1. Introduction
In recent years, special attention has been given to the development of mechatronic rehabilitation systems, which can provide high intensity and frequency of treatment for improved motor recovery [
1], particularly when used in a tele-rehabilitation framework. For lower limb rehabilitation, robotic systems are now commercially available as an alternative to conventional therapy, and technological complement to Body-Weight Supported Treadmill Training (BWSTT) [
2,
3].
Generally, robot-assisted lower limb therapy consists of the simulation of joint or foot path, such as gait trajectories produced by non-impaired people. The resulting movement may possibly integrate other technologies, such as Functional Electrical Stimulation [
4], or additional levels of control, such as the ability to assist-as-needed [
5,
6]. Mechanical support is often delivered to the patient using either an exoskeletal device [
2], or an end-effector-based robot [
3,
5]. While exoskeleton-based systems may lessen the strain on therapists, studies suggest that patient engagement on therapy may also be reduced [
7], which may indicate that the neurological pathways required for rehabilitation are not properly stimulated. In view of this issue, recent research has proposed new treadmill control schemes [
8], as well as structurally innovative treadmills [
9]. Nevertheless, in this work, we focus on end-effector systems.
End-effector-based lower limb rehabilitation systems represent an alternative to these approaches. Some of those systems were designed for BWSTT [
3,
5], while others have targeted ankle rehabilitation only [
10,
11]. To the best of our knowledge, none of these systems provide BWSTT capability and independent six degree-of-freedom (DOF) movement of each foot. A system combining such features may not only be used for gait training, but also in balance assessment and exercises, an area that has also seen development of specific methods [
12] and devices [
13].
This study utilizes a gait simulator system based on two Stewart–Gough platforms used for lower limb rehabilitation. A thorough description of its mechanical design and implementation is reported in [
14]. We propose in this paper novel control strategies that provide the system with additional tele-rehabilitation capabilities.
In terms of control strategies, force control is often used in robot-aided rehabilitation and, more generally, in human–robot interaction. Despite the advantages of approaches based on force control, challenges exist, particularly in a tele-rehabilitation scenario [
15], to apply these methods in our SGP-based system. Hence, the original version of the gait simulator employed position control, simply emulating standard gait trajectories, which remained fixed for the duration of the rehabilitation session. In order to improve overall safety (especially for use in tele-rehabilitation), provide a more intuitive therapist interface, and enable more active patient engagement, two main techniques are proposed in this paper.
Firstly, we propose a robot walking velocity modulation based on patient motion (Self-Modulation Mode, SMM), which is similar to the idea proposed in [
13]. However, instead of using a mechanical structure attached to the upper limb, we have used wearable sensors on the trunk, and velocity is updated based on the patient’s posture. Secondly, the platforms may also be directly controlled using the therapist’s mirrored motion (Therapist Modulation Mode, TMM). In our work, we have applied a similar approach as in [
16], i.e., by using an intuitive interface based on wearable sensors, the therapist may control the slave robotic system intuitively and possibly from a remote location.
Indeed, both control strategies proposed in this work may be further expanded by the use of tele-rehabilitation, in which the therapist is located remotely [
17]. Within a session employing TMM, the therapist may control the system motion using his own body movement, while monitoring patient response. When the system is operated using the SMM, the therapist may remotely assess patient movement based on video and data from the wearable sensors, particularly if methods for automatic quantitative assessment are used [
18,
19]. In order to validate the tele-rehabilitation component of this system, series of simulated experiments were conducted to verify the feasibility of our technical solution.
This paper is organized as follows.
Section 2 presents the gait simulator, including details on its mechanical design, low-level control, and additional development required to implement new operation modes, as well as the proposed control strategies, SMM and TMM. The method employed to validate the tele-rehabilitation component is also described in this Section. Experimental evaluation is presented in
Section 3, including data from tests to validate each subsystem separately and preliminary experiments designed to evaluate the feasibility of the overall system when using the novel operation modes. These trials involved healthy subjects. These results are discussed in
Section 4. Finally, we draw conclusions and discuss future works in
Section 5.
