
Endoscopy at Bedside in Isolated Patients with Severe COVID-19: Our Approach during the Pandemic

 , , ,
, , ,
Abstract
:1. Introduction
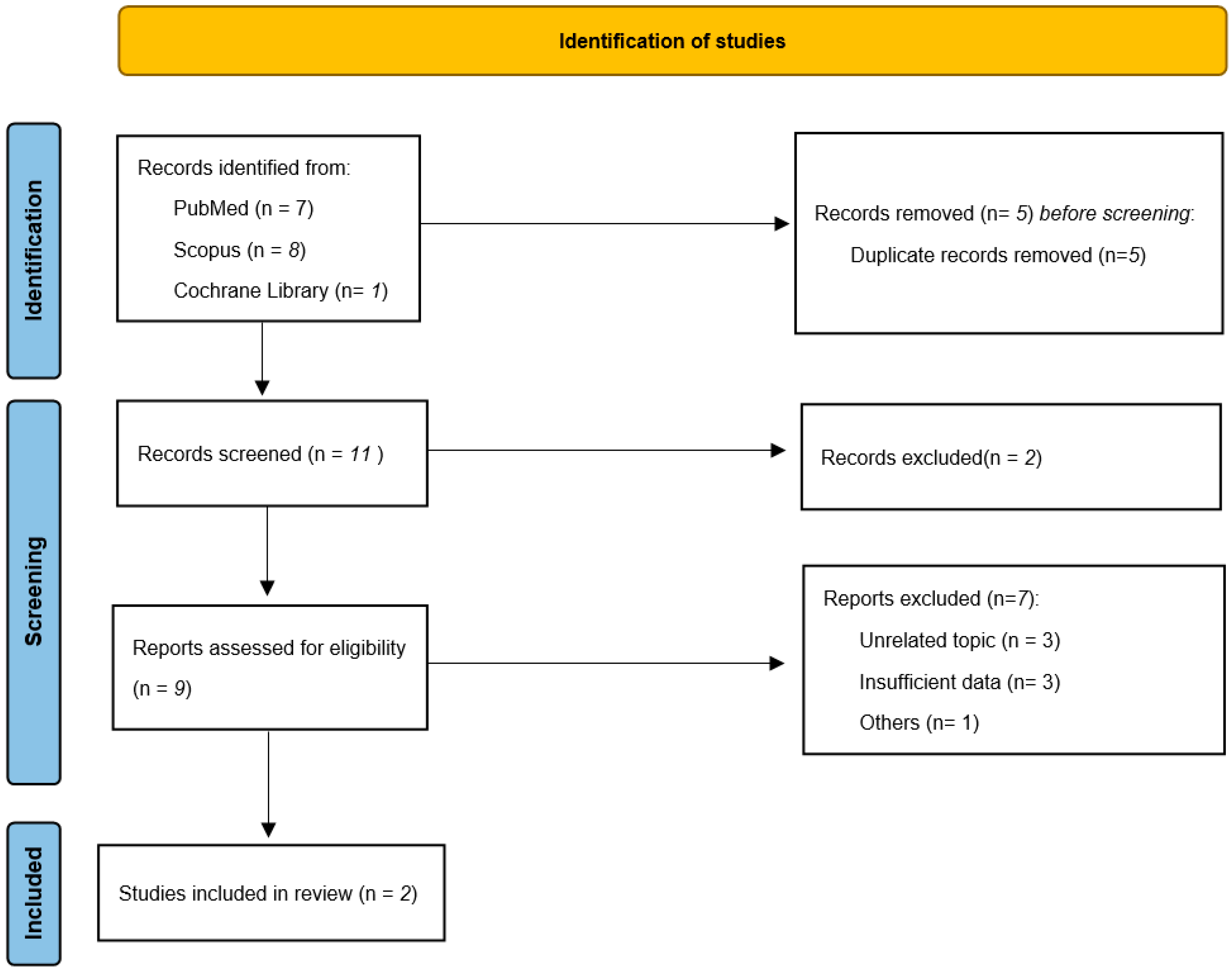
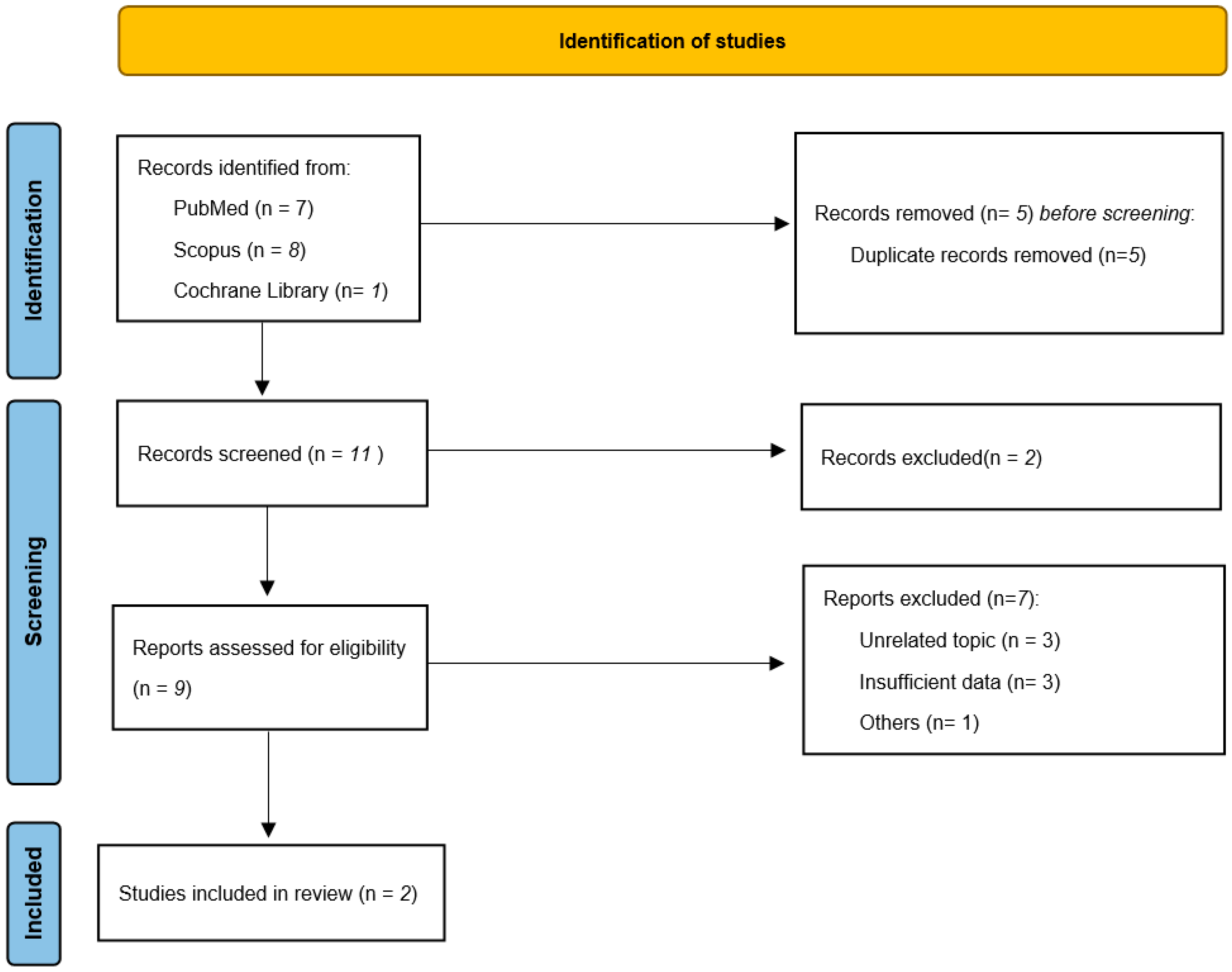
2. Research in Context
3. Our Experience
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hunt, R.H.; East, J.E.; Lanas, A.; Malfertheiner, P.; Satsangi, J.; Scarpignato, C.; Webb, G.J. COVID-19 and Gastrointestinal Disease: Implications for the Gastroenterologist. Dig. Dis. 2021, 39, 119–139. [Google Scholar] [CrossRef] [PubMed]
- Maida, M. Screening of gastrointestinal cancers during COVID-19: A new emergency. Lancet Oncol. 2020, 21, e338. [Google Scholar] [CrossRef]
- Aparicio, T.; Layese, R.; Hemery, F.; Tournigand, C.; Paillaud, E.; De Angelis, N.; Quero, L.; Ganne, N.; Prat, F.; Pachev, A.; et al. Effect of lockdown on digestive system cancer care among older patients during the first wave of COVID-19: The cadigcovage multicentre cohort study. Dig. Liver Dis. 2021. [Google Scholar] [CrossRef]
- Zhang, S.; Wu, X.; Feng, Y.; Wang, Q.; Jiang, Q.; Guo, T.; Wu, D.; Xu, T.; Li, R.; Yang, A. GI endoscopy infection control strategy after COVID-19 peak: Changing strategy for a changing epidemic. Gastrointest. Endosc. 2021, 93, 530–532.e1. [Google Scholar] [CrossRef] [PubMed]
- Petrocelli, G.; Dioscoridi, L.; Forti, E.; Pugliese, F.; Cintolo, M.; Bonato, G.; Rosa, R.; Mutignani, M. The first “exclusive COVID-19” endoscopy project. Endoscopy 2021, 53, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Somerville, C.C.; Shoaib, M.; Kuschner, C.E.; Brune, Z.; Trindade, A.J.; Benias, P.C.; Becker, L.B. Prospective analysis of SARS-CoV-2 dissemination to environmental surfaces during endoscopic procedures. Endosc. Int. Open 2021, 9, E701–E705. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.-D.; Wang, Z.-Y.; Zhang, S.-F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.B.; Dong, Y.-Z.; Chi, X.