A Survey on Artificial Intelligence Techniques for Biomedical Image Analysis in Skeleton-Based Forensic Human Identification




Abstract
1. Introduction
2. Methodological Background
2.1. Forensic Anthropology and Human Identification
- Sex estimation of adult individuals. It is recommended to employ the pelvic and skull morphologic traits [16]. When this is not possible, the discriminant formulas for postcranial skeleton proposed by [17] are recommended. Sex is the first characteristic to be estimated, since many formulas in remaining steps vary depending on sex.
- Sex estimation of subadults (i.e., children). Sexual characteristics are not fully developed and discriminant until puberty has been passed. For this reason, estimating the sex of children is one of the main difficulties faced by FA when studying subadult individuals. However, there are some approaches that have shown a high potential, like the analysis of morphological features of the ilium, mainly the sciatic notch [18].
- Age estimation of dead adult individuals. The analysis of the degenerative processes of the pubic symphysis is recommended, preferably following the method proposed in [19]. This method should be combined with the analysis of canine root transparency (presented in [20]) according to the two-step procedure proposed in [21]. When this is not possible, the recommended methods are: that proposed in [22] for the analysis of the coxal atrial veneer; that proposed in [23] for the sternal end of the fourth rib; and finally the analysis of the processes of obliteration of the cranial sutures proposed in [24], this being the least reliable method but the only one available on many occasions.
- Age estimation of dead children. For individuals who have not yet reached maturity (subadults), the methods proposed by Scheuer and Black in 2004 [25] are recommended.
- Age estimation of the living. The hand and wrist development atlas introduced in [26], the method for dental development proposed in [27], and the analysis of ossification status of the sternal epiphysis of the clavicle presented in [28] are recommended for different age ranges. Age estimation of the living acquires special relevance when determining the legal age of the person being scrutinized (i.e., to determine if the person is 18 years old to carry out age-dependent legal procedures appropriately in accordance with the rule of law).
- Stature estimation is performed employing long bones. When the remains are contemporary and of Mediterranean origin, it is recommended to use the formulas proposed in [29] for the femur and humerus, and those proposed in [30] for the tibia. When the remains are from the North American population, the formulas proposed in [31] as well as the FORDISC computer program [32] will preferably be applied.
- The estimation of population ancestry is the most inaccurate element of the BP given the low reliability of its results. It should only be used as an orientation criterion when there is a good agreement between the human study groups and skeletal biology, giving preference to morphological criteria of the skull.
2.2. Artificial Intelligence and Forensic Human Identification
3. Forensic Human Identification through the Analysis of Biomedical Images
3.1. AI-Based Approaches for Biological Profile Estimation
3.1.1. Sex Estimation from Skeletal Structures
3.1.2. Age Estimation from Skeletal Structures
3.2. AI-Based Approaches for Traumatism and Pathology Analysis
3.3. AI-Based Approaches for Comparative Radiography
3.3.1. 2D-2D Approaches for Comparative Radiography
3.3.2. 3D-2D Approaches for Comparative Radiography
3.3.3. 3D-3D Approaches for Comparative Radiography
3.3.4. Virtopsy
3.4. AI-Based Approaches for Craniofacial Superimposition
3.4.1. Acquisition and Processing of the Materials
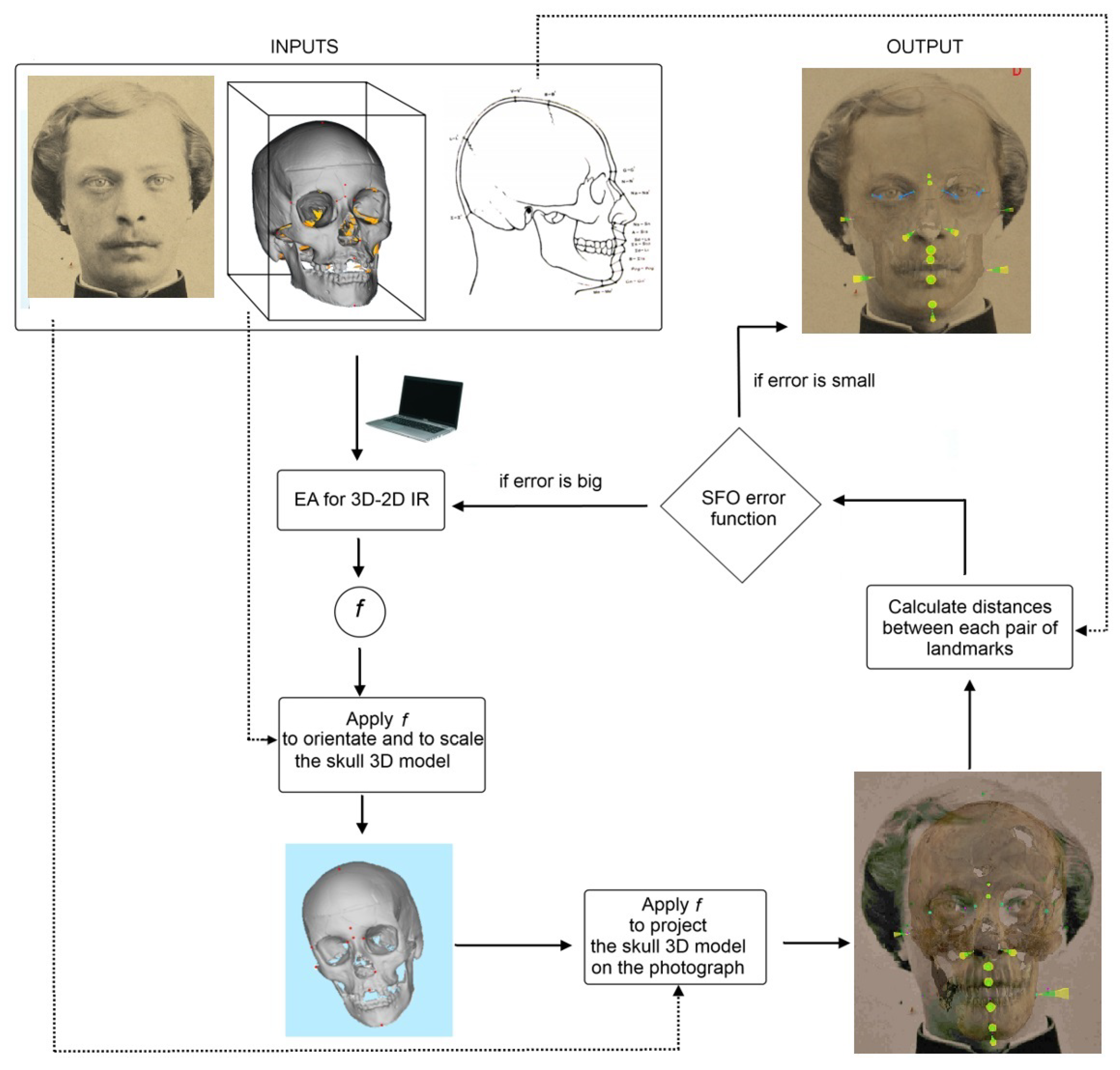
3.4.2. Skull-Face Overlay
3.4.3. Skull-Face Overlay Assessment and Decision Making
3.4.4. 3D-3D Computer-Aided Approaches for Craniofacial Superimposition
3.5. AI-Based Approaches for Facial Reconstruction
4. Discussion and Conclusions
- The reduced number of multidisciplinary research groups including forensic researchers in anthropology and related sciences (odontology, forensic medicine or anatomy) and AI experts. This interaction is essential in order to establish a fluid and productive collaboration between different scientific disciplines. On one hand, it allows unifying terminology and facilitating the useful transfer of knowledge among scientists. On the other hand, it allows joining forces in a common direction towards challenging research projects. This interdisciplinary collaboration should bear fruit in the recognition that machines are not here to replace human beings, but to assist them and facilitate their work in those tasks that humans do not want perform or want to perform faster and easier.
- With few and commendable exceptions [213,214], there is a lack of large and open public data sets for research purposes in FA. Currently, data availability is the starting point and requirement for the validation and comparison of many proposed AI techniques (like DL approaches). This is specially true nowadays, in the DL era; since we need to remark one of the main characteristics, and at the same time limitations, of ML models (largely used nowadays in many of the described tasks, like classification, regression, or segmentation): the result will be as good as the data available, so if the dataset used to train these systems is not broad and diverse enough, the results will surely be suboptimal. Furthermore, to compare the performance of newly developed methods, a common forensic dataset of known case studies should be available. This is a common practice in other fields as close as clinical medicine and biomedical research, with representative examples such as classification and localization of common thorax diseases in chest X-ray [215], melanoma classification in skin photographs [216], the cancer imaging archive [217], the Allen mouse and human brain atlases for combining genomics and neuroanatomy [218], the MIMIC critical care database that contains health data associated with approximately 40,000 critical care patients [219], the Alzheimer’s Disease neuroimaging initiative [220], or the OpenNeuro initiative for sharing MRI and fMRI data [221], among others. It is also important to recognize the fact that it is not only about acquiring and storing data, but how these data are compiled in order to meet ethical requirements and avoid machine bias [222], among others. All this problematic, related to the absence of large and complete datasets, may also be at the root of the inadequacy found in how some methods calculate, express and interpret the obtained errors (for instance, in age estimation [223]).
- Many of today’s most popular and successful AI techniques to tackle imaging problems are rarely used in FA applications. This fact will undoubtedly open a niche for its application. We can think about techniques of few-shot learning [224] (to train models from a few examples), generative adversarial networks [225] or non-adversarial generative models [226] (for example, to generate data when these are scarce), or Siamese networks [227] (to establish if two images provided as input belong to the same class). Similarly, the use of 3D ConvNets [228] to directly process three-dimensional information is non-existent, as well as the combined use of recurrent and convolutional networks [229] to carry out more complex tasks (such as the textual description of images automatically, i.e., image captioning). Even the automation of certain tasks, like landmarking [230] or head pose estimation [231], is seldom performed using state-of-the-art ML/CV approaches.
- As in many other medical applications, the accuracy of the results is not the only goal to be accomplished. The results are also intended to be understandable by human users. The recently introduced concept of explainable AI encompasses AI systems for opening black box models, for improving the understanding and comprehensibility of what the models have learned, and/or for explaining individual predictions [232,233]. FA demands solutions designed considering the required explainability of some particular tasks while achieving the required performance and accuracy, providing the designed (human-centric) models or decision support systems with the ability to trust the system output [234]. These types of approaches are very scarce within the research topic addressed in this article. However, its introduction into the field would be highly desirable, due to the necessity for the conclusions of a FA report to be understood by a medical examiner or a judge.