2. Materials and Methods
2.1. Gait Simulator
The gait simulator employed in this work is based on the operation of two parallel manipulators capable of performing on-site walking. Its main goal is to induce lower limb movements on a user standing on his/her feet over the platform. As depicted in
Figure 1, the platform is designed to enable independent 6-DOF movement of each foot, thus producing motions ranging from normal walking to arbitrary lower extremity movements, hence potentially contributing for the restoration of motor function in different clinical scenarios.
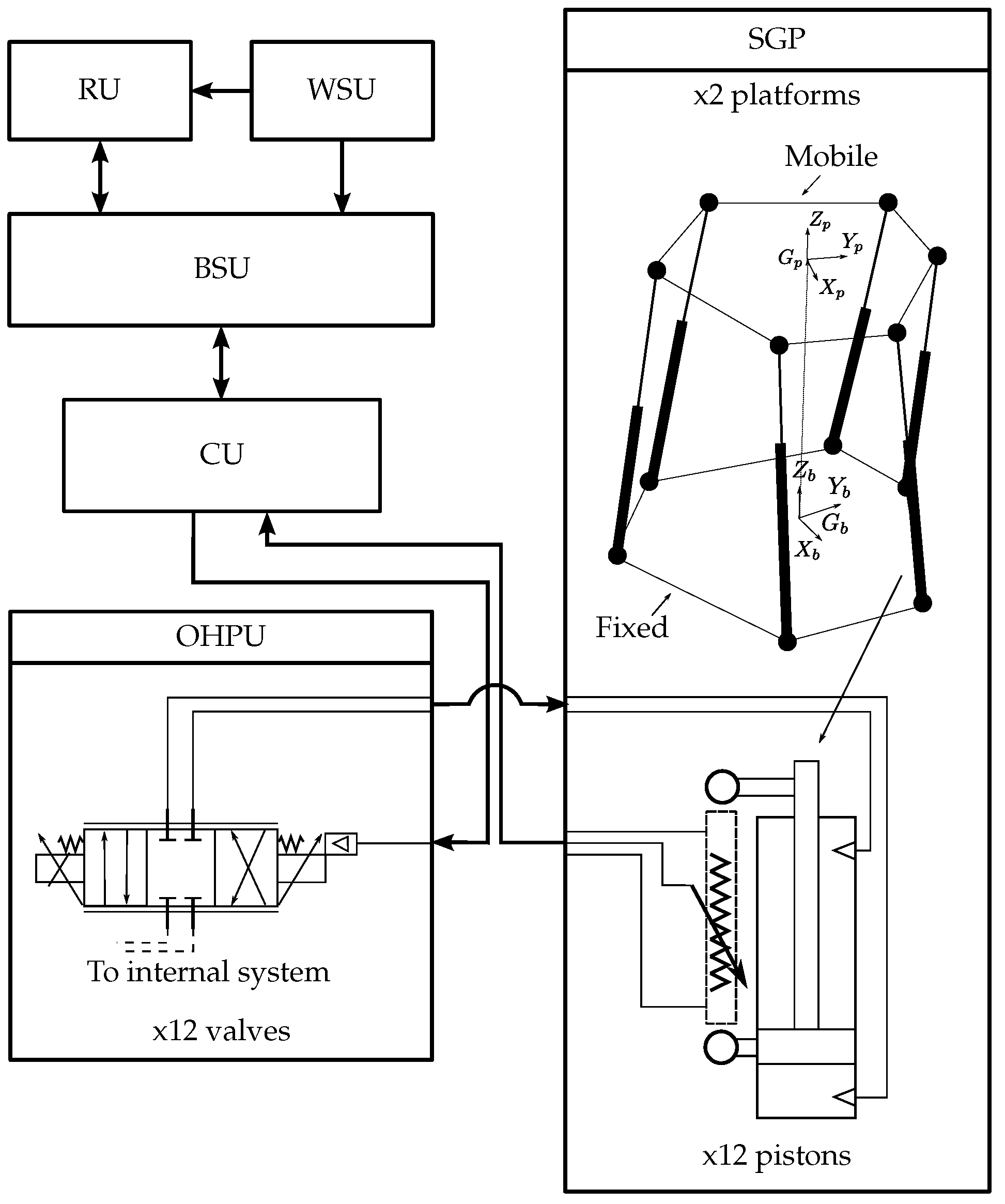
An overview of the gait simulator is illustrated in
Figure 2. It is composed of two Stewart–Gough Platforms (SGP), each comprised of six pistons, whose coordinated displacement moves the upper platform to the desired position. They are connected to the Oil Hydraulic Power Unit (OHPU), which is comprised of valves that regulate oil flow through hosepipes in order to increase or decrease pressure and thus produce piston displacement.
