
Knee MRI Underestimates the Grade of Cartilage Lesions

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Curl, W.W.; Krome, J.; Gordon, E.S.; Rushing, J.; Smith, B.P.; Poehling, G.G. Cartilage Injuries: A Review of 31,516 Knee Arthroscopies. Arthroscopy 1997, 13, 456–460. [Google Scholar] [CrossRef]
- Cibere, J.; Sayre, E.C.; Guermazi, A.; Nicolaou, S.; Kopec, J.A.; Esdaile, J.M.; Thorne, A.; Singer, J.; Wong, H. Natural History of Cartilage Damage and Osteoarthritis Progression on Magnetic Resonance Imaging in a Population-Based Cohort with Knee Pain. Osteoarthr. Cartil. 2011, 19, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Palmer, A.J.R.; Brown, C.P.; McNally, E.G.; Price, A.J.; Tracey, I.; Jezzard, P.; Carr, A.J.; Jones, G.S. Non-Invasive Imaging of Cartilage in Early Osteoarthritis. Bone Jt. J. 2013, 95, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, D.; Calvo, R.; Vaisman, A.; Carrasco, M.A.; Moraga, C.; Delgado, I. Knee Chondral Lesions: Incidence and Correlation Between Arthroscopic and Magnetic Resonance Findings. Arthroscopy J. Arthrosc. Relat. Surg. 2007, 23, 312–315. [Google Scholar] [CrossRef]
- Bredella, M.A.; Tirman, P.F.; Peterfy, C.G.; Zarlingo, M.; Feller, J.F.; Bost, F.W.; Belzer, J.P.; Wischer, T.K.; Genant, H.K. Accuracy of T2-Weighted Fast Spin-Echo MR Imaging with Fat Saturation in Detecting Cartilage Defects in the Knee: Comparison with Arthroscopy in 130 Patients. Am. J. Roentgenol. 1999, 172, 1073–1080. [Google Scholar] [CrossRef]
- Thomas, S.; Pullagura, M.; Robinson, E.; Cohen, A.; Banaszkiewicz, P. The Value of Magnetic Resonance Imaging in Our Current Management of ACL and Meniscal Injuries. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 533–536. [Google Scholar] [CrossRef]
- Guermazi, A.; Alizai, H.; Crema, M.D.; Trattnig, S.; Regatte, R.R.; Roemer, F.W. Compositional MRI Techniques for Evaluation of Cartilage Degeneration in Osteoarthritis. Osteoarthr. Cartil. 2015, 23, 1639–1653. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, K.M.; Mamisch, T.C.; Plank, C.; Langs, G.; Marlovits, S.; Salomonowitz, E.; Trattnig, S.; Welsch, G. Diffusion-Weighted Imaging for the Follow-up of Patients after Matrix-Associated Autologous Chondrocyte Transplantation. Eur. J. Radiol. 2010, 73, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Lesperance, L.M.; Gray, M.L.; Burstein, D. Determination of Fixed Charge Density in Cartilage Using Nuclear Magnetic Resonance. J. Orthop. Res. 1992, 10, 1–13. [Google Scholar] [CrossRef]
- Allen, R.G.; Burstein, D.; Gray, M.L. Monitoring Glycosaminoglycan Replenishment in Cartilage Explants with Gadolinium-Enhanced Magnetic Resonance Imaging: Monitoring Glycosaminoglycan Replenishment with Mri. J. Orthop. Res. 1999, 17, 430–436. [Google Scholar] [CrossRef]
- Bashir, A.; Gray, M.L.; Boutin, R.D.; Burstein, D. Glycosaminoglycan in Articular Cartilage: In Vivo Assessment with Delayed Gd (DTPA) (2-)-Enhanced MR Imaging. Radiology 1997, 205, 551–558. [Google Scholar] [CrossRef]
- Regatte, R.R.; Akella, S.V.S.; Lonner, J.H.; Kneeland, J.B.; Reddy, R. T1ρ Relaxation Mapping in Human Osteoarthritis (OA) Cartilage: Comparison of T1ρ with T2. J. Magn. Reson. Imaging 2006, 23, 547–553. [Google Scholar] [CrossRef]
- Burstein, D.; Velyvis, J.; Scott, K.T.; Stock, K.W.; Kim, Y.J.; Jaramillo, D.; Boutin, R.D.; Gray, M.L. Protocol Issues for Delayed Gd (DTPA) (2-)-Enhanced MRI (DGEMRIC) for Clinical Evaluation of Articular Cartilage. Magn. Reason. Med. 2001, 45, 36–41. [Google Scholar] [CrossRef]
- Abrar, D.B.; Schleich, C.; Radke, K.L.; Frenken, M.; Stabinska, J.; Ljimani, A.; Wittsack, H.J.; Antoch, G.; Bittersohl, B.; Hesper, T.; et al. Detection of Early Cartilage Degeneration in the Tibiotalar Joint Using 3 T GagCEST Imaging: A Feasibility Study. Magn. Reason. Mater. Phy. 2020. [Google Scholar] [CrossRef]
- Shakoor, D.; Guermazi, A.; Kijowski, R.; Fritz, J.; Farahani, J.S.; Mohajer, B.; Eng, J.; Demehri, S. Diagnostic Performance of Three-Dimensional MRI for Depicting Cartilage Defects in the Knee: A Meta-Analysis. Radiology 2018, 289, 71–82. [Google Scholar] [CrossRef]
