
An Ancient Mesiodens Investigated by Cone Beam CT

 ,
,  and
and 
Abstract
:1. Introduction
1.1. Archaeological Background
1.2. Supernumerary Teeth
2. Materials and Methods
3. Results
3.1. Sex, Stature and Age
3.2. Inspection of the Jaws
3.2.1. The Maxilla
3.2.2. The Mandible
3.2.3. The Teeth
3.2.4. The Occlusion
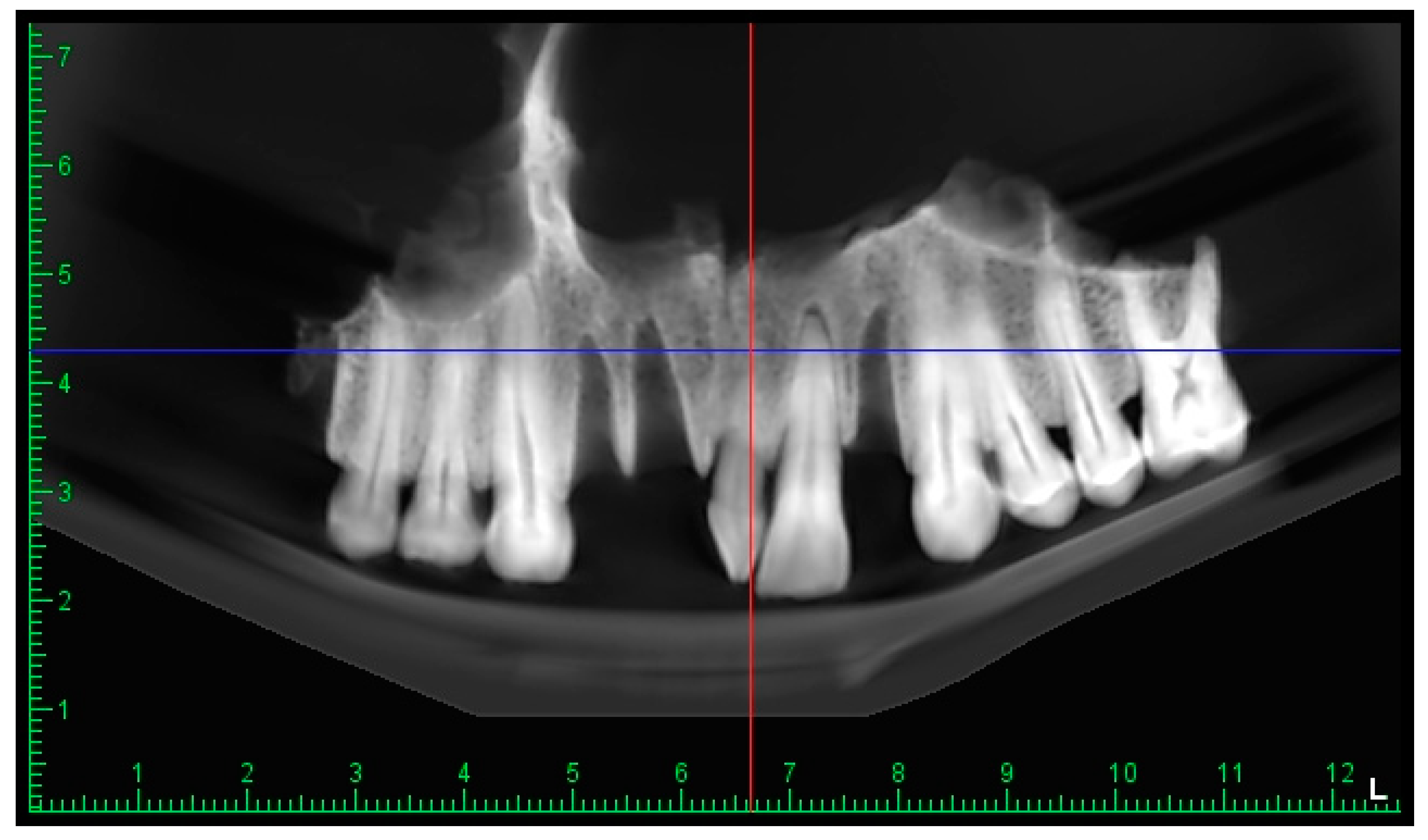
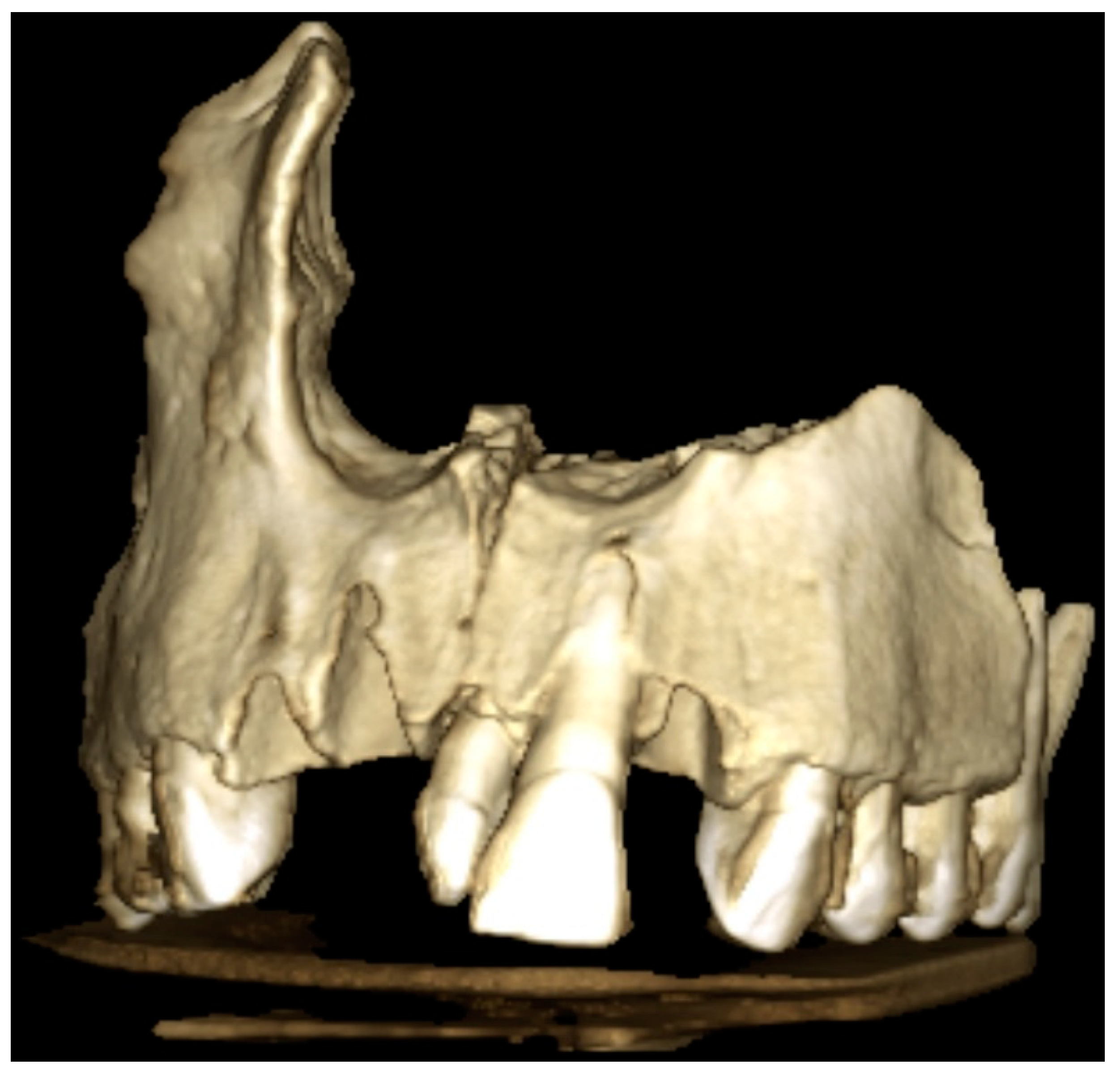
3.2.5. The Mesiodens
3.3. The CBCT Scan
4. Discussion
4.1. Tooth Development and Why Tooth Anomalies of Number, Size and Structure Are Connected
4.2. Is Hypodontia More Frequent in Present-Day Populations and Were Supernumeraries More Frequent in the Past?
4.3. The Role of CBCT in Paleoimaging
4.4. The “Individual 1” Case
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pearce, M. The ‘Copper Age’-A History of the Concept. J. World Prehistory 2019, 32, 229–250. [Google Scholar] [CrossRef] [Green Version]
- Stratton, S. Burial and Identity in the Late Neolithic and Copper Age of South-East Europe. Ph.D. Thesis, Cardiff University, Cardiff, Wales, 2016. [Google Scholar]
- Mallory, J.P.; Adams, D.Q. (Eds.) Encyclopedia of Indo-European Culture; Fitzroy Dearborn Publishers: London, UK; Chicago, IL, USA, 1997. [Google Scholar]
- Jochim, M. The Lower and Middle Palaeolithic. In European Prehistory; Milisauskas, S., Ed.; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012; pp. 15–54. [Google Scholar]
- Raczky, P.; Siklósi, Z. Reconsideration of the Copper Age chronology of the eastern Carpathian Basin: A Bayesian approach. Antiquity 2013, 87, 555–573. [Google Scholar] [CrossRef]
- Diaconescu, D. Consideraţii Privind Cronologia Epocii Timpurii a Cuprului în Estul Bazinului Carpatic (Cultura Tiszapolgár). Available online: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=mZeUHyIAAAAJ&citation_for_view=mZeUHyIAAAAJ:9yKSN-GCB0IC (accessed on 23 August 2020).
- Sava, V. Neolithic and Eneolithic in the Lower Mures Basin; Mega Publishing House: Cluj-Napoca, Romania, 2015; p. 89. [Google Scholar]
- Rajab, L.D.; Hamdan, M.A.M. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int. J. Paediatr. Dent. 2002, 12, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Indira, M.D.; Dhull, K.S.; Sujartha, R.; Kumar Ps, P.; Devi Bm, G. Molariform mesiodens in primary dentition: A case report. J. Clin. Diagn. Res. 2014, 8, 33–35. [Google Scholar] [CrossRef]
- Scheiner, M.A.; Sampson, W.J. Supernumerary teeth: A review of the literature and four case reports. Aust. Dent. J. 1997, 42, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández Montenegro, P.; Valmaseda Castellón, E.; Berini Aytés, L.; Gay Escoda, C. Retrospective study of 145 supernumerary teeth. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, 240–245. [Google Scholar]