The basic design of the SGP is inspired by kinematic and dynamic features of human walking. Thus, one fundamental condition concerns the platform displacement range on the sagittal plane, which must allow adequate step width. The workspace and the maximum output forces produced by the system are listed in
Table 1. Regarding the actuators, hydraulic actuation composed of 12 pistons (6 for each platform) driven by a 3 kW power OHPU are controlled by proportional electronic valves. A linear potentiometer is attached to each piston to assess the actual displacement.
Regarding the hardware/software architecture, three computational units allow the user (i.e., therapist) to control the gait simulator. First, the Base Station Unit (BSU) is composed of a “local” Personal Computer (PC) with a Graphical User Interface (GUI) application, which serves to set up the platform operation mode, and an internet-based communication software that establishes communication with a “remote” PC or Remote Unit (RU) for tele-rehabilitation purposes. Second, the Wearable Sensing Unit (WSU) is based on wireless inertial sensors (3space, Yost Technology, Ohio, USA) that allow the acquisition of the patient or therapist movement. Third, the microcontroller-based Control Unit (CU) implements a local closed-loop control of piston displacement. Either the BSU or the RU (i.e., local or remote PCs) may be used to acquired movement data from wireless inertial sensors.
In order to evaluate the system tele-rehabilitation capabilities between users in different locations, possibly distinct countries, a specific software was developed. In particular, an internet-based software enables the interconnection between the BSU and a RU using TCP/IP connectivity. Through that connection, a therapist may, for instance, obtain real-time information from ongoing therapy, as well as send direct commands to control the robotic device. In this case, time delays and packet loss involved in internet communication may lead to instability. This issue is particularly important, since communication tests were done between Montpellier, France; Brasilia, Brazil; and the gait simulator located in Lima, Perú.
Each parallel manipulator composing the system, referred to as left
l and right
r, has one fixed base and one mobile platform onto which the user stands. The coordinate systems for the fixed base and the mobile platform are defined as
and
, respectively, as depicted in
Figure 2, and the
origin coincides with the foot median position. From a kinematic control perspective, high-level platform motion commands computed by each of the control strategies proposed in this work must enable computing corresponding piston displacements that will provide an appropriate
trajectory. However, solving the inverse kinematic equations for SGP is complex, due to closed kinematic chain and constrained configuration. In this work, a numerical solution based on unique geometric features of SGP is used. Further details are provided in [
14]. For all control strategies, hard-coded measures to avoid inter-platform collision are implemented by reducing the available operational space.
