Computational Fluid Dynamics Study of Superselective Intra-arterial Chemotherapy for Oral Cancer: Flow Simulation of Anticancer Agent in the Linguofacial Trunk


Abstract
1. Introduction
2. Materials and Methods
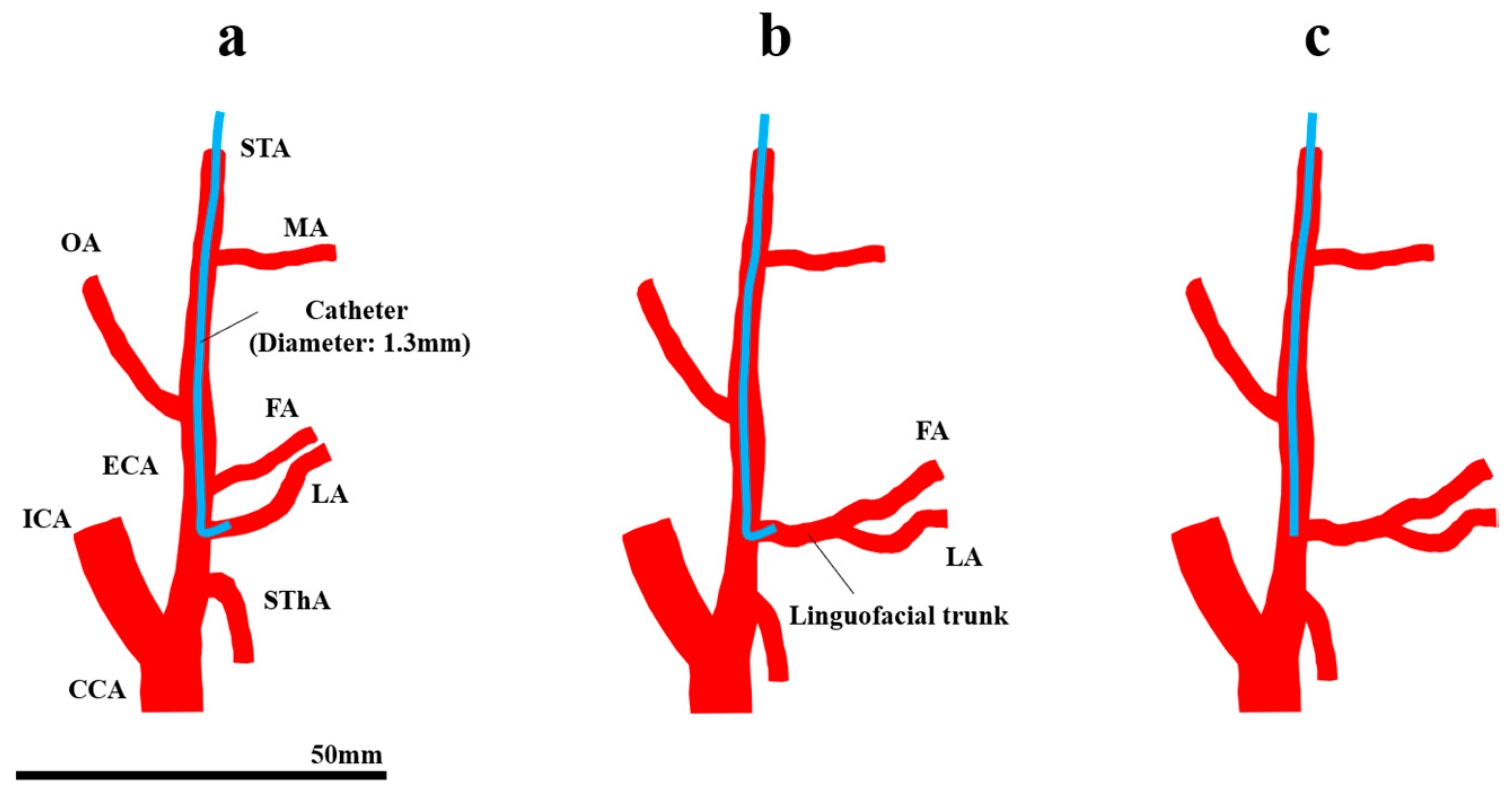
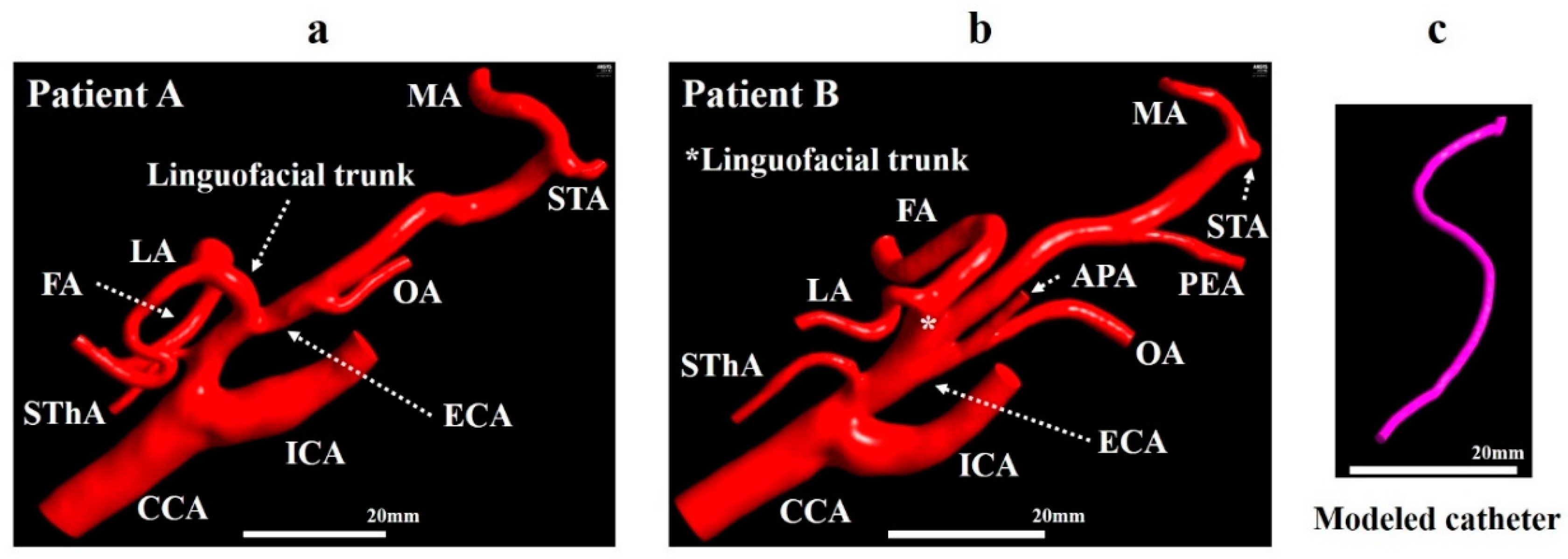
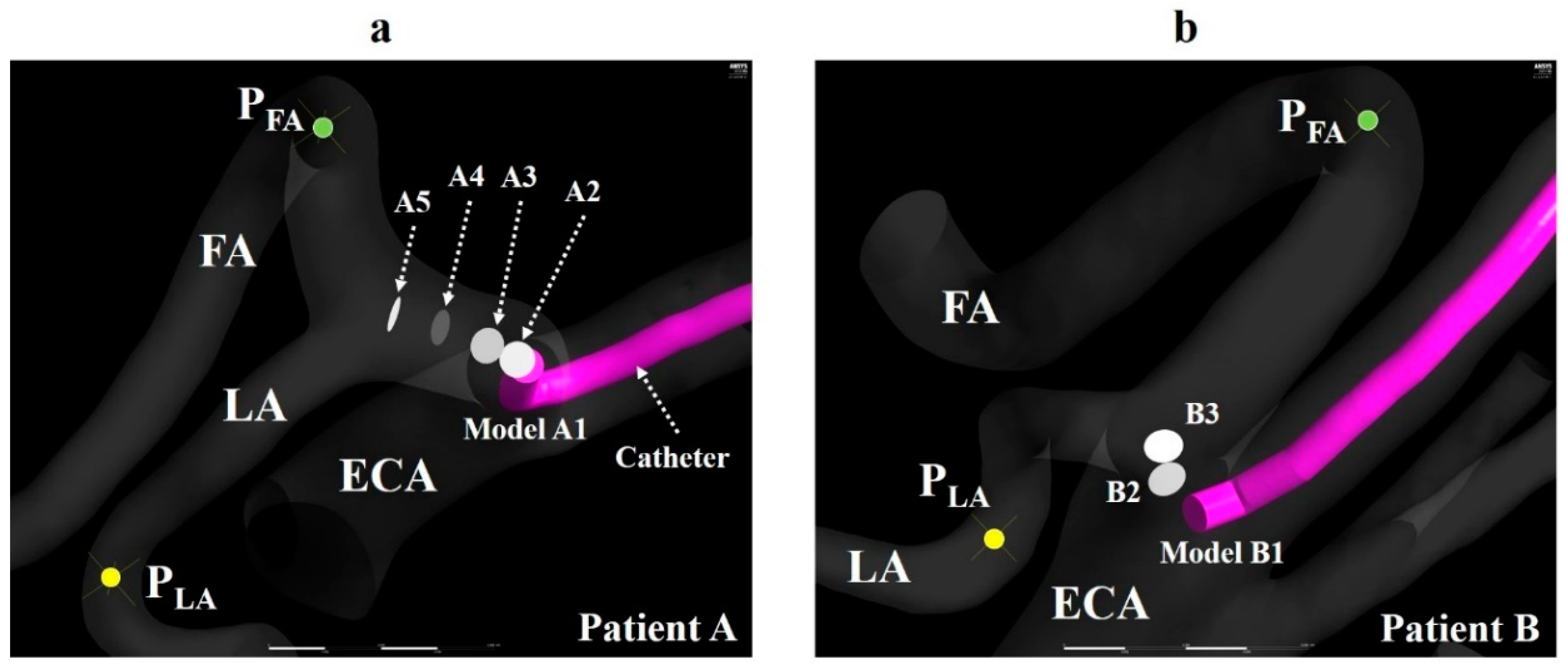
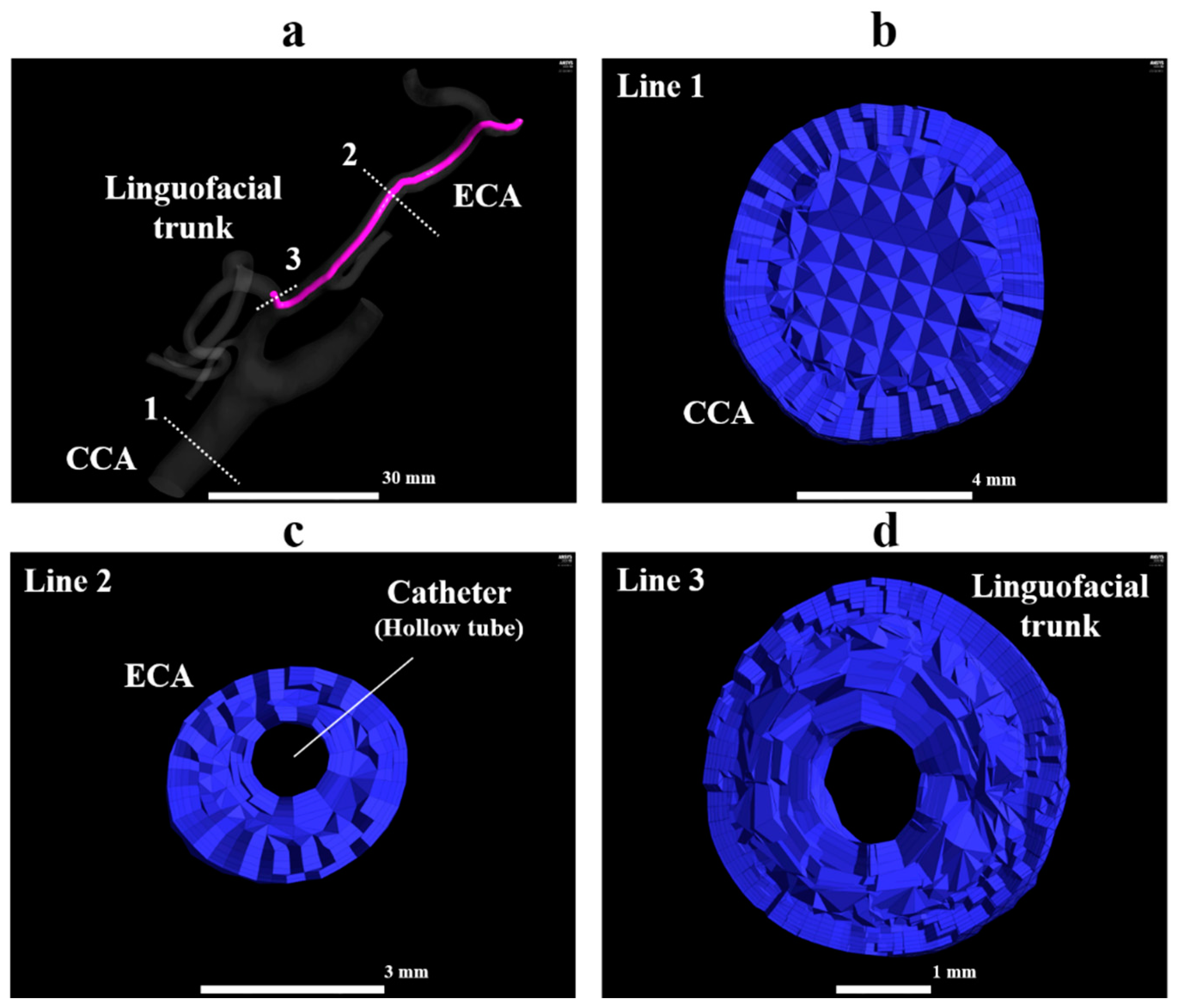
2.1. Geometrical Model and Mesh Generation
2.2. Numerical Method
2.3. Boundary Condition
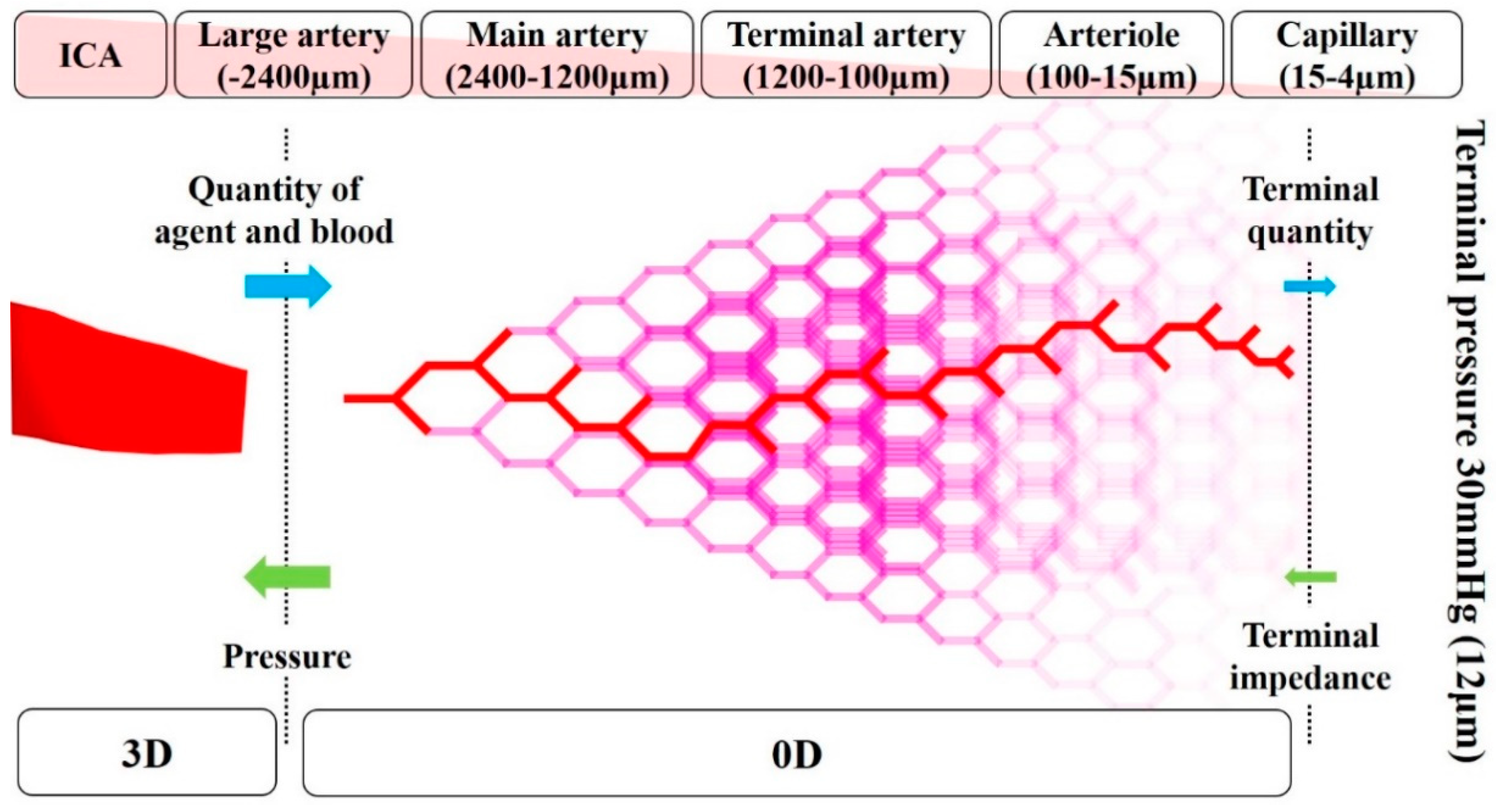
2.4. Zero-Dimensional Resistance Model
2.5. Properties of fluids
2.6. Numerical Condition
2.7. Wall Share Stress Observation
3. Results
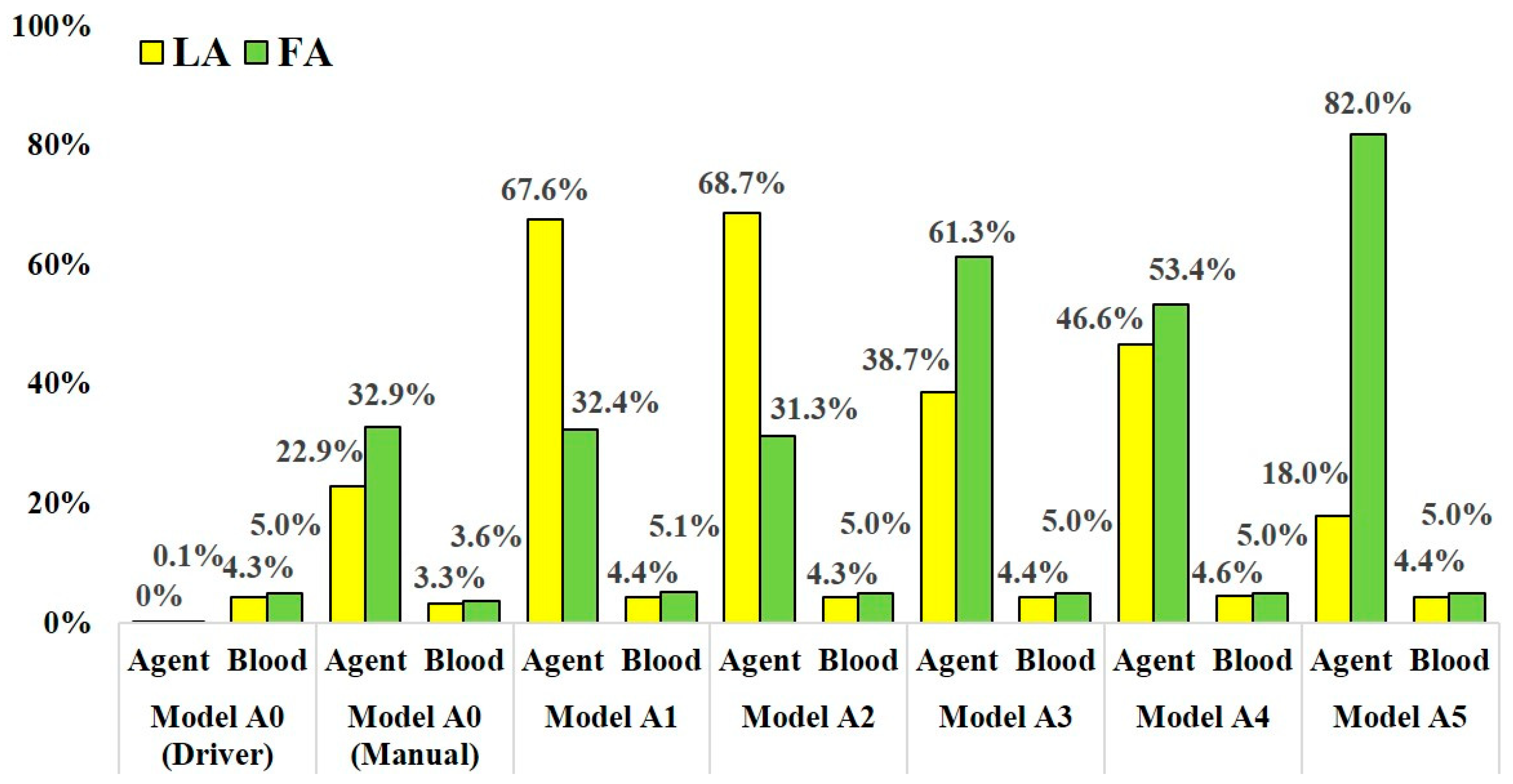
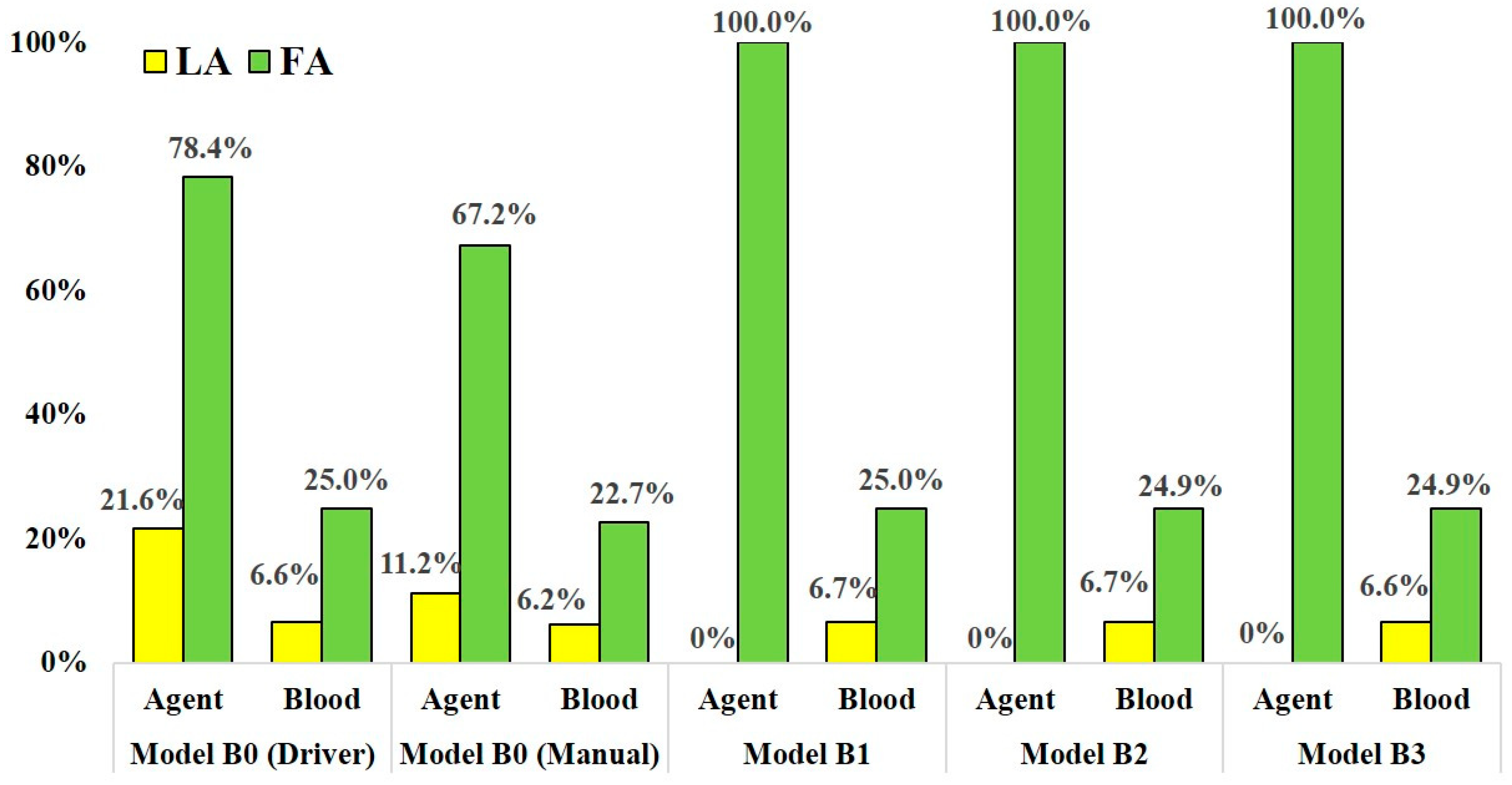
3.1. Mass Distribution of the Agent and Blood
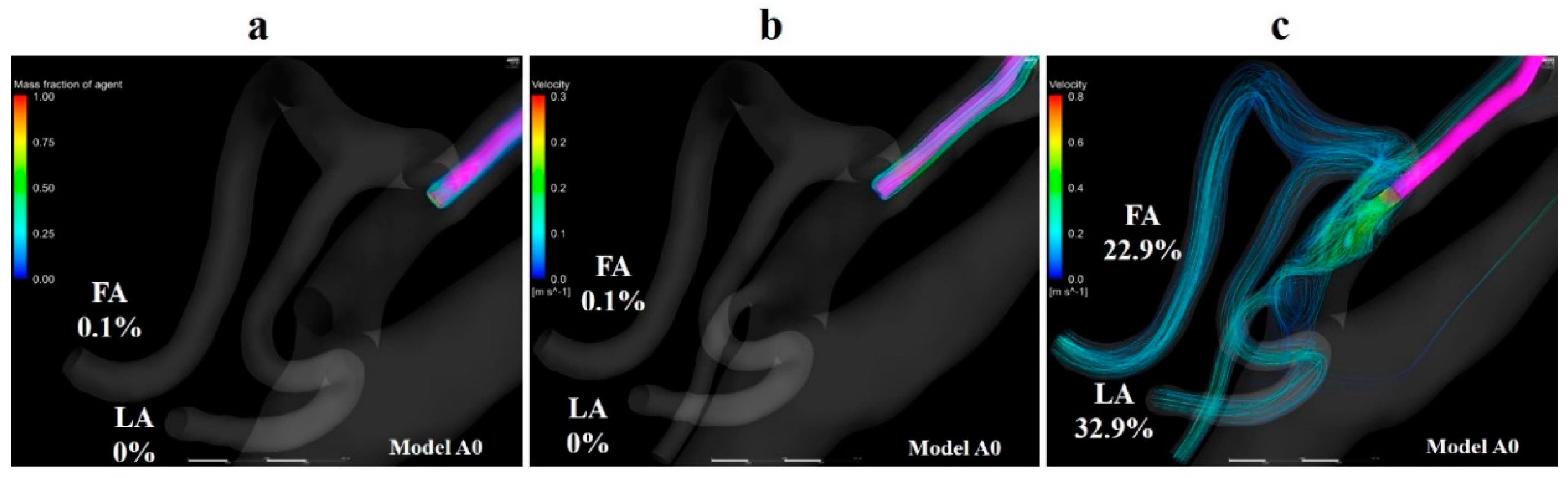
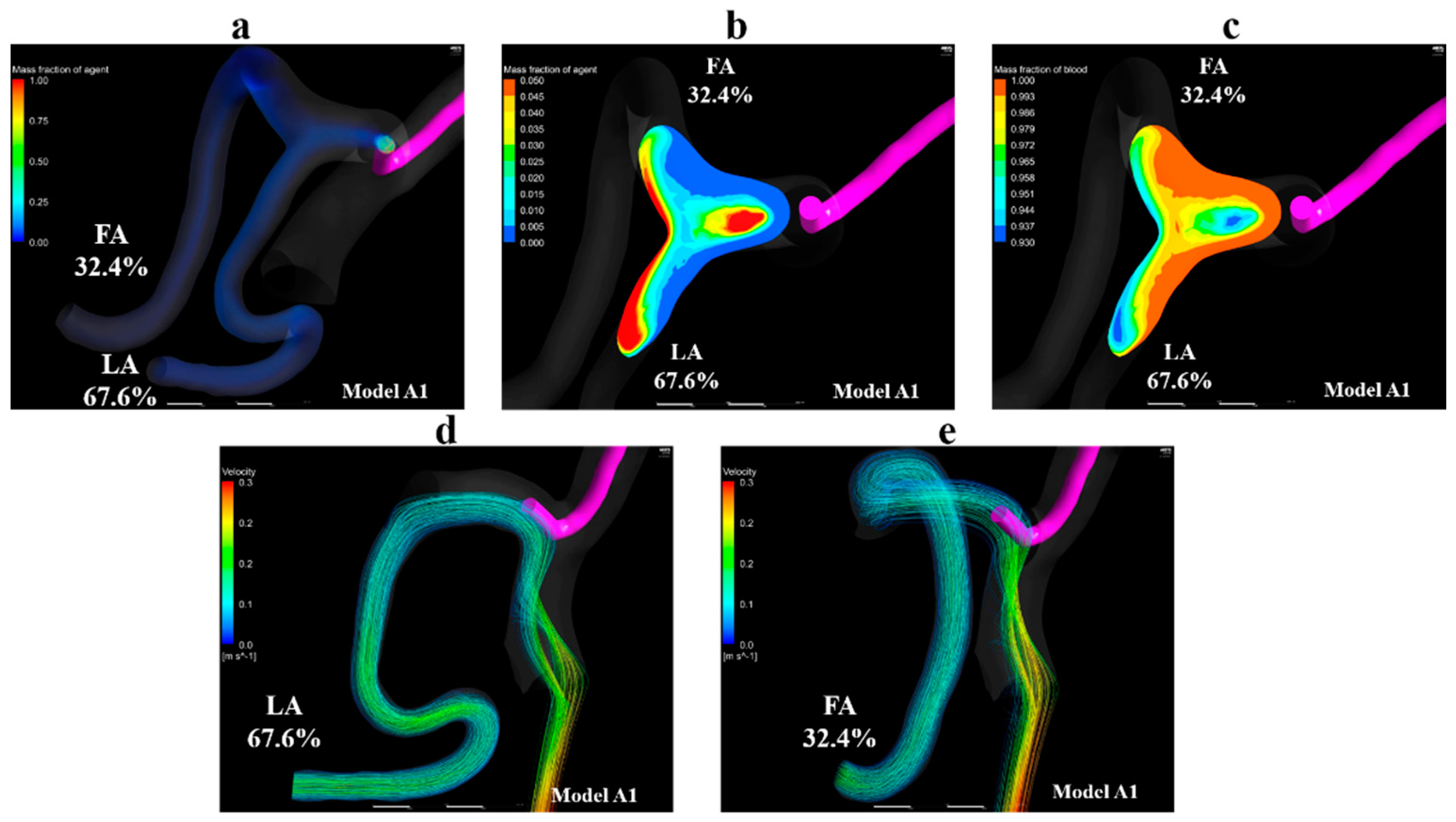
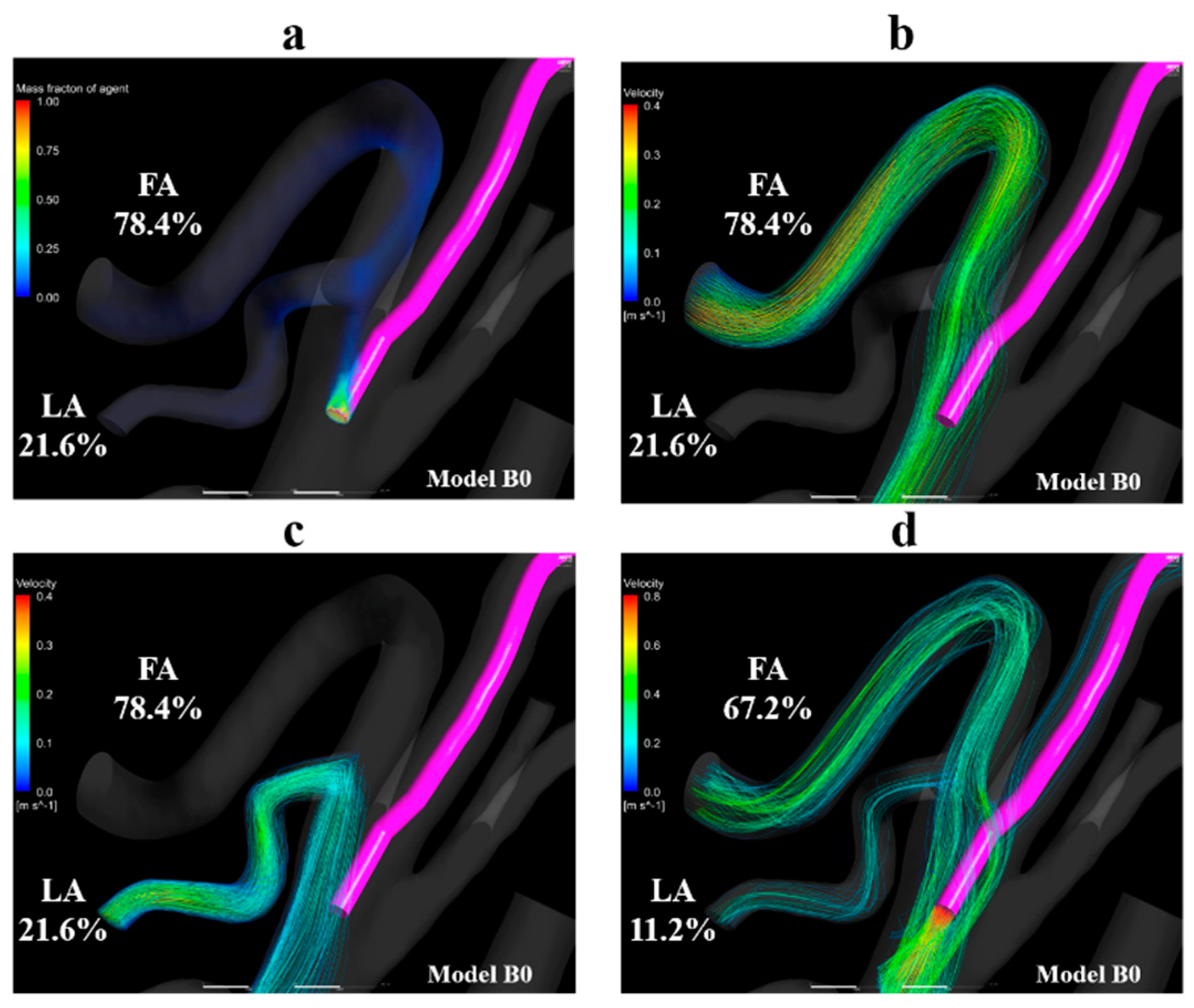
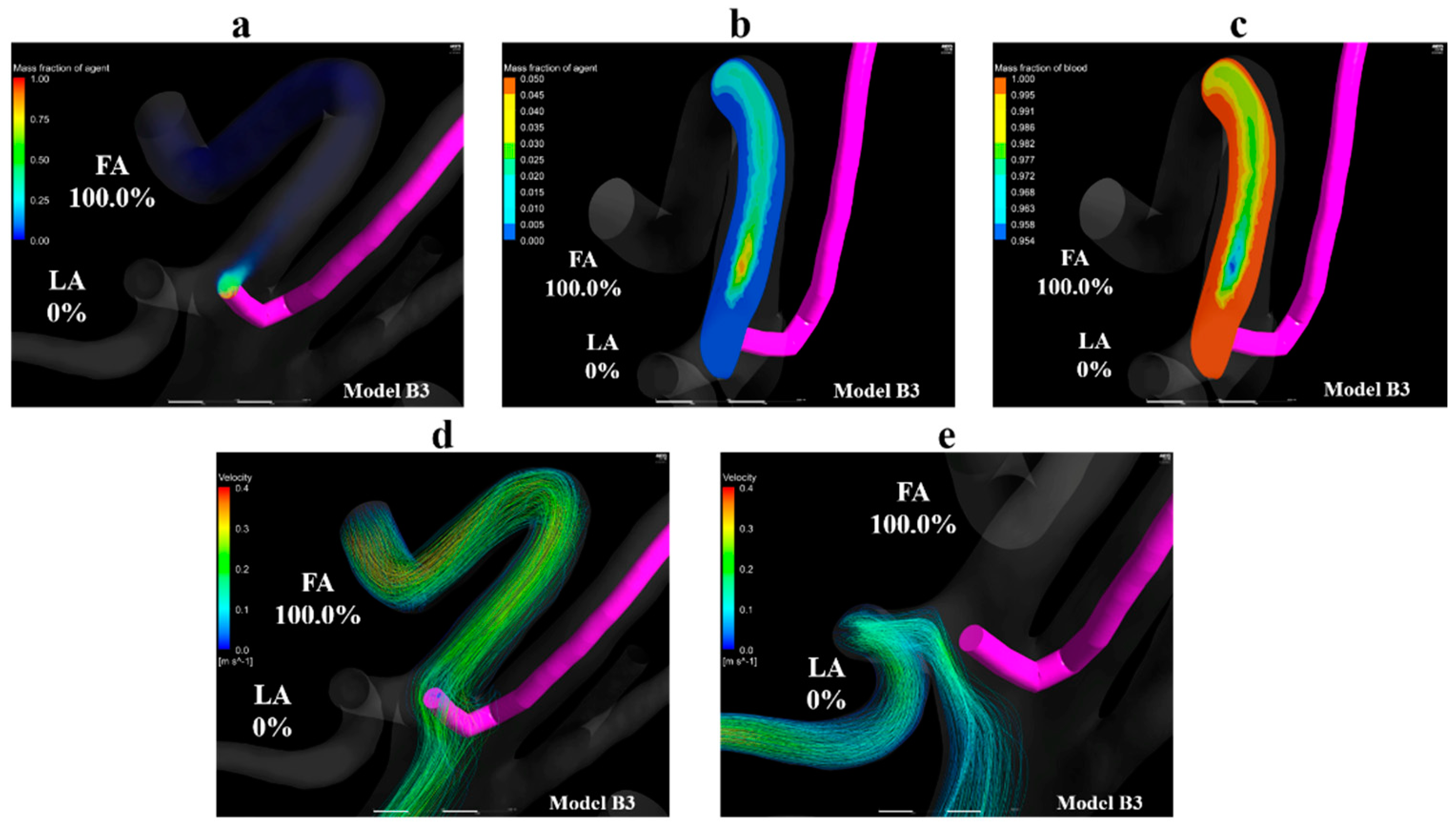
3.2. Volume Rendering Images and Streamlines
3.3. Gradient of Mass Fraction of the Agent
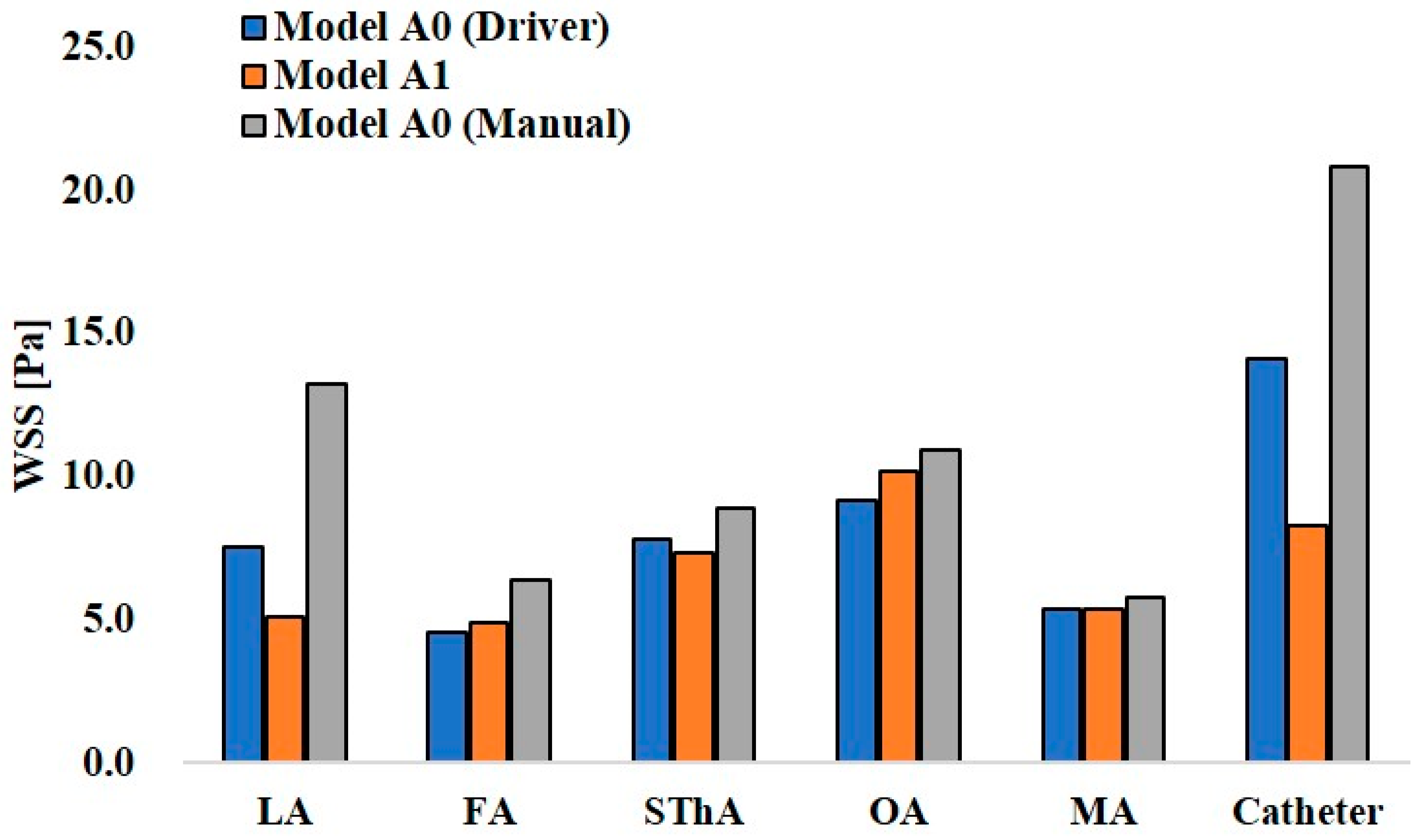
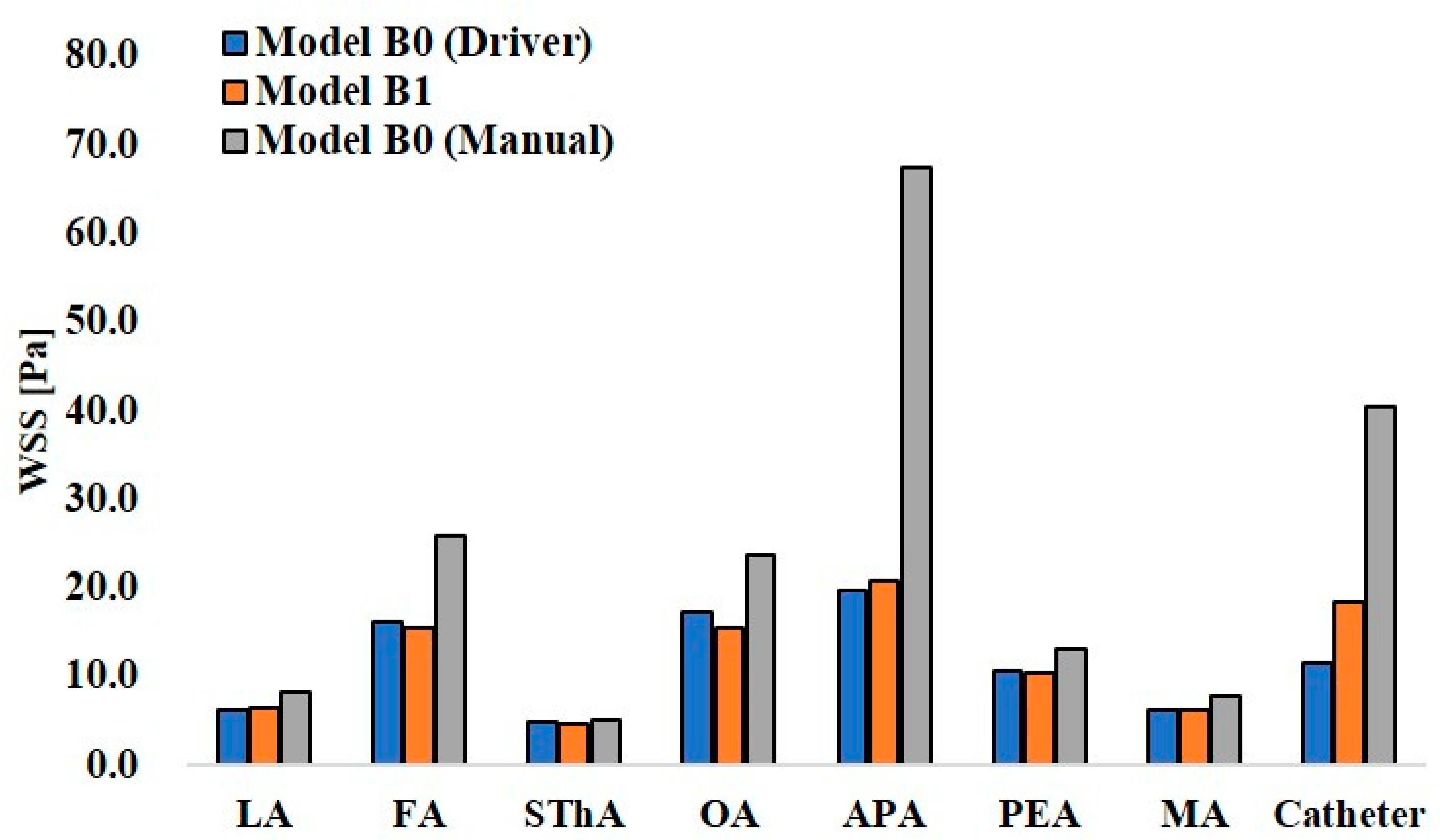
3.4. Wall Share Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| 0D | zero-dimensional |
| 3D | three-dimensional |
| APA | ascending pharyngeal artery |
