in a qualitative manner by applying the same standards.
The interoperability reference model created can enable the use of medical imaging on a large scale. As a large amount of data is required for deep learning, the process of increasing the quality of data before image training is important. It is necessary to check whether quantified images increase deep learning performance; we will conduct a further study that shows the results of applying deep learning techniques to MRI images with a reference model.
The use of medical devices that apply artificial intelligence is growing within the medical devices industry. For example, integrating the reference model to other medical visualization modules that can transfer informative medical volume such as clustering data [
25] and are suitable for handing large amounts of medical imaging data [
26] is able to contribute to improving medical image artificial intelligence performance.
In addition, the U.S. Food and Drug Administration (FDA) has defined the concept of Software as a Medical Device (SaMD) and allowed the foundation for artificial intelligence to be certified as a medical tool [
27]. The interoperability reference model proposed by this study is believed to be able to provide further developments to the artificial intelligence medical devices industry.



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}