2.2. Control Strategies
The gait simulator described in
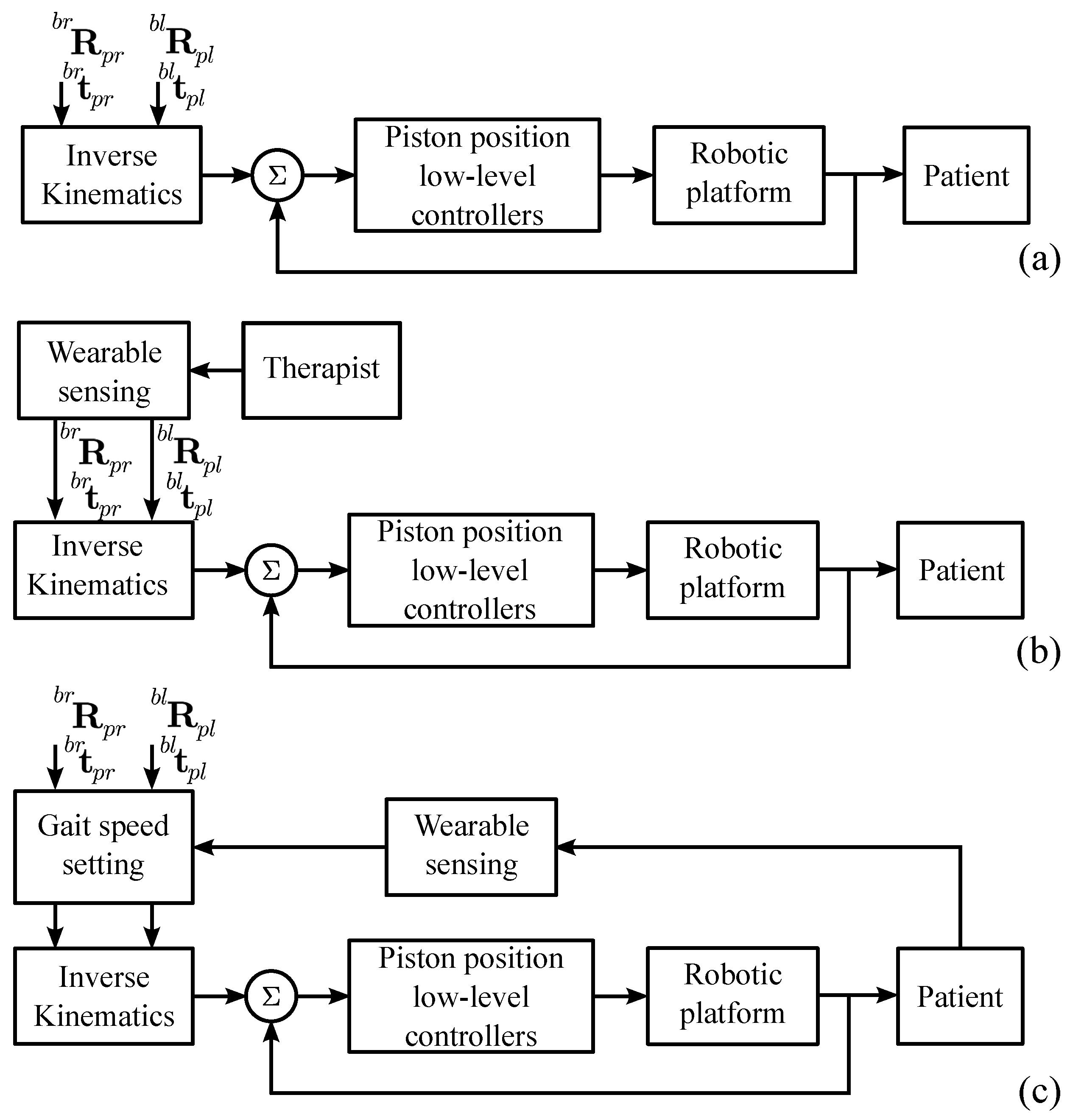
Section 2.1 enables independent 6-DOF movement of each foot. Based on this system, feet trajectories that promote rehabilitation may be created. This basic control strategy is referred to as Fixed Gait Trajectory Mode (FGTM) (
Figure 3a). In this work, novel strategies that enable modulating platform movement in real time are proposed.
Regarding the FGTM, emulating standard gait trajectories may be one of the first approaches applied in lower limb robotic rehabilitation systems [
2]. For that purpose, feet pose during gait was recorded using optic motion capture [
20] to serve as a high-level reference to the CU. The reference trajectory for each foot was measured with respect to the standard double support position. This is the same starting position used in the gait simulator, defined by the rotation matrix
and position
, both known constants in our setup. Note that, in the convention used here, while
represents the position of the coordinate system
in terms of
,
is used to compute rotations from
to
. For each data point measured by the motion capture system, corresponding high-level commands to the robotic system were computed using Equation (
1).