- Mossaz, J.; Kloukos, D.; Pandis, N.; Suter, V.G.A.; Katsaros, C.; Bornstein, M.M. Morphologic characteristics, location, and associated complications of maxillary and mandibular supernumerary teeth as evaluated using cone beam computed tomography. Eur. J. Orthod. 2014, 36, 708–718. [Google Scholar] [CrossRef] [Green Version]
- Ramesh, K.; Venkataraghavan, K.; Kunjappan, S.; Ramesh, M. Mesiodens: A clinical and radiographic study of 82 teeth in 55 children below 14 years. J. Pharm. Bioallied Sci. 2013, 5 (Suppl. 1), 60–62. [Google Scholar] [CrossRef] [PubMed]
- Meighani, G.; Pakdaman, A. Diagnosis and management of supernumerary (mesiodens): A review of the literature. J. Dent. (Tehran) 2010, 7, 41–49. [Google Scholar]
- Orhan, A.I.; Ozer, L.; Orhan, K. Familial occurrence of nonsyndromal multiple supernumerary teeth. A rare condition. Angle Orthod. 2006, 76, 891–897. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Gentile, M.; Inchingolo, A.M.; Dipalma, G. Non-syndromic multiple supernumerary teeth in a family unit with a normal karyotype: Case report. Int. J. Med. Sci. 2010, 7, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.F.; Marcushamer, M.; King, D.L.; Henry, R.J. Supernumerary and congenitally absent teeth: A literature review. J. Clin. Pediatr. Dent. 1996, 20, 87–95. [Google Scholar]
- Türkkahraman, H.; Yılmaz, H.H.; Çetin, E. A non-syndrome case with bilateral supernumerary canines: Report of a rare case. Dentomaxillofac. Radiol. 2005, 34, 319–321. [Google Scholar] [CrossRef]
- Parolia, A.; Kundabala, M.; Dahal, M.; Mohan, M.; Thomas, M.S. Management of supernumerary teeth. J. Conserv. Dent. 2011, 14, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Brook, A.H.; Griffin, R.C.; Smith, R.N.; Townsend, G.C.; Kaur, G.; Davis, G.R.; Fearne, J. Tooth size patterns in patients with hypodontia and supernumerary teeth. Arch. Oral Biol. 2009, 54 (Suppl. 1), 63–70. [Google Scholar] [CrossRef] [PubMed]
- Brook, A.H. Multilevel complex interactions between genetic, epigenetic and environmental factors in the aetiology of anomalies of dental development. Arch. Oral Biol. 2009, 54 (Suppl. 1), 3–17. [Google Scholar] [CrossRef] [PubMed]
- Van Buggenhout, G.; Bailleul-Forestier, I. Mesiodens. Eur. J. Med. Genet. 2008, 51, 178–181. [Google Scholar] [CrossRef]
- Högström, A.; Andersson, L. Complications related to surgical removal of anterior supernumerary teeth in children. ASDC J. Dent. Child. 1987, 54, 341–343. [Google Scholar] [PubMed]