- In relation to CFS, it would be especially relevant to carry out systematic and massive studies to verify its effectiveness as a forensic identification technique. AI techniques would be very useful in carrying out massive experiments and in automating and objectifying the sub-tasks involved in the CFS process. All this would contribute to increasing the scientific support of CFS, as well as considering CFS as a primary identification technique (instead of secondary) (Remember that primary identification methods are those that allow positive identification of a person. While secondary identification techniques are those that allow candidates to be discarded, i.e., they do not “tell” if the AM and PM materials correspond to the same person, but rather if they are not compatible and, therefore, do not correspond to the same person.). In practical terms, this massive validation would proceed under the hypothesis that the skull is like a fingerprint, which, in case this hypothesis is empirically validated, would serve to give more validity to CFS as evidence in a court of justice.
- CR already is a primary identification technique. The main task to be carried out would be the automation and integration of all stages of the CR process:
- -
- Automatic analysis and segmentation of any type of skeletal structure in any type of image, radiographs or CT scans.
- -
- Automatic location and classification of morphological patterns on radiographs and CT scans that can help with identification.
- -
- Automatic superimposition of AM and PM materials, regardless of whether they are radiographs, 3D surface models and/or CT scans.
- -
- Lastly, the development of a decision support system able to aggregate as much information as possible to help the forensic expert in the decision-making process.
- In relation to BP, there is also a real need (and urgent need in many cases (For instance, the age estimation of living individuals, that could be related to cases of pedophilia in pictures or videos, or the determination of the legal age in cases unaccompanied minor migrants.)) to incorporate tools that facilitate BP estimation.
- -
- The usual methodology in FA is generally limited in effectiveness. Many of these methods use very subjective criteria and, in many cases, have not been properly validated [223]. Some of the most commonly used BP methods were developed 50–100 years ago, as Todd’s ten-phase method to analyze the pubic symphysis to estimate age [235], the Greulich and Pyle method based on the atlas [26] from the late fifties, and that of Tanner-Whitehouse [79], developed in 1975. These were elaborated with a limited number of examples (a few hundred), normally biased by a common ancestry, and a limited age range compared to modern populations. In addition, the phases/patterns were observed and documented by one or a few researchers (based on their experience, knowledge and ability to recognize patterns), and a large group of methods is based on a series of linear measurements directly taken from the bone with the caliber or on radiographic images. From this point of view, it is necessary to develop identification methods with a higher degree of certainty and discriminant capability, which ensure compliance with scientific standards and, consequently, their admissibility as expert evidence.
- -
- Despite the publication of new and more sophisticated methods for BP estimation, these are not integrated into the usual practice of FA. Such daily practice is almost exclusively based on the use of manual measurement tools and spreadsheets, and thus practitioners usually perceive these new methods as more complex than traditional approaches. The use of specific software is thus limited to a small number of practitioners. The lack of tools and computer platforms that facilitate and integrate the use of more complex and effective methods causes anthropologists to continue using methods that are already obsolete, though easy to use.
- -
- In order to face the two former limitations, it is also essential to address the difficulty of obtaining appropriate data/case studies for the development and validation of BP methods. On the one hand, as already mentioned before, study samples are very scarce or difficult to achieve. We refer, for example, to skeletal human remains, access to corpses available for research, invasive clinical studies, etc. On the other hand, such samples must meet important requirements: absence of pathological conditions or trauma (main limitation in clinical studies), both sexes, age groups and different ancestries well represented, complete and reliable AM information from official records, etc.
Funding
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| AM | Ante-Mortem |
| BP | Biological Profile |
| CFS | Craniofacial Superimposition |
| ConvNet | Convolutional Neural Network |
| CR | Comparative Radiography |
| CT | Computed Tomography |
| CV | Computer Vision |
| DL | Deep Learning |
| FA | Forensic Anthropology |
| ID | Human Identification |
| ML | Machine Learning |
| MRI | Magnetic Resonance Imaging |
| PM | Post-Mortem |
| ROI | Region of Interest |
| SC | Soft Computing |
| SFI | Skeleton-based Forensic Identification |
| SFO | Skull-Face Overlay |
References
- Thompson, T.; Black, S. Forensic Human Identification: An Introduction; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Thibault, E.A.; Lynch, L.M.; McBride, R.B.; Walsh, G. Proactive Police Management; Prentice Hall: Upper Saddle River, NJ, USA, 2004. [Google Scholar]
- Ubelaker, D.H. Forensic anthropology: Methodology and diversity of applications. In Biological Anthropology of the Human Skeleton; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2008; pp. 41–69. [Google Scholar]
- Beauthier, J.P.; Valck, E.; Lefevre, P.; Winne, J.D. Mass disaster victim identification: The tsunami experience. Open Forensic Sci. J. 2009, 2. [Google Scholar] [CrossRef]
- Damas, S.; Cordón, O.; Ibáñez, O.; Santamaría, J.; Alemán, I.; Botella, M.; Navarro, F. Forensic identification by computer-aided craniofacial superimposition: A survey. ACM Comput. Surv. (CSUR) 2011, 43, 1–27. [Google Scholar] [CrossRef]
- Nissan, E. Computer Applications for Handling Legal Evidence, Police Investigation and Case Argumentation; Springer: Berlin/Heidelberg, Germany, 2012; Volume 5. [Google Scholar]
- Jain, A.K.; Li, S.Z. Handbook of Face Recognition; Springer: Berlin/Heidelberg, Germany, 2011; Volume 1. [Google Scholar]
- Valentine, T.; Davis, J.P. Forensic facial identification: A practical guide to best practice. In Forensic Facial Identification: Theory and Practice of Identification from Eyewitnesses, Composites and CCTV; John Wiley & Sons: Chichester, UK, 2015; pp. 323–347. [Google Scholar]
- Stephan, C.N.; Caple, J.M.; Guyomarc’h, P.; Claes, P. An overview of the latest developments in facial imaging. Forensic Sci. Res. 2019, 4, 10–28. [Google Scholar] [CrossRef]
- Zhao, W.; Chellappa, R.; Phillips, P.; Rosenfeld, A. Face recognition: A literature survey. ACM Comput. Surv. 2003, 35, 399–458. [Google Scholar] [CrossRef]
- Ding, C.; Tao, D. A comprehensive survey on pose-invariant face recognition. ACM Trans. Intell. Syst. Technol. 2016, 7, 1–42. [Google Scholar] [CrossRef]
- England, N.; Improvement, N. Diagnostic Imaging Dataset Statistical Release; Department of Health: London, UK, 2016; Volume 421.
- Laserson, J.; Lantsman, C.D.; Cohen-Sfady, M.; Tamir, I.; Goz, E.; Brestel, C.; Bar, S.; Atar, M.; Elnekave, E. Textray: Mining clinical reports to gain a broad understanding of chest x-rays. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; pp. 553–561. [Google Scholar]
- Yen, K.; Lövblad, K.O.; Scheurer, E.; Ozdoba, C.; Thali, M.J.; Aghayev, E.; Jackowski, C.; Anon, J.; Frickey, N.; Zwygart, K.; et al. Post-mortem forensic neuroimaging: Correlation of MSCT and MRI findings with autopsy results. Forensic Sci. Int. 2007, 173, 21–35. [Google Scholar] [CrossRef]
- Obenauer, S.; Herold, T.; Fischer, U.; Grabbe, E.; Fadjasch, G.; Saternus, K.; Koebke, J. Evaluation of injuries of the upper cervical spine in a postmortem study with digital radiography, CT and MRI. RoeFo-Fortschritte auf dem Gebiete der Roentgenstrahlen und der Neuen Bildgebenden Verfahren 1999, 171, 473–479. [Google Scholar]
- Ferembach, D. Recomendations for age and sex diagnosis of skeletons. J. Hum. Evolut. 1980, 9, 517–549. [Google Scholar]
- Aguilera, I.A. Determinación del Sexo en el Esqueleto Postcraneal. Estudio de una Población Mediterránea Actual. Ph.D. Thesis, Universidad de Granada, Granada, Spain, 1997. [Google Scholar]
- Olivares, J.I.; Aguilera, I.A. Validation of the sex estimation method elaborated by Schutkowski in the Granada Osteological Collection of identified infant and young children: Analysis of the controversy between the different ways of analyzing and interpreting the results. Int. J. Leg. Med. 2016, 130, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.; Suchey, J.M. Skeletal age determination based on the os pubis: A comparison of the Acsádi-Nemeskéri and Suchey-Brooks methods. Hum. Evolut. 1990, 5, 227–238. [Google Scholar] [CrossRef]
