Abstract
Healthcare costs continue to increase dramatically, while quality remains a significant problem. Reform measures initiated by the government will drive expansion of these costs, further stressing taxpayers and employers, and forcing hospitals to adopt fundamental changes as they try to adjust to increased demands for services and to lessening reimbursements from all payers. This struggle is best seen at the point of entry for many at a hospital: the emergency department (ED). It is at the emergency department that patients’ expectations regarding staff communication with patients, wait times, the triage process, capacity and payment will determine a significant part of a hospital’s revenue. Using Dr. Eliyahu M. Goldratt’s Thinking Process, we will determine what core problem(s) are causing a 362-bed regional West Texas hospital emergency department to lose revenue. Evaluation of the current emergency department will determine the Undesirable Effects (UDE). Using that information will lead to the construction of the Current Reality Tree (CRT), which will bring focus to the core problem(s). To break the constraints, which are the core problem(s), an Evaporative Cloud (EC) is generated. And, the end result will be to construct a Future Reality Tree (FRT), which will validate the idea(s) generated in the EC. It was determined that there are ten major UDE’s that affected this hospital’s emergency department. They were focused around staff communication, wait times, triage process, information management, service provided and bill collections. A conclusion was made that the core problem dealt with triaging patients and utilization of the services provided by the hospital. Since the reimbursement rate is affected by the patient’s satisfaction, the areas to focus on would be: triage, education, communication and retention. Although it may be neither feasible nor desirable to meet all the patient’s expectations, increased focus on those areas may increase the emergency department’s efficiency and the hospital’s bottom line.
1. Introduction
In our opinion, the current healthcare system in the United States of America suffers from inadequate quality, poor access and high costs. From personal experience, it is obvious that these organizations are under heavy scrutiny to contain costs, advance healthcare accessibility, improve customer service and manage the difficulties within their healthcare business model. The recently adopted reform legislation greatly expands access to healthcare, but does not address the failures underlying these problems. With the federal government and insurance payers basing their reimbursement rates on patient satisfaction with the services rendered, these organizations have to implement measures that meet or exceed the patient’s expectations. The executive leadership at the hospitals is trying to implement programs, such as the Thinking Process, Lean production and/or Six Sigma. Implemented properly, these programs can have a successful bottom line impact. At the forefront of this struggle and where it is most evident is at the emergency departments in their hospitals.
2. Background
In 2010, Americans spent over $ 2.6 trillion on healthcare services [7]. A good portion of this expenditure happens at regional hospitals across the United States. In West Texas, there is a 362-bed regional hospital that treats more than 100,000 patients annually through its emergency department, either as hospital admissions or as outpatients. Emergency room visits started to increase as a result of the 1986 Emergency Medical Treatment and Active Labor Act (EMTALA) that requires hospitals to perform examinations and provide stabilizing treatment before a person can be transferred to another provider. As a result of this legislation, this regional hospital has seen a significant increase in the number of patients that visit its emergency department year after year. This has led to issues such as overcrowding, degraded quality of care, communication shortfalls, untrained staff and skilled staff leaving for a competitor. On top of those issues, the hospital is also facing lower reimbursement rates for services rendered, as Medicare, Medicaid and private payers currently make payments to the hospital based on patient satisfaction. Therefore, the hospital is looking for ways to meet or exceed patients’ expectations, which will have a positive impact on the bottom line.
3. Literature Review
Increased patient volume, overcrowding and excessive wait times have forced EDs to provide more complex and prolonged care than ever before. This places patients at risk by delaying access to care and reducing the ability of ED staff to provide quality care. Dissatisfied ED patients who leave without being seen by a physician are now recognized as an important ED quality indicator [8]. The authors were correct in that the increase in patient volume has resulted in overcrowding at the West Texas hospital. Currently, this hospital only has 15 ED rooms to use, which results in wait times above one hour. In their research, 51.3% of respondents believed that patients with non-life threatening problems should wait <1 hour, and 44.6% expected to spend no more than two hours in the ED [1]. The researchers’ findings were validated at this West Texas hospital, where the majority of the patients who expect to wait less than one hour and conclude their visit in two hours actually wait on average >1 hour, and the complete ED visit is >3 hours. Yet another research group’s study suggests that problems of overcrowding and inappropriate use for non-urgent needs would not be solved by policies that just target the ED itself [15]. The policy makers do not have a clear understanding of why the public turns to the ED as a frequent source of care. The battle will be to redirect these patients to other providers like clinics, urgent care centers and/or private physicians. There needs to be a triage team that will assess patients and determine the correct course of action. The lack of triaging has led to a great deal of patient dissatisfaction.
Another issue that this hospital faces is staffing of skilled employees. In response to the current crisis in healthcare spending, hospitals have employed a variety of means to reduce costs, including limiting length of stay, restricting formularies, and gradually increasing patient-to-nurse (PTN) ratios, potentially undermining patient safety [11]. The researchers were looking for a link between skilled employee staffing and patient outcomes. Their findings proved that there was a direct link between having the correct amount of skilled staff and a positive patient experience. The results of their analysis showed that eight patients per nurse was the least expensive ratio, but was associated with the highest patient deaths. The ideal ratio was four patients per nurse, which related to lower patient deaths and shortened length of stay, and resulted in being the most cost-effective ratio. However, it is not as easy just hiring more skilled employees. Professional labor is the biggest cost component of healthcare in a hospital, yet the answer to any issue in the service delivery model is to add more people. This is a quick fix to a problem that cannot wait for investigation, measurement, redesign or process change. This attitude of quality control, being in direct conflict with cost containment, quickly achieves diminishing returns [12]. The research centered on a nurse staffing model that had been developed for a regional hospital. The conclusion of the study was a model that would predict the appropriate staffing for any given hour, shift, day or week. The model took into account the patient demand and the associated activity time required to meet that demand. Unfortunately, the model used by the regional West Texas hospital takes patient demand into account, and not the active time required to meet that demand. The norm is to just keep hiring skilled staff because turnover is so high.