| CCA | common carotid artery |
| CIAC | conventional intra-arterial chemotherapy |
| ECA | external carotid artery |
| FA | facial artery |
| ICA | internal carotid artery |
| LA | lingual artery |
| MA | maxillary artery |
| OA | occipital artery |
| PAA | posterior auricular artery |
| SSIAC | superselective intra-arterial chemotherapy |
| STA | superficial temporal artery |
| SThA | superior thyroid artery |
| WSS | wall share stress |
References
- Homma, A.; Onimaru, R.; Matsuura, K.; Robbins, K.T.; Fujii, M. Intra-arterial chemoradiotherapy for head and neck cancer. Jpn. J. Clin. Oncol. 2016, 46, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Robbins, K.T. The evolving role of combined modality therapy in head and neck cancer. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Robbins, K.T.; Kumar, P.; Wong, F.S.; Hartsell, W.F.; Flick, P.; Palmer, R.; Weir, A.B., 3rd; Neill, H.B.; Murry, T.; Ferguson, C.; et al. Targeted chemoradiation for advanced head and neck cancer: Analysis of 213 patients. Head Neck 2000, 22, 687–693. [Google Scholar] [CrossRef]
- Tohnai, I. Chemotherapy using intra-arterial infusion for oral cancer. Nagoya J. Med. Sci. 2006, 68, 101–108. [Google Scholar] [PubMed]