- Açıkgöz, A.; Açıkgöz, G.; Tunga, U.; Otan, F. Characteristics and prevalence of non-syndrome multiple supernumerary teeth: A retrospective study. Dentomaxillofac. Radiol. 2006, 35, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Buikstra, J.E.; Ubelaker, D.H. Standards for Data Collection from Human Skeletal Remains: Proceedings of a Seminar at the Field Museum of Natural History; Research Series, 1; Arkansas Archeological Survey: Fayetteville, AR, USA, 1994. [Google Scholar]
- Lovejoy, C.O.; Meindl, R.S.; Pryzbeck, T.R.; Mensforth, R.P. Chronological metamorphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. Am. J. Phys. Anthropol. 1985, 68, 15–28. [Google Scholar] [CrossRef]
- White, T.; Folkens, P. The Human Bone Manual, 1st ed.; Academic Press Elsevier: Amsterdam, The Nedherlands, 2005; pp. 127–152. [Google Scholar]
- Sjøvold, T. Estimation of stature from long bones utilizing the line of organic correlation. Hum. Evol. 1990, 5, 431–447. [Google Scholar] [CrossRef]
- Gurler, G.; Delilbasi, C.; Delilbasi, E. Investigation of impacted supernumerary teeth: A cone beam computed tomograph (cbct) study. J. Istanb. Univ. Fac. Dent. 2017, 51, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Katheria, B.C.; Kau, C.H.; Tate, R.; Chen, J.W.; English, J.; Bouquot, J. Effectiveness of impacted and supernumerary tooth diagnosis from traditional radiography versus cone beam computed tomography. Pediatr. Dent. 2010, 32, 304–309. [Google Scholar]
- Nardi, C.; Vignoli, C.; Pietragalla, M.; Tonelli, P.; Calistri, L.; Franchi, L.; Preda, L.; Colagrande, S. Imaging of mandibular fractures: A pictorial review. Insights Imaging 2020, 11, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, G.; Harris, E.F.; Lesot, H.; Clauss, F.; Brook, A. Morphogenetic fields within the human dentition: A new, clinically relevant synthesis of an old concept. Arch. Oral Biol. 2009, 54 (Suppl. 1), 34–44. [Google Scholar] [CrossRef]
- Al-Ani, A.H.; Antoun, J.S.; Thomson, W.M.; Merriman, T.R.; Farella, M. Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. BioMed Res. Int. 2017, 2017, 9378325. [Google Scholar] [CrossRef] [PubMed]
- Gomes, R.R.; Da Fonseca, J.A.C.; Paula, L.M.; Faber, J.; Acevedo, A.C. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur. J. Orthod. 2010, 32, 302–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fekonja, A. Hypodontia in orthodontically treated children. Eur. J. Orthod. 2005, 27, 457–460. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, P.T. Homeobox genes and orofacial development. Connect. Tissue Res. 1995, 32, 17–25. [Google Scholar] [CrossRef]
- Mitsiadis, T.A.; Smith, M.M. How do genes make teeth to order through development? J. Exp. Zool. B Mol. Dev. Evol. 2006, 306, 177–182. [Google Scholar] [CrossRef]