The inadequate number and quality of health professionals in the health system arise from several factors, such as inadequate output from the training institutions, poor motivation and the migration of health professionals to competitors [10]. The researchers were trying to determine what the financial implications of migration of nurses were to an institution. They determined that healthcare at district level facilities suffer the most from the human resources shortages, as they are rurally based and have difficulties recruiting health workers. As a result of this, many cases requiring general care are referred to hospitals in more densely populated areas. This is a huge loss of investment for a hospital in a rural setting, as they must spend their dollars on recruitment, training, benefits, hiring bonuses and higher base salaries to bring these people into their area. Another research team concluded that the decision to leave clinical nursing often is conceptualized as one influenced by multiple factors that compound over time [9]. Some of these factors were lack of training and communication. New nurses were left to determine how to treat a patient because of the lack of communication from their supervisors and/or doctors on the proper treatment. They were not getting the necessary training from their mentors. These occurrences have led to what another research group found, that patients and their family caregivers often perceive that they are not adequately prepared for discharge and attribute post discharge problems to their unmet informational needs [13]. Poor discharge preparation contributes to readmission to the hospital, and payers will not reimburse hospitals for patients that are readmitted for previously treated procedures within a certain time frame. The research proved that the lack of communication caused patient dissatisfaction and lower payments. And yet, another research group found that communication failures (disrupted flow of critical information from caregiver to caregiver or between patient and caregiver) were associated with 31% (28 cases out of 90 cases) of adverse events [14]. That is a significant amount of cases that went wrong, and this cost the hospital time and money to correct. If proper training and protocols were in place, it would lessen the chances of adverse events happening. The researchers concluded that doing case reviews of risk management files will help in uncovering system problems that are affecting the quality of care that the hospital is trying to provide.
Healthcare costs continue to increase dramatically, while quality remains a significant problem [7]. Americans do not receive commensurate value for this level of spending [7]. In their research, the authors found that in the United States, Americans spend more on healthcare than anywhere else in the world. But that does not constitute better quality of care; instead there is a deterioration of quality and a greater degree of rationing of healthcare services. As more and more patients are becoming knowledgeable about what their money is paying for in terms of healthcare services, many are choosing to go to competitors, even if it means paying more. The authors noted that this has led to hospitals rethinking their business model and paying very close attention to patient satisfaction. It has also caught the attention of federal payers (Medicare and Medicaid) and private payers (Blue Cross, United Healthcare and Aetna), who are now reimbursing hospitals based on their “report cards”. Theses “report cards” heavily take into account a patient’s expectations and if they were met. Therefore, every department in a hospital, including the emergency department, is looking for ways to provide quality healthcare services and meet, or exceed, the patient’s expectations.
4. The Thinking Process and the Theory of Constraints
During the 1980s, Goldratt [4] wrote a book entitled The Goal. In this book, he conveys the story of a plant manager struggling to keep his plant afloat while searching for a way to improve the plant’s performance. With the help of an old college professor, the manager learns how to improve the performance of his plant, while also learning a method for resolving problems to the point of a win-win situation. Goldratt’s Theory of Constraints (TOC) focuses on the efficiency of all the processes as a whole, rather than the efficiency of any one single process. While the TOC was developed for manufacturing through Goldratt’s Thinking Process, the Thinking Process system can be used to work through many other business processes and problems.
In Goldratt’s TOC, a given group of processes will have a weakest link, and the weakest link controls the entire system’s production rate. In order to maximize the system’s production, the weakest link must be improved and all other links in the processes regulated to the speed of the weakest link. The weakest link is the constraint, and all steps must be examined together to determine the constraint; the core problem for termination.
Since the constraint is not always obvious, Goldratt [4] developed the Thinking Process. This is a series of steps used to locate the constraint (What to Change?), determine the solution (What to change to?) and how to implement the solution (How to make the change?). These steps are actually referred to as the Thinking Process. Goldratt’s next book, It’s Not Luck [6], describes the Thinking Process in much more detail.
5. What to Change?
If the symptoms of a core problem are undesirable effects (UDE’s), then the undesirable effects are merely symptoms brought on by the core problem itself. This core problem needs to be determined and eliminated. The methodology employed in the search for a core problem is based on cause and effect relationships. These cause and effect relationship are used to uncover the core problem associated with the UDE’s. The core problem is also the weak link in the operation when it concerns obtaining the goal of the company.
By determining the true core problem in a situation, it is helpful to write the current state in a diagram format. This diagram shows a logical explanation of the situation. With practice and logically based common sense, the major UDE’s can be interconnected through cause and effect relationships in a Current Reality Tree (CRT). Creating this tool leads to the process of determining “What to Change.” Goldratt [3] claims that the analytical method of a CRT is used in attempting to reveal the Archimedes point—the identification of the root cause.
This analysis method also provides a tool to understand the existing nature of the cause. It does this by discussing and scrutinizing our basic intuitive sense, which exists in our environment. It is somewhat different from the management approach of correlation and classification. All past unsuccessful efforts to eliminate the undesirable effects failed to attack and eliminate the core problem. That’s why the symptoms returned. In general, employees want to do a good job. They want to do what is best for the organization, but don’t always feel current procedures allow for core problem elimination.
6. Undesirable Effects
According to Goldratt [6] the first step in the Thinking Process is to develop a list of at least 10–12 undesirable effects that currently apply to the problem at hand.
- UDE #1: We have invested major time and money in the training of the lost staff.
- UDE #2: Skilled staff leaves for a competing medical facility.
- UDE #3: Patient wait times exceeding 15 minutes will result in patient dissatisfaction.
- UDE #4: The staff, in the Emergency Department is not properly collecting insurance co-pays and deductibles.
- UDE #5: Patients will expect us to provide a higher quality of care.
- UDE #6: We do not properly triage patients to better utilize our services.
- UDE #7: Patients expect the Emergency Department to be a Level 1 Trauma Center capable of handling all medical issues.
- UDE #8: We will not have the correct amount of staff at the right times, the right places or with the correct training.
- UDE #9: The lack of communication by the staff results in dissatisfaction.
- UDE #10: The Emergency Department becomes over capacitated to the point that there are more patients than available treatment spaces.
7. The Current Reality Tree
After organizing the Undesirable Effects in an effect-cause-effect relationship analysis, a tree took shape that identified UDE #6, “We do not properly triage patients to better utilize our services,” as the core problem. The core problem will be located at the bottom of the tree, with all other UDE’s leading from the core problem. The Current Reality Tree is read from the bottom, starting with the core problem and progressing upward through the tree using if-then statements in a logical order.
The tree reads as follows:
- If we do not properly triage patients to better utilize our services, and improper triaging causes lack of patient turnover, then the Emergency Department becomes over-capacitated to the point that there are more patients available than treatment spaces.
- If we do not properly triage patients to better utilize our services, and sufficient communication is important, then the lack of communication by the staff results in dissatisfaction.
- If we do not properly triage patients to better utilize our services, and time is critical in the healing process, then patient wait times exceeding 15 minutes will result in patient dissatisfaction. If patient wait times exceeding 15 minutes will result in patient dissatisfaction, and the patient wait time does in fact exceed 15 minutes, then the patient will be dissatisfied.