- Tohnai, I.; Fuwa, N.; Hayashi, Y.; Kaneko, R.; Tomaru, Y.; Hibino, Y.; Ueda, M. New superselective intra-arterial infusion via superficial temporal artery for cancer of the tongue and tumour tissue platinum concentration after carboplatin (CBDCA) infusion. Oral. Oncol. 1998, 34, 387–390. [Google Scholar] [CrossRef]
- Fuwa, N.; Kodaira, T.; Furutani, K.; Tachibana, H.; Nakamura, T.; Nakahara, R.; Tomoda, T.; Inokuchi, H.; Daimon, T. Intra-arterial chemoradiotherapy for locally advanced oral cavity cancer: Analysis of therapeutic results in 134 cases. Br. J. Cancer 2008, 98, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Mata, J.R.; Mata, F.R.; Souza, M.C.; Nishijo, H.; Ferreira, T.A. Arrangement and prevalence of branches in the external carotid artery in humans. Ital. J. Anat. Embryol. 2012, 117, 65–74. [Google Scholar] [PubMed]
- Ozgur, Z.; Govsa, F.; Ozgur, T. Assessment of origin characteristics of the front branches of the external carotid artery. J. Craniofacial Surg. 2008, 19, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Yonenaga, K.; Tohnai, I.; Mitsudo, K.; Mori, Y.; Saijo, H.; Iwai, T.; Yonehara, Y.; Ota, Y.; Torigoe, K.; Takato, T. Anatomical study of the external carotid artery and its branches for administration of superselective intra-arterial chemotherapy via the superficial temporal artery. Int. J. Clin. Oncol. 