2.2.1. Therapist Modulation Mode (TMM)
An alternative to the FGTM, in which the robotic motion is performed without any online modulation, is to enable therapists to transfer movements in real-time to the gait simulator. In addition to the possibility of creating arbitrary lower extremity motion, the method is particularly useful for tele-rehabilitation.
In order to track the therapist’s feet trajectory, the adopted approach involves the use of sensors, such as wireless inertial sensors, attached to the feet. Other sensing systems may be used, particularly if reliable position tracking is desired. As illustrated in
Figure 3b, based on the measured pose with respect to the initial position provided by such sensors, i.e.,
and
, the same computations described in Equation (
1) may be used to provide high-level commands to the platforms. The main difference with the previous strategy is that those estimates are transferred in real time to the robot.
In tele-rehabilitation, the corresponding time delay may produce instability. This is especially the case when therapy involves fast movements. In order to limit the effects of these potential issues, in addition to optimization of communication software to reduce delay and packet loss and use of low-pass filtering to minimize the effect of high-frequency fluctuations, control gains are reduced. Finally, two additional functionalities are proposed to improve the overall usability of this operation mode. First, the therapist may directly deactivate any DOF or reset his/her initial position at any moment. Moreover, the performed trajectories may be recorded to be used in open-loop, such as in FGTM.
2.2.2. Self-Modulation Mode (SMM)
In order to increase patient engagement during therapy and consequently the overall positive outcome, an additional proposed control strategy involves real-time modulation of robot motion based on patient control. As a first implementation towards more complex scenarios, discussions with clinicians supported the use of trunk inclination to modulate gait trajectory speed.
For that purpose, a wireless inertial sensor is attached to the patient’s upper body. Measurements of upper body angular displacement on the sagittal plane are used to increase or decrease the cadence of gait trajectory employed at the FGTM. Considering an upper-body angle
, we defined a maximum trunk flexion
, which is used to compute the applied gait speed using Equation (
2):
where
g is the gait speed,
is the minimum gait speed (0 km/h in this case, but often 0.8 km/h may be used [
4]), and
is a gain defined by the user. In this work,
is computed considering maximum trunk flexion
(
in this work) leads to the maximum defined gait speed (4.8 km/h in this case).
2.3. Feasibility Study
The experiments were designed to investigate the feasibility of both proposed control strategies in terms of system performance and user subjective perception. In this section, data obtained from an individual with no gait impairments (male, 27 years old, 65 kg) is depicted. In the trial involving a therapist, another individual took part in the test (male, 34 years old, 77 kg).
Within the experiments performed in this work, the sensors were attached either to the user trunk, where it provided upper-body flexion/extension estimates for the SMM, or to the feet, providing plantar flexion/dorsiflexion, eversion/inversion, and external/internal rotation readings for the TMM. For the latter, ideally foot position would also have to be measured and employed for controlling the SGP, but in this work only attitude was evaluated.
Regarding the protocol, the therapist in the TMM trial and the patient in the SMM trial were told to move the orientation of their feet/trunk freely. In the TMM trial, the therapist was positioned behind the patient, as illustrated in the bottom panel of
Figure 4. Although a human subject standing on the platform was not required to evaluate the system performance, we have chosen this configuration to prevent prediction of platform movement by the patient, which would possibly occur in tele-rehabilitation.
Tele-rehabilitation feature is validated by testing interconnection between the BSU (Lima, Peru) and an RU located at Montepellier, France. The BSU and RU have a client and server TCP/IP application, respectively, which allow sending commands to the SGP and requesting data from wireless inertial sensors. Public IPs are assigned to both BSU and RU computers. An initial testing using the “ping” command is conducted to assess the typical delay transmitting and receiving data packets during the experiment. No virtual private network nor dedicated internet connection is used in this experiment. Once the sanity check is done, a TCP/IP port is open in both computers to establish communication. Command transfer and SGP data queries were conducted between 5:00 to 7:00 p.m., Montpellier local time, to evaluate the performance requirements during peak hours.