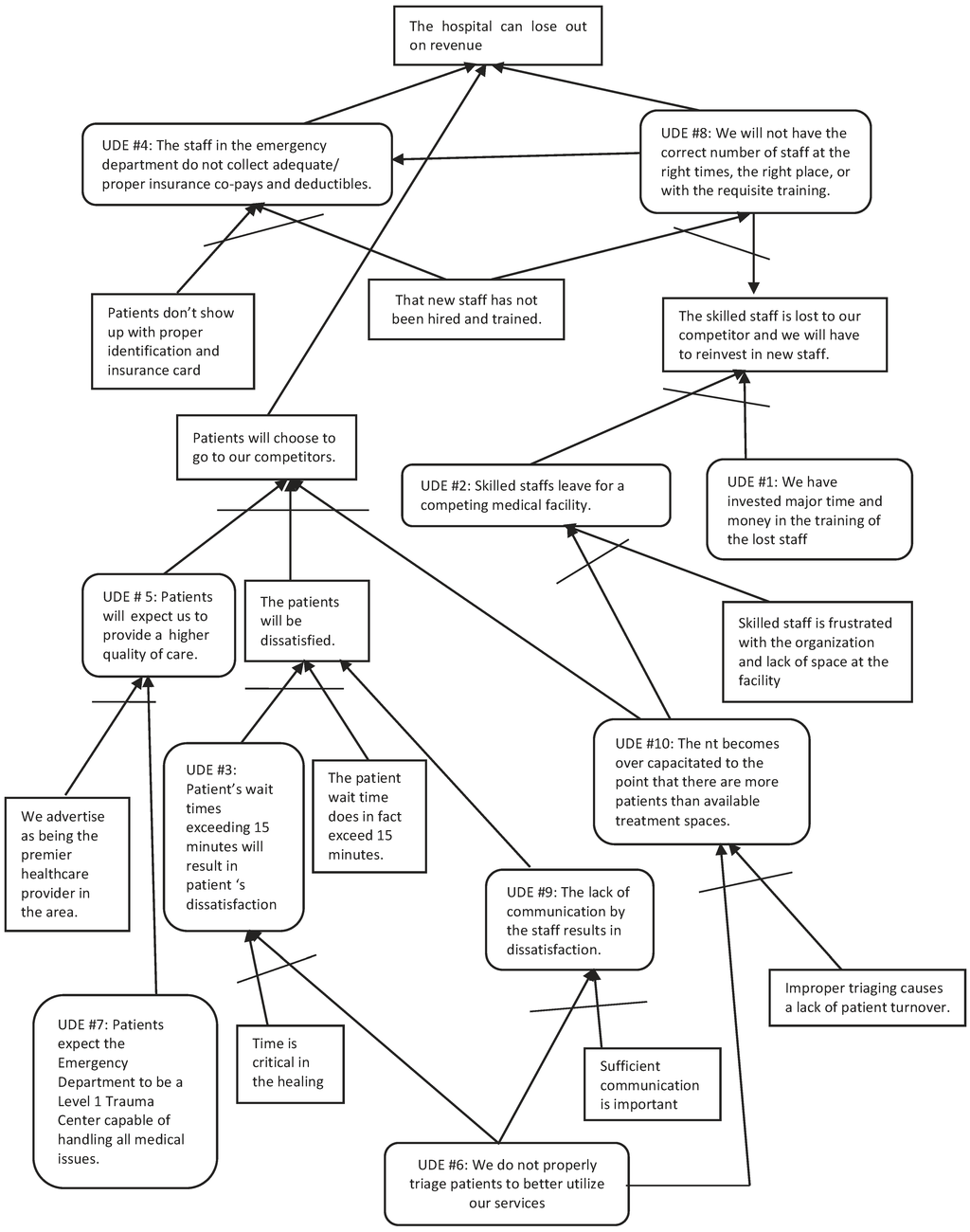
Figure 1.
Current Reality Tree of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
Figure 1.
Current Reality Tree of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
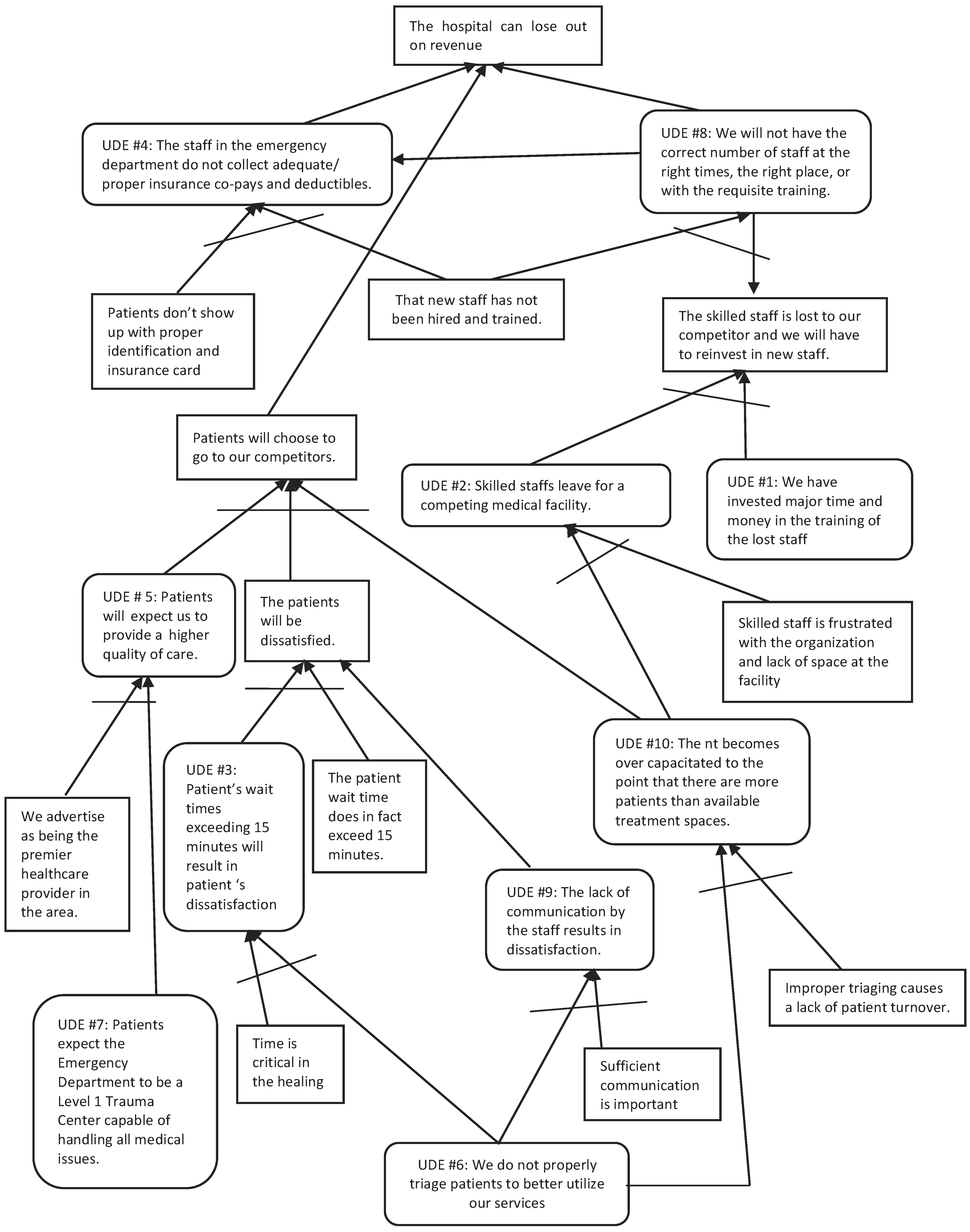
- If we do not properly triage patients to better utilize our services, and sufficient communication is important, then lack of communication results in dissatisfaction. If lack of communication results in dissatisfaction, then the patients will be dissatisfied.