- Lamendin, H.; Baccino, E.; Humbert, J.; Tavernier, J.; Nossintchouk, R.; Zerilli, A. A simple technique for age estimation in adult corpses: The two criteria dental method. J. Forensic Sci. 1992, 37, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Baccino, E.; Zerilli, A. The two step strategy (TSS) or the right way to combine a dental (Lamendin) and an anthropological (Suchey–Brooks system) method for age determination. Proc. Am. Acad. Forensic Sci. 1997, 3, 150. [Google Scholar]
- Lovejoy, C.O.; Meindl, R.S.; Pryzbeck, T.R.; Mensforth, R.P. Chronological metamorphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. Am. J. Phys. Anthropol. 1985, 68, 15–28. [Google Scholar] [CrossRef]
- Işcan, M.Y.; Loth, S.R.; Wright, R.K. Age estimation from the rib by phase analysis: White males. J. Forensic Sci. 1984, 29, 1094–1104. [Google Scholar]
- Meindl, R.S.; Lovejoy, C.O. Ectocranial suture closure: A revised method for the determination of skeletal age at death based on the lateral-anterior sutures. Am. J. Phys. Anthropol. 1985, 68, 57–66. [Google Scholar] [CrossRef]
- Scheuer, L.; Black, S. The Juvenile Skeleton; Elsevier: Amsterdam, The Netherlands, 2004. [Google Scholar]
- Greulich, W.W.; Pyle, S.I. Radiographic Atlas of Skeletal Development of the Hand and Wrist; Stanford University Press: Redwood City, CA, USA, 1959. [Google Scholar]
- Demirjian, A.; Goldstein, H.; Tanner, J.M. A new system of dental age assessment. Hum. Biol. 1973, 45, 211–227. [Google Scholar] [PubMed]
- Kellinghaus, M.; Schulz, R.; Vieth, V.; Schmidt, S.; Schmeling, A. Forensic age estimation in living subjects based on the ossification status of the medial clavicular epiphysis as revealed by thin-slice multidetector computed tomography. Int. J. Leg. Med. 2010, 124, 149–154. [Google Scholar] [CrossRef]
- Nunes de Mendonça, M. Contribución para la identificación humana a partir del estudio de las estructuras óseas. In Determinacion de la Talla a Traves de la Longitud de los Huesos Largos; Universidad Complutense de Madrid: Madrid, Spain, 1998. [Google Scholar]
- Belmonte, M. Determinación de la Estatura a Través de la Tibia en Población Española Contemporánea. Ph.D. Thesis, Universidad de Granada, Granada, Spain, 2012. [Google Scholar]
- Trotter, M.; Gleser, G.C. A re-evaluation of estimation of stature based on measurements of stature taken during life and of long bones after death. Am. J. Phys. Anthropol. 1958, 16, 79–123. [Google Scholar] [CrossRef]
- Ousley, S.D.; Jantz, R.L. FORDISC 2.0: Personal Computer Forensic Discriminant Functions; University of Tennessee: Knoxville, TX, USA, 1996. [Google Scholar]
- Stephan, C.N.; Amidan, B.; Trease, H.; Guyomarc’h, P.; Pulsipher, T.; Byrd, J.E. Morphometric comparison of clavicle outlines from 3D bone scans and 2D chest radiographs: A shortlisting tool to assist radiographic identification of human skeletons. J. Forensic Sci. 2014, 59, 306–313. [Google Scholar] [CrossRef]
- Christensen, A.M.; Smith, M.A.; Gleiber, D.S.; Cunningham, D.L.; Wescott, D.J. The Use of X-ray Computed Tomography Technologies in Forensic Anthropology. Forensic Anthropol. 2018, 1, 124. [Google Scholar] [CrossRef]
- Hatch, G.M.; Dedouit, F.; Christensen, A.M.; Thali, M.J.; Ruder, T.D. RADid: A pictorial review of radiologic identification using postmortem CT. J. Forensic Radiol. Imaging 2014, 2, 52–59. [Google Scholar] [CrossRef]
- Thali, M.J.; Braun, M.; Dirnhofer, R. Optical 3D surface digitizing in forensic medicine: 3D documentation of skin and bone injuries. Forensic Sci. Int. 2003, 137, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Fleischman, J.M. Radiographic identification using midline medical sternotomy wires. J. Forensic Sci. 2015, 60, S3–S10. [Google Scholar] [CrossRef] [PubMed]
- Iscan, M.Y.; Helmer, R. Forensic Analysis of the Skull; Willey-Liss: New York, NY, USA, 1993. [Google Scholar]
- Stephan, C.N. Craniofacial identification: Techniques of facial approximation and craniofacial superimposition. In Handbook of Forensic Anthropology and Archaeology; Left Coast Press: Walnut Creek, CA, USA, 2009; Volume 25, pp. 304–321. [Google Scholar]
- Damas, S.; Wilkinson, C.; Kahana, T.; Veselovskaya, E.; Abramov, A.; Jankauskas, R.; Jayaprakash, P.; Ruiz, E.; Navarro, F.; Huete, M.; et al. Study on the performance of different craniofacial superimposition approaches (II): Best practices proposal. Forensic Sci. Int. 2015, 257, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Huete, M.; Kahana, T.; Ibáñez, O. Past, present, and future of CFS: Literature and international surveys. Leg. Med. 2015, 17, 267–278. [Google Scholar] [CrossRef] [PubMed]
- Damas, S.; Cordón, O.; Ibáñez, O. Handbook on Craniofacial Superimposition: The MEPROCS Project; Springer Nature: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Stephan, C.N.; Henneberg, M. Building faces from dry skulls: Are they recognized above chance rates? J. Forensic Sci. 2001, 46, 432–440. [Google Scholar] [CrossRef]
- Taylor, R.; Craig, P. The wisdom of bones: Facial approximation on the skull. In Computer Graphic Facial Reconstruction; Academic Press: Boston, MA, USA, 2005; pp. 33–55. [Google Scholar]
- Wilkinson, C. Forensic Facial Reconstruction; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar]
- Wilkinson, C.; Rynn, C. Craniofacial Identification; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Lee, W.J.; Wilkinson, C.M.; Hwang, H.S. An accuracy assessment of forensic computerized facial reconstruction employing cone-beam computed tomography from live subjects. J. Forensic Sci. 2012, 57, 318–327. [Google Scholar] [CrossRef]
- Claes, P.; Vandermeulen, D.; De Greef, S.; Willems, G.; Clement, J.G.; Suetens, P. Computerized craniofacial reconstruction: Conceptual framework and review. Forensic Sci. Int. 2010, 201, 138–145. [Google Scholar] [CrossRef]
- Parks, C.L.; Richard, A.H.; Monson, K.L. Preliminary performance assessment of computer automated facial approximations using computed tomography scans of living individuals. Forensic Sci. Int. 2013, 233, 133–139. [Google Scholar] [CrossRef]
- Guyomarc’h, P.; Dutailly, B.; Charton, J.; Santos, F.; Desbarats, P.; Coqueugniot, H. Anthropological Facial Approximation in Three Dimensions (AFA3D): Computer-Assisted Estimation of the Facial Morphology Using Geometric Morphometrics. J. Forensic Sci. 2014, 59, 1502–1516. [Google Scholar] [CrossRef]
- de Buhan, M.; Nardoni, C. A facial reconstruction method based on new mesh deformation techniques. Forensic Sci. Res. 2018, 3, 256–273. [Google Scholar] [CrossRef]
- Foster, K.R.; Huber, P.W. Judging Science: Scientific Knowledge and the Federal Courts; MIT Press: Cambridge, MA, USA, 1999. [Google Scholar]
- Forsyth, D.A.; Ponce, J. Computer Vision: A Modern Approach; Prentice Hall Professional Technical Reference: Upper Saddle River, NJ, USA, 2002. [Google Scholar]
- Bishop, C.M. Pattern Recognition and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Engelbrecht, A.P. Computational Intelligence: An Introduction; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Zadeh, L.A. Soft computing and fuzzy logic. In Fuzzy Sets, Fuzzy Logic, and Fuzzy Systems: Selected Papers by Lotfi a Zadeh; World Scientific: Singapore, 1996; pp. 796–804. [Google Scholar]
- Eiben, A.E.; Smith, J.E. Introduction to Evolutionary Computing; Springer: Berlin/Heidelberg, Germany, 2003; Volume 53. [Google Scholar]
- Aja-Fernández, S.; de Luis-Garcıa, R.; Martın-Fernández, M.A.; Alberola-López, C. A computational TW3 classifier for skeletal maturity assessment. A computing with words approach. J. Biomed. Inform. 2004, 37, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Stern, D.; Ebner, T.; Bischof, H.; Grassegger, S.; Ehammer, T.; Urschler, M. Fully automatic bone age estimation from left hand MR images. Med. Image Comput. Comput. Assist. Interv. 2014, 17, 220–227. [Google Scholar] [PubMed]
- Mansourvar, M.; Ismail, M.A.; Herawan, T.; Gopal Raj, R.; Abdul Kareem, S.; Nasaruddin, F.H. Automated bone age assessment: Motivation, taxonomies, and challenges. Comput. Math. Methods Med. 2013, 2013, 391626. [Google Scholar] [CrossRef]
- Pinto, S.C.D.; Urbanová, P.; Cesar, R.M., Jr. Two-Dimensional Wavelet Analysis of Supraorbital Margins of the Human Skull for Characterizing Sexual Dimorphism. IEEE Trans. Inf. Forensics Secur. 2016, 11, 1542–1548. [Google Scholar] [CrossRef]
- Abdullah, H.; Jamil, M.M.A.; Nor, F.M. Automated Haversian Canal Detection for Histological Sex Determination. In Proceedings of the IEEE Symposium on Computer Applications & Industrial Electronics (ISCAIE), Langkawi, Malaysia, 24–25 April 2017; pp. 69–74. [Google Scholar]
- Pietka, E.; Gertych, A.; Pospiech, S.; Cao, F.; Huang, H.; Gilsanz, V. Computer-assisted bone age assessment: Image preprocessing and epiphyseal/metaphyseal ROI extraction. IEEE Trans. Med. Imaging 2001, 20, 715–729. [Google Scholar] [CrossRef] [PubMed]