-Y.; et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg. Infect. Dis. J. 2020, 26, 1583. [Google Scholar]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Wang, H.-F.; Fang, Y.; Lu, Y.; Shen, Z.; Wang, Y.; Wu, X.; Cen, L.; Chen, Y.-S. Analysis of an improved workflow of endoscope reprocessing for bedside endoscopic diagnosis and treatment on COVID-19 patients. J. Zhejiang Univ. Sci. B 2020, 21, 416–422. [Google Scholar] [CrossRef]
- Tian, Q.; Yan, X.; Shi, R.; Wang, G.; Xu, X.; Wang, H.; Wang, Q.; Yang, L.; Liu, Z.; Wang, L.; et al. Endoscopic mask innovation and protective measures changes during the coronavirus disease-2019 pandemic: Experience from a Chinese hepato-biliary-pancreatic unit. Dig. Endosc. 2020, 32, 1105–1110. [Google Scholar] [CrossRef]
- Lisotti, A.; Bacchilega, I.; Linguerri, R.; Fusaroli, P. Endoscopic ultrasound-guided gallbladder drainage as a strategy to overcome shortage of operating rooms and intensive care unit beds during COVID-19 crisis. Endoscopy 2020, 52, E263–E264. [Google Scholar] [CrossRef] [PubMed]
- Franzini, T.A.P.; Kotinda, A.P.S.T.; Moura, D.; Badana, M.L.V.; De Medeiros, M.S.; Lima, P.G.R.; De Mello, B.F.; Kayano, R.P.; Carmona, M.J.C.; Rocha, M.C.; et al. Approach to endoscopic procedures: A routine protocol from a quaternary university referral center exclusively for coronavirus disease 2019 patients. Clinics 2020, 75, e1989. [Google Scholar] [CrossRef] [PubMed]
- Traina, M.; Amata, M.; Granata, A.; Ligresti, D.; Gaetano, B. The C-Cube: An endoscopic solution in the time of COVID-19. Endoscopy 2020, 52, E351–E352. [Google Scholar] [CrossRef] [PubMed]
- Rerknimitr, R.; Soetikno, R.; Ratanachu-Ek, T.; Tiankanon, K.; Kongkam, P.; Ridtitid, W. Additional measures for bedside endoscope cleaning to prevent contaminated splash during COVID-19 pandemic. Endoscopy 2020, 52, 706–707. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Zhang, Z.; Gao, M.; Zhang, Z.; Lin, Z.; Huang, S.; Ren, J.; Luo, M.; Xu, X.; Chen, G.; et al. Practical experience of endoscope reprocessing and working-platform disinfection in COVID-19 patients: A report from Guangdong China during the pandemic. Gastroenterol. Res. Pract. 2020, 2020, 1–4. [Google Scholar] [CrossRef]