- If we do not properly triage patients to better utilize our services, and improper triaging causes a lack of patient turnover, then the Emergency Department becomes over-capacitated to the point that there are more patients than available treatment spaces.
- If patients expect the Emergency Department to be a Level 1 Trauma Center capable of handling all medical issues, and we advertise as being the premier healthcare provider in the area, then patients will expect us to provide a higher quality of care.
- If patients will expect us to provide a higher quality of care, and the patients will be dissatisfied, and the Emergency Department becomes over-capacitated to the point that there are more patients than available treatment spaces, then patients will choose to go to our competitors. If patients will choose to go to our competitors, then the hospital can lose out on revenue.
- If the Emergency Department becomes over-capacitated to the point that there are more patients than available treatment spaces, and skilled staff is frustrated with the organization and lack of space at the facility, then skilled staff leaves for a competing medical facility. If skilled staff leaves for a competing medical facility, and we have invested major time and money in the training of the lost staff, then the skilled staff is lost to our competitor, and we have to reinvest in new staff. If that new staff has not been hired and trained, and the skilled staff is lost to our competitor, and we will have to reinvest in new staff, then we will not have the correct amount of staff at the right times, the right places or with the correct training. If we will not have the correct number of staff at the right times, the right places or with the requisite training, then the hospital can lose out on revenue.
- If patients do not show up with proper identification and an insurance card, and a new and untrained staff person is on duty, and we will not have the correct number of staff at the right times, the right places or with the requisite training, then the staff in the Emergency Department will not collect adequate/proper insurance co-pays and deductible information. If we will not have the correct number of staff at the right times, the right places or with the requisite training, then the staff in the Emergency Department will not collect adequate/proper insurance co-pays and deductible information, and then the hospital can lose out on revenue.
8. What to Change to?
Once the Current Reality Tree is formed, a conflict emerges that pulls the situation in two directions. The most common way of managing conflict is to compromise in some way. However, if compromise were a true solution for the problem, the conflict would have been eliminated a long time ago. Therefore the tendency to look for a compromise to handle the situation should be overcome, and the true core problem should be eliminated.