- Kohl, S.; Meier, S.; Ahmad, S.S.; Bonel, H.; Exadaktylos, A.K.; Krismer, A.; Evangelopoulos, D.S. Accuracy of Cartilage-Specific 3-Tesla 3D-DESS Magnetic Resonance Imaging in the Diagnosis of Chondral Lesions: Comparison with Knee Arthroscopy. J. Orthop. Surg. Res. 2015, 10, 191. [Google Scholar] [CrossRef] [PubMed]
- Gomoll, A.H.; Farr, J.; Gillogly, S.D.; Kercher, J.S.; Minas, T. Surgical Management of Articular Cartilage Defects of the Knee. Instr. Course Lect. 2011, 60, 461–483. [Google Scholar] [PubMed]
- Smith, G.D.; Knutsen, G.; Richardson, J.B. A Clinical Review of Cartilage Repair Techniques. J. Bone Jt. Surg. Br. Vol. 2015, 87-B, 445–449. [Google Scholar] [CrossRef]
- Bryan, S.; Bungay, H.P.; Weatherburn, G.; Field, S. Magnetic Resonance Imaging for Investigation of the Knee Joint: A Clinical and Economic Evaluation. Int. J. Technol. Assess. Health Care 2004, 20, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.O.; Drew, B.T.; Toms, A.P.; Donell, S.T.; Hing, C.B. Accuracy of Magnetic Resonance Imaging, Magnetic Resonance Arthrography and Computed Tomography for the Detection of Chondral Lesions of the Knee. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2367–2379. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.L.; Briggs, K.K.; Steadman, J.R. Reproducibility and Reliability of the Outerbridge Classification for Grading Chondral Lesions of the Knee Arthroscopically. Am. J. Sports Med. 2003, 31, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Brittberg, M.; Winalski, C.S. Evaluation of Cartilage Injuries and Repair. J. Bone Jt. Surg. Am. 2003, 85, 58–69. [Google Scholar] [CrossRef]
- Cohen, J. Weighted Kappa: Nominal Scale Agreement Provision for Scaled Disagreement or Partial Credit. Psychol. Bull. 1968, 70, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Bangdiwala, S.I.; Haedo, A.S.; Natal, M.L.; Villaveces, A. The Agreement Chart as an Alternative to the Receiver-Operating Characteristic Curve for Diagnostic Tests. J. Clin. Epidemiol. 2008, 61, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Bangdiwala, S.I.; Shankar, V. The Agreement Chart. BMC Med. Res. Methodol. 2013, 13, 97. [Google Scholar] [CrossRef]