{kind=link}
| Total COVID-19 Patients Requiring Endoscopic Procedures: | 25 | ||||
|---|---|---|---|---|---|
| Sex (M/F) | 21/4 | ||||
| Age (mean + SD) | 53.2 ± 8.87 | ||||
| Deaths (%) | 14 (56%) | ||||
| Endoscopic procedures | Total: 61 | EGDS: 50 (81.96%) | Colon: 7 (11.47%) | ERCP: 3 (4.91%) | EUS: 1 (1.64%) |
| Indications | Bleeding 15 | GI Bleeding 6 | CBD stones 1 | WOPN drainage 1 | |
| TEF 20 | Colitis 1 | Acute biliary pancreatitis 1 | |||
| PEG/PEG-J insertion 10 | Cholangitis 1 | ||||
| GI perforation 2 | |||||
| Feeding tube insertion 3 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granata, A.; Martucci, G.; Rizzo, G.E.M.; Ligresti, D.; Stornello, C.; Panarello, G.; Arcadipane, A.; Traina, M. Endoscopy at Bedside in Isolated Patients with Severe COVID-19: Our Approach during the Pandemic. Appl. Sci. 2021, 11, 9704. https://doi.org/10.3390/app11209704
Granata A, Martucci G, Rizzo GEM, Ligresti D, Stornello C, Panarello G, Arcadipane A, Traina M. Endoscopy at Bedside in Isolated Patients with Severe COVID-19: Our Approach during the Pandemic. Applied Sciences. 2021; 11(20):9704. https://doi.org/10.3390/app11209704
Chicago/Turabian StyleGranata, Antonino, Gennaro Martucci, Giacomo Emanuele Maria Rizzo, Dario Ligresti, Caterina Stornello, Giovanna Panarello, Antonio Arcadipane, and Mario Traina. 2021. "Endoscopy at Bedside in Isolated Patients with Severe COVID-19: Our Approach during the Pandemic" Applied Sciences 11, no. 20: 9704. https://doi.org/10.3390/app11209704
APA StyleGranata, A., Martucci, G., Rizzo, G. E. M., Ligresti, D., Stornello, C., Panarello, G., Arcadipane, A., & Traina, M. (2021). Endoscopy at Bedside in Isolated Patients with Severe COVID-19: Our Approach during the Pandemic. Applied Sciences, 11(20), 9704. https://doi.org/10.3390/app11209704