Goldratt [3] stated that, since a vacuum does not exist, eliminating the core problem means creating a new reality in which the opposite of the core problem exists. To eliminate the core problem, a tool known as the Evaporating Cloud (EC) should be used. An EC, according to Goldratt [5], lets a person precisely present the conflict facilitating the core problem and then helps find a solution by challenging the assumptions causing the conflict. The EC starts with an objective that is the opposite of the core problem. From the objective, the requirements (minimum of two) are listed. Each requirement will have at least one prerequisite. It is the prerequisites that depict the conflict. All of the requirements and prerequisites are based on assumptions that have been ingrained into our minds over time. It is these assumptions that keep us in the conflicted environment. This is the first step in freeing ourselves from the binding controversy.
9. Evaporating Cloud
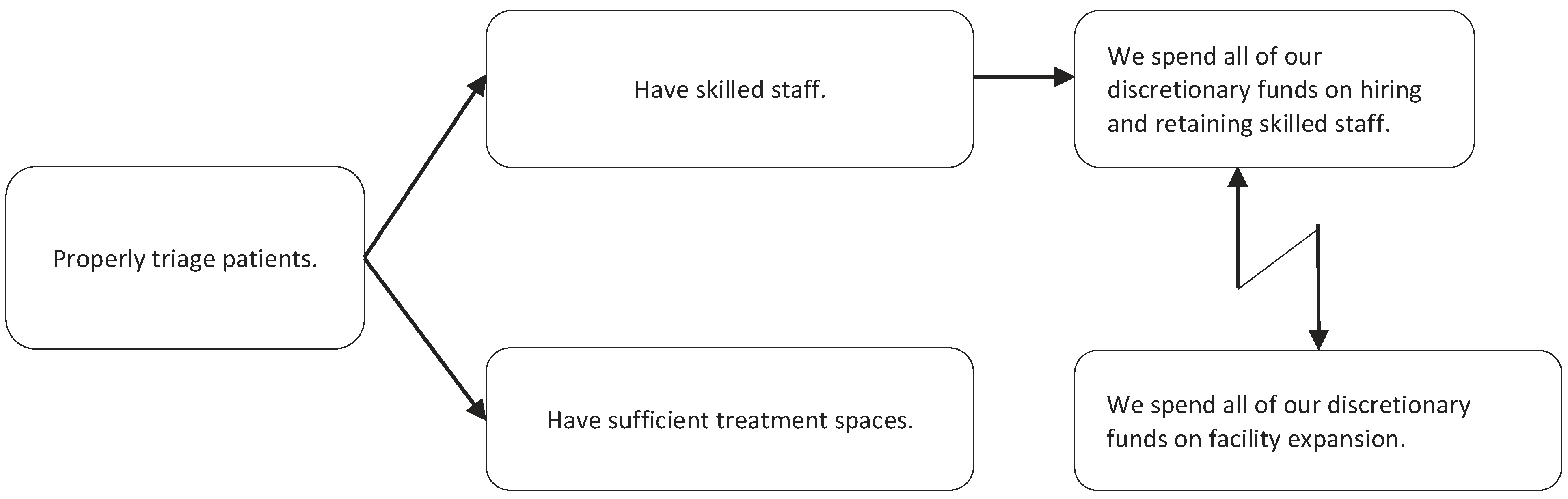
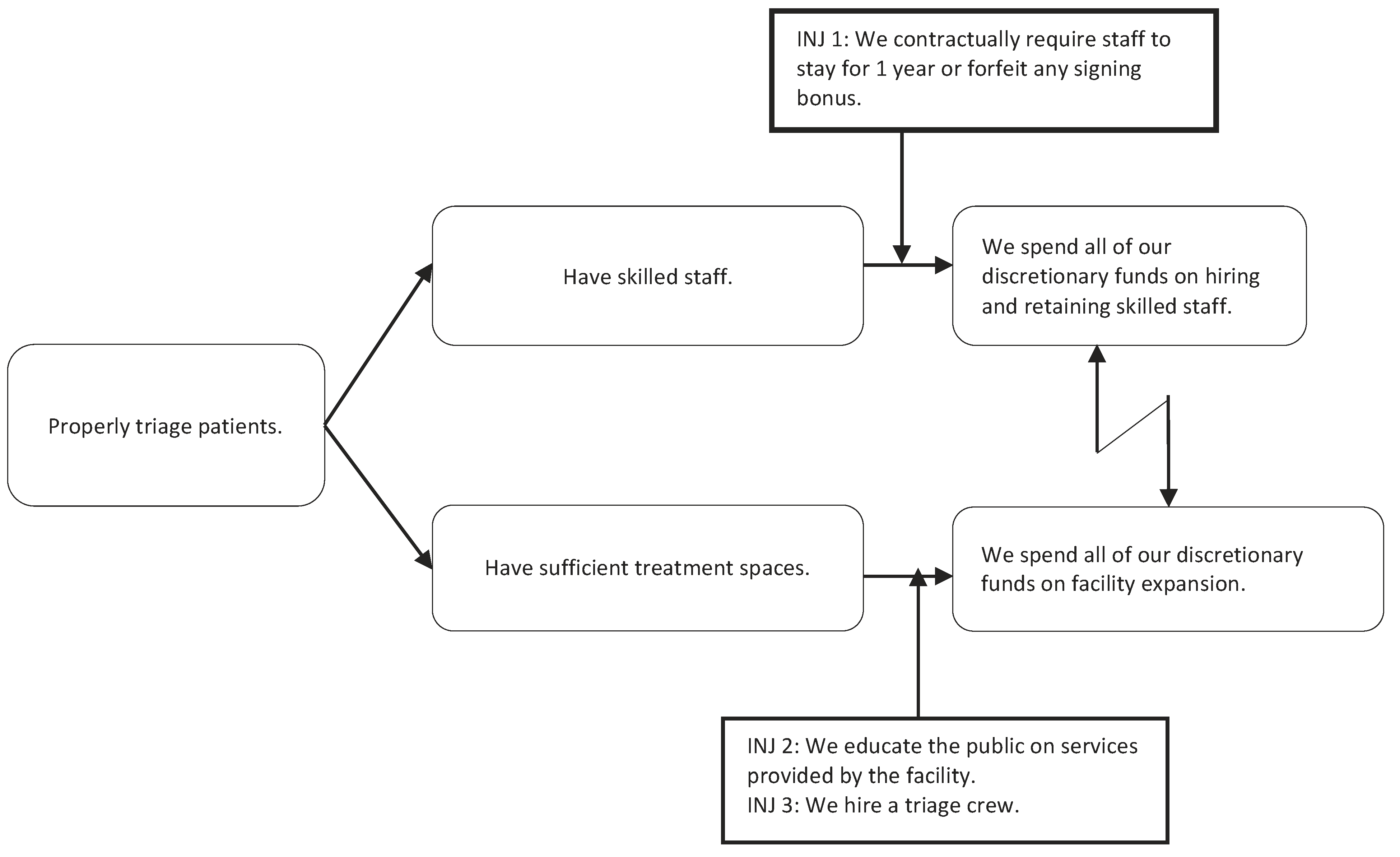
Goldratt contends that compromising does not solve the core problem, though short-term success may be realized. He suggests using the Evaporating Cloud to search for real solutions that will break the conflict and bring about a win-win solution for everyone. The core problem is, “We do not properly triage patients to better utilize our services,” so the objective of the EC will be, “Properly triage patients.” Next, we must list a minimum of two requirements. Each requirement will have at least one prerequisite. It is the prerequisites that depict the conflict. The zigzag arrow between the two prerequisites represents the conflict.
To read the EC, one would use “in order to …we (they) must” syntax.
- In order to (properly triage patients) we must (have skilled staff), and at the same time, we must (have sufficient treatment spaces). In order to (have skilled staff), we must (spend all of our discretionary funds on hiring and retaining skilled staff). In order to (have sufficient treatment spaces) we must (spend all of our discretionary funds on facility expansion).
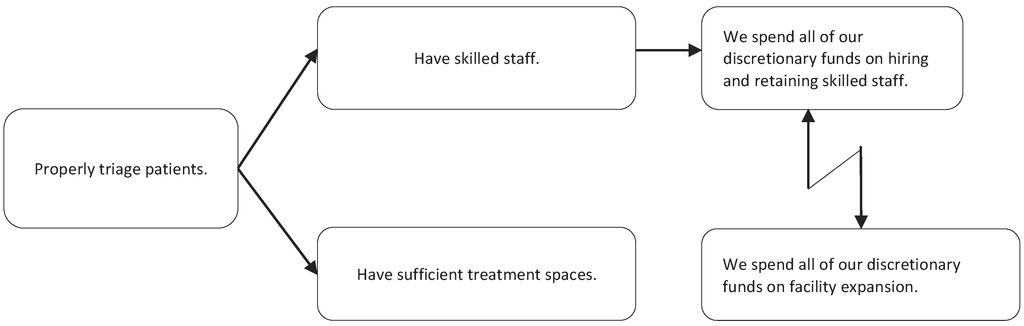
Figure 2.
Evaporative Cloud of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
Figure 2.
Evaporative Cloud of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
The injections in this instance are:
- We contractually require staff to stay for one year or forfeit any signing bonus.
- We educate the public on services provided by the facility.
- We hire a triage crew.