- On behalf of the College of Intensive Care Medicine of Australia and New Zealand [CICM] Ultrasound Special Interest Group [USIG]; Orde, S.; Slama, M.; Yastrebov, K.; Mclean, A.; Huang, S. Subjective Right Ventricle Assessment by Echo Qualified Intensive Care Specialists: Assessing Agreement with Objective Measures. Crit. Care 2019, 23, 70. [Google Scholar] [CrossRef] [PubMed]
- Munoz, S.R.; Bangdiwala, S.I. Interpretation of Kappa and B Statistics Measures of Agreement. J. Appl. Stat. 1997, 24, 105–112. [Google Scholar] [CrossRef]
- Warrens, M.J. Five Ways to Look at Cohen’s Kappa. J. Psychol. Psychother. 2015, 5, 1. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Roemer, F.; Jarraya, M.; Niu, J.; Silva, J.; Frobell, R.; Guemrazi, A. Increased Risk for Radiographic Osteoarthritis Features in Young Active Athletes: A Cross-Sectional Matched Case–Control Study. Osteoarthr. Cartil. 2015, 23, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Królikowska, A.; Czamara, A.; Kentel, M. Does Gracilis Tendon Harvest During ACL Reconstruction with a Hamstring Autograft Affect Torque of Muscles Responsible for Shin Rotation? Med. Sci. Monit. 2015, 21, 2084–2093. [Google Scholar] [CrossRef]
- Abrar, D.B.; Schleich, C.; Nebelung, S.; Frenken, M.; Ullrich, T.; Radke, K.L.; Antoch, G.; Vordenbäumen, S.; Brinks, R.; Schneider, M.; et al. Proteoglycan Loss in the Articular Cartilage Is Associated with Severity of Joint Inflammation in Psoriatic Arthritis—a Compositional Magnetic Resonance Imaging Study. Arthritis Res. Ther. 2020, 22, 124. [Google Scholar] [CrossRef]
- Said, O.; Schock, J.; Krämer, N.; Thüring, J.; Hitpass, L.; Schad, P.; Kuhl, C.; Abrar, D.; Truhn, D.; Nebelung, S. An MRI-Compatible Varus–Valgus Loading Device for Whole-Knee Joint Functionality Assessment Based on Compartmental Compression: A Proof-of-Concept Study. Magn. Reason. Mater. Phy. 2020, 33, 839–854. [Google Scholar] [CrossRef]