2011, 16, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Troupis, T.G.; Dimitroulis, D.; Paraschos, A.; Michalinos, A.; Protogerou, V.; Vlasis, K.; Troupis, G.; Skandalakis, P. Lingual and facial arteries arising from the external carotid artery in a common trunk. Am. Surg. 2011, 77, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Gemmete, J.J. Complications associated with selective high-dose intraarterial cisplatin and concomitant radiation therapy for advanced head and neck cancer. J. Vasc. Interv. Radiol. 2003, 14, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Takagi, S.; Inenaga, R.; Oya, R.; Nakamura, S.; Ikemura, K. Blood vessel density correlates with the effects of targeted intra-arterial carboplatin infusion with concurrent radiotherapy for squamous cell carcinomas of the oral cavity and oropharynx. Br. J. Cancer 2006, 94, 1580–1585. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kitajima, H.; Oshima, M.; Iwai, T.; Ohhara, Y.; Yajima, Y.; Mitsudo, K.; Tohnai, I. Computational fluid dynamics study of intra-arterial chemotherapy for oral cancer. Biomed. Eng. Online 2017, 16, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Ohhara, Y.; Oshima, M.; Iwai, T.; Kitajima, H.; Yajima, Y.; Mitsudo, K.; Krdy, A.; Tohnai, I. Investigation