This tool will logically show that once the injections are implemented, the desirable effects can be accomplished. When the EC is broken, the FRT is built using the injections from the EC. The injections are connected with the cause-and-effect logic, and “clarities” and “insufficiencies” may be used where additional information is required. This process tests the solution and is enhanced by criticism and negative comments. If criticisms, negative comments and UDEs can be overcome by the proposed solution, then this provides proof of the solution and leads to the next step in the process. This process taps into the natural tendencies of criticism and negativity.
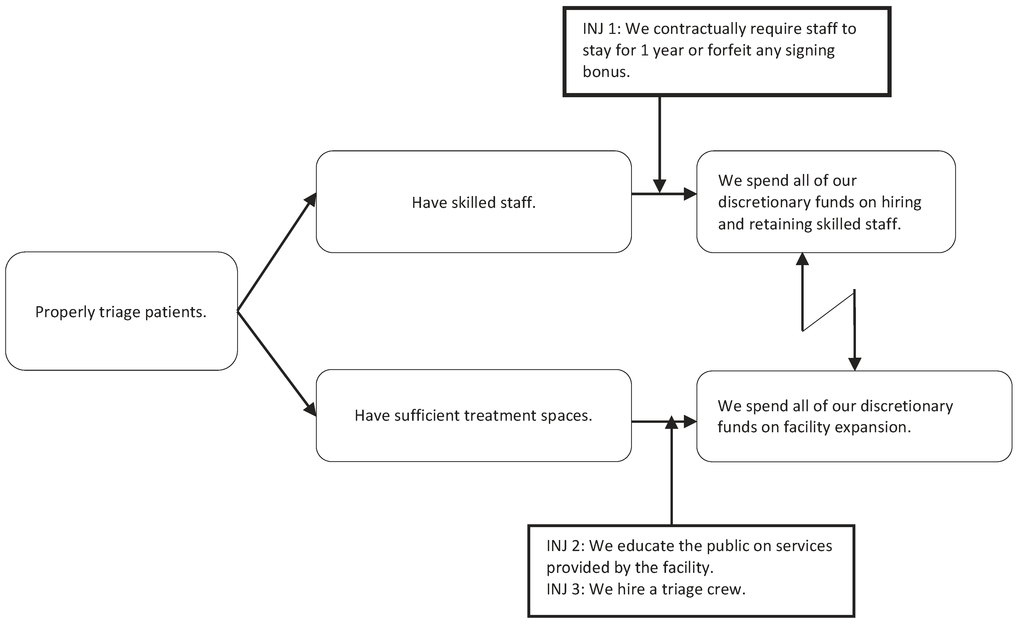
Figure 3.
Evaporative Cloud with Injections of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
Figure 3.
Evaporative Cloud with Injections of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
10. How to Cause the Change
Next, consider whether the injections will direct desirable effects. An injection allows for an acceptable resolution to one side of the conflict. With the injections and the logically based common sense cause and effect relationships, the desired effects can be connected, and the future outcome developed. This technique is called building the Future Reality Tree (FRT). The FRT, according to Goldratt [5], is the thinking process that enables a person to construct a solution that, when implemented, replaces the existing undesirable effects by desirable effects, without creating devastating new ones. Goldratt [4] goes on to add that the analytical method of the FRT is used to construct and scrutinize such a solution.
This tool will logically show that, once the injections are implemented, the desirable effects can be accomplished. When the EC conflict is broken, the FRT is built using the injections from the EC. The injections are connected with the Effect-Cause-Effect logic and use clarities and insufficiencies where additional information is required. This process tests the solution and is enhanced by criticism and negative comments. If criticisms, negative comments and UDEs can be overcome by the proposed solution, then this provides proof of the solution and leads to the next step in the process. This process taps into the natural tendencies of criticism and negativity.
11. Future Reality Tree
A FRT was then constructed in an effort to ensure that all of the UDEs would be eliminated using the resolution identified in the EC. The FRT is essentially the same as the CRT; however the injection(s) identified in the EC are placed into the tree to create a vision of the “future reality.” The FRT is read from the bottom up using if-then statements in a logical format, just as the CRT.
The tree reads as follows:
- If we hire a triage crew, then we will be properly triaging patients to better utilize our services. If we are properly triaging patients to better utilize our services, and proper triage allows for patient turnover, then the Emergency Department becomes effectively used to the point that there are sufficient treatment spaces available for the patients.
- If we hire a triage crew, then we will be properly triaging patient to better utilize our services. If we are properly triaging patients to better utilize our services, and sufficient communication is important, then the effective communication between the staff results in patient satisfaction. If the effective communication by the staff results in patient satisfaction, then the patient will be satisfied.
- If we are properly triaging patients to better utilize our services, and time is critical in the healing process, then patient wait times that do not exceed 15 minutes will result in patient satisfaction. If patient wait times that do not exceed 15 minutes will result in patient satisfaction, then the patient will be satisfied.
- If we educate the public on services provided by the facility, then patients expect the Emergency Department to provide the services we advertise. If patients expect the Emergency Department to provide the services we advertise, and we advertise as being the premier healthcare provider in the area, then we will be providing a high quality of care, which will meet the patient’s expectation.
- If the Emergency Department becomes effectively used to the point that there are sufficient treatment spaces available for the patients, and the patients will be satisfied, and we will be providing a high quality of care to meet patient’s expectation, then patients will choose to patronize us instead of our competitors. If patients will choose to patronize us instead of our competitors, then loss of revenue will be drastically reduced.