- Krakowski, P.; Nogalski, A.; Jurkiewicz, A.; Karpiński, R.; Maciejewski, R.; Jonak, J. Comparison of Diagnostic Accuracy of Physical Examination and MRI in the Most Common Knee Injuries. Appl. Sci. 2019, 9, 4102. [Google Scholar] [CrossRef]
- Crema, M.D.; Roemer, F.W.; Marra, M.D.; Burstein, D.; Gold, G.E.; Eckstein, F.; Baum, T.; Mosher, T.J.; Carrino, J.A.; Guermazi, A. Articular Cartilage in the Knee: Current MR Imaging Techniques and Applications in Clinical Practice and Research. Radiographics 2011, 31, 37–61. [Google Scholar] [CrossRef]
- Marx, R.G.; Connor, J.; Lyman, S.; Amendola, A.; Andrish, J.T.; Kaeding, C.; McCarty, E.C.; Parker, R.D.; Wright, R.W.; Spindler, K.P. Multirater Agreement of Arthroscopic Grading of Knee Articular Cartilage. Am. J. Sports Med. 2005, 33, 1654–1657. [Google Scholar] [CrossRef] [PubMed]
- Javed, A.; Siddique, M.; Vaghela, M.; Hui, A.C.W. Interobserver Variations in Intra-Articular Evaluation during Arthroscopy of the Knee. J. Bone Jt. Surg. Br. 2002, 84, 48–49. [Google Scholar] [CrossRef]
- Wong, K.P.L.; Han, A.X.; Wong, J.L.Y.; Lee, D.Y.H. Reliability of Magnetic Resonance Imaging in Evaluating Meniscal and Cartilage Injuries in Anterior Cruciate Ligament-Deficient Knees. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Hafner, T.; Schock, J.; Post, M.; Abrar, D.B.; Sewerin, P.; Linka, K.; Knobe, M.; Kuhl, C.; Truhn, D.; Nebelung, S. A Serial Multiparametric Quantitative Magnetic Resonance Imaging Study to Assess Proteoglycan Depletion of Human Articular Cartilage and Its Effects on Functionality. Sci. Rep. 2020, 10, 15106. [Google Scholar] [CrossRef] [PubMed]
- Akella, S.V.S.; Regatte, R.R.; Gougoutas, A.J.; Borthakur, A.; Shapiro, E.M.; Kneeland, J.B.; Leigh, J.S.; Reddy, R. Proteoglycan-Induced Changes InT1? Relaxation of Articular Cartilage at 4T. Magn. Reson. Med. 2001, 46, 419–423. [Google Scholar] [CrossRef]