of blood flow in the external carotid artery and its branches with a new 0D peripheral model. Biomed. Eng. Online 2016, 15, 16. [Google Scholar] [CrossRef] [PubMed]
- Haynes, W.M. CRC Handbook of Chemistry and Physics, 93rd ed.; CRC Press: Boca Raton, FL, USA, 2012; Section 6; pp. 250–251. [Google Scholar]
- Holz, M.; Heil, S.R.; Sacco, A. Temperature-dependent self-diffusion coefficients of water and six selected molecular liquids for calibration in accurate 1H NMR PFG measurements. Phys. Chem. Chem. Phys. 2000, 2, 4740–4742. [Google Scholar] [CrossRef]
- Antiga, L.; Piccinelli, M.; Botti, L.; Ene-Iordache, B.; Remuzzi, A.; Steinman, D.A. An image-based modeling framework for patient-specific computational hemodynamics. Med. Biol. Eng. Comput. 2008, 46, 1097–1112. [Google Scholar] [CrossRef] [PubMed]
- Torii, R.; Keegan, J.; Wood, N.B.; Dowsey, A.W.; Hughes, A.D.; Yang, G.-Z.; Firmin, D.N.; Thom, S.A.M.G.; Xu, X.Y. MR image-based geometric and hemodynamic investigation of the right coronary artery with dynamic vessel motion. Ann. Biomed. Eng. 2010, 38, 2606–2620. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, S.; Kemmerling, E.M.C. The effect of inlet and outlet boundary conditions in image-based CFD modeling of aortic flow. Biomed. Eng. Online 2018, 17, 66. [Google Scholar] [CrossRef] [PubMed]