- Townsend, G.C.; Bockmann, M.; Hughes, T.; Brook, A. Genetic, Epigenetic and Environmental Influences on Human Tooth Number, Size and Shape. Odontology 2012, 100, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vastardis, H. The genetics of human tooth agenesis: New discoveries for understanding dental anomalies. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 650–656. [Google Scholar] [CrossRef]
- Ercal, P.; Taysi, A.E. Third molar agenesis: Prevalence and Association with agenesis of other teeth in a Turkish population. Niger. J. Clin. Pract. 2020, 23, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Reshitaj, A.; Krasniqi, D.; Reshitaj, K.; Milosevic, S.A. Hypodontia, gender-based differences and its correlation with other dental clinical features in kosovar adolescents. Acta Stomatol. Croat. 2019, 53, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Mattheeuws, N.; Dermaut, L.; Martens, G. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur. J. Orthod. 2004, 26, 99–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heuck Henriksson, C.; Andersson, M.E.M.; Møystad, A. Hypodontia and retention of third molars in Norwegian medieval skeletons: Dental radiography in osteoarchaeology. Acta Odontol. Scand. 2019, 77, 310–314. [Google Scholar] [CrossRef]
- Forshaw, R. The Two Brothers: An enlightening study of ancient Egyptian teeth. Br. Dent. J. 2019, 226, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Benazzi, S.; Buti, L.; Franzo, L.; Kullmer, O.; Winzen, O.; Gruppioni, G. Report of three fused primary human teeth in an archaeological material. Int. J. Osteoarchaeol. 2010, 20, 481–485. [Google Scholar] [CrossRef]
- Ripamonti, U.; Petit, J.C.; Thackeray, J.F. A supernumerary tooth in a 1.7 million-year-old Australopithecus robustus from Swartkrans, South Africa. Eur. J. Oral Sci. 1999, 107, 317–321. [Google Scholar] [CrossRef]
- Ceperuelo, D.; Lozano, M.; Duran-Sindreu, F.; Mercadé, M. Supernumerary fourth molar and dental pathologies in a Chalcolithic individual from the El Mirador Cave site (Sierra de Atapuerca, Burgos, Spain). HOMO 2015, 66, 15–26. [Google Scholar] [CrossRef]
- Villotte, S.; Ogden, A.R.; Trinkaus, E. Dental abnormalities and oral pathology of the pataud 1 upper paleolithic human. Bull. Mem. Soc. Anthropol. Paris 2018, 30, 153–161. [Google Scholar] [CrossRef]
- Villa, C.; Davey, J.; Craig, P.J.G.; Drummer, O.H.; Lynnerup, N. The advantage of CT scans and 3D visualizations in the analysis of three child mummies from the Graeco-Roman Period. Anthropol. Anz. 2015, 72, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Sacks, L. Multiple supernumerary teeth in a likely syndromic individual from prehistoric Illinois. Arch. Oral Biol. 2018, 93, 100–106. [Google Scholar] [CrossRef]