- MacKay, J.W.; Low, S.B.L.; Smith, T.O.; Toms, A.P.; McCaskie, A.W.; Gilbert, F.J. Systematic Review and Meta-Analysis of the Reliability and Discriminative Validity of Cartilage Compositional MRI in Knee Osteoarthritis. Osteoarthr. Cartil. 2018, 26, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- Svoboda, S.J. ACL Injury and Posttraumatic Osteoarthritis. Clin. Sports Med. 2014, 33, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.H.; Spindler, K.P. Risk Factors for Radiographic Joint Space Narrowing and Patient Reported Outcomes of Post-Traumatic Osteoarthritis after ACL Reconstruction: Data from the MOON Cohort: Ptoa After Acl Reconstruction in Moon. J. Orthop. Res. 2017, 35, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Quatman, C.E.; Hettrich, C.M.; Schmitt, L.C.; Spindler, K.P. The Clinical Utility and Diagnostic Performance of Magnetic Resonance Imaging for Identification of Early and Advanced Knee Osteoarthritis: A Systematic Review. Am. J. Sports Med. 2011, 39, 1557–1568. [Google Scholar] [CrossRef]
- Kijowski, R.; Davis, K.W.; Woods, M.A.; Lindstrom, M.J.; De Smet, A.A.; Gold, G.E.; Busse, R.F. Knee Joint: Comprehensive Assessment with 3D Isotropic Resolution Fast Spin-Echo MR Imaging—Diagnostic Performance Compared with That of Conventional MR Imaging at 3.0 T. Radiology 2009, 252, 486–495. [Google Scholar] [CrossRef]
- Carotti, M.; Salaffi, F.; Di Carlo, M.; Giovagnoni, A. Relationship between Magnetic Resonance Imaging Findings, Radiological Grading, Psychological Distress and Pain in Patients with Symptomatic Knee Osteoarthritis. Radiol. Med. 2017, 122, 934–943. [Google Scholar] [CrossRef]
- Vanhoenacker, F.; De Vos, N.; Van Dyck, P. Common Mistakes and Pitfalls in Magnetic Resonance Imaging of the Knee. J. Belg. Soc. Radiol. 2016, 100, 99. [Google Scholar] [CrossRef]
- Solivetti, F.M.; Guerrisi, A.; Salducca, N.; Desiderio, F.; Graceffa, D.; Capodieci, G.; Romeo, P.; Sperduti, I.; Canitano, S. Appropriateness of Knee MRI Prescriptions: Clinical, Economic and Technical Issues. Radiol. Med. 2016, 121, 315–322. [Google Scholar] [CrossRef]
- García, G.J.M.; Romero, G.F.J.; Jiménez, A.M.; Gracia, N.J.F.; Mollá, S.M. Appropriateness of Magnetic Resonance Imaging Requested by Primary Care Physicians for Patients with Knee Pain. Int. J. Qual. Health Care 2018, 30, 565–570. [Google Scholar] [CrossRef]