- Rhode, S.; Paul, M.C.; Martens, E.; Campbell, D.F. Simulation of hemodynamic flow in head and neck cancer chemotherapy. Biomed. Eng. Online 2011, 10, 104. [Google Scholar] [CrossRef] [PubMed]
- Fry, D. Acute vascular endothelial changes associated with increased blood velocity gradients. Circ. Res. 1968, 22, 165–197. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model A0 (Driver) | Model A0 (Manual) | Model A1 | Model A2 | Model A3 | Model A4 | Model A5 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agent | Blood | Agent | Blood | Agent | Blood | Agent | Blood | Agent | Blood | Agent | Blood | Agent | Blood | |
| LA | 0 | 4.3 | 22.9 | 3.3 | 67.6 | 4.4 | 68.7 | 4.3 | 38.7 | 4.4 | 46.6 | 4.6 | 18.0 | 4.4 |
| FA | 0.1 | 5.0 | 32.9 | 3.6 | 32.4 | 5.1 | 31.3 | 5.0 | 61.3 | 5.0 | 53.4 | 5.0 | 82.0 | 5.0 |
| SThA | 0 | 2.7 | 18 | 1.8 | 0 | 2.7 | 0 | 2.7 | 0 | 2.7 | 0 | 2.7 | 0 | 2.7 |
| OA | 1.8 | 4.7 | 2.1 | 4.8 | 0 | 4.7 | 0 | 4.7 | 0 | 4.7 | 0 | 4.7 | 0 | 4.7 |
| MA | 98.1 | 13.8 | 22.9 | 13.2 | 0 | 13.9 | 0 | 13.8 | 0 | 13.8 | 0 | 13.8 | 0 | 13.9 |
| ICA | 0 | 69.5 | 0.9 | 73.3 | 0 | 69.3 | 0 | 69.5 | 0 | 69.4 | 0 | 69.3 | 0 | 69.4 |