After the experiments, the simulated participant filled a questionnaire to evaluate his experience. Since no standard instrument to evaluate the usability of such a type of system was found, a customized form composed of open questions was applied.
3. Results
Within the feasibility study described in
Section 2.3, series of trials were conducted to explore the system performance, particularly with respect to overall system behavior, and both participants’ perceptions as patient and therapist. The ability to be applied in tele-rehabilitation settings was also evaluated.
In
Figure 4, the results from the TMM trial are depicted. The data in the first and second row correspond to the right foot orientation and the displacement reference given to the six pistons of the right platform, respectively. Furthermore, the figures in the third row refer to two particular moments when the therapist is performing dorsiflexion (left picture) or plantar flexion (right picture).
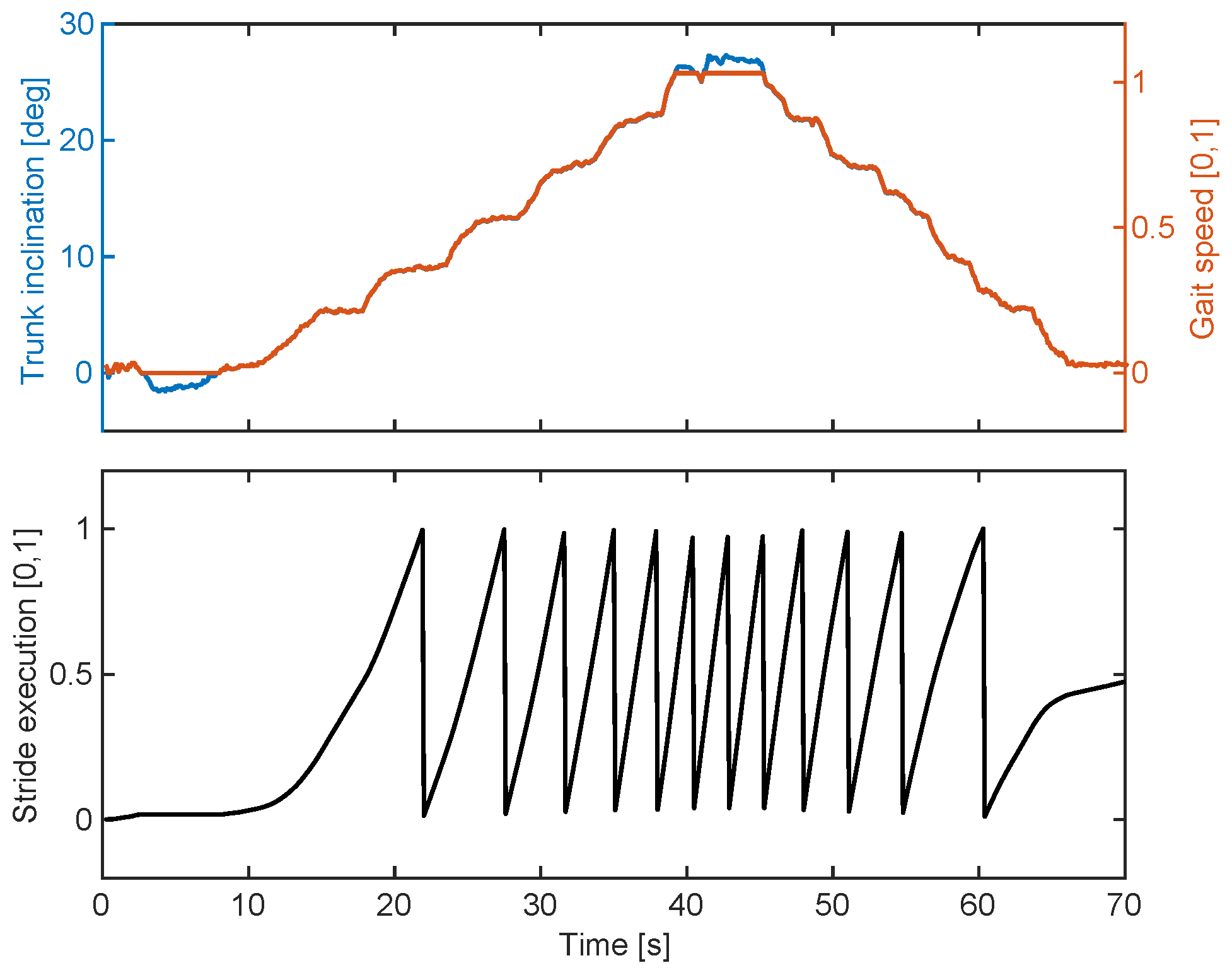
In
Figure 5, sample results from the SMM trial are depicted. In this trial, the user has increased his trunk inclination until reaching maximum gait speed, and then reduced back until no robot movement was produced. We can observe that the trunk inclination is directly translated into the normalized gait speed (top), and also how this modulation affects the normalized stride duration (bottom).