- Pietka, E. Computer-assisted bone age assessment—Database adjustment. Int. Congr. Ser. 2003, 1256, 87–92. [Google Scholar] [CrossRef]
- Pietka, E.; Gertych, A.; Pospiechâ, S.; Cao, F.; Huang, H.; Gilzanz, V. Computer-assisted bone age assessment: Graphical user interface for image processing and comparison. J. Digit. Imaging 2004, 17, 175–188. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Afifi, M. 11K Hands: Gender recognition and biometric identification using a large dataset of hand images. Multimedia Tools Appl. 2019, 78, 20835–20854. [Google Scholar] [CrossRef]
- du Jardin, P.; Ponsaillé, J.; Alunni-Perret, V.; Quatrehomme, G. A comparison between neural network and other metric methods to determine sex from the upper femur in a modern French population. Forensic Sci. Int. 2009, 192, 127.e1-6. [Google Scholar] [CrossRef] [PubMed]
- Navega, D.; Vicente, R.; Vieira, D.N.; Ross, A.H.; Cunha, E. Sex estimation from the tarsal bones in a Portuguese sample: A machine learning approach. Int. J. Leg. Med. 2015, 129, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Buikstra, J.E. Standards for data collection from human skeletal remains. Ark. Archaeol. Surv. Res. Ser. 1994, 44. [Google Scholar] [CrossRef]
- Krishan, K.; Chatterjee, P.M.; Kanchan, T.; Kaur, S.; Baryah, N.; Singh, R. A review of sex estimation techniques during examination of skeletal remains in forensic anthropology casework. Forensic Sci. Int. 2016, 261, 165.e1–165.e8. [Google Scholar] [CrossRef]
- Sierp, I.; Henneberg, M. The Difficulty of Sexing Skeletons from Unknown Populations. J. Anthropol. 2015, 2015, 1–13. [Google Scholar] [CrossRef]
- Darmawan, M.F.; Yusuf, S.M.; Rozi, M.A.; Haron, H. Hybrid PSOANN for sex estimation based on length of left hand bone. In Proceedings of the 2015 IEEE Student Conference on Research and Development (SCOReD), Kuala Lumpur, Malaysia, 13–14 December 2015; pp. 478–483. [Google Scholar]
- Bewes, J.; Low, A.; Morphett, A.; Pate, F.D.; Henneberg, M. Artificial intelligence for sex determination of skeletal remains: Application of a deep learning artificial neural network to human skulls. J. Forensic Leg. Med. 2019, 62, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Kaloi, M.A.; He, K. Child Gender Determination with Convolutional Neural Networks on Hand Radio-Graphs. arXiv 2018, arXiv:1811.05180. [Google Scholar]
- Mahfouz, M.; Badawi, A.; Merkl, B.; Fatah, E.E.A.; Pritchard, E.; Kesler, K.; Moore, M.; Jantz, R.; Jantz, L. Patella sex determination by 3D statistical shape models and nonlinear classifiers. Forensic Sci. Int. 2007, 173, 161–170. [Google Scholar] [CrossRef]
- Yang, W.; Liu, X.; Wang, K.; Hu, J.; Geng, G.; Feng, J. Sex determination of three-dimensional skull based on improved backpropagation neural network. Comput. Math. Methods Med. 2019, 2019, 9163547. [Google Scholar] [CrossRef]
- Arigbabu, O.A.; Liao, I.Y.; Abdullah, N.; Noor, M.H.M. Can computer vision techniques be applied to automated forensic examinations? A study on sex identification from human skulls using head CT scans. In Proceedings of the Asian Conference on Computer Vision, Taipei, Taiwan, 20–24 November 2016; pp. 342–359. [Google Scholar]
- Tanner, J.M.; Whitehouse, R.; Cameron, N.; Marshall, W.; Healy, M.; Goldstein, H. Assessment of Skeletal Maturity and Prediction of Adult Height (TW2 Method); Saunders: London, UK, 2001. [Google Scholar]
- Prieto, J.; Mihaila, S.; Hilaire, A.; Fanton, L.; Odet, C.; Revol-Muller, C. Age estimation from 3D X-ray CT images of human fourth ribs. In Proceedings of the International Conference on Image Processing, Computer Vision, and Pattern Recognition (IPCV), Las Vegas, NV, USA, 16–19 July 2012; p. 1. [Google Scholar]
- Breen, M.A.; Tsai, A.; Stamm, A.; Kleinman, P.K. Bone age assessment practices in infants and older children among Society for Pediatric Radiology members. Pediatr. Radiol. 2016, 46, 1269–1274. [Google Scholar] [CrossRef]
- Malina, R.M.; Beunen, G.P. Assessment of skeletal maturity and prediction of adult height (TW3 method). Am. J. Hum. Biol. 2002, 14, 788–789. [Google Scholar] [CrossRef]
- Pinchi, V.; De Luca, F.; Ricciardi, F.; Focardi, M.; Piredda, V.; Mazzeo, E.; Norelli, G.A. Skeletal age estimation for forensic purposes: A comparison of GP, TW2 and TW3 methods on an Italian sample. Forensic Sci. Int. 2014, 238, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.R.; Shim, W.H.; Yoon, H.M.; Hong, S.H.; Lee, J.S.; Cho, Y.A.; Kim, S. Computerized Bone Age Estimation Using Deep Learning Based Program: Evaluation of the Accuracy and Efficiency. Am. J. Roentgenol. 2017, 209, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Larson, D.B.; Chen, M.C.; Lungren, M.P.; Halabi, S.S.; Stence, N.V.; Langlotz, C.P. Performance of a deep-learning neural network model in assessing skeletal maturity on pediatric hand radiographs. Radiology 2018, 287, 313–322. [Google Scholar] [CrossRef]
- Lee, H.; Tajmir, S.; Lee, J.; Zissen, M.; Yeshiwas, B.A.; Alkasab, T.K.; Choy, G.; Do, S. Fully automated deep learning system for bone age assessment. J. Digit. Imaging 2017, 30, 427–441. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, K.G. Applying Deep Learning in Medical Images: The Case of Bone Age Estimation. Healthc. Inform. Res. 2018, 24, 86–92. [Google Scholar] [CrossRef]
- Mutasa, S.; Chang, P.D.; Ruzal-Shapiro, C.; Ayyala, R. MABAL: A Novel Deep-Learning Architecture for Machine-Assisted Bone Age Labeling. J. Digit. Imaging 2018, 31, 513–519. [Google Scholar] [CrossRef]
- Hsieh, C.W.; Jong, T.L.; Chou, Y.H.; Tiu, C.M. Computerized geometric features of carpal bone for bone age estimation. Chin. Med. J. 2007, 1, 767–770. [Google Scholar] [CrossRef]
- Mansourvar, M.; Asemi, A.; Raj, R.G.; Kareem, S.A.; Antony, C.D.; Idris, N.; Baba, M.S. A fuzzy inference system for skeletal age assessment in living individual. Int. J. Fuzzy Syst. 2017, 19, 838–848. [Google Scholar] [CrossRef]
- Spampinato, C.; Palazzo, S.; Giordano, D.; Aldinucci, M.; Leonardi, R. Deep learning for automated skeletal bone age assessment in X-ray images. Med. Image Anal. 2017, 36, 41–51. [Google Scholar] [CrossRef]
- Rucci, M.; Coppini, G.; Nicoletti, I.; Cheli, D.; Valli, G. Automatic analysis of hand radiographs for the assessment of skeletal age: A subsymbolic approach. Comput. Biomed. Res. 1995, 28, 239–256. [Google Scholar] [CrossRef] [PubMed]
- Gross, G.W.; Boone, J.M.; Bishop, D.M. Pediatric skeletal age: Determination with neural networks. Radiology 1995, 195, 689–695. [Google Scholar] [CrossRef]
- Mahmoodi, S.; Sharif, B.S.; Chester, E.G.; Owen, J.P.; Lee, R. Skeletal growth estimation using radiographic image processing and analysis. IEEE Trans. Inf. Technol. Biomed. 2000, 4, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Gertych, A.; Zhang, A.; Sayre, J.; Pospiech-Kurkowska, S.; Huang, H. Bone age assessment of children using a digital hand atlas. Comput. Med. Imaging Graph. 2007, 31, 322–331. [Google Scholar] [CrossRef]
- Gertych, A.; Piętka, E.; Liu, B.J. Segmentation of regions of interest and post-segmentation edge location improvement in computer-aided bone age assessment. Pattern Anal. Appl. 2007, 10, 115–123. [Google Scholar] [CrossRef]
- Hsieh, C.; Jong, T.; Tiu, C. Bone age estimation based on phalanx information with fuzzy constrain of carpals. Med. Biol. Eng. Comput. 2007, 45, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Gertych, A.; Liu, B.J. Automatic bone age assessment for young children from newborn to 7-year-old using carpal bones. Comput. Med. Imaging Graph. 2007, 31, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Qi, J.; Liu, Z.; Ning, Q.; Luo, X. Automatic bone age assessment based on intelligent algorithms and comparison with TW3 method. Comput. Med. Imaging Graph. 2008, 32, 678–684. [Google Scholar] [CrossRef]
- Tristán-Vega, A.; Arribas, J.I. A radius and ulna TW3 bone age assessment system. IEEE Trans. Biomed. Eng. 2008, 55, 1463–1476. [Google Scholar] [CrossRef] [PubMed]
- Thodberg, H.H.; Kreiborg, S.; Juul, A.; Pedersen, K.D. The BoneXpert method for automated determination of skeletal maturity. IEEE Trans. Med. Imaging 2009, 28, 52–66. [Google Scholar] [CrossRef]
- Thodberg, H.H. An automated method for determination of bone age. J. Clin. Endocrinol. Metab. 2009, 94, 2239–2244. [Google Scholar] [CrossRef] [PubMed]
- Giordano, D.; Spampinato, C.; Scarciofalo, G.; Leonardi, R. An Automatic System for Skeletal Bone Age Measurement by Robust Processing of Carpal and Epiphysial/Metaphysial Bones. IEEE Trans. Instrum. Meas. 2010, 59, 2539–2553. [Google Scholar] [CrossRef]
- Martin, D.D.; Meister, K.; Schweizer, R.; Ranke, M.B.; Thodberg, H.H.; Binder, G. Validation of automatic bone age rating in children with precocious and early puberty. J. Pediatr. Endocrinol. Metab. 2011, 24, 1009–1014. [Google Scholar] [CrossRef]
- Davis, L.M.; Theobald, B.; Bagnall, A.J. Automated Bone Age Assessment Using Feature Extraction. In Intelligent Data Engineering and Automated Learning (IDEAL); Yin, H., Costa, J.A.F., Barreto, G.D.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 7435, pp. 43–51. [Google Scholar]