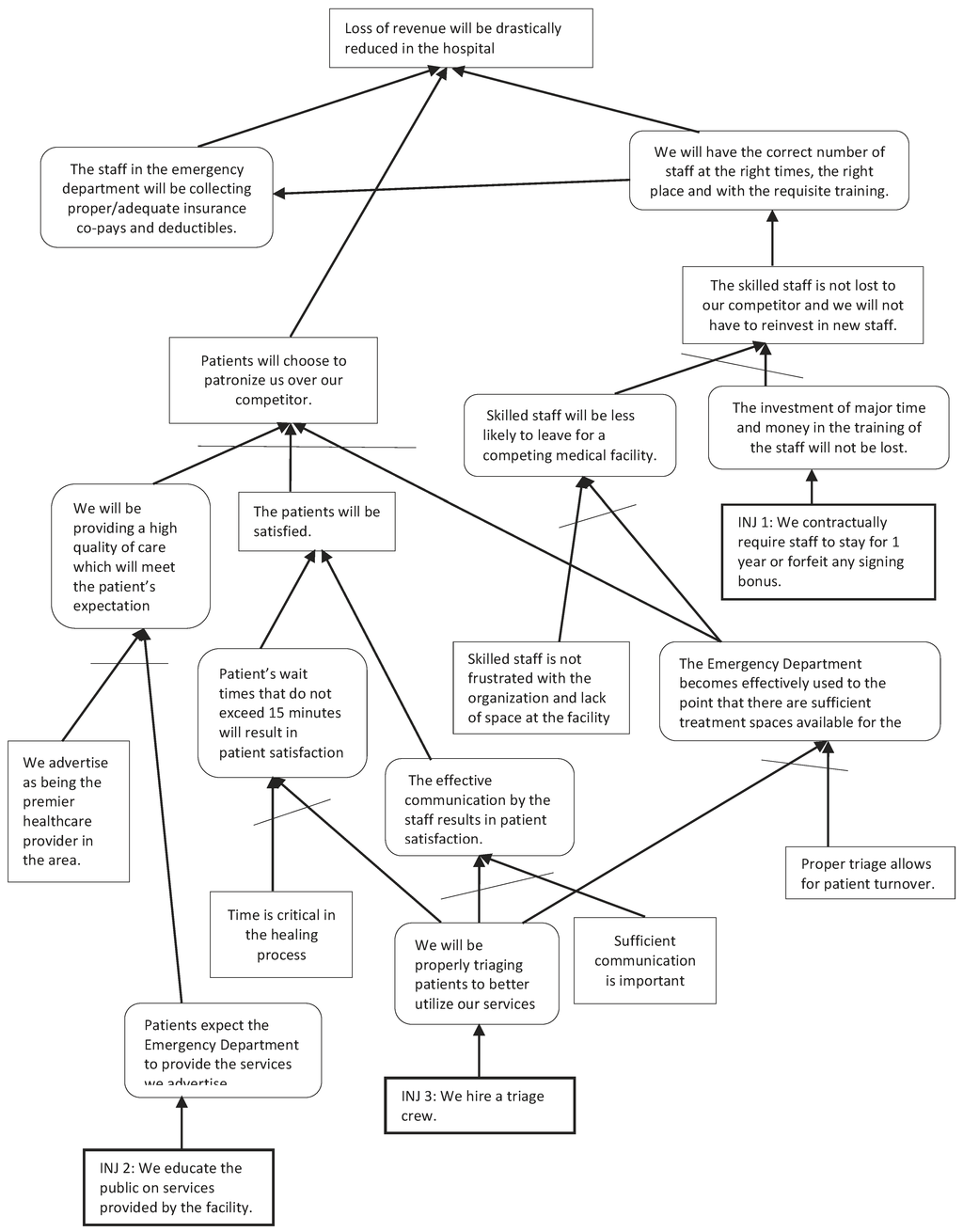
Figure 4.
Future Reality Tree of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
Figure 4.
Future Reality Tree of Goldratt’s Theory Applied to the Problems Associated with an Emergency Department at a Hospital.
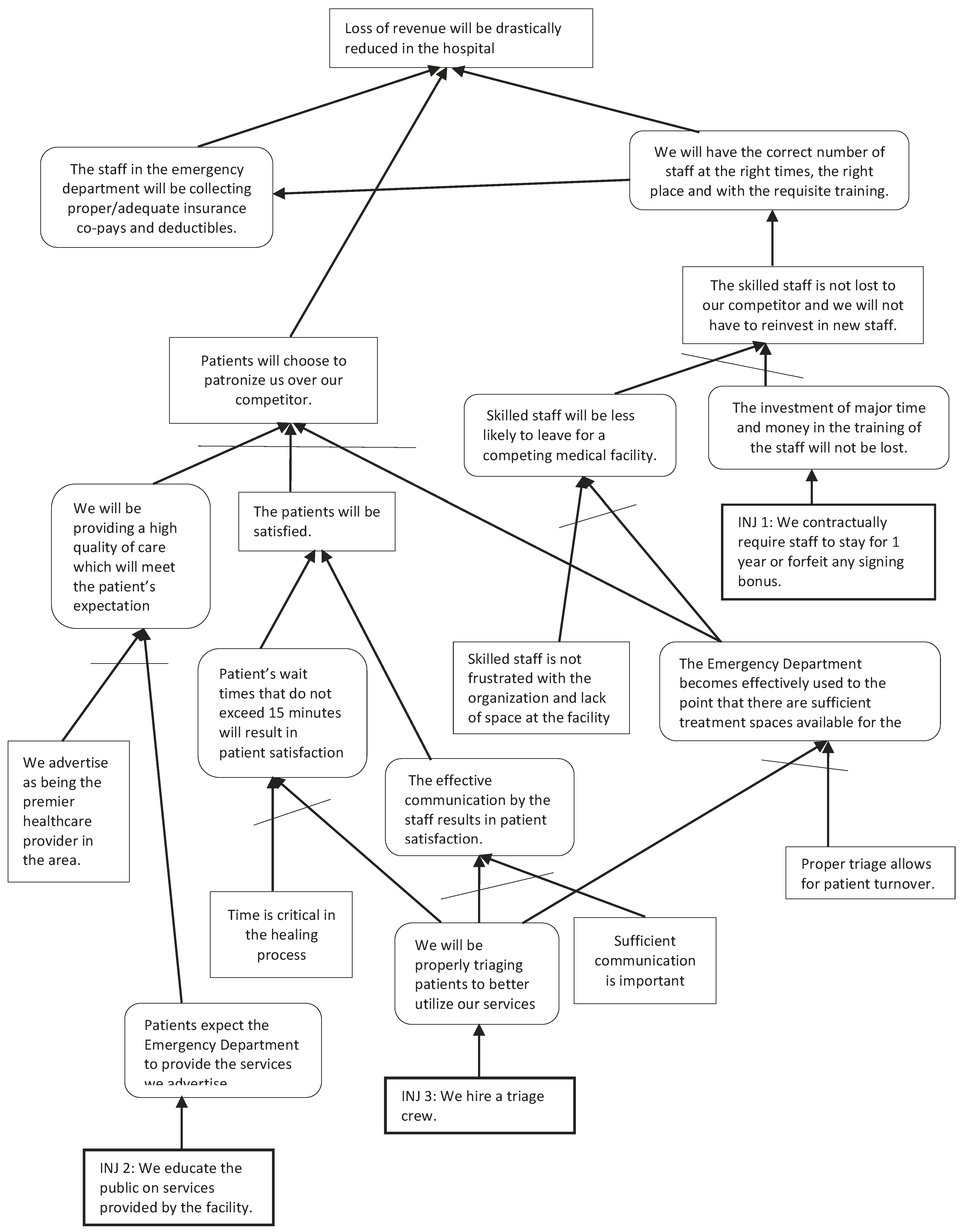
- If the Emergency Department becomes effectively used to the point that there are sufficient treatment spaces available for the patients, and skilled staff is not frustrated with the organization, then skilled staff will be less likely to leave for a competing medical facility.