| Model B0 (Driver) | Model B0 (Manual) | Model B1 | Model B2 | Model B3 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Agent | Blood | Agent | Blood | Agent | Blood | Agent | Blood | Agent | Blood | |
| LA | 21.6 | 6.6 | 11.2 | 6.2 | 0 | 6.7 | 0 | 6.7 | 0 | 6.6 |
| FA | 78.4 | 25.0 | 67.2 | 22.7 | 100.0 | 25.0 | 100.0 | 24.9 | 100.0 | 24.9 |
| SThA | 0 | 2.8 | 0 | 3.0 | 0 | 2.8 | 0 | 2.83 | 0 | 2.8 |
| OA | 0 | 8.9 | 0.5 | 9.4 | 0 | 8.9 | 0 | 8.92 | 0 | 8.9 |
| APA | 0 | 3.5 | 0.2 | 3.4 | 0 | 3.5 | 0 | 3.49 | 0 | 3.5 |
| PEA | 0 | 4.0 | 8.3 | 3.8 | 0 | 4.0 | 0 | 3.97 | 0 | 4.0 |
| MA | 0 | 4.2 | 12.6 | 3.7 | 0 | 4.2 | 0 | 4.23 | 0 | 4.2 |
| ICA | 0 | 45.0 | 0 | 47.7 | 0 | 44.9 | 0 | 45.0 | 0 | 45.0 |
| Model A0 (Driver) | Model 0 (Manual) | Model A1 | Model A2 | Model A3 | Model A4 | Model A5 | |
|---|---|---|---|---|---|---|---|
| Catheter zone | 1093.8 | 236.1 | 351.4 | 311.6 | 309.5 | 253.3 | 351.4 |
| LA zone | 0 | 89.8 | 24.7 | 25.8 | 15.0 | 24.8 | 24.7 |
| FA zone | 0 | 45.2 | 12.2 | 12.9 | 15.2 | 17.0 | 12.2 |
| Model B0 (Driver) | Model B0 (Manual) | Model B1 | Model B2 | Model 3 | |
|---|---|---|---|---|---|
| Catheter zone | 440.2 | 57.2 | 307.3 | 163.5 | 93.6 |
| LA zone | 8.4 | 9.7 | 0 | 0 | 0 |