- De Vos, W.; Casselman, J.; Swennen, G.R. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: A systematic review of the literature. Int. J. Oral Maxillofac. Surg. 2009, 38, 609–625. [Google Scholar] [CrossRef]
- Nematolahi, H.; Abadi, H.; Mohammadzade, Z.; Soofiani Ghadim, M. The Use of Cone Beam Computed Tomography (CBCT) to Determine Supernumerary and Impacted Teeth Position in Pediatric Patients: A Case Report. J. Dent. Res. Dent. Clin. Dent. Prospect. 2013, 7, 47–50. [Google Scholar] [CrossRef]
- Rossi, M.; Casali, F.; Chirco, P.; Morigi, M.P.; Nava, E.; Querzola, E.; Zanarini, M. X-ray 3D Computed Tomography of Bronze Archaeological Samples. IEEE Trans. Nucl. Sci. 1999, 46, 897–903. [Google Scholar] [CrossRef]
- Morigi, M.P.; Casali, F.; Bettuzzi, M.; Bianconi, D.; Brancaccio, R.; Cornacchia, S.; Pasini, A.; Rosi, A.; Aldrovandi, A.; Cauzzi, D. CT investigation of two paintings on wood tables by Gentile da Fabriano. Nucl. Instrum. Methods Phys. Res. A 2007, 580, 735–738. [Google Scholar] [CrossRef]
- Du, C.; Zhu, Y.; Hong, L. Age-related changes in pulp cavity of incisors as a determinant for forensic age identification. J. Forensic. Sci. 2011, 56, S72–S76. [Google Scholar] [CrossRef]
- De Angelis, D.; Gibelli, D.; Gaudio, D.; Cipriani Noce, F.; Guercini, N.; Varvara, G.; Sguazza, E.; Sforza, C.; Cattaneo, C. Sexual dimorphism of canine volume: A pilot study. Leg. Med. (Tokyo) 2015, 17, 163–166. [Google Scholar] [CrossRef]
- Demiralp, K.Ö.; Bayrak, S.; Orhan, M.; Alan, A.; Kurşun Çakmak, E.Ş.; Orhan, K. Anatomical characteristics of the lingual foramen in ancient skulls: A cone beam computed tomography study in an Anatolian population. Folia Morphol. 2018, 77, 514–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Przystańska, A.; Lorkiewicz-Muszyńska, D.; Abreu-Głowacka, M.; Glapiński, M.; Sroka, A.; Rewekant, A.; Hyrchała, A.; Bartecki, B.; Żaba, C.; Kulczyk, T. Analysis of human dentition from Early Bronze Age: 4000-year-old puzzle. Odontology 2017, 105, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Izzetti, R.; Gaeta, R.; Caramella, D.; Giuffra, V. Cone-Beam Computed Tomography vs. Multi-Slice Computed Tomography in paleoiaging: Where we stand. HOMO 2020, 71, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Kendall, R.; Kendall, E.J.; Macleod, I.; Gowland, R.; Beaumont, J. An unusual exostotic lesion of the maxillary sinus from Roman Lincoln. Int. J. Paleopathol. 2015, 11, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, E.J.; Lee, W.-J.; Hu, K.-S.; Hwang, J.J. Paleopathological Study of Dwarfism-Related Skeletal Dysplasia in a Late Joseon Dynasty (South Korean) Population. PLoS ONE 2015, 10, e0140901. [Google Scholar] [CrossRef]