- Mansourvar, M.; Raj, R.G.; Ismail, M.A.; Kareem, S.A.; Shanmugam, S.; Wahid, S.; Mahmud, R.; Abdullah, R.H.; Nasaruddin, F.H.F.; Idris, N. Automated web based system for bone age assessment using histogram technique. Malays. J. Comput. Sci. 2012, 25, 107–121. [Google Scholar]
- Lin, H.; Shu, S.; Lin, Y.; Yu, S. Bone age cluster assessment and feature clustering analysis based on phalangeal image rough segmentation. Pattern Recognit. 2012, 45, 322–332. [Google Scholar] [CrossRef]
- Adeshina, S.A.; Lindner, C.; Cootes, T.F. Automatic segmentation of carpal area bones with random forest regression voting for estimating skeletal maturity in infants. In Proceedings of the 2014 11th International Conference on Electronics, Computer and Computation (ICECCO), Abuja, Nigeria, 29 September–1 October 2014; pp. 1–4. [Google Scholar]
- Stern, D.; Urschler, M. From individual hand bone age estimates to fully automated age estimation via learning-based information fusion. In Proceedings of the IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016; pp. 150–154. [Google Scholar]
- Giordano, D.; Kavasidis, I.; Spampinato, C. Modeling skeletal bone development with hidden Markov models. Comput. Methods Progr. Biomed. 2016, 124, 138–147. [Google Scholar] [CrossRef]
- Kashif, M.; Deserno, T.M.; Haak, D.; Jonas, S.M. Feature description with SIFT, SURF, BRIEF, BRISK, or FREAK? A general question answered for bone age assessment. Comput. Biol. Med. 2016, 68, 67–75. [Google Scholar] [CrossRef]
- Seok, J.; Kasa-Vubu, J.; DiPietro, M.A.; Girard, A.R. Expert system for automated bone age determination. Expert Syst. Appl. 2016, 50, 75–88. [Google Scholar] [CrossRef]
- Li, Y.; Huang, Z.; Dong, X.; Liang, W.; Xue, H.; Zhang, L.; Zhang, Y.; Deng, Z. Forensic age estimation for pelvic X-ray images using deep learning. Eur. Radiol. 2019, 29, 2322–2329. [Google Scholar] [CrossRef]
- Štern, D.; Payer, C.; Urschler, M. Automated age estimation from MRI volumes of the hand. Med. Image Anal. 2019, 58, 101538. [Google Scholar] [CrossRef]
- Thodberg, H.H.; Neuhof, J.; Ranke, M.B.; Jenni, O.G.; Martin, D.D. Validation of bone age methods by their ability to predict adult height. Horm. Res. Paediatr. 2010, 74, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Mesejo, P.; Pizarro, D.; Abergel, A.; Rouquette, O.; Beorchia, S.; Poincloux, L.; Bartoli, A. Computer-aided classification of gastrointestinal lesions in regular colonoscopy. IEEE Trans. Med. Imaging 2016, 35, 2051–2063. [Google Scholar] [CrossRef] [PubMed]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. J. Am. Med. Assoc. 2016, 316, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Kooi, T.; Litjens, G.; Van Ginneken, B.; Gubern-Mérida, A.; Sánchez, C.I.; Mann, R.; den Heeten, A.; Karssemeijer, N. Large scale deep learning for computer aided detection of mammographic lesions. Med. Image Anal. 2017, 35, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Hua, K.L.; Hsu, C.H.; Hidayati, S.C.; Cheng, W.H.; Chen, Y.J. Computer-aided classification of lung nodules on computed tomography images via deep learning technique. OncoTargets Therapy 2015, 8, 2015–2022. [Google Scholar] [PubMed]
- Franchi, A. Epidemiology and classification of bone tumors. Clin. Cases Miner. Bone Metab. 2012, 9, 92. [Google Scholar]
- Olczak, J.; Fahlberg, N.; Maki, A.; Razavian, A.S.; Jilert, A.; Stark, A.; Sköldenberg, O.; Gordon, M. Artificial intelligence for analyzing orthopedic trauma radiographs: Deep learning algorithms—Are they on par with humans for diagnosing fractures? Acta Orthop. 2017, 88, 581–586. [Google Scholar] [CrossRef]
- Chung, S.W.; Han, S.S.; Lee, J.W.; Oh, K.S.; Kim, N.R.; Yoon, J.P.; Kim, J.Y.; Moon, S.H.; Kwon, J.; Lee, H.J.; et al. Automated detection and classification of the proximal humerus fracture by using deep learning algorithm. Acta Orthop. 2018, 89, 468–473. [Google Scholar] [CrossRef]
- Gupta, A.; Venkatesh, S.; Chopra, S.; Ledig, C. Generative image translation for data augmentation of bone lesion pathology. arXiv 2019, arXiv:1902.02248. [Google Scholar]
- Sandström, S.; Ostensen, H.; Pettersson, H.; Åkerman, K. The WHO Manual of Diagnostic Imaging: Radiographic Technique and Projections; World Health Organization: Brussels, Belgium, 2003; Volume 2. [Google Scholar]
- Daffner, R.H.; Hartman, M. Clinical Radiology: The Essentials; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Rigby, D.; Hacking, L. Interpreting the chest radiograph. Anaesth Intensive Care 2018, 19, 50–54. [Google Scholar] [CrossRef]
- Van Ginneken, B.; Romeny, B.T.H.; Viergever, M.A. Computer-aided diagnosis in chest radiography: A survey. IEEE Trans. Med. Imaging 2001, 20, 1228–1241. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.M. Assessing the variation in individual frontal sinus outlines. Am. J. Phys. Anthropol. 2005, 127, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.M. Testing the reliability of frontal sinuses in positive identification. J. Forensic Sci. 2005, 50, 18–22. [Google Scholar] [CrossRef]
- Maxwell, A.B.; Ross, A.H. A radiographic study on the utility of cranial vault outlines for positive identifications. J. Forensic Sci. 2014, 59, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.K.; Chen, H. Matching of dental X-ray images for human identification. Pattern Recognit. 2004, 37, 1519–1532. [Google Scholar] [CrossRef]
- Chen, H.; Jain, A.K. Dental biometrics: Alignment and matching of dental radiographs. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Nomir, O.; Abdel-Mottaleb, M. Human identification from dental x-ray images based on the shape and appearance of the teeth. IEEE Trans. Inf. Forensics Secur. 2007, 2, 188–197. [Google Scholar] [CrossRef]
- Caple, J.; Byrd, J.; Stephan, C.N. Elliptical fourier analysis: Fundamentals, applications, and value for forensic anthropology. Int. J. Leg. Med. 2017, 131, 1675–1690. [Google Scholar] [CrossRef]
- Devi, P.; Thimmarasa, V.; Mehrotra, V.; Singla, V. Automated dental identification system: An aid to forensic odontology. J. Indian Acad. Oral Med. Radiol. 2011, 23, 360. [Google Scholar] [CrossRef]
- Anuja, P.; Doggalli, N. Software in forensic odontology. Indian J. Multidiscip. Dent. 2018, 8, 94. [Google Scholar]
- Derrick, S.M.; Hipp, J.A.; Goel, P. The Computer-Assisted Decedent Identification Method of Computer-Assisted Radiographic Identification. In New Perspectives in Forensic Human Skeletal Identification; Academic Press: Cambridge, MA, USA, 2018; pp. 265–276. [Google Scholar]
- Tabor, Z.; Karpisz, D.; Wojnar, L.; Kowalski, P. An automatic recognition of the frontal sinus in x-ray images of skull. IEEE Trans. Biomed. Eng. 2008, 56, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Pfaeffli, M.; Vock, P.; Dirnhofer, R.; Braun, M.; Bolliger, S.A.; Thali, M.J. Post-mortem radiological CT identification based on classical ante-mortem X-ray examinations. Forensic Sci. Int. 2007, 171, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Shinkawa, N.; Hirai, T.; Nishii, R.; Yukawa, N. Usefulness of 2D fusion of postmortem CT and antemortem chest radiography studies for human identification. Jpn. J. Radiol. 2017, 35, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Niespodziewanski, E.; Stephan, C.N.; Guyomarc’h, P.; Fenton, T.W. Human Identification via Lateral Patella Radiographs: A Validation Study. J. Forensic Sci. 2016, 61, 134–140. [Google Scholar] [CrossRef] [PubMed]
- D’Alonzo, S.S.; Guyomarc’h, P.; Byrd, J.E.; Stephan, C.N. A Large-Sample Test of a Semi-Automated Clavicle Search Engine to Assist Skeletal Identification by Radiograph Comparison. J. Forensic Sci. 2017, 62, 181–186. [Google Scholar] [CrossRef]
- Gómez, O.; Ibáñez, O.; Valsecchi, A.; Cordón, O.; Kahana, T. 3D-2D silhouette-based image registration for comparative radiography-based forensic identification. Pattern Recognit. 2018, 83, 469–480. [Google Scholar] [CrossRef]
- Thali, M.J.; Brogdon, B.; Viner, M.D. Forensic Radiology; CRC Press: Boca Raton, FL, USA, 2002. [Google Scholar]
- Gómez, O.; Mesejo, P.; Ibáñez, O.; Valsecchi, A.; Cordón, O. Deep architectures for high-resolution multi-organ chest X-ray image segmentation. Neural Comput. Appl. 2019, 1–15. [Google Scholar] [CrossRef]
- Gómez, Ó.; Mesejo, P.; Ibáñez, Ó.; Cordón, Ó. Deep architectures for the segmentation of frontal sinuses in XRay images: Towards an automatic forensic identification system in comparative radiography. Neurcomputing 2020, in press. [Google Scholar]
- Gómez, Ó.; Mesejo, P.; Ibáñez, Ó.; Valsecchi, A.; Cordón, Ó. A real-coded evolutionary algorithm-based registration approach for forensic identification using the radiographic comparison of frontal sinuses. In Proceedings of the 22nd IEEE Congress on Evolutionary Computation (IEEE CEC), Glasgow, UK, 19–24 July 2020. [Google Scholar]
- Iino, M.; Fujimoto, H.; Yoshida, M.; Matsumoto, H.; Fujita, M.Q. Identification of a jawless skull by superimposing post-mortem and ante-mortem CT. J. Forensic Radiol. Imaging 2016, 6, 31–37. [Google Scholar] [CrossRef]