| FA zone | 6.7 | 15.4 | 5.5 | 7.5 | 3.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitajima, H.; Iwai, T.; Yajima, Y.; Mitsudo, K. Computational Fluid Dynamics Study of Superselective Intra-arterial Chemotherapy for Oral Cancer: Flow Simulation of Anticancer Agent in the Linguofacial Trunk. Appl. Sci. 2020, 10, 7496. https://doi.org/10.3390/app10217496
Kitajima H, Iwai T, Yajima Y, Mitsudo K. Computational Fluid Dynamics Study of Superselective Intra-arterial Chemotherapy for Oral Cancer: Flow Simulation of Anticancer Agent in the Linguofacial Trunk. Applied Sciences. 2020; 10(21):7496. https://doi.org/10.3390/app10217496
Chicago/Turabian StyleKitajima, Hiroaki, Toshinori Iwai, Yasuharu Yajima, and Kenji Mitsudo. 2020. "Computational Fluid Dynamics Study of Superselective Intra-arterial Chemotherapy for Oral Cancer: Flow Simulation of Anticancer Agent in the Linguofacial Trunk" Applied Sciences 10, no. 21: 7496. https://doi.org/10.3390/app10217496
APA StyleKitajima, H., Iwai, T., Yajima, Y., & Mitsudo, K. (2020). Computational Fluid Dynamics Study of Superselective Intra-arterial Chemotherapy for Oral Cancer: Flow Simulation of Anticancer Agent in the Linguofacial Trunk. Applied Sciences, 10(21), 7496. https://doi.org/10.3390/app10217496