- Giuffra, V.; Minozzi, S.; Riccomi, G.; Naccarato, A.G.; Castagna, M.; Lencioni, R.; Chericoni, S.; Mongelli, V.; Felici, C. Multiple osteomata from medieval Tuscany, Italy (ca. 10th–12th AD). Int. J. Paleopathol. 2019, 25, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Gaeta, R.; Fornaciari, A.; Izzetti, R.; Caramella, D.; Giuffra, V. Severe atherosclerosis in the natural mummy of Girolamo Macchi (1648–1734), “major writer” of Santa Maria della Scala Hospital in Siena (Italy). Atherosclerosis 2018, 280, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Carlson, D.S.; Van Gerven, D.P. Masticatory function and post-Pleistocene evolution in Nubia. Am. J. Phys. Anthropol. 1977, 46, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Papagrigorakis, M.J.; Synodinos, P.N.; Baziotopoulou-Valavani, E. Dental status and orthodontic treatment needs of an 11-year-old female resident of Athens, 430 BC. Angle Orthod. 2008, 78, 152–156. [Google Scholar] [CrossRef] [Green Version]
- Alrousan, M.; Estebaranz-Sánchez, F.; Al-Shorman, A.; Martínez, L.M.; Gharaibeh, N.; Otum, K.; Pérez-Pérez, A. Buccal dental microwear as an indicator of dietary habits and dietary adaptation of the Byzantine people of Jordan. Anthropol. Anz. 2019, 76, 352–362. [Google Scholar] [CrossRef]
- Sperduti, A.; Giuliani, M.R.; Guida, G.; Petrone, P.P.; Rossi, P.F.; Vaccaro, S.; Frayer, D.W.; Bondioli, L. Tooth grooves, occlusal striations, dental calculus, and evidence for fiber processing in an Italian eneolithic/bronze age cemetery. Am. J. Phys. Anthropol. 2018, 167, 234–243. [Google Scholar] [CrossRef]
- Tomczyk, J.; Zalewska, M. Mechanical and chemical dental wear in historical population from the Syrian lower Euphrates valley. Arch. Oral Biol. 2016, 62, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Fuss, J.; Uhlig, G.; Böhme, M. Earliest evidence of caries lesion in hominids reveal sugar-rich diet for a middle miocene dryopithecine from Europe. PLoS ONE 2018, 13, e0203307. [Google Scholar] [CrossRef] [PubMed]
- Lacy, S.A. The oral pathological conditions of the Broken Hill (Kabwe) 1 cranium. Int. J. Paleopathol. 2014, 7, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Munoz, O. Transition to agriculture in South-Eastern Arabia: Insights from oral conditions. Am. J. Phys. Anthropol. 2017, 164, 702–719. [Google Scholar] [CrossRef] [PubMed]
- Sutton, P.R. Tooth eruption and migration theories: Can they account for the presence of a 13,000-year-old mesiodens in the vault of the palate? Oral Surg. Oral Med. Oral Pathol. 1985, 59, 252–255. [Google Scholar] [CrossRef]
- Ives, R. An unusual double supernumerary maxillary mesiodens in a Middle Iron Age skeleton from South Uist, Western Isles, Scotland. Arch. Oral Biol. 2014, 59, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Hurlen, B.; Humerfelt, D. Hyperdontia in 14th-18th century Norwegian populations: A radiographic study on skulls. Dentomaxillofac. Radiol. 1984, 13, 135–139. [Google Scholar] [CrossRef]