- Ruder, T.D.; Brun, C.; Christensen, A.M.; Thali, M.J.; Gascho, D.; Schweitzer, W.; Hatch, G.M. Comparative radiologic identification with CT images of paranasal sinuses—Development of a standardized approach. J. Forensic Radiol. Imaging 2016, 7, 1–9. [Google Scholar] [CrossRef]
- Hacl, A.; Costa, A.L.F.; Oliveira, J.M.; Tucunduva, M.J.; Girondi, J.R.; Nahás-Scocate, A.C.R. Three-dimensional volumetric analysis of frontal sinus using medical software. J. Forensic Radiol. Imaging 2017, 11, 1–5. [Google Scholar] [CrossRef]
- Deloire, L.; Diallo, I.; Cadieu, R.; Auffret, M.; Alavi, Z.; Ognard, J.; Ben Salem, D. Post-mortem X-ray computed tomography (PMCT) identification using ante-mortem CT-scan of the sphenoid sinus. J. Neuroradiol. 2019, 46, 248–255. [Google Scholar] [CrossRef]
- Zhong, X.; Yu, D.; Foong, K.W.; Sim, T.; San Wong, Y.; Cheng, H.L. Towards automated pose invariant 3D dental biometrics. In Proceedings of the 2011 International Joint Conference on Biometrics (IJCB), Washington, DC, USA, 11–13 October 2011; pp. 1–7. [Google Scholar]
- Zhong, X.; Yu, D.; Wong, Y.S.; Sim, T.; Lu, W.F.; Foong, K.W.C.; Cheng, H.L. 3D dental biometrics: Alignment and matching of dental casts for human identification. Comput. Ind. 2013, 64, 1355–1370. [Google Scholar] [CrossRef]
- Zhang, Z.; Ong, S.H.; Zhong, X.; Foong, K.W.C. Efficient 3D dental identification via signed feature histogram and learning keypoint detection. Pattern Recognit. 2016, 60, 189–204. [Google Scholar] [CrossRef]
- Gibelli, D.; Cellina, M.; Cappella, A.; Gibelli, S.; Panzeri, M.M.; Oliva, A.G.; Termine, G.; De Angelis, D.; Cattaneo, C.; Sforza, C. An innovative 3D-3D superimposition for assessing anatomical uniqueness of frontal sinuses through segmentation on CT scans. Int. J. Leg. Med. 2019, 133, 1159–1165. [Google Scholar] [CrossRef]
- Decker, S.J.; Ford, J.M. Forensic personal identification utilizing part-to-part comparison of CT-derived 3D lumbar models. Forensic Sci. Int. 2019, 294, 21–26. [Google Scholar] [CrossRef]
- Dirnhofer, R.; Jackowski, C.; Vock, P.; Potter, K.; Thali, M.J. VIRTOPSY: Minimally invasive, imaging-guided virtual autopsy. Radiographics 2006, 26, 1305–1333. [Google Scholar] [CrossRef]
- O’Sullivan, S.; Holzinger, A.; Zatloukal, K.; Saldiva, P.; Sajid, M.I.; Wichmann, D. Machine learning enhanced virtual autopsy. Autopsy Case Rep. 2017, 7, 3. [Google Scholar] [CrossRef]
- O’Sullivan, S.; Holzinger, A.; Wichmann, D.; Saldiva, P.H.N.; Sajid, M.I.; Zatloukal, K. Virtual autopsy: Machine learning and ai provide new opportunities for investigating minimal tumor burden and therapy resistance by cancer patients. Autopsy Case Rep. 2018, 8, e2018003. [Google Scholar] [CrossRef]
- O’Sullivan, S.; Heinsen, H.; Grinberg, L.T.; Chimelli, L.; Amaro, E.; do Nascimento Saldiva, P.H.; Jeanquartier, F.; Jean-Quartier, C.; Martin, M.d.G.M.; Sajid, M.I.; et al. The role of artificial intelligence and machine learning in harmonization of high-resolution post-mortem MRI (virtopsy) with respect to brain microstructure. Brain Inform. 2019, 6, 3. [Google Scholar] [CrossRef][Green Version]
- Holzinger, A. Interactive machine learning for health informatics: When do we need the human-in-the-loop? Brain Inform. 2016, 3, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Kelliher, T.; Leue, B.; Lorensen, B.; Lauric, A. Computer-Aided Forensics: Metal Object Detection. Stud. Health Technol. Inform. 2006, 119, 249. [Google Scholar] [PubMed]
- Ebert, L.C.; Heimer, J.; Schweitzer, W.; Sieberth, T.; Leipner, A.; Thali, M.; Ampanozi, G. Automatic detection of hemorrhagic pericardial effusion on PMCT using deep learning—A feasibility study. Forensic Sci. Med. Pathol. 2017, 13, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Peña-Solórzano, C.; Albrecht, D.; Harris, P.; Bassed, R.; Gillam, J.; Dimmock, M. Semi-supervised labelling of the femur in a whole-body post-mortem CT database using deep learning. Comput. Biol. Med. 2020, 122, 103797. [Google Scholar] [CrossRef]
- Nickerson, B.A.; Fitzhorn, P.A.; Koch, S.K.; Charney, M. A methodology for near-optimal computational superimposition of two-dimensional digital facial photographs and three-dimensional cranial surface meshes. J. Forensic Sci. 1991, 36, 480–500. [Google Scholar] [CrossRef]
- Yoshino, M.; Imaizumi, K.; Miyasaka, S.; Seta, S. Evaluation of anatomical consistency in craniofacial superimposition images. Forensic Sci. Int. 1995, 74, 125–134. [Google Scholar] [CrossRef]
- Yoshino, M.; Matsuda, H.; Kubota, S.; Imaizumi, K.; Miyasaka, S.; Seta, S. Computer assisted skull identification system using video superimposition. Forensic Sci. Int. 1997, 90, 231–244. [Google Scholar] [CrossRef]
- Ghosh, A.; Sinha, P. An economised craniofacial identification system. Forensic Sci. Int. 2001, 117, 109–119. [Google Scholar] [CrossRef]
- Santamaría, J.; Cordón, O.; Damas, S. Evolutionary approaches for automatic 3D modeling of skulls in forensic identification. In Workshops on Applications of Evolutionary Computation; Springer: Berlin/Heidelberg, Germany, 2007; pp. 415–422. [Google Scholar]
- Santamaría, J.; Cordón, O.; Damas, S.; García-Torres, J.M.; Quirin, A. Performance evaluation of memetic approaches in 3D reconstruction of forensic objects. Soft Comput. 2009, 13, 883–904. [Google Scholar] [CrossRef]
- Ballerini, L.; Cordón, O.; Damas, S.; Santamaría, J. Automatic 3D modeling of skulls by scatter search and heuristic features. In Applications of Soft Computing. Updating the State of the Art; Avineri, E., Koepen, M., Dahal, K., Sunitiyoso, Y., Roy, R., Eds.; Springer: Berlin, Germany, 2009; pp. 149–158. [Google Scholar]
- Ibáñez, O.; Ballerini, L.; Cordón, O.; Damas, S.; Santamaría, J. An experimental study on the applicability of evolutionary algorithms to craniofacial superimposition in forensic identification. Inf. Sci. 2009, 179, 3998–4028. [Google Scholar] [CrossRef]
- Ibánez, O.; Cordon, Ó.; Damas, S.; Santamaria, J. Modeling the skull–face overlay uncertainty using fuzzy sets. IEEE Trans. Fuzzy Syst. 2011, 19, 946–959. [Google Scholar]
- Campomanes-Álvarez, B.R.; Cordón, O.; Damas, S. Evolutionary multiobjective optimization for mesh simplification of 3d open models. Integr. Comput. Aided Eng. 2013, 20, 375–390. [Google Scholar] [CrossRef]
- Duan, F.; Yang, Y.; Li, Y.; Tian, Y.; Lu, K.; Wu, Z.; Zhou, M. Skull identification via correlation measure between skull and face shape. IEEE Trans. Inf. Forensics Secur. 2014, 9, 1322–1332. [Google Scholar] [CrossRef]
- Campomanes-Álvarez, B.R.; Ibánez, O.; Campomanes-Álvarez, C.; Damas, S.; Cordón, O. Modeling facial soft tissue thickness for automatic skull-face overlay. IEEE Trans. Inf. Forensics Secur. 2015, 10, 2057–2070. [Google Scholar] [CrossRef]
- Campomanes-Alvarez, C.; Ibáñez, O.; Cordón, O. Design of criteria to assess craniofacial correspondence in forensic identification based on computer vision and fuzzy integrals. Appl. Soft Comput. 2016, 46, 596–612. [Google Scholar] [CrossRef]
- Bermejo, E.; Campomanes-Álvarez, C.; Valsecchi, A.; Ibáñez, O.; Damas, S.; Cordón, O. Genetic algorithms for skull-face overlay including mandible articulation. Inf. Sci. 2017, 420, 200–217. [Google Scholar] [CrossRef]
- Nagpal, S.; Singh, M.; Jain, A.; Singh, R.; Vatsa, M.; Noore, A. On matching skulls to digital face images: A preliminary approach. In Proceedings of the 2017 IEEE International Joint Conference on Biometrics (IJCB), Denver, CO, USA, 1–4 October 2017; pp. 813–819. [Google Scholar]
- Singh, M.; Nagpal, S.; Singh, R.; Vatsa, M.; Noore, A. Learning a shared transform model for skull to digital face image matching. In Proceedings of the 2018 IEEE 9th International Conference on Biometrics Theory, Applications and Systems (BTAS), Los Angeles, CA, USA, 22–25 October 2018; pp. 1–7. [Google Scholar]
- Campomanes-Alvarez, C.; Ibáñez, O.; Cordón, O.; Wilkinson, C. Hierarchical information fusion for decision making in craniofacial superimposition. Inf. Fusion 2018, 39, 25–40. [Google Scholar] [CrossRef]
- Campomanes-Alvarez, C.; Martos-Fernández, R.; Wilkinson, C.; Ibánez, O.; Cordón, O. Modeling skull-face anatomical/morphological correspondence for craniofacial superimposition-based identification. IEEE Trans. Inf. Forensics Secur. 2018, 13, 1481–1494. [Google Scholar] [CrossRef]
- Valsecchi, A.; Damas, S.; Cordón, O. A Robust and Efficient Method for Skull-Face Overlay in Computerized Craniofacial Superimposition. IEEE Trans. Inf. Forensics Secur. 2018, 13, 1960–1974. [Google Scholar] [CrossRef]
- Faria-Porto, L.; Correia-Lima, L.; Flores, M.; Valsecchi, A.; Ibáñez, O.; Machado-Palharese, C.; de Barros-Vidala, F. Automatic cephalometric landmarks detection on frontal faces: An approach based on supervised learning techniques. Digit. Investig. 2019, 30, 108–116. [Google Scholar] [CrossRef]
- San Tan, J.; Liao, I.Y.; Venkat, I.; Belaton, B.; Jayaprakash, P. Computer-aided superimposition via reconstructing and matching 3D faces to 3D skulls for forensic craniofacial identifications. Vis. Comput. 2019, 1–15. [Google Scholar] [CrossRef]