- Roberts, T.T.; Singer, N.; Hushmendy, S.; Dempsey, I.J.; Roberts, J.T.; Uhl, R.L.; Johnson, P.E. MRI for the Evaluation of Knee Pain: Comparison of Ordering Practices of Primary Care Physicians and Orthopaedic Surgeons. J. Bone Jt. Surg. Am. Vol. 2015, 97, 709–714. [Google Scholar] [CrossRef]
- Nacey, N.C.; Geeslin, M.G.; Miller, G.W.; Pierce, J.L. Magnetic Resonance Imaging of the Knee: An Overview and Update of Conventional and State of the Art Imaging: Knee MRI: Overview and Update. J. Magn. Reson. Imaging 2017, 45, 1257–1275. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.; Gold, G.E.; Andriacchi, T.P. Considerations in Measuring Cartilage Thickness Using MRI: Factors Influencing Reproducibility and Accuracy. Osteoarthr. Cartil. 2005, 13, 782–789. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
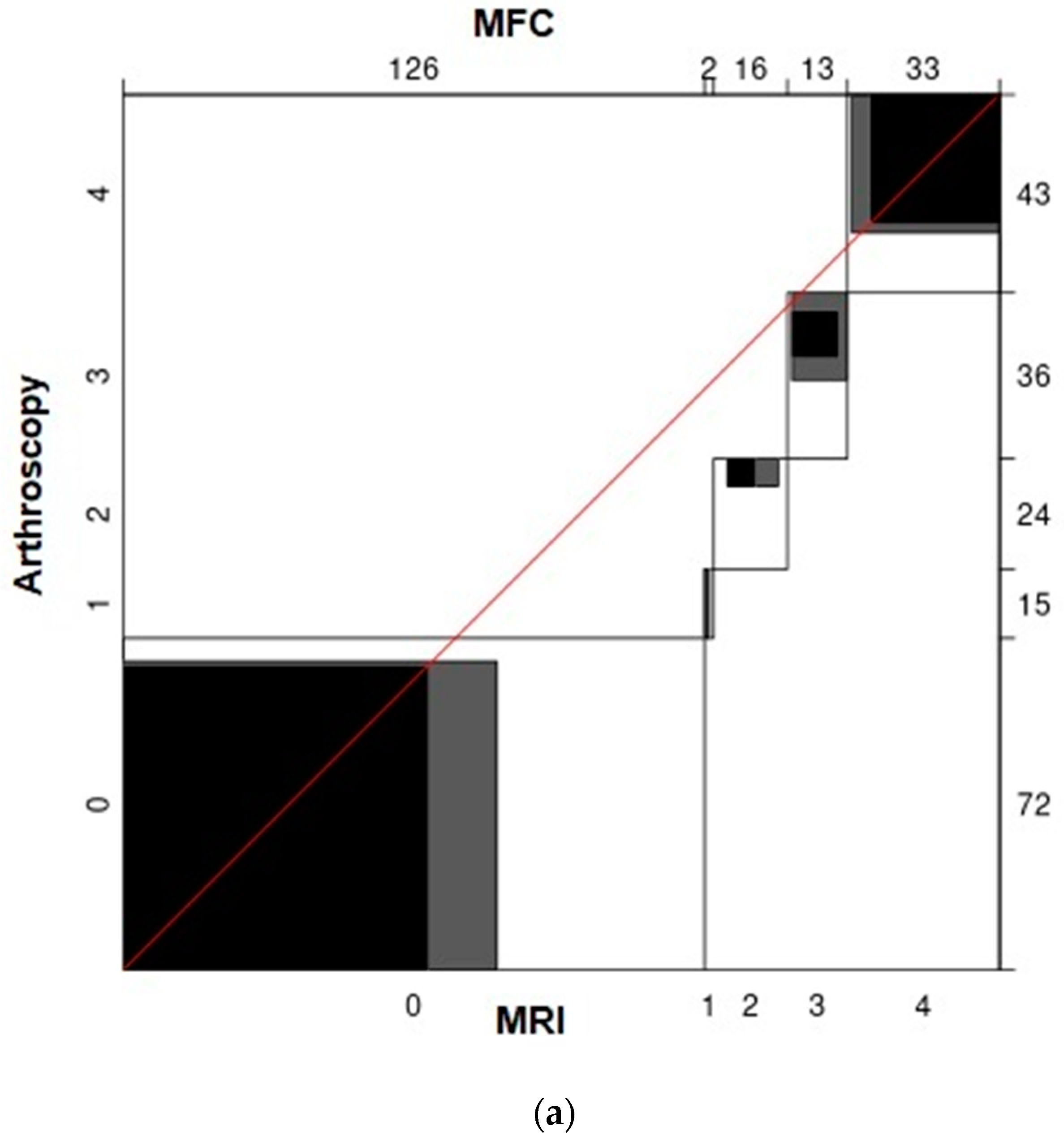
| Location | Cartilage Status According to ICRS | Cartilage Lesions in Total | ||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | ||
| MFC | 72 | 15 | 24 | 36 | 43 | 118 |
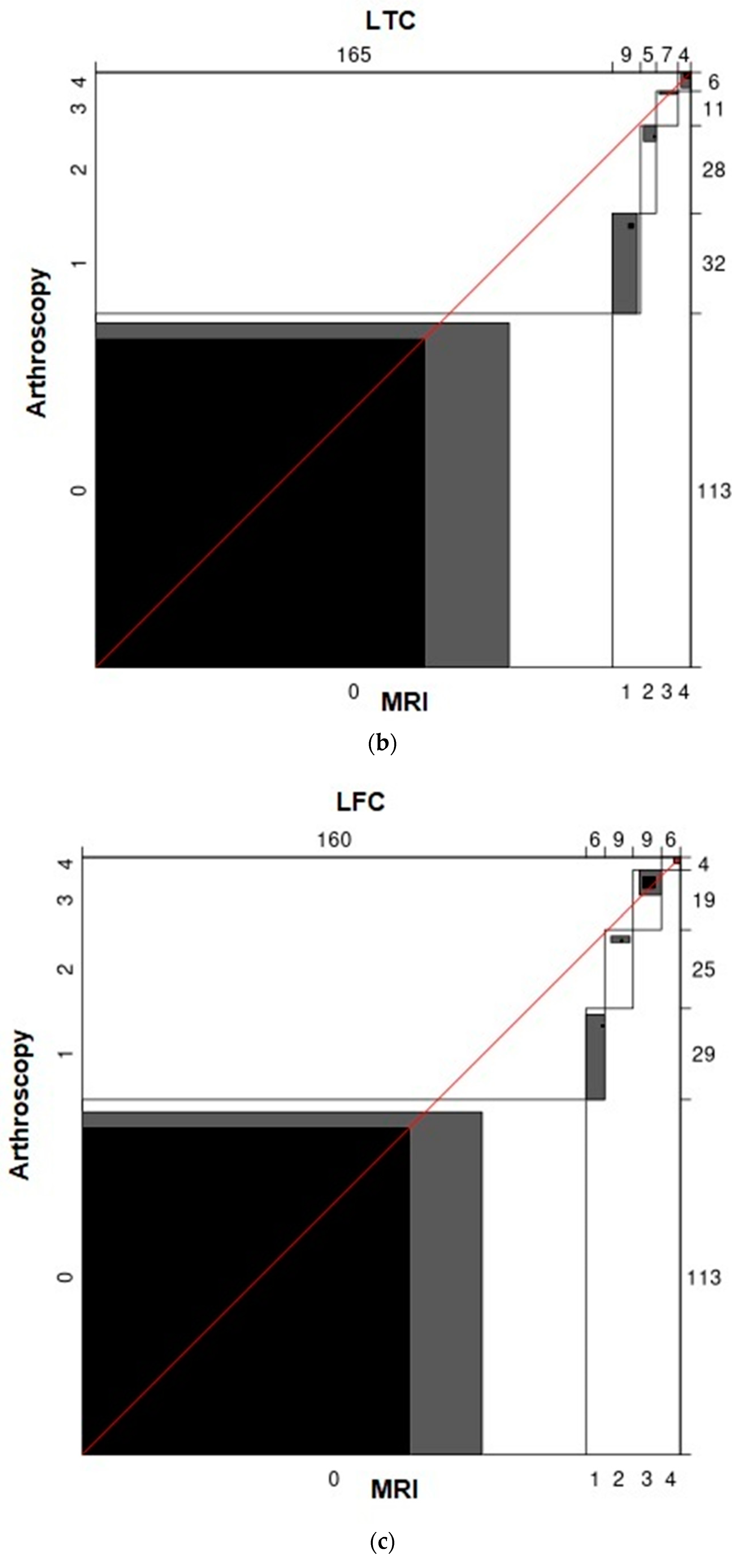
| LFC | 113 | 29 | 25 | 19 | 4 | 77 |
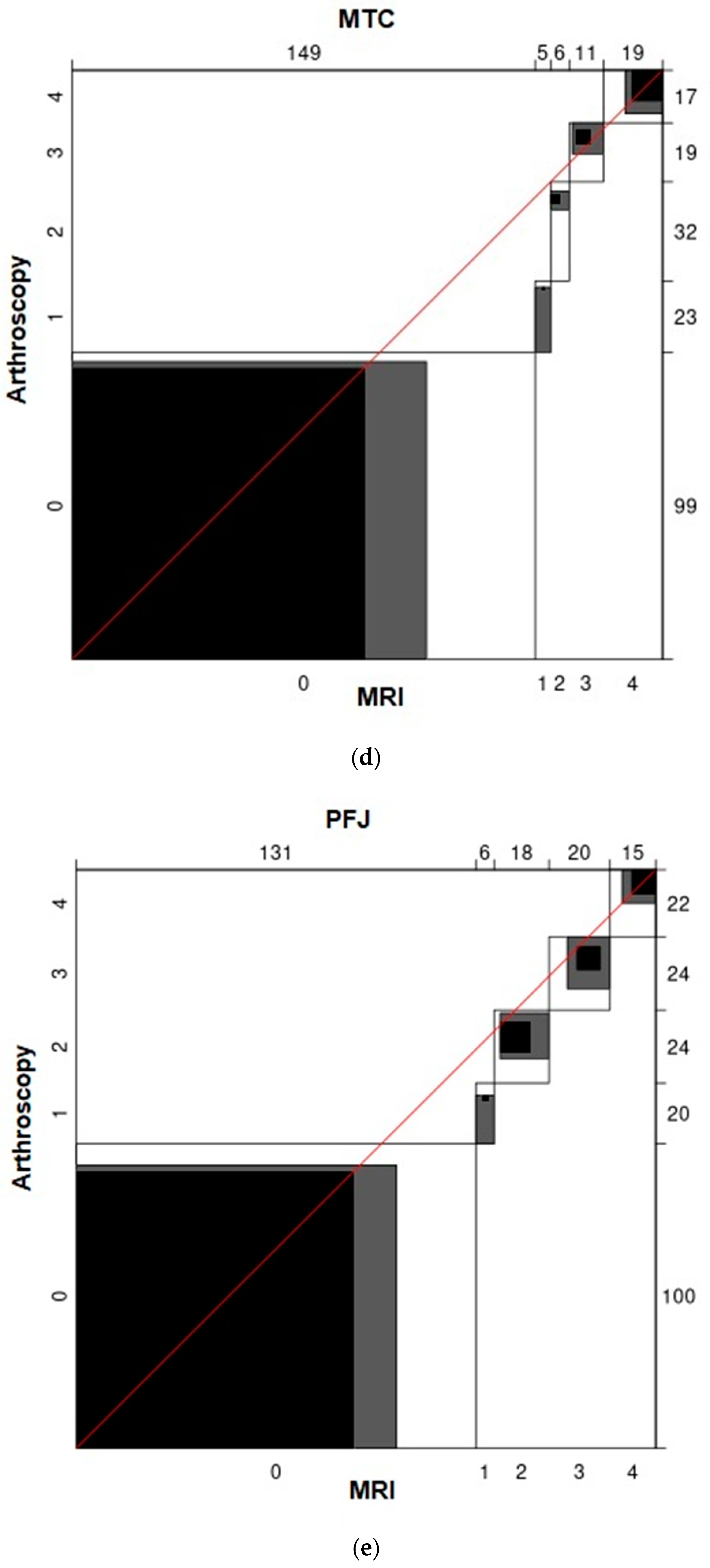
| MTC | 99 | 23 | 32 | 19 | 17 | 91 |
| LTC | 113 | 32 | 28 | 11 | 6 | 77 |
| PFJ | 100 | 20 | 24 | 24 | 22 | 90 |
| Total | 497 | 119 | 133 | 109 | 92 | 453 |
| MFC | LFC | MTC | LTC | PFJ | Mean | ||
|---|---|---|---|---|---|---|---|
| 0 | Sensitivity | 91.67% | 92.04% | 94.95% | 92.92% | 91.00% | 92.51% |
| Specificity | 49.15% | 27.27% | 39.56% | 22.08% | 55.56% | 38.72% | |
| 1 | Sensitivity | 0.00% | 3.45% | 4.35% | 6.25% | 10.00% | 4.81% |
| Specificity | 98.86% | 96.89% | 97.60% | 95.57% | 97.65% | 97.31% | |
| 2 | Sensitivity | 25.00% | 4.00% | 9.38% | 3.57% | 41.67% | 16.72% |
| Specificity | 93.98% | 95.15% | 98.10% | 97.53% | 95.18% | 95.99% | |
| 3 | Sensitivity | 27.78% | 21.05% | 26.32% | 0.00% | 33.33% | 21.70% |
| Specificity | 98.05% | 97.08% | 96.49% | 96.09% | 92.77% | 96.10% | |
| 4 | Sensitivity | 65.12% | 0.00% | 58.82% | 33.33% | 36.36% | 38.73% |