- Stermer Beyer-Olsen, E.M. Premaxillary hyperdontia in medieval Norwegians: A radiographic study. Dentomaxillofac. Radiol. 1989, 18, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Aoun, G.; Nasseh, I. Mesiodens within the Nasopalatine Canal: An Exceptional Entity. Clin. Pract. 2016, 6, 903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalakkal, P.; Krishnan, R.; De Souza, N.; Da Costa, G.C. A rare occurrence of supplementary maxillary lateral incisors and a detailed review on supernumerary teeth. J. Oral Maxillofac. Pathol. 2018, 22, 149. [Google Scholar] [CrossRef]
- Brook, A.H.; O’Donnell, M.B.; Hone, A.; Hart, E.; Hughes, T.E.; Smith, R.N.; Townsend, G.C. General and craniofacial development are complex adaptive processes influenced by diversity. Aust. Dent. J. 2014, 59 (Suppl. 1), 13–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, P.R.; Lopes, M.C.; Martins-Filho, I.E.; Haye Biazevic, M.G.; Michel-Crosato, E. Tooth crown mesiodistal measurements for the determination of sexual dimorphism across a range of populations: A systematic review and meta-analysis. J. Forensic Odontostomatol. 2019, 37, 2–19. [Google Scholar] [PubMed]
- Khalaf, K.; Robinson, D.L.; Elcock, C.; Smith, R.N.; Brook, A.H. Tooth size in patients with supernumerary teeth and a control group measured by image analysis system. Arch. Oral Biol. 2005, 50, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, K.; Smith, R.N.; Elcock, C.; Brook, A.H. Multiple crown size variables of the upper incisors in patients with supernumerary teeth compared with controls. Arch. Oral Biol. 2009, 54 (Suppl. 1), 71–78. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth | Presence | Development | Wear | Caries | Abscess | Calculus | Hypoplasia |
|---|---|---|---|---|---|---|---|
| UR8 | Unobservable, region damaged | - | - | - | - | - | - |
| UR7 | Unobservable, region damaged | - | - | - | - | - | - |
| UR6 | Unobservable, region damaged | - | - | - | - | - | - |
| UR5 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| UR4 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| UR3 | Present | complete | 4 | 0 | 0 | 2 | 0 |
| UR2 | Missing, lost post-mortem | - | - | - | - | - | - |
| UR1 | Missing, lost post-mortem | - | - | - | - | - | - |
| Mesiodens | Present | complete | 4 | 0 | 0 | 1 | 0 |
| UL1 | Present | complete | 4 | 0 | 0 | 1 | 0 |
| UL2 | Missing, lost post-mortem | - | - | - | - | - | - |
| UL3 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| UL4 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| UL5 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| UL6 | Present | complete | 4 | 0 | 0 | 2 | 0 |