- Park, H.K.; Chung, J.W.; Kho, H.S. Use of hand-held laser scanning in the assessment of craniometry. Forensic Sci. Int. 2006, 160, 200–206. [Google Scholar] [CrossRef]
- Cummaudo, M.; Guerzoni, M.; Marasciuolo, L.; Gibelli, D.; Cigada, A.; Obertovà, Z.; Ratnayake, M.; Poppa, P.; Gabriel, P.; Ritz-Timme, S.; et al. Pitfalls at the root of facial assessment on photographs: A quantitative study of accuracy in positioning facial landmarks. Int. J. Leg. Med. 2013, 127, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Austin-Smith, D.; Maples, W.R. The reliability of skull/photograph superimposition in individual identification. J. Forensic Sci. 1994, 39, 446–455. [Google Scholar] [CrossRef]
- Jayaprakash, P.T.; Srinivasan, G.J.; Amravaneswaran, M.G. Cranio-facial morphoanalysis: A new method for enhancing reliability while identifying skulls by photo superimposition. Forensic Sci. Int. 2001, 117, 121–143. [Google Scholar] [CrossRef]
- Pesce Delfino, V.; Vacca, E.; Potente, F.; Lettini, T.; Colonna, M. Shape analytical morphometry in computer-aided skull identification via video superimposition. In Forensic Analysis of the Skull: Craniofacial Analysis, Reconstruction and Identification; Wiley: New York, NY, USA, 1993; pp. 131–159. [Google Scholar]
- Ricci, A.; Marella, G.L.; Apostol, M.A. A new experimental approach to computer-aided face/skull identification in forensic anthropology. Am. J. Forensic Med. Pathol. 2006, 27, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, O.; Vicente, R.; Navega, D.; Wilkinson, C.; Jayaprakash, P.; Huete, M.; Briers, T.; Hardiman, R.; Navarro, F.; Ruiz, E.; et al. Study on the performance of different craniofacial superimposition approaches (I). Forensic Sci. Int. 2015, 257, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Vandermeulen, D.; Claes, P.; Loeckx, D.; De Greef, S.; Willems, G.; Suetens, P. Computerized craniofacial reconstruction using CT-derived implicit surface representations. Forensic Sci. Int. 2006, 159, S164–S174. [Google Scholar] [CrossRef]
- Vandermeulen, D.; Claes, P.; De Greef, S.; Willems, G.; Clement, J.; Suetens, P. Automated facial reconstruction. Craniofacial Identif. 2012, 203. [Google Scholar] [CrossRef]
- Tu, P.; Book, R.; Liu, X.; Krahnstoever, N.; Adrian, C.; Williams, P. Automatic face recognition from skeletal remains. In Proceedings of the 2007 IEEE Conference on Computer Vision and Pattern Recognition, Minneapolis, MN, USA, 17–22 June 2007; pp. 1–7. [Google Scholar]
- Liu, C.; Li, X. Superimposition-guided facial reconstruction from skull. arXiv 2018, arXiv:1810.00107. [Google Scholar]
- Imaizumi, K.; Taniguchi, K.; Ogawa, Y.; Matsuzaki, K.; Maekawa, H.; Nagata, T.; Moriyama, T.; Okuda, I.; Hayakawa, H.; Shiotani, S. Development of three-dimensional facial approximation system using head CT scans of Japanese living individuals. J. Forensic Radiol. Imaging 2019, 17, 36–45. [Google Scholar] [CrossRef]
- Mesejo, P.; Ibáñez, O.; Cordón, O.; Cagnoni, S. A survey on image segmentation using metaheuristic-based deformable models: State of the art and critical analysis. Appl. Soft Comput. 2016, 44, 1–29. [Google Scholar] [CrossRef]
- Claes, P.; Liberton, D.K.; Daniels, K.; Rosana, K.M.; Quillen, E.E.; Pearson, L.N.; McEvoy, B.; Bauchet, M.; Zaidi, A.A.; Yao, W.; et al. Modeling 3D facial shape from DNA. PLoS Genet. 2014, 10, e1004224. [Google Scholar] [CrossRef]
- Claes, P.; Roosenboom, J.; White, J.D.; Swigut, T.; Sero, D.; Li, J.; Lee, M.K.; Zaidi, A.; Mattern, B.C.; Liebowitz, C.; et al. Genome-wide mapping of global-to-local genetic effects on human facial shape. Nat. Genet. 2018, 50, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Frudakis, T. Molecular Photofitting: Predicting Ancestry and Phenotype Using DNA; Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Kayser, M.; Schneider, P.M. DNA-based prediction of human externally visible characteristics in forensics: Motivations, scientific challenges, and ethical considerations. Forensic Sci. Int. Genet. 2009, 3, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Sulem, P.; Gudbjartsson, D.F.; Stacey, S.N.; Helgason, A.; Rafnar, T.; Magnusson, K.P.; Manolescu, A.; Karason, A.; Palsson, A.; Thorleifsson, G.; et al. Genetic determinants of hair, eye and skin pigmentation in Europeans. Nat. Genet. 2007, 39, 1443. [Google Scholar] [CrossRef]
- Walsh, S.; Liu, F.; Ballantyne, K.N.; van Oven, M.; Lao, O.; Kayser, M. IrisPlex: A sensitive DNA tool for accurate prediction of blue and brown eye colour in the absence of ancestry information. Forensic Sci. Int. Genet. 2011, 5, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Rollo, R.; Ovenden, J.; Dudgeon, C.; Bennett, M.; Tucker, K.; Stephan, C. The utility of the IrisPlex system for estimating iris colour of Australians from their DNA. Forensic Sci. Int. 2018, 7, 98–115. [Google Scholar]
- Pneuman, A.; Budimlija, Z.M.; Caragine, T.; Prinz, M.; Wurmbach, E. Verification of eye and skin color predictors in various populations. Leg. Med. 2012, 14, 78–83. [Google Scholar] [CrossRef]
- Walsh, S.; Wollstein, A.; Liu, F.; Chakravarthy, U.; Rahu, M.; Seland, J.H.; Soubrane, G.; Tomazzoli, L.; Topouzis, F.; Vingerling, J.R.; et al. DNA-based eye colour prediction across Europe with the IrisPlex system. Forensic Sci. Int. Genet. 2012, 6, 330–340. [Google Scholar] [CrossRef]
- Kastelic, V.; Pośpiech, E.; Draus-Barini, J.; Branicki, W.; Drobnič, K. Prediction of eye color in the Slovenian population using the IrisPlex SNPs. Croat. Med. J. 2013, 54, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Spichenok, O.; Budimlija, Z.M.; Mitchell, A.A.; Jenny, A.; Kovacevic, L.; Marjanovic, D.; Caragine, T.; Prinz, M.; Wurmbach, E. Prediction of eye and skin color in diverse populations using seven SNPs. Forensic Sci. Int. Genet. 2011, 5, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Maroñas, O.; Phillips, C.; Söchtig, J.; Gomez-Tato, A.; Cruz, R.; Alvarez-Dios, J.; de Cal, M.C.; Ruiz, Y.; Fondevila, M.; Carracedo, Á.; et al. Development of a forensic skin colour predictive test. Forensic Sci. Int. Genet. 2014, 13, 34–44. [Google Scholar] [CrossRef]
- Ibáñez, Ó.; Corbal, I.; Gómez, I.; Gómez, Ó.; González, A.; Macías, M.; Prada, K.; Valsecchi, A.; Mesejo, P. Skeleton-ID: Artificial Intelligence at the service of Forensic Anthropology. In Proceedings of the 11th International Scientific Meeting of the Spanish Association of Forensic Anthropology and Odontology (AEAOF), Pastrana, Spain, 8–10 November 2019. [Google Scholar]
- Edgar, H.; Daneshvari Berry, S.; Moes, E.; Adolphi, N.; Bridges, P.; Nolte, K. New Mexico Decedent Image Database; Office of the Medical Investigator, University of New Mexico: Albuquerque, NM, USA, 2020. [Google Scholar]
- Halabi, S.S.; Prevedello, L.M.; Kalpathy-Cramer, J.; Mamonov, A.B.; Bilbily, A.; Cicero, M.; Pan, I.; Pereira, L.A.; Sousa, R.T.; Abdala, N.; et al. The RSNA pediatric bone age machine learning challenge. Radiology 2019, 290, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. Chestx-ray8: Hospital-scale chest x-ray database and benchmarks on weakly-supervised classification and localization of common thorax diseases. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2097–2106. [Google Scholar]
- Brinker, T.J.; Hekler, A.; Enk, A.H.; Klode, J.; Hauschild, A.; Berking, C.; Schilling, B.; Haferkamp, S.; Schadendorf, D.; Holland-Letz, T.; et al. Deep learning outperformed 136 of 157 dermatologists in a head-to-head dermoscopic melanoma image classification task. Eur. J. Cancer 2019, 113, 47–54. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Lein, E.S.; Hawrylycz, M.J.; Ao, N.; Ayres, M.; Bensinger, A.; Bernard, A.; Boe, A.F.; Boguski, M.S.; Brockway, K.S.; Byrnes, E.J.; et al. Genome-wide atlas of gene expression in the adult mouse brain. Nature 2007, 445, 168–176. [Google Scholar] [CrossRef]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Li-wei, H.L.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef]
- Jack Jr, C.R.; Bernstein, M.A.; Fox, N.C.; Thompson, P.; Alexander, G.; Harvey, D.; Borowski, B.; Britson, P.J.L.; Whitwell, J.; Ward, C.; et al. The Alzheimer’s disease neuroimaging initiative (ADNI): MRI methods. J. Magn. Reson. Imaging 2008, 27, 685–691. [Google Scholar] [CrossRef]
- Poldrack, R.A.; Barch, D.M.; Mitchell, J.; Wager, T.; Wagner, A.D.; Devlin, J.T.; Cumba, C.; Koyejo, O.; Milham, M. Toward open sharing of task-based fMRI data: The OpenfMRI project. Front. Neuroinform. 2013, 7, 12. [Google Scholar] [CrossRef]
- Dressel, J.; Farid, H. The accuracy, fairness, and limits of predicting recidivism. Sci. Adv. 2018, 4, eaao5580. [Google Scholar] [CrossRef]
- Valsecchi, A.; Irurita-Olivares, J.; Mesejo, P. Age estimation in forensic anthropology: Methodological considerations about the validation studies of prediction models. Int. J. Leg. Med. 2019, 133, 1915–1924. [Google Scholar] [CrossRef] [PubMed]
- Snell, J.; Swersky, K.; Zemel, R. Prototypical networks for few-shot learning. In Proceedings of the Annual Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; pp. 4077–4087. [Google Scholar]