Regarding tele-rehabilitation validation, inter-connectivity between BSU and RU through internet was tested used the ping command. The mean time to transmit and receive a TCP/IP package (56 data bytes) between RU and BSU (Lima–Montpellier) is ≈206 milliseconds.
4. Discussion
To the best of the authors’ knowledge, this paper presents a first attempt to implement control strategies such as SMM and TMM in an SGP-based lower limb robot for tele-rehabilitation. Nevertheless, while the proof-of-concept experiments helped us to evaluate the overall usability of the system, some of its potential limitations became evident.
Within the SMM trial, the user needed to maintain his balance, while simultaneously changing his trunk inclination to modulate gait speed. Despite the supplementary action required in this case, user acceptance was immediate, and no specific concerns were raised. The provided control interface was sufficiently intuitive for the user to control gait speed, as illustrated in
Figure 5.
Nonetheless, it may be also noted that other movement intention sources could be used to modulate gait speed, such as myoelectric activity of lower limb muscles, upper limb oscillatory movement, and others. While each of those measures feature specific drawbacks, the strategy employed in this work (i.e., trunk inclination) also present disadvantages. For instance, momentary loss of balance could be wrongly interpreted as intention to accelerate or decelerate. While additional signal processing may assist in extracting the volitional movement, we believe further clinical study is required to validate this hypothesis. Furthermore, sensor location in this configuration may be less practical if a harness for body weight support is used. In this case, an alternative is to place the sensor on the neck or another body part.
Regarding the TMM trial, the participant that took the role of the patient mentioned that being unaware of future robot movements produced a degree of anxiety. Since we consider it is an undesirable effect in rehabilitation, strategies must be designed to prevent it. One alternative involves a common practice in physiotherapy: verbally explaining each movement before execution.
One of the potential limiting features when using TMM is that there may be the need to scale therapist movements for a patient of different body dimensions. Nevertheless, particularly considering that the system operates at a limited speed, one finding from these preliminary tests is that the therapist adapts their movement based on the observed patient movement, i.e., avoiding the requirement of additional technical solutions. Indeed, this particular adaptation is commonly observed in human–robot interaction [
21,
22].
The lack of feedback to the therapist of interaction forces involved may be one additional limitation of the proposed framework when using TMM. Indeed, different modalities exist to provide this real-time information to the therapist [
23]. While we recognize this issue may limit the range of interventions that may be applied, we also understand visual (and kinematic) feedback alone are sufficient to enable different therapeutic interventions using such a mechatronic system.
The use of position control on both control strategies, instead of techniques based on force control, features additional implications. For instance, strategies based on force control would enable a higher degree of adaptability depending on the interaction forces between the user and the platform. Nevertheless, when comparing to exoskeleton-based systems, an end-effector system using position control would be safer to exoskeletons using a similar approach, particularly in cases of spasticity, for instance.
Certainly, testing of the tele-rehabilitation feature requires a higher number of experiments from different locations. Intercontinental connection implies that only one country is within the peak hours. Further assessment should be done with an RU located in similar geographical longitude as it might reveal additional issues regarding package loss and delay due to a higher concentration of network users. Moreover, we understand future works should be conducted to investigate the stability of such tele-rehabilitation system.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}