| UL7 | Unobservable, region damaged | - | - | - | - | - | - |
| UL8 | Unobservable, region damaged | - | - | - | - | - | - |
| LL8 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LL7 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LL6 | Present | complete | 4 | 0 | 0 | 2 | 0 |
| LL5 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LL4 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LL3 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LL2 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LL1 | Missing, lost post-mortem | - | - | - | - | - | - |
| LR1 | Missing, lost post-mortem | - | - | - | - | - | - |
| LR2 | Missing, lost post-mortem | - | - | - | - | - | - |
| LR3 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LR4 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LR5 | Present | complete | 3 | 0 | 0 | 2 | 0 |
| LR6 | Present | complete | 4 | 0 | 0 | 2 | 0 |
| LR7 | Present | complete | 4 | 0 | 0 | 2 | 0 |
| LR8 | Unobservable, region damaged | - | - | - | - | - | - |
| Tooth | Mesio–Distal Diameter (mm) |
|---|---|
| UL1 | 9.13 |
| UL3 | 7.82 |
| UR3 | 7.96 |
| LL3 | 7.18 |
| LR3 | 7.11 |
| Dimension | mm |
|---|---|
| Mesio–distal diameter | 5.05 |
| Maximal crown length (from CEJ to incisal margin) | 8.99 |
| Subject Gender | UR3 | LR3 | |
|---|---|---|---|
| “Individual 1” | M | 7.96 | 7.11 |
| Greeks | M | 8.04 | 7.17 |
| F | 7.74 | 6.83 | |
| Turks | M | 7.89 | 6.95 |
| F | 7.49 | 6.58 | |
| Indians | M | 7.84 | 6.84 |
| F | 7.51 | 6.47 | |
| Subject | U1 | U3 | L3 |
|---|---|---|---|
| “Individual 1” | 9.13 | 7.96 | 7.11 |
| Controls with supernumeraries | 9.05 | 8.01 | 7.06 |
| Controls without supernumeraries | 8.68 | 7.84 | 6.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beschiu, L.M.; Craiovan, B.A.; Popa, S.; Micle, D.; Ardelean, L.C.; Rusu, L.C. An Ancient Mesiodens Investigated by Cone Beam CT. Appl. Sci. 2021, 11, 11703. https://doi.org/10.3390/app112411703
Beschiu LM, Craiovan BA, Popa S, Micle D, Ardelean LC, Rusu LC. An Ancient Mesiodens Investigated by Cone Beam CT. Applied Sciences. 2021; 11(24):11703. https://doi.org/10.3390/app112411703
Chicago/Turabian StyleBeschiu, Laura Maria, Bogdan Alin Craiovan, Stefan Popa, Dorel Micle, Lavinia Cosmina Ardelean, and Laura Cristina Rusu. 2021. "An Ancient Mesiodens Investigated by Cone Beam CT" Applied Sciences 11, no. 24: 11703. https://doi.org/10.3390/app112411703
APA StyleBeschiu, L. M., Craiovan, B. A., Popa, S., Micle, D., Ardelean, L. C., & Rusu, L. C. (2021). An Ancient Mesiodens Investigated by Cone Beam CT. Applied Sciences, 11(24), 11703. https://doi.org/10.3390/app112411703