- If we contractually require staff to stay for one year or forfeit any signing bonus, then the investment of major time and money in the training of the staff will not be lost, and skilled staff will be less likely to leave for a competing medical facility, then the skilled staff will not be lost to our competitor, and we will not have to reinvest in new staff. If the skilled staff is not lost to our competitor, and we will not have to reinvest in new staff, then we will have the correct number of staff at the right times, the right place and with the requisite training. If we will have the correct number of staff at the right times, the right place and with the requisite training, then loss of revenue will be drastically reduced in the hospital.
- If we have the correct number of staff at the right times, the right place and with the requisite training, then the staff in the Emergency Department will collect proper/adequate insurance co-pays and deductibles. If the staff in the Emergency Department collects proper/adequate insurance co-pays and deductibles, then loss of revenue will be drastically reduced in the hospital.
12. Conclusion
Patients value effective communication and short wait times over many other aspects of care at a hospital’s emergency department. And with the payers basing reimbursements to hospitals on patient satisfaction, hospitals are now being forced to evaluate all their policies and procedures to make them meet or exceed a patient’s expectations. Using Goldratt’s Thinking Process, it was determined that hiring a triage crew would resolve the core problem of patients not being properly triaged to better utilize the emergency department’s services. As everyone heads into the future, healthcare will become more competitive on cost, quality, speed and customer service. Hospitals will see better bottom-line results as skilled staff become better utilized and provide quick, quality and customer-focused healthcare.
13. Summary
This procedure, although somewhat different from the normal methods of analysis, is so practical that it can be applied to any problem, anywhere, at any time. According to Goldratt [4], you start with an effect in reality. Then, hypothesize a plausible cause for the existence of that effect. Since the aim is to reveal the underlying causes that govern the entire subject, try to validate the hypothesis by predicting what else this hypothesis must cause. Once such predictions are found, concentrate efforts to verify whether or not each prediction holds water by asking questions. If it turns out that one of the predictions doesn’t hold up, find another hypothesis. If all of them hold up, continue until the entire subject is understood through the bonds of cause and effect.
Bob Fox [2], President of the Goldratt Institute, states:
“I do not believe any longer that the challenge is the technology of what to do. That has been well developed—maybe not disseminated very well yet, but developed. The issue is the resistance to change once we know what to do, and I believe there is a solution to that. This method of problem solving requires abilities that everyone has and stems from systematic methods and thinking processes. It provides you with the framework necessary to direct these efforts and to verbalize your intuition to gain a better understanding of management’s ‘intestinal sensations’.”
Everyone has self-doubt. This self-doubt makes it very difficult to use the scientific method of analysis. Goldratt [4] reveals that the scientific method involves reaching into the unknown; speculating a cause and determining predicted effects probably requires an awkward personality that thrives on the unknown. However, we are dealing with the known, with current reality. There must be an equivalent method, a thinking process that facilitates building a current reality tree within the known, and we can effectively use it on any subject that we have intuition for and care about.
This cause and effect approach is used in many areas of science and mathematics. The demonstrated thinking process is what managers need the most. To carry out a successful process of ongoing improvement, there is nothing more important than the ability to answer: “What to change?”, “What to change to?” and “How to cause the change?” The results are well worth the required investments.
References
- Cooke, T.; Watt, D.; Wertzler, W.; Quan, H. Patient expectations of emergency department care: Phase II—A cross-sectional survey. CJEM 2006, 8(3), 148–157. [Google Scholar]
- Fox, R.E. The constraint theory. In Internal working paper; Avraham Y. Goldratt Institute: New Haven, CT, USA, 1989. [Google Scholar]
- Goldratt, E.M. An Introduction to Theory Of Constraints: The Production Approach; Avraham Y. Goldratt Institute: New Haven, CT, USA, 1992. [Google Scholar]
- Goldratt, E.M. An Introduction to Theory Of Constraints: The Goal Approach; Avraham Y. Goldratt Institute: New Haven, CT, USA, 1992. [Google Scholar]
- Goldratt, E.M. What is the theory of constraints? APICS The Performance Advantage 1993, June, 18–20. [Google Scholar]
- Goldratt, E. M. It’s Not Luck; North River Press: Great Barrington, MA, USA, 1994. [Google Scholar]
- Kellis, D.S.; Rumberger, J.S.; Bartels, B. Healthcare reform and the hospital industry: What can we expect? J. Healthc. Manag. 2010, 55(4), 283–297. [Google Scholar]
- Knapman, M.; Bonner, A. Overcrowding in medium-volume emergency departments: Effects of aged patients in emergency departments on wait times for non-emergent triage-level patients. Int. J. Nurs. Prac. 2010, 16(3), 310–317. [Google Scholar] [CrossRef]
- MacKusick, C.; Minick, P. Why are nurses leaving? Findings From an initial qualitative study on nursing attrition. MEDSURG Nursing 2010, 19(6), 335–340. [Google Scholar]
- Muula, A.S.; Panulo Jr., B.; Maseko, F.C. The financial losses from the migration of nurses from Malawi. BMC Nursing 2006, 5, 9–6. [Google Scholar] [CrossRef]
- Rothberg, M.B.; Abraham, I.; Lindenauer, P.K.; Rose, D.N. Improving nurse-to-patient staffing ratios as a cost-effective safety intervention. Medical Care 2005, 43(8), 785–791. [Google Scholar]
- Stansfield, T.C.; Massey, R.; Manuel, J. Life support for hospital staff. Industrial Engineer 2011, 43(2), 28–33. [Google Scholar]
- Weiss, M.E.; Yakusheva, O.; Bobay, K.L. Quality and cost analysis of nurse staffing, discharge preparation, and post discharge utilization. Health Serv. Res. 2011, 46(5), 1473–1494. [Google Scholar]
- White, A.A.; Pichert, J.W.; Bledsoe, S.H.; Irwin, C.; Entman, S.S. Cause and effect analysis of closed claims in obstetrics and gynecology. Obstet. Gynecol. 2005, 105(5), 1031–1038. [Google Scholar]
- Zuckerman, S.; Shen, Y. Characteristics of occasional and frequent emergency department users: Do insurance coverage and access to care matter? Medical Care 2004, 42(2), 176–182. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).