| Specificity | 96.60% | 96.77% | 94.80% | 98.91% | 95.83% | 96.58% | |
| Mean | Sensitivity | 41.91% | 24.11% | 38.76% | 27.22% | 42.47% | |
| Specificity | 87.33% | 82.63% | 85.31% | 82.04% | 87.40% |
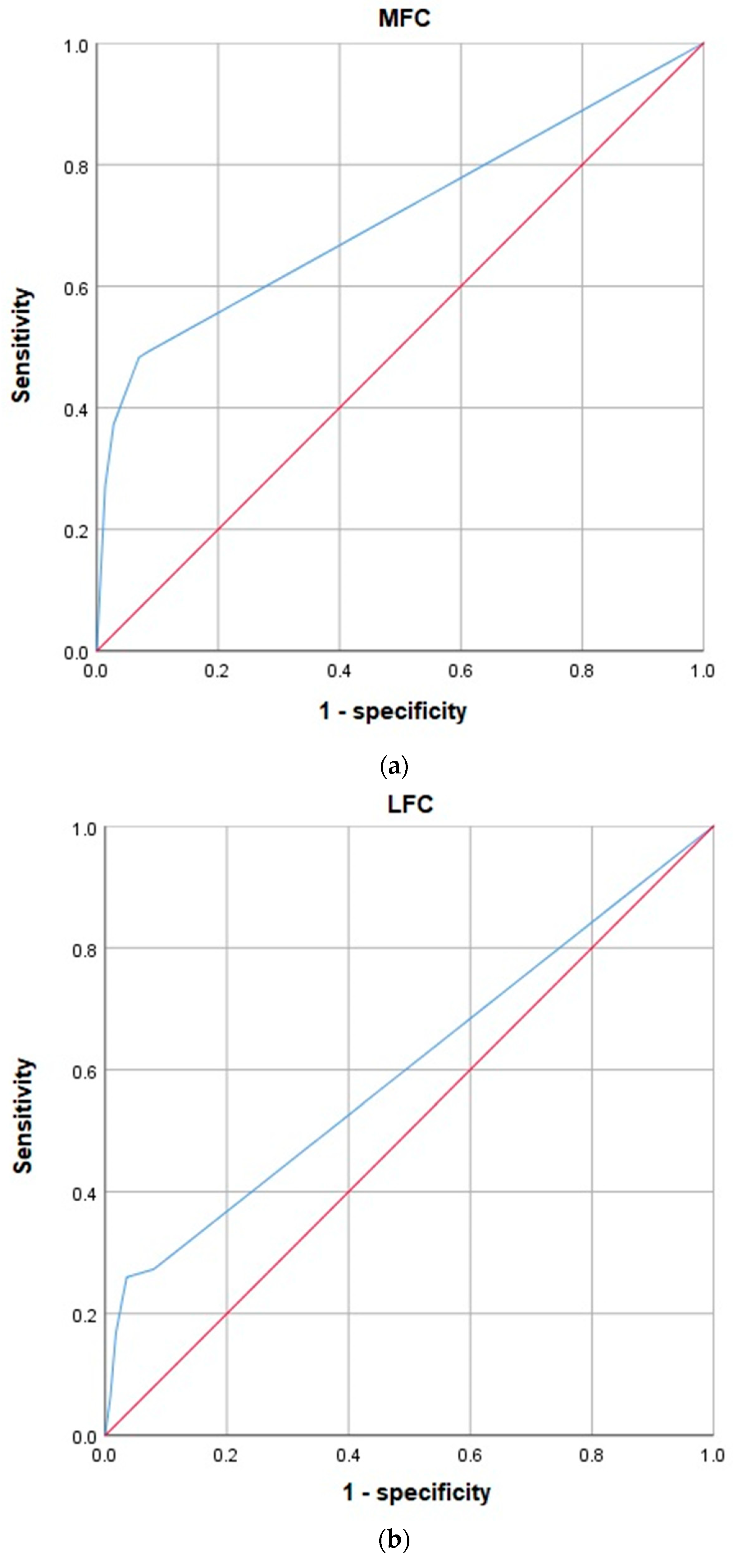
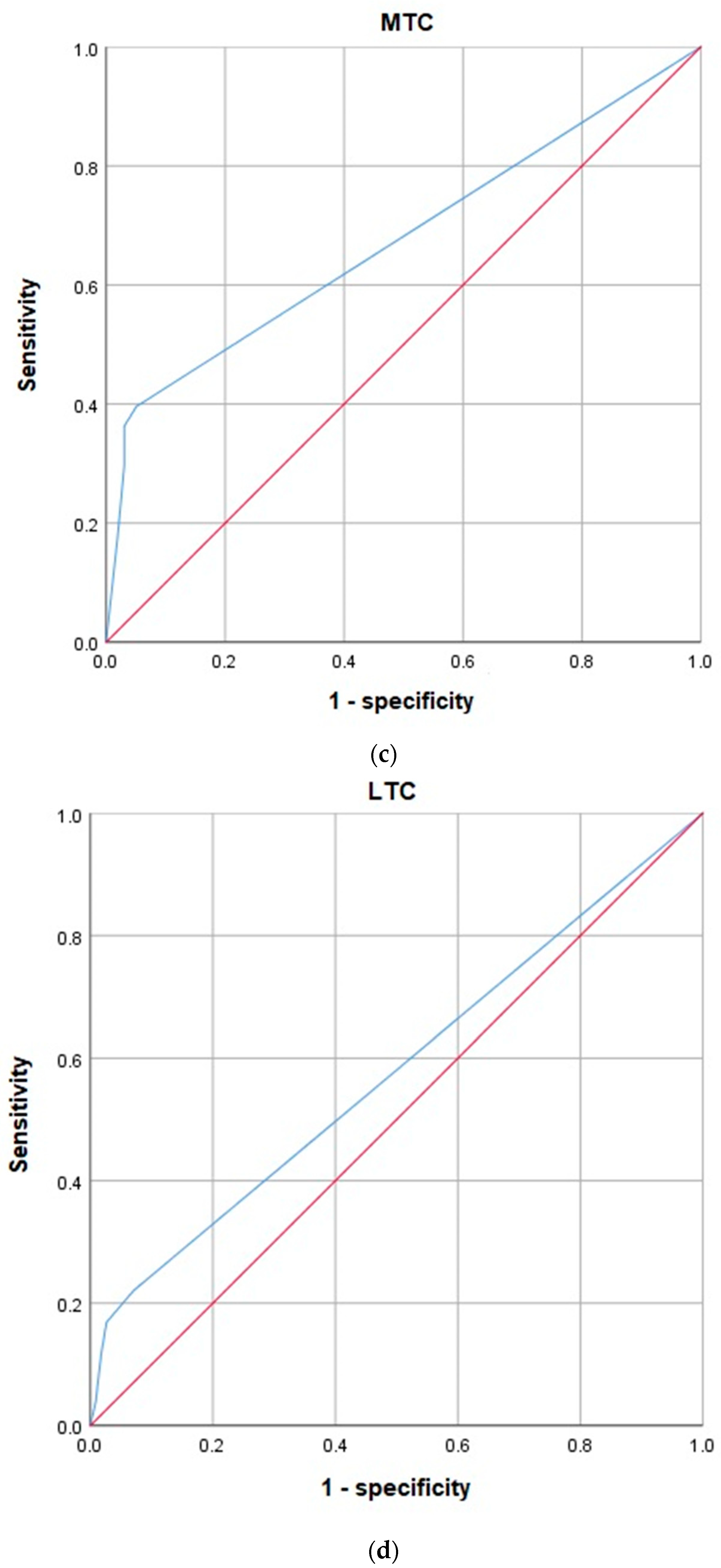
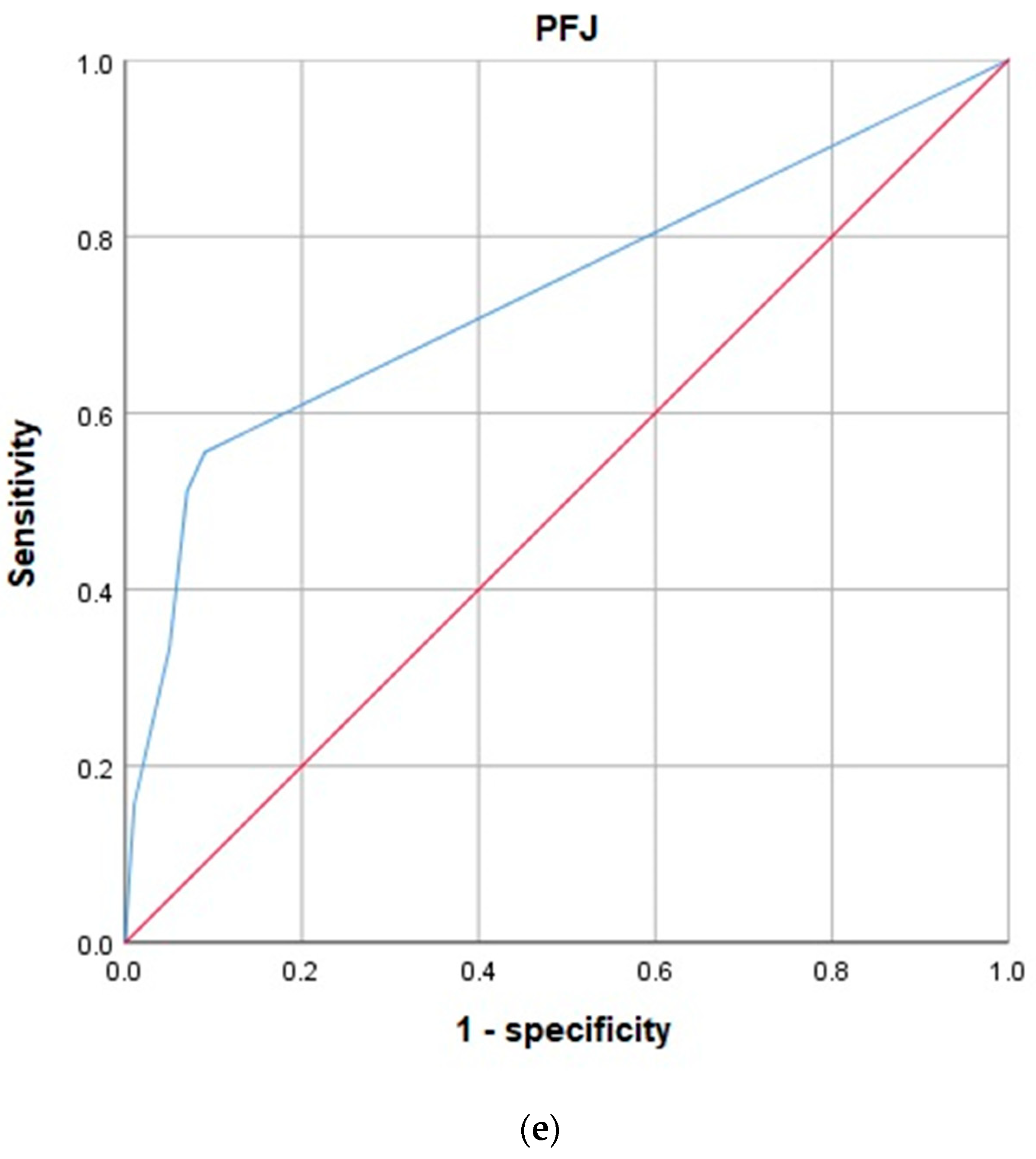
| Asymptotic 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| Tested Variables | Area under the Curve | SD | Asymptotic Significance | Inferior Boundary Value | Superior Boundary Value |
| MFC | 0.715 | 0.036 | 0.000 | 0.643 | 0.786 |
| LFC | 0.603 | 0.043 | 0.016 | 0.518 | 0.687 |
| MTC | 0.675 | 0.040 | 0.000 | 0.597 | 0.752 |
| LTC | 0.578 | 0.043 | 0.068 | 0.493 | 0.663 |
| PFJ | 0.737 | 0.037 | 0.000 | 0.664 | 0.811 |
| Value | ASE | z | ||
|---|---|---|---|---|
| MFC | Unweighted | 0.39 | 0.046 | 8.387 |
| Weighted | 0.57 | 0.054 | 10.684 | |
| LFC | Unweighted | 0.13 | 0.042 | 3.015 |
| Weighted | 0.36 | 0.077 | 4.739 | |
| MTC | Unweighted | 0.29 | 0.047 | 6.094 |
| Weighted | 0.56 | 0.064 | 8.777 | |
| LTC | Unweighted | 0.10 | 0.041 | 2.473 |
| Weighted | 0.35 | 0.092 | 3.819 | |
| PFJ | Unweighted | 0.38 | 0.049 | 7.626 |
| Weighted | 0.50 | 0.069 | 7.335 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krakowski, P.; Karpiński, R.; Jojczuk, M.; Nogalska, A.; Jonak, J. Knee MRI Underestimates the Grade of Cartilage Lesions. Appl. Sci. 2021, 11, 1552. https://doi.org/10.3390/app11041552
Krakowski P, Karpiński R, Jojczuk M, Nogalska A, Jonak J. Knee MRI Underestimates the Grade of Cartilage Lesions. Applied Sciences. 2021; 11(4):1552. https://doi.org/10.3390/app11041552
Chicago/Turabian StyleKrakowski, Przemysław, Robert Karpiński, Mariusz Jojczuk, Agata Nogalska, and Józef Jonak. 2021. "Knee MRI Underestimates the Grade of Cartilage Lesions" Applied Sciences 11, no. 4: 1552. https://doi.org/10.3390/app11041552
APA StyleKrakowski, P., Karpiński, R., Jojczuk, M., Nogalska, A., & Jonak, J. (2021). Knee MRI Underestimates the Grade of Cartilage Lesions. Applied Sciences, 11(4), 1552. https://doi.org/10.3390/app11041552