- Goodfellow, I. NIPS 2016 tutorial: Generative adversarial networks. arXiv 2016, arXiv:1701.00160. [Google Scholar]
- Hoshen, Y.; Li, K.; Malik, J. Non-adversarial image synthesis with generative latent nearest neighbors. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 16–20 June 2019; pp. 5811–5819. [Google Scholar]
- Bertinetto, L.; Valmadre, J.; Henriques, J.F.; Vedaldi, A.; Torr, P.H. Fully-convolutional siamese networks for object tracking. In Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 11–14 October 2016; pp. 850–865. [Google Scholar]
- Ji, S.; Xu, W.; Yang, M.; Yu, K. 3D convolutional neural networks for human action recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2012, 35, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Karpathy, A.; Fei-Fei, L. Densecap: Fully convolutional localization networks for dense captioning. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 4565–4574. [Google Scholar]
- Lathuilière, S.; Mesejo, P.; Alameda-Pineda, X.; Horaud, R. DeepGUM: Learning deep robust regression with a Gaussian-Uniform mixture model. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 202–217. [Google Scholar]
- Lathuilière, S.; Juge, R.; Mesejo, P.; Munoz-Salinas, R.; Horaud, R. Deep mixture of linear inverse regressions applied to head-pose estimation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4817–4825. [Google Scholar]
- Samek, W.; Wiegand, T.; Müller, K.R. Explainable artificial intelligence: Understanding, visualizing and interpreting deep learning models. arXiv 2017, arXiv:1708.08296. [Google Scholar]
- Castelvecchi, D. Can we open the black box of AI? Nat. News 2016, 538, 20. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.T.; Singh, S.; Guestrin, C. “Why should I trust you?” Explaining the predictions of any classifier. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 1135–1144. [Google Scholar]
- Todd, T.W. Age changes in the pubic bone. I. The male white pubis. Am. J. Phys. Anthropol. 1920, 3, 285–334. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Methods | Data |
|---|---|---|
| Mahfouz et al., 2007 [76] | 3D Statistical Shape Models, Fuzzy C-Means & Linear Discriminant Classification | 228 patella CT scans |
| Darmawan et al., 2015 [73] | PSO & Neural Network | 333 hand-wrist radiographs |
| Pinto et al., 2016 [62] | Wavelet transform & shape analysis | 19 3D point clouds of the skull supraorbital margin |
| Abdullah et al., 2017 [63] | Image processing tools | 39 Haversian canal microscopic images |
| Kaloi & He, 2018 [75] | ConvNet | 12,614 hand-wrist radiographs |
| Bewes et al., 2019 [74] | ConvNet | 1000 skull CT scans |
| Yang et al., 2019 [77] | Artificial Neural Network | 267 skull CT scans |
| Reference | Methods | Data |
|---|---|---|
| Rucci et al., 1995 [92] | Neural Network | 72 hand-wrist radiographs |
| Gross et al., 1995 [93] | Neural Network | 521 hand-wrist radiographs |
| Mahmoodi et al., 2000 [94] | Active Shape Model & Bayesian regression | 57 hand-wrist radiographs |
| Pietka et al., 2001, 2003 & 2004 [64,65,66] | Gibbs random fields, Active Contours, Wavelets & image processing tools | 1540 hand-wrist radiographs |
| Aja-Fernández et al., 2004 [59] | Fuzzy ID3 decision tree | 142 hand-wrist radiographs |
| Gertych et al., 2007 [95] | Fuzzy classifiers | 300 hand-wrist radiographs |
| Gertych et al., 2007 [96] | Gibbs random fields & active contours | 1100 hand-wrist radiographs |
| Hsieh et al., 2007 [89] | Neural Network | 909 hand-wrist radiographs |
| Hsieh et al., 2007 [97] | Fuzzy classification | 720 hand-wrist radiographs |
| Zhang et al., 2007 [98] | Fuzzy classification | 205 hand-wrist radiographs |
| Liu et al., 2008 [99] | PSO-based ROI search/feature extraction & Neural Network | 1046 hand-wrist radiographs |
| Tristan-Vega & Arribas, 2008 [100] | Adaptive Clustering &Neural Network | 158 hand-wrist radiographs |
| Thodberg et al., 2009 [101,102] | BoneXpert system: Active Appearance Model & PCA | 1559 & 719 hand-wrist radiographs, respectively |
| Giordano et al., 2010 [103] | Snakes, image processing & geometric features analysis | 106 hand-wrist radiographs |
| Martin et al., 2011 [104] | BoneXpert system | 752 hand-wrist radiographs |
| Prieto et al., 2012 [80] | Shape descriptors | 14 human 4th rib CTs |
| Davis et al., 2012 [105] | 2D shape descriptors & C4.5 | 100 hand-wrist radiographs |
| Mansourvar et al., 2012 [106] | Histogram matching | 32 hand-wrist radiographs |
| Lin et al., 2012 [107] | Fuzzy neural network | 600 hand-wrist radiographs |
| Adeshina et al., 2014 [108] | Statistical Appearance Model & Random Forest | Hand-wrist radiographs |
| Stern et al., 2014 [60] | Random Forest | 56 MR hand images |
| Stern & Urschler, 2016 [109] | Random Forest | 132 MR hand images |
| Giordano et al., 2016 [110] | Hidden Markov Models | 360 hand-wrist radiographs |
| Kashif et al., 2016 [111] | Feature extractors & SVM | 1101 hand-wrist radiographs |
| Seok et al., 2016 [112] | Ensemble of classifiers | 135 hand-wrist radiographs |
| Mansourvar et al., 2017 [90] | Mamdani fuzzy inference system | Hand-wrist radiographs |
| Kim et al., 2017 [84] | ConvNet | 200 hand-wrist radiographs |
| Lee et al., 2017 [86] | ConvNet | 8325 hand-wrist radiographs |
| Spampinato et al., 2017 [91] | ConvNet | 1391 hand-wrist radiographs |
| Larson et al., 2018 [85] | ConvNet | 14,036 hand-wrist radiographs |
| Lee & Kim, 2018 [87] | ConvNet | ∼12,000 hand-wrist radiographs |
| Mutasa et al., 2018 [88] | ConvNet | 10,289 hand-wrist radiographs |
| Li et al., 2019 [113] | ConvNet | 1875 pelvic radiographs |
| Stern et al., 2019 [114] | ConvNet and Random Forest | 328 MR hand images |
| APM | SFO | ADM | Remarks | |
|---|---|---|---|---|
| Nickerson et al., 1991 [166] | ✔ | 3D-2D Image Registration (IR), binary-coded genetic algorithm | ||
| Yoshino et al., 1995 and 1997 [167,168] | ✔ | Contour comparison using Fourier descriptors | ||
| Ghosh and Sinha, 2001 [169] | ✔ | 2D-2D IR using Artificial Neural Network | ||
| Santamaría et al., 2007 and 2009 [170,171] | ✔ | 3D skull model reconstruction using evolutionary algorithms | ||
| Ballerini et al., 2009 [172] | ✔ | 3D skull model reconstruction using heuristic features | ||
| Ibáñez et al., 2009 [173] | ✔ | 3D-2D IR, real-coded evolutionary algorithm | ||
| Ibáñez et al., 2011 [174] | ✔ | 3D-2D IR, 2D fuzzy landmark location | ||
| Campomanes-Alvarez et al., 2013 [175] | ✔ | 3D skull model simplification using multi-objective evolutionary algorithms | ||
| Duan et al., 2014 [176] | ✔ | ✔ | 3D-3D morphology correlation using canonical analysis | |
| Campomanes-Alvarez et al., 2015 [177] | ✔ | 3D-2D IR, fuzzy modeling of soft tissue depth | ||
| Campomanes-Alvarez et al., 2016 [178] | ✔ | SFO assessment using CV methods | ||
| Bermejo et al., 2017 [179] | ✔ | 3D-2D IR, mandible articulation using evolutionary algorithms | ||
| Nagpal et al., 2017 and 2018 [180,181] | ✔ | ✔ | 2D-2D Shared Transform Model for learning discriminative representations | |
| Campomanes-Alvarez et al., 2018 [182,183] | ✔ | ✔ | Hierarchical decision support system | |
| Valsecchi et al., 2018 [184] | ✔ | 3D-2D IR, state-of-the-art SFO method | ||
| Faria-Porto et al., 2019 [185] | ✔ | 2D cephalometric landmark location using ML | ||
| Tan et al., 2019 [186] | ✔ | ✔ | 3D-3D IR and matching using analytical curvature B-spline |
| Method | Correct Decisions | Ground Truth | Decision | Decision (%) | ||
|---|---|---|---|---|---|---|
| P | N | P | N | |||
| Expert Mean | 78.99% | P | 100 | 90 | 52.63% | 47.3% |
| N | 152 | 810 | 15.80% | 84.20% | ||
| Best Expert 1 | 93.33% | P | 8 | 2 | 80.00% | 20.00% |
| N | 2 | 48 | 4.00% | 96.00% | ||
| Best Expert 2 | 88.14% | P | 6 | 3 | 66.67% | 33.33% |
| N | 4 | 46 | 8.00% | 92.00% | ||
| Best Expert 3 | 86.21% | P | 5 | 3 | 62.50% | 37.50% |
| N | 5 | 45 | 10.00% | 90.00% | ||
| CADSS | 90.00% | P | 6 | 4 | 60.00% | 40.00% |
| N | 2 | 48 | 4.00% | 96.00% | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesejo, P.; Martos, R.; Ibáñez, Ó.; Novo, J.; Ortega, M. A Survey on Artificial Intelligence Techniques for Biomedical Image Analysis in Skeleton-Based Forensic Human Identification. Appl. Sci. 2020, 10, 4703. https://doi.org/10.3390/app10144703
Mesejo P, Martos R, Ibáñez Ó, Novo J, Ortega M. A Survey on Artificial Intelligence Techniques for Biomedical Image Analysis in Skeleton-Based Forensic Human Identification. Applied Sciences. 2020; 10(14):4703. https://doi.org/10.3390/app10144703
Chicago/Turabian StyleMesejo, Pablo, Rubén Martos, Óscar Ibáñez, Jorge Novo, and Marcos Ortega. 2020. "A Survey on Artificial Intelligence Techniques for Biomedical Image Analysis in Skeleton-Based Forensic Human Identification" Applied Sciences 10, no. 14: 4703. https://doi.org/10.3390/app10144703
APA StyleMesejo, P., Martos, R., Ibáñez, Ó., Novo, J., & Ortega, M. (2020). A Survey on Artificial Intelligence Techniques for Biomedical Image Analysis in Skeleton-Based Forensic Human Identification. Applied Sciences, 10(14), 4703. https://doi.org/